
Download
ORIGINAL ARTICLE
Corilagin attenuates airway inflammation and collagen deposition in ovalbumin-induced asthmatic mice
Yan Jin, Chunhua Yi*
Department of Emergency Internal Medicine, the Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University, Changzhou, Jiangsu, China
Abstract
Objective: To investigate the effects of corilagin on inflammation and collagen deposition in ovalbumin (OVA)-induced asthma mouse model and uncover the mechanism.
Methods: We constructed a mouse model of OVA-induced asthma. Enzyme-linked-immunosorbent serologic assays were conducted to detect the effects of corilagin on cytokines and Immunoglobulin E (IgE) production. Hematoxylin and eosin staining was used to show pathological features in lung tissues. Masson trichrome assay was used to examine collagen deposition. In addition, the lung function was detected by mouse lung function apparatus. Immunoblot was used to confirm the mechanism.
Results: Corilagin alleviates OVA-induced cytokine and IgE production. In addition, corilagin alleviates OVA-induced pathological changes and collagen deposition in lung tissues. Corilagin also suppressed airway resistance and lung function in mice. Mechanically, corilagin activated the adenosine monophosphate-activated protein kinase (AMPK) pathway in lung tissues.
Conclusion: Corilagin attenuates airway inflammation and collagen deposition in OVA-induced asthmatic mice via AMPK pathway.
Key words: airway resistance, AMPK pathway, asthma, collagen deposition, ovalbumin (OVA)
*Corresponding author: Chunhua Yi, Department of Emergency Internal Medicine, the Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University, No. 29, Xinglong Lane, Tianning District, Changzhou, Jiangsu 213000, China. Email address: [email protected]
Received 5 September 2023; Accepted 9 October 2023; Available online 1 November 2023
Copyright: Jin Y and Yi C
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Asthma is a heterogeneous disease featured by inflammation and hyperresponsiveness.1 It affects 1–18% of the global population. The clinical manifestations of asthma usually begin in childhood.2 Repeated asthmatic attacks can impair lung function, worsen airway damage, and impose psychological burden. Airway inflammation is considered as the essence of asthma.3 Anti-inflammatory therapy and bronchiectasis are the main treatments for asthma.4 However, inhaled corticosteroids may aggravate airway remodeling and epithelial damage in patients with asthma. Patients in remission of clinical asthma may have no clinical manifestations but still have pathological features of inflammation and remodeling. Relieving airway inflammation, mucus secretion, and collagen deposition are effective means to intervene asthma.5 Therefore, it is crucial to develop effective therapeutic drugs for treating asthma.
Corilagin, a natural polyphenol tannic acid compound, is the main active ingredient of medicinal plants, such as caryophyllum, geranium, etc.6 Recent pharmacological studies have shown that corilagin has a variety of biological activities, such as antioxidant and anti-inflammatory properties.7 For example, corilagin prevents inflammation by inhibiting oligomerization domain-like receptor family pyrin domain-containing 3 (NLRP3) inflammasome activation and pyroptosis.8 Treatment with corilagin significantly reduced inflammatory cell infiltration, production of pro--inflammatory cytokines, and oxidative stress in lung tissue with acute lung injury.9 Corilagin alleviates oxidative stress and apoptosis through the adenosine monophosphate--activated protein kinase–deacetylase sirtuin 1 (AMPK/SIRT1)-autophagy pathway, thereby alleviating intestinal ischemia/reperfusion injury.10 In addition, corilagin also has anti-allergic effects, which inhibit mast cell release mediators and reduce serum concentrations of immunoglobulin E, thereby improving skin allergies. However, the role of corilagin in asthma remains unclear.
In this study, we intended to investigate the effect of corilagin on asthma and reveal its mechanism. We constructed a mouse model of ovalbumin (OVA)-induced asthma, and results showed that corilagin attenuated airway inflammation and collagen deposition in OVA-induced asthmatic mice.
Materials and Methods
Mouse allergic model construction
Male BALB/c mice (aged 8–10 weeks) were purchased from Shanghai Jiesijie Laboratory Animal Co. Ltd. (China). Ethical approval for the present research was obtained from the Ethics Committee of the Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University (Approval 2022 KY118-01). Post-experiment, the mice were sacrificed by cervical dislocation, and the lack of heartbeat confirmed death of animals. The mice were monitored once a day before the beginning of experiment and twice a day until the end of the experiment. The animals were randomly divided into the following four groups (n = 6): (1) control, (2) OVA, (3) OVA+corilagin (20 mg/kg), and (4) OVA+corilagin (40 mg/kg). Briefly, the mice were sensitized with 40-μg OVA (Sigma, Hertfordshire, UK) in phosphate-buffered saline solution (PBS) on day 0, 7, and 14. For corilagin treatment, the mice were administrated with 0.2-mL corilagin at 20 or 40 mg/kg every day for 14 days by gavage. The model was constructed according to the previous study.9 Mice in the control group were given with equal amount of PBS per day by gavage.
Analysis of inflammatory cytokines in -bronchoalveolar lavage fluid and serum
Bronchoalveolar lavage fluid (BALF) was collected after the ligation of the left bronchial tubes. Then the mice were instilled twice with PBS in right lungs. BALF was centrifuged to obtain supernatant for further cytokine analysis. Pellets were collected for inflammatory cell assessment.
Immunoglobulin (IgE) in serum was monitored according to the manual (ZY545Hu011; HZb Science, USA).
Hematoxylin and eosin staining and lung histopathology
The left lung tissues were fixed in 4% paraformaldehyde (PFA) overnight and embedded in paraffin. Then, tissues were cut into sections and stained with hematoxylin and eosin (H&E). Lung histopathology was evaluated: 0 (no inflammatory cells), grade 1 (rarely little inflammatory cells), grade 2 (bronchi were surrounded by one layer of inflammatory cells), grade 3 (bronchi were surrounded by two to four layers of inflammatory cells), and grade 4 (most bronchi were surrounded by more than four layers of inflammatory cells).
Masson trichrome staining
Collagen deposition in airways and lung parenchyma was detected by Masson trichrome staining with Masson staining kit (G1340; Solarbio Life Sciences, Beijing, China).
Western blotting analysis
The lung tissue proteins were separated by 10% sodium dodecyl sulfate–polyacrylamide gel electrophoresis (SDS-PAGE), and the total proteins were transferred onto polyvinylidene fluoride (PVDF) membranes (24937; Millipore Sigma, MA, USA). The membranes were then blocked with 5% skimmed milk and incubated with primary antibodies against smooth muscle alpha-actin (α-SMA; Cat# ab7817, 1:1000; Abcam, Cambridge, UK), AMPK (Cat# ab2047, 1:1000), phosphorylated AMPK (p-AMPK; Cat# ab133448, 1:1000), matrix metallopeptidase 9 (MMP9) (Cat# ab76003, 1:2000), and β-actin (Cat# ab8226, 1:3000) at 4°C overnight. The membranes were incubated with secondary antibodies for 1 h. Each blot was then visualized using enhanced chemiluminescence (ECL) kit (GE, SA).
Airway hyperresponsiveness assessment
After last OVA administration for 24 h, airway hyper--responsiveness (AHR) was evaluated by forced oscillation technique. The trachea was exposed and inserted with a catheter and connected to a Master Screen (MS)-IOS pulmonary function detector (Jaeger Co. Hanover, Germany). Airway responsiveness was quantified by the level of inhaled methacholine chloride ranging from 3.125 to 25 mg/mL.
Statistical analysis
Data were analyzed using the GraphPad 8.0 software (GraphPad Software Inc., La Jolla, CA, USA). Error bars represent mean ± SD. One-way ANOVA followed by Tukey’s post hoc test was used for multiple comparisons. P < 0.05 was considered statistically significant. Each experiment was repeated thrice.
Results
Corilagin attenuates airway inflammation and IgE production
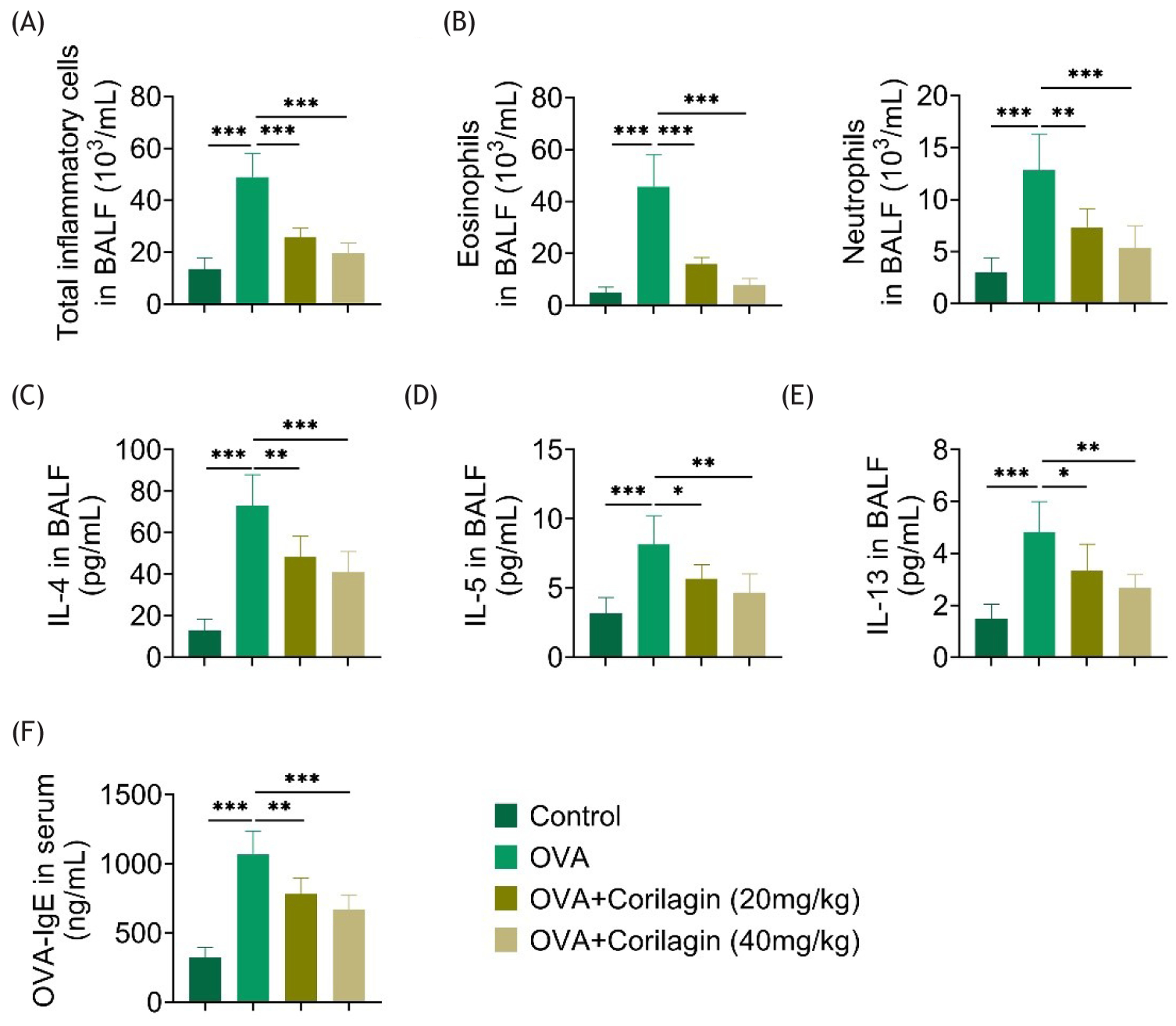
To study the effect of corilagin on inflammation-related factors, including interleukin 4 (IL-4), IL-5, IL-13, and IgE in BALF, asthma model was established and BALF was collected. The levels of factors were measured using enzyme-linked-immunosorbent serologic assay (ELISA). The number of total inflammatory cells, eosinophils and neutrophils, were enriched in OVA group (Figures 1a and 1b), and these cells were dramatically reduced in corilagin-treated mice. Similarly, the levels of all four factors were elevated in the OVA group. Treatment of corilagin at 20 and 40 mg/kg significantly decreased the levels of IL-4, IL-5, IL-13, and IgE (Figures 1c–1f). Therefore, corilagin attenuates airway inflammation and IgE production in the OVA-induced mouse lungs.
Figure 1 Corilagin attenuates airway inflammation and IgE production. (a and b) Total inflammatory cells, eosinophils and neutrophils, in the control, OVA, OVA+corilagin (20 mg/kg), and OVA+corilagin (40 mg/kg) groups. (c–f) Levels of IL-4, IL-5, IL-13, and IgE in the control, OVA, OVA+corilagin (20 mg/kg), and OVA+corilagin (40 mg/kg) groups. *P < 0.05.
Corilagin alleviates OVA-induced pathological changes in lung tissues
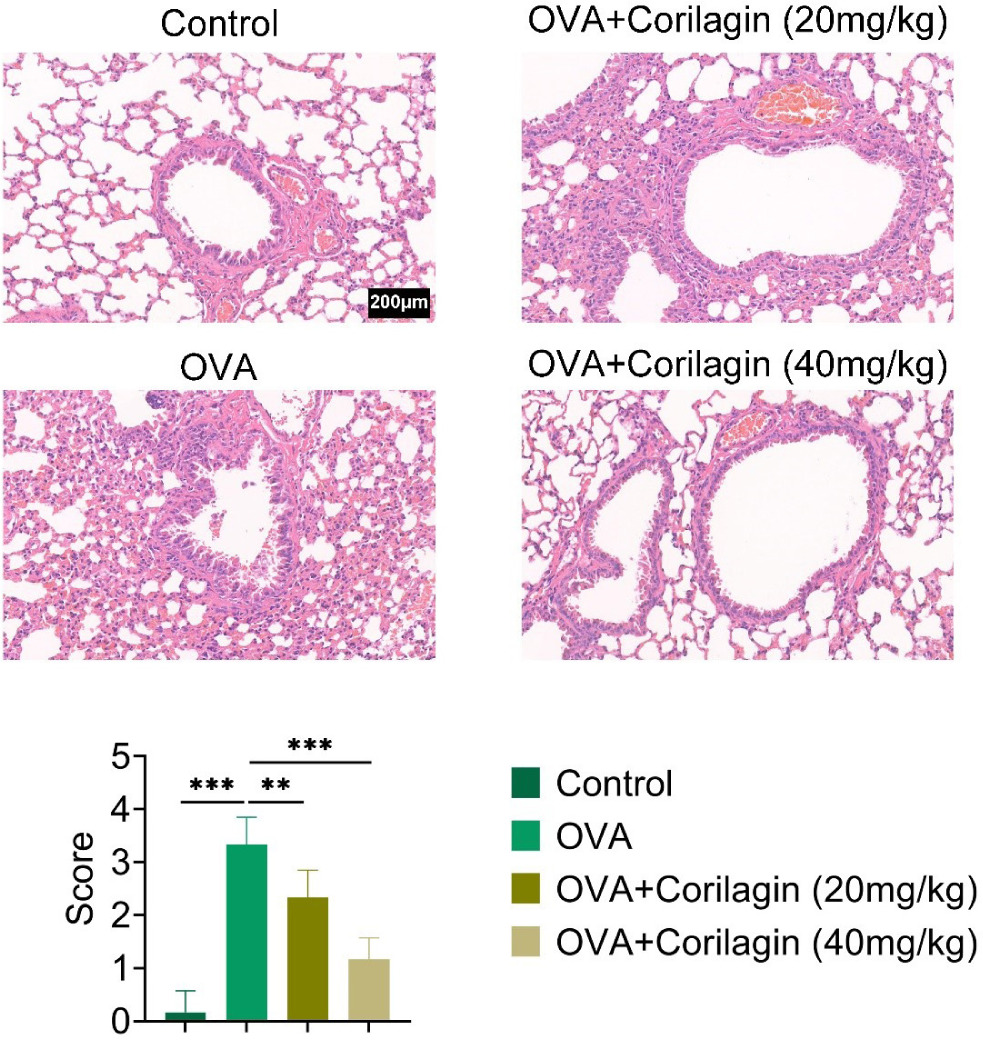
Since corilagin improved inflammatory response, we investigated the role of corilagin in attenuation of lung tissue injury. H&E staining was conducted to analyze pathological damage after OVA stimulation. Lung tissues in the OVA group displayed disordered lung tissue structure, significantly thickened alveolar wall, and the infiltration of inflammatory cells around the bronchi. However, corilagin treatment significantly improved these alterations accompanied by the reduced histological assessment score (Figure 2).
Figure 2 Corilagin alleviates OVA-induced pathological changes in lung tissues. H&E staining in the control, OVA, OVA+corilagin (20 mg/kg), and OVA+corilagin (40 mg/kg) groups. *P < 0.05.
Corragine alleviates OVA-induced collagen -deposition in lung tissues
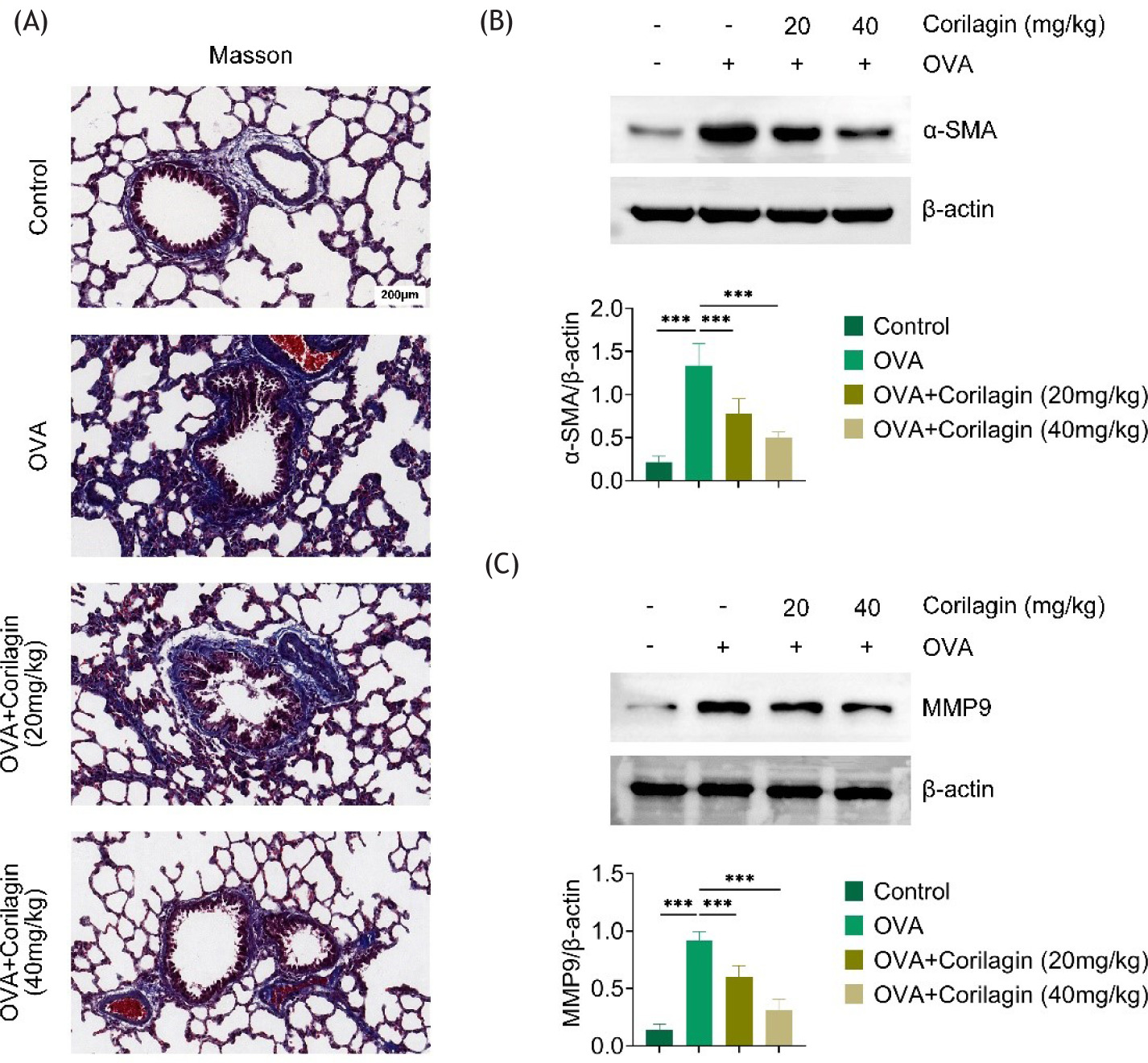
Masson staining was conducted, and as shown in Figure 3a, almost no collagen deposition was observed in lung tissues of mice in the control group, while the collagen deposition was dramatically enriched in the OVA group. Corilagin treatment significantly attenuated collagen deposition staining in both 20- and 40-mg/kg groups (Figure 3a). Moreover, the expressions of α-SMA and MMP9 were significantly elevated in the OVA group, while administration of corilagin markedly alleviated the expression of these proteins in a dose-dependent manner (Figures 3b and 3c).
Figure 3 Corragine alleviates OVA-induced collagen deposition in lung tissues. (a) Masson staining in the control, OVA, OVA+corilagin (20 mg/kg), and OVA+corilagin (40 mg/kg) groups. (b–c) Level of a-SMA and MMP9 in the control, OVA, OVA+corilagin (20 mg/kg), and OVA+corilagin (40 mg/kg) groups. *P < 0.05.
Corilagin suppresses airway resistance and lung function in OVA-induced mice
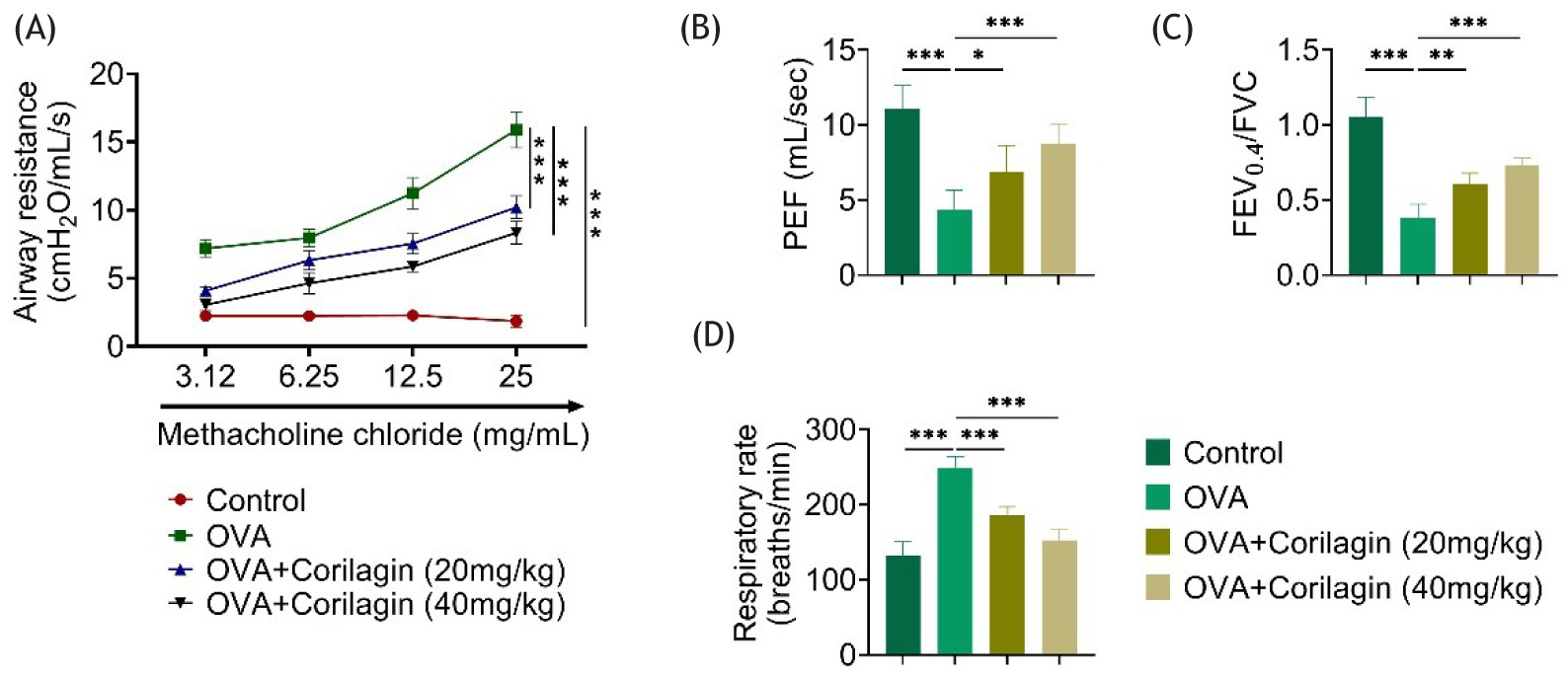
The lung function of mice was examined to assess the role of corilagin. OVA induction reduced the values of both peak expiratory flow (PEF) and forced expiratory volume in 0.4 s–forced vital capacity (FEV0.4/FVC) ratio. However, 20- or 40-mg/kg corilagin promoted PEF and FEV0.4–FVC ratio in OVA-induced asthmatic mice (Figures 4a–4c). In addition, OVA induced accelerated respiratory rate, while corilagin could restore respiratory rate nearly to a normal level (Figure 4d). These results suggested that corilagin suppressed airway resistance and improved lung function in OVA-induced mice.
Figure 4 Corilagin suppresses airway resistance and lung functioning in OVA-induced mice. (a) Airway resistance in the control, OVA, OVA+corilagin (20 mg/kg), and OVA+corilagin (40 mg/kg) groups. (b–d) PEF, FEV0.4/FVC ratio and respiratory rate in the control, OVA, OVA+corilagin (20 mg/kg), and OVA+corilagin (40 mg/kg) groups. *P < 0.05.
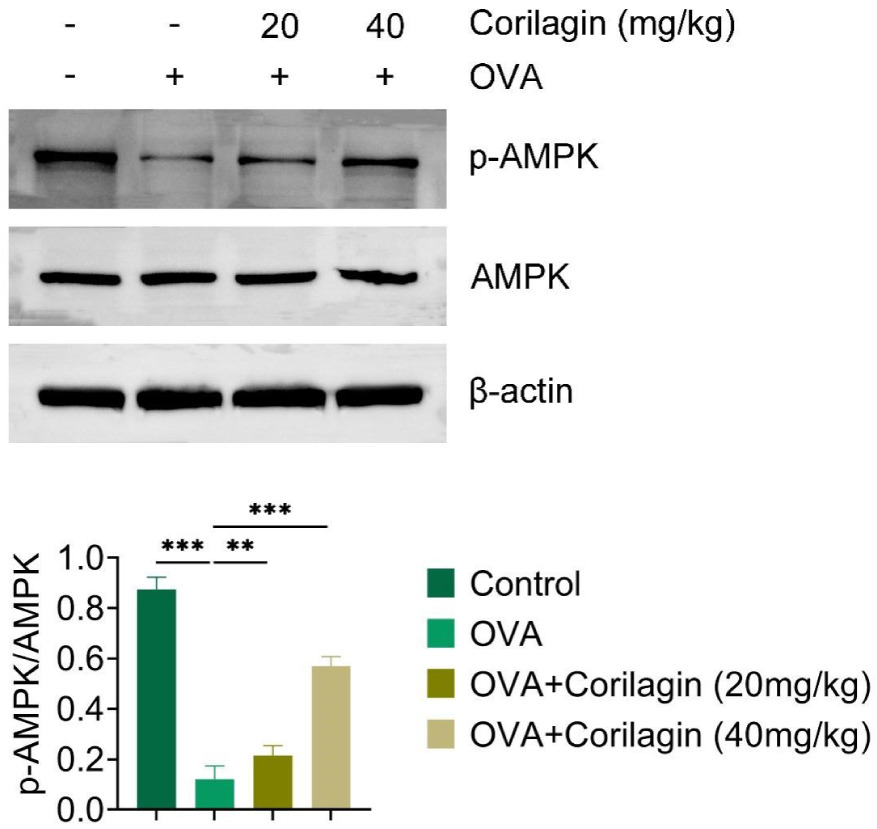
Corilagin activates AMPK pathway in lung tissues
Corilagin is known to alleviate oxidative stress and apoptosis through the AMPK/SIRT1-autophagy pathway, thereby alleviating intestinal ischemia/reperfusion injury. However, it remains to be verified whether corilagin affects MAPK pathway in OVA-induced asthma. We noticed that OVA induction suppressed the expression levels of p-AMPK. Corilagin treatment significantly increased p-AMPK levels (Figure 5). These data indicated that corilagin activated the AMPK pathway in lung tissues.
Figure 5 Corilagin activated AMPK pathway in lung tissues. The expression of p-AMPK and AMPK in the control, OVA, OVA+corilagin (20 mg/kg), and OVA+corilagin (40 mg/kg) groups. *P < 0.05.
Discussion
Asthma is a common respiratory disease, and its pathogenesis, closely related to genetic, neurological, and immunologic factors, as well as airway inflammation, is considered as the essence of asthma.11 Chronic airway inflammation is the result of the interaction of various inflammatory cells, inflammatory mediators, and cytokines. Other mechanisms of persistent airflow obstruction in asthma include airway remodeling.12 The early manifestations of the disease are mild and mostly occur in winter, and are relieved after spring warming. The course of the disease is slow, which initially is not noticed by patients. However, with progress of the disease to advanced stage, it is complicated by obstructive emphysema and the lung functioning is impaired.11
Physical exercise training is one of the rehabilitation strategies with anti-inflammatory effects and may become a good plan of action for treating airway inflammation.12 If the bronchitis in is stable and does not cause discomfort to the patient, then moderate running at this stage could improve the heart and lung functioning and immunity, and enhance physical fitness, which is beneficial for ameliorating asthma.
Notably, the thickening of type 1 collagen deposition in the airway sub-epithelium is one of the main features of airway remodeling in patients with asthma, and reversing the process of airway remodeling could also be one of the mechanisms of asthma therapy.13 Therefore, suppressing inflammation and deposition of collagen were the effective means to combat asthma.14 Increased airway resistance and reduced lung function are also important features of asthma.15 Herein, we revealed that corilagin attenuates airway inflammation and collagen deposition in an OVA-induced asthmatic mice model.
Corilagin has been reported to have effects on several cardiovascular diseases (CVDs), including hypertension, atherosclerosis, stroke, congestive heart failure, and ischemic cardiomyopathy.16 Moreover, it has antioxidant, anti-tumor, and anti-virus effects.17,,18 Corilagin inhibited the activation of oligomerization domain-like receptor family pyrin domain-containing 3 (NLRP3) inflammasome and pyroptosis via the reactive oxygen species–thioredoxin-interacting protein–-NLRP3 (ROS/TXNIP/NLRP3) axis to suppress inflammation. Corilagin could alleviate liver fibrosis via restraining indoleamine 2,3-dioxygenase-1 (IDO1)-mediated macrophage repolarization.19 In addition, corilagin could attenuate BV2 microglial activation and inflammation by regulating toll-like receptor 2 (TLR2)-mediated endoplasmic reticulum (ER) stress.16
Similarly, we also revealed effects of corilagin on inflammation in asthmatic mice. Consistently, another study indicated that corilagin ameliorated inflammation of macrophages in atherosclerosis via toll-like receptor 4–nuclear factor kappa B–mitogen-activated protein kinase (TLR4-NFκB/MAPK) axis. However, we here indicated that corilagin mediated AMPK pathway and therefore suppressed inflammation in asthmatic mice. Furthermore, corilagin alleviated intestinal ischemia/reperfusion injury (IRI) via relieving oxidative stress and apoptosis via AMPK/Sirt1-autophagy axis. Next, we must clarify whether corilagin alleviated asthma via suppressing apoptosis.
Herein, we also revealed that corilagin alleviated asthma via the AMPK pathway.8 AMPK is a key serine/threonine protein kinase for maintaining cellular energy homeostasis. It exerts NF-κB inhibitory activity through phosphorylation of its downstream target proteins, thereby blocking the process of inflammatory response and alleviating asthma manifestations.18 AMPK consists of a catalytic subunit and two regulatory subunits, which mainly regulate cellular energy metabolism. Emerging evidence supports that AMPK acts as a “metabolic brake” on energy-expenditure processes that drive inflammation and fibrosis.20 Study indicated that activation of AMPK pathway could alleviate asthma. Recent studies have shown that activated AMPK regulate energy metabolism homeostasis at both global and cellular levels. At the same time, this signaling pathway can also affect cell migration, and regulate cell differentiation and development. Several related genes, such as MMP series proteins and SMA, are affected by this signaling pathway.18–20
However, some limitations were observed to this study, such as lack of detailed molecular mechanism analysis. Next, we should carefully analyze the downstream proteins of corilagin that inhibit progression of asthma through AMPK, which can be analyzed and identified by multi-omics (different omic groups) methods.
Conclusion
We revealed that corilagin attenuated airway inflammation and collagen deposition in OVA-induced asthmatic mice by regulating AMPK signaling pathway.
Availability of Data and Materials
All data generated or analyzed in this study are included in the published article. The datasets used and/or analyzed are available from the corresponding author on reasonable request.
Conflict of Interest
The authors stated that they had no conflict of interest to disclose.
Author Contributions
Both authors contributed to conception and designing of the study. Material preparation and experiments were performed by Yan Jin. Data collection and analysis were conducted by Chunhua Yi. The first draft of the manuscript was prepared by Yan Jin and both authors commented on the previous versions of the manuscript. Both authors read and approved the final manuscript.
REFERENCES
1. Li H, Bi Q, Cui H, Lv C, Wang M. Suppression of autophagy through JAK2/STAT3 contributes to the therapeutic action of rhynchophylline on asthma. BMC Compl Med Ther. 2021;21(1):21. 10.1186/s12906-020-03187-w
2. Lv C, Li H, Cui H, Bi Q, Wang M. Solid lipid nanoparticle delivery of rhynchophylline enhanced the efficiency of allergic asthma treatment via the upregulation of suppressor of cytokine signaling 1 by repressing the p38 signaling pathway. Bioengineered. 2021;12(1):8635-49. 10.1080/21655979.2021.1988364
3. Wang M, Li H, Zhao Y, Lv C, Zhou G. Rhynchophylline attenuates allergic bronchial asthma by inhibiting transforming growth factor-beta1-mediated Smad and mitogen-activated protein kinase signaling transductions in vivo and in vitro. Exp Ther Med. 2019;17(1):251–9. 10.3892/etm.2018.6909
4. Guo J, Zhang YY, Sun M, Xu LF. Therapeutic potential of curcumin in a rat model of dextran sulfate sodium-induced ulcerative colitis by regulating the balance of Treg/Th17 cells. Inflammation. 2022;45(6):2163–71. 10.1007/s10753-022-01678-1
5. Park BG, Lee HS, Jung SH, Hong CO, Won HJ, Park HY, et al. A 90-day repeated oral toxicity study on plantamajoside concentrate from Plantago asiatica. Phytother Res (PTR). 2007;21(12):1118–23. 10.1002/ptr.2217
6. Widowati W, Kusuma HSW, Arumwardana S, Afifah E, Wahyuni CD, Wijayanti CR, et al. Corilagin potential in inhibiting oxidative and inflammatory stress in LPS-induced murine macrophage cell lines (RAW 264.7). Iran J Basic Med Sci. 2021;24(12):1656–65. 10.22038/IJBMS.2021.59348.13174
7. Liao M, Zhang R, Wang Y, Mao Z, Wu J, Guo H, et al. Corilagin prevents non-alcoholic fatty liver disease via improving lipid metabolism and glucose homeostasis in high fat diet-fed mice. Front Nutr. 2022;9:983450. 10.3389/fnut.2022.983450
8. Liu FC, Lee HC, Liao CC, Chou AH, Yu HP. Role of NADPH oxidase-derived ROS-mediated IL-6/STAT3 and MAPK/NF-kappaB signaling pathways in protective effect of corilagin against acetaminophen-induced liver injury in mice. Biology. 2023; 12(2):334. 10.3390/biology12020334.
9. Meng D, Deng X, Wu Y, Wu J, Zhang Y, Zhang J, et al. Corilagin ameliorates macrophages inflammation in atherosclerosis through TLR4-NFkappaB/MAPK pathway. Heliyon. 2023; 9(6):e16960. 10.1016/j.heliyon.2023.e16960
10. Yang MH, Baek SH, Hwang ST, Um JY, Ahn KS. Corilagin exhibits differential anticancer effects through the modulation of STAT3/5 and MAPKs in human gastric cancer cells. Phytother Res (PTR). 2022;36(6):2449–62. 10.1002/ptr.7419
11. Huang WC, Liou CJ, Shen SC, Hu S, Chao JC, Hsiao CY, et al. Urolithin A inactivation of TLR3/TRIF signaling to block the NF-kappaB/STAT1 axis reduces inflammation and enhances antioxidant defense in Poly(I:C)-induced RAW264.7 cells. Int J Mol Sci. 2022;23(9):4697. 10.3390/ijms23094697.
12. Pooladanda V, Thatikonda S, Bale S, Pattnaik B, Sigalapalli DK, Bathini NB, et al. Nimbolide protects against endotoxin--induced acute respiratory distress syndrome by inhibiting TNF-alpha mediated NF-kappaB and HDAC-3 nuclear translocation. Cell Death Dis. 2019;10(2):81. 10.1038/s41419-018-1247-9
13. Song X, Qian Y. IL-17 family cytokines mediated signaling in the pathogenesis of inflammatory diseases. Cell Signal. 2013;25(12):2335–47. 10.1016/j.cellsig.2013.07.021
14. Li T, Zhou Y, Li D, Zeng Z, Zhang S. The role of genome-scale leukocyte long noncoding RNA in identifying acute aortic dissection. Signa Vitae. 2022;18(3):101–10. 10.22514/sv.2022.030
15. Luan Y, Jin Y, Zhang P, Li H, Yang Y. Mitochondria-associated endoplasmic reticulum membranes and cardiac hypertrophy: Molecular mechanisms and therapeutic targets. Front Cardiovasc Med. 2022;9:1015722. 10.3389/fcvm.2022.1015722
16. Tan S, Su Y, Huang L, Deng S, Yan G, Yang X, et al. Corilagin attenuates osteoclastic osteolysis by enhancing HO-1 and inhibiting ROS. J Biochem Mol Toxicol. 2022;36(7):e23049. 10.1002/jbt.23049
17. Guan S, Miao F, Wang D, Hu J, Wang H. Corilagin attenuates morphine-induced BV2 microglial activation and inflammation via regulating TLR2-mediated endoplasmic reticulum stress. J Toxicol Sci. 2023;48(7):387–98. 10.2131/jts.48.387
18. Li B, Li W, Zheng M, Wang Y, Diao Y, Mou X, et al. Corilagin alleviates intestinal ischemia/reperfusion injury by relieving oxidative stress and apoptosis via AMPK/Sirt1-autophagy pathway. Exp Biol Med. 2023;248(4):317–26. 10.1177/15353702221147560
19. Wang Y, Huang S, Kong W, Wu C, Zeng T, Xie S, et al. Corilagin alleviates liver fibrosis in zebrafish and mice by repressing IDO1-mediated M2 macrophage repolarization. Phytomed Int J Phytother Phytopharmacol. 2023;119:155016. 10.1016/j.phymed.2023.155016.
20. Luo T, Zhou X, Qin M, Lin Y, Lin J, Chen G, et al. Corilagin restrains NLRP3 inflammasome activation and pyroptosis through the ROS/TXNIP/NLRP3 pathway to prevent inflammation. Oxidative Med Cell Long. 2022;2022:1652244. 10.1155/2022/1652244