
Download
REVIEW ARTICLE
Risk of allergic rhinitis in patients with inflammatory bowel disease: A systematic review and meta-analysis
Jie Liua†, Lun Caia†, Rongrong Yanga†, Liping Weia, Huazheng Luoa, Xiongbin Guib*
aDepartment of Internal Medicine, The First Affiliated Hospital of Guangxi University of Chinese Medicine, Guangxi University of Chinese Medicine, Nanning, China
bDepartment of Otorhinolaryngology, The First Affiliated Hospital of Guangxi University of Chinese Medicine, Guangxi University of Chinese Medicine, Nanning, China
†Jie Liu, Lun Cai, and Rongrong Yang are co-first authors.
*Corresponding author: Xiongbin Gui, Department of Otorhinolaryngology, The First Affiliated Hospital of Guangxi University of Chinese Medicine, Guangxi University of Chinese Medicine, Nanning 530023, P. R. China. Email address: [email protected]
Abstract
Background: Numerous parallels exist between inflammatory bowel disease (IBD) and allergic rhinitis (AR), which include risk factors (such as environmental and genetic factors), pathogenesis (immune disorders, epithelial cell barriers, etc.), and treatment (immunosuppressants and immunomodulators, such as cyclosporine and steroids). However, the risk of AR in IBD patients is unknown.
Objective: In this systematic review and meta-analysis, patients with IBD are examined for their risk of AR.
Methods: Several databases are accessible in both Chinese and English, including PubMed, BioRXiv, WanFang, the China National Knowledge Infrastructure (CNKI), Web of Science, METSTR, and MedRxiv. Findings presented at allergy, rhinology, thoracic, and gastrointestinal conferences were analyzed. Based on the inclusion and exclusion criteria, two evaluators independently retrieved data, read the literature, and evaluated bias risk. The data analysis was conducted using RevMan 5.4. Case-control and cohort studies were eligible study designs for this research.
Results: There were 10 case-control studies and 1 cohort study included in the meta-analysis. The experimental group consisted of 65,687 IBD patients, of whom 5838 had AR. A total of 345,176 participants without IBD were included in the control group, of whom 24,625 developed AR. The outcomes demonstrated that IBD patients had a higher risk of developing AR (odds ratio [OR] = 1.48, 95% confidence interval [CI] [1.12, 1.95], Z = 2.78, P = 0.005) than those without IBD.
Conclusion: The risk of AR is higher in IBD patients. Further investigation is required to determine the mechanism behind the association between AR and IBD.
Key words: allergic rhinitis, inflammatory bowel disease, meta-analysis
Received 23 June 2023; Accepted 22 September 2023; Available online 1 November 2023
Copyright: Liu J, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
A chronic condition referred to as allergic rhinitis (AR) is described as the inflammatory changes in mucous membranes in the nose caused by exposure to allergens found in the air.1 There is actually a significant prevalence of AR. Studies have shown that AR affects 40% of the global population, with differences between adults and children and between different countries in the world.2 In the International Study of Asthma and Allergies in Childhood (ISAAC) Phase III, the prevalence of AR in Turkey population aged 10–18 year is 2.9%, while in Nigeria the prevalence of AR in population aged 13–14 years is 54.1%.3 In adults, the prevalence of AR ranges from 9 to 42% in the United States. In Europe, the prevalence of AR in adults is 17% in Italy, 28.5% in Belgium, 24.5% in France, 21.5% in Spain, 20.6% in Germany, and 26% in the United Kingdom.4 A total of € 961.1 per person was spent on AR in Sweden in 2015.5 Costs will continue to rise due to an increase in disease severity and comorbidities.
Researchers have discovered that AR in children is caused by environmental and genetic risk factors,6 such as antibiotic usage, air pollution, cigarette smoking, intense physical activity, and epigenetic alterations.7 However, there is still much to learn about the risk factors of AR. Recognizing the comorbidities of AR may help with early diagnosis, therapy, and further research in the pathophysiology of AR.
Inflammatory bowel disease (IBD) occurs when there is an abnormal immune response in the mucosal lining, which can be triggered by infection with a particular pathogen or the breakdown of the mucosal barrier.8–10 It manifests as abdominal pain and diarrhea, and in the case of ulcerative colitis as blood in the stool. It consists of Crohn’s disease (CD), ulcerative colitis (UC), and IBD-unspecified (IBDU).10 About 25% of IBD patients develop the disease before the age of 20, about 18% before the age of 10, and about 4% before the age of 5, and the prevalence continues to rise.11 Although the incidence of IBD may be lower than AR, it is also a common disease within the population.
Many investigations have been performed on the comorbidity of IBD with other disorders, particularly allergies. These diseases share many similarities in terms of risk factors (such as environment and genetics), pathogenesis (including the microbiome, epithelial cell barrier, and immune disorders), and therapeutic approaches (which may involve immunomodulators and immunosuppressants such as steroids and cyclosporine).12–17 The overactive immune response of the digestive system is regarded as the root cause of IBD. Additionally, they have been linked to numerous extraintestinal symptoms, such as common allergy illnesses (asthma, atopic dermatitis, AR, etc.).18,19 IBD patients, however, are unknown to be at risk for AR. Therefore, we performed a meta-analysis of individuals with and without IBD to ascertain whether there is a connection between IBD and AR and whether IBD patients may be at more risk for AR.
Methods
This meta-analysis followed PRISMA standards.20 INPLASY has registered the meta-analysis protocol (Registration No. INPLASY202350077).
Eligibility standards
The following eligibility standards were used: (1) The study had a specific publication year and was a case-control or cohort study. (2) The research intended to investigate the risk of AR in people with IBD. (3) Subjects had IBD or were without IBD (IBD was diagnosed by clinical manifestations and the history of attacks, supplemented by gastrointestinal sampling, colonoscopy, endoscopy, etc.). (4) The diagnosis criterion of AR based on clinical manifestations and related examinations. The clinical manifestations are sneezing, nasal congestion, runny and itchy nose. Relevant tests include allergen excitation, skin prick test, enzyme allergy absorption test, and serum total IgE. (5) Chinese or English publications were used for the study.
The exclusion standards were as follows: (1) In IBD or non-IBD populations, patients with AR were not mentioned in the studies, or the data that were provided were duplicated. (2) Neither the experimental nor control groups met the study standards. (3) The sample information was insufficient. (4) The essay was a review of previously published works. (5) Drug or animal studies were reported.
Non-IBD population was the control group, while IBD population was the experimental group.
Information sources
To locate pertinent research, literature searches were carried out in the following databases: PubMed, WanFang, BioRXiv, China National Knowledge Infrastructure (CNKI), Web of Science, METSTR, and MedRxiv. Additionally, major allergy conferences, such as the World Allergy Organization, Eurasian Respiratory and Allergy Consortium, American Academy of Allergy, Asthma, and Immunology, European Academy of Allergy and Clinical Immunology, were referred. Major nasal conferences, such as American Rhinologic Society, European Rhinologic Society, and major gastroenterological meetings such as the European Joint Gastroenterological Week, American Gastroenterological Association, and Digestive Disease Week were included along with thoracic meetings such as the European Respiratory Society, American Thoracic Society, and American College of Chest Physicians. The retrieval period was from database inception to July 2023, and either Chinese or English was used as the publication language.
Search strategy
The following search terms were combined: “Crohn's Disease,” “Ulcerative Colitis,” “IBD-unspecified (IBDU),” “Inflammatory bowel disease,” “hay fever,” and “allergic rhinitis.”
Extraction of data and quality evaluation
Two investigators individually examined the literature using the same search strategy and screened it using the criteria for inclusion or exclusion. Studies that were peer-reviewed and unreviewed were both included. Reading the papers’ titles and abstracts served as the first screening, and reading the entire texts of the articles served as the second screening. Studies that satisfied the criteria as a whole were chosen and included. Discussions or third-party assistance were used if there was a dispute. Author, year, country, research type, sample size, age, sex, the total number of experimental and control groups, and the number of AR cases were the primary contents of the data extraction.
Quality assessment
Ten case-control studies and one cohort study were included in the meta-analysis; hence, the Newcastle–Ottawa Scale (NOS) served to analyze the quality of the studies.21 Three criteria were used to evaluate the studies: case selection, group comparability, and exposure factor assessment. Scores for studies might range from 0 to 9, with ≥ 6 points indicating reliability. Two researchers assessed the literature separately, and they settled disagreements through discussions and the help of a third party.
Analysis of statistics
In this research, with Review Manager version 5.4, heterogeneity tests, odds ratios (ORs), and 95% confidence intervals (CIs) were calculated. The chi-square test was used to assess interstudy heterogeneity. The I2 statistic, which showed the percentage of heterogeneity in the overall range of effect size, was used to assess and express the heterogeneity of the included literature. I2 > 50% showed blatant heterogeneity. If P > 0.1 and I2 < 50%, the fixed effect model was used for merging. If P ≤ 0.1 and I2 ≥ 50%, the random effects model was used for merging. Sensitivity analysis and subgroup analysis were also employed to examine the steady combined results and investigate potential causes of heterogeneity when the heterogeneity of test results was high.
Results
Study search results
Characteristics of included studies
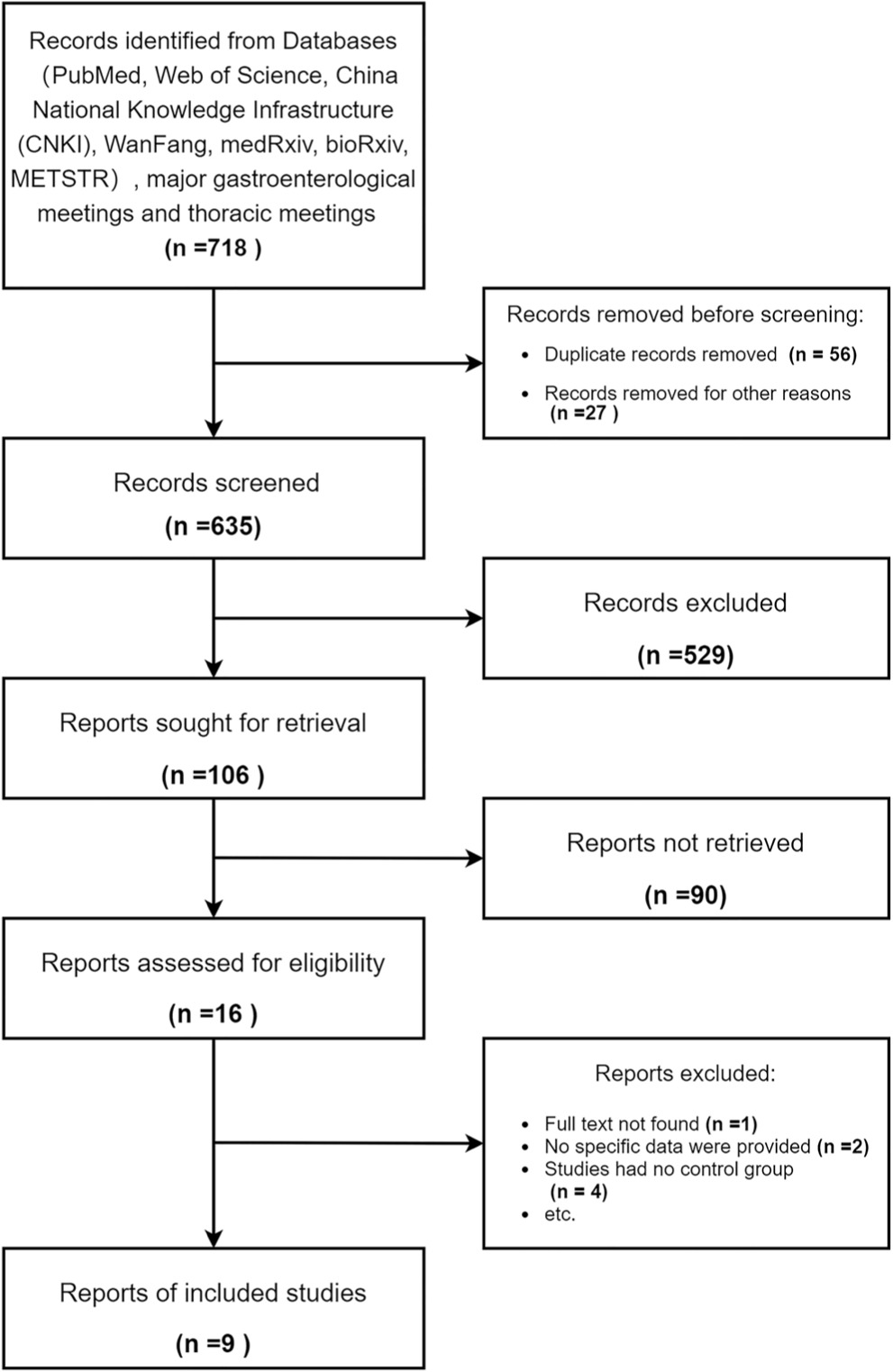
From the initial database search, 866 articles were found. There were 716 references left after deleting duplicates. 11 publications altogether from the 24 studies that were -chosen for full-text examination were used in the meta-analysis. 13 papers were excluded: 3 lacked any particular data, 1 did not have the entire text available, and 9 studies did not disclose a control group. All the included studies were from peer-reviewed journal, with no study from preprints. Figure 1 shows the flowchart detailing the procedure for choosing research.
Figure 1 PRISMA flow diagram showing the selection of clinical studies included in the review.
Information about the included studies
Overall, there were 345,176 controls without IBD and 65,687 patients with IBD in the 11 studies. Of these, 5838 IBD patients had AR, and 24,625 controls without IBD had AR. The details of the study are provided in Table 1. The studies were published between 1968 and 2023. In this paper, only the study by Alenezy et al. was a cohort study,22 while other studies were case-control studies.17,23–32 All patients in the experimental group suffered from IBD, and patients without IBD were included in the control group. However, all studies differed in age, location, and time; and some of the studies did not describe the sex distribution of patients. Two of the studies were carried out in North America,22,24 and nine were carried out in Europe.17,23,25–28,30–32 In some research, the majority of the patients were middle aged adults, with a mean age of 38–48 years;28 in other investigations, the majority of the patients were teens, with a mean age of 10–15 years.17,24,25 In the study by Myrelid et al.,26 the two groups ranged in age from 18 to 50. Only the research by Card et al.23 comprised all age categories. The specific age distribution and sex distribution of the two groups are not mentioned in the works of Hammer et al.,32 Alenezy et al.,22 D’Arienzo et al.,27,31 Myrelid et al.,26 and Pugh et al.30 Additionally, seven of these studies had large sample sizes,22–26,30,32 whereas the other studies had smaller samples.17,27,28,31 We also performed a sensitivity analysis of the outcomes. We discovered that the studies with smaller samples had no significant effect on the result, and this finding was relatively robust.
Table 1 Basic characteristics of included studies.
| Country | Type of studies | Country | Number of cases | IBD diagnostic method | AR diagnostic method | Experimental group | Control group | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total, n | Mean age | Gender (male/female) | Total, n | Mean Age | Gender (male/female) | ||||||
| Alenezy et al., 2023 | Cohort study | Canada | 64769 | Clinical diagnosis | A prescription nasal spray was used | 6346 | NA | NA | 58423 | NA | NA |
| Card et al., 2016 | Case–control studies | UK | 336479 | Clinical diagnosis | Clinical diagnosis | 56097 | 47.20 | 26283/29814 | 280382 | 47.20 | 131352/149030 |
| D'Arienzo, 2000 | Case–control studies | Italy | 100 | Clinical diagnosis (histopathological) | Clinical diagnosis (skin prick test) | 50 | 38.34 | 32/18 | 50 | 40.04 | 25/25 |
| D'Arienzo et al., 2002 | Case–control studies | Italy | 77 | Clinical diagnosis (endoscopic and histopathological) | Clinical diagnosis (skin prick test) | 40 | NA | NA | 37 | NA | 14/23 |
| Hammer et al., 1968 | Case–control studies | UK | 562 | Clinical diagnosis (histological data and radiological) | Questionnaire | 243 | NA | NA | 319 | NA | NA |
| Jewell and Truelove, 1972 | Case–control studies | UK | 119 | Clinical diagnosis (endoscopic and histopathological) | Clinical diagnosis (intradermal testing) | 81 | NA | NA | 38 | NA | NA |
| Kappelman et al., 2011 | Case–control studies | America | 4595 | Clinical diagnosis | Clinical diagnosis | 1242 | 15.00 | 683/559 | 3353 | 16.00 | 1811/1542 |
| Myrelid et al., 2004 | Case–control studies | Sweden | 1059 | Clinical diagnosis (endoscopic, histopathological, and radiological ) | Questionnaire | 280 | NA | 135/145 | 779 | NA | 360/413 |
| Pugh et al., 1979 | Case–control studies | UK | 754 | Clinical diagnosis (histopathological and radiological) | Questionnaire | 500 | NA | NA | 254 | NA | NA |
| Radon et al., 2007 | Case–control studies | Germany | 2229 | Clinical diagnosis | Questionnaire | 748 | NA | 430/318 | 1481 | 13.10 | 711/770 |
| Wasielewska et al., 2019 | Case–control studies | Poland | 120 | Clinical diagnosis (endoscopic, histopathological, and radiological ) | Questionnaire | 60 | 14.72 | 35/25 | 60 | 14.85 | 26/34 |
Experimental group: IBD with AR group; Control group: Non-IBD with AR group
Evaluation of the involved studies’ quality
All investigations obtained an average score of 7.2 using the NOS quality rating technique, as shown in Table 2. The final score was between 7 and 8. Because all patients were diagnosed based on standard clinical criteria, the diagnostic results were reliable. For exposure variables, the 11 studies did not provide response rates. A quality evaluation score of 8 was provided for two of the surveys, mostly as a result of variations in the control group. In other investigations with only outpatients, the studies scored 7. The choice of control groups was different among these investigations. In the 11 investigations, hospitalized personnel (non-IBD patients with other conditions),23,32 patients’families or companions,27,30 clinical and paramedical workers,28 and healthy persons17,22,24–26,31 made up the control group, which varied.
Table 2 Quality evaluation of included studies.
| Study | Selection | Comparability Control for important factor | Exposure | Scores | |||||
|---|---|---|---|---|---|---|---|---|---|
| Adequate definition of cases | Representa-tiveness of the cases | Selection of controls | Definition of controls | Ascertain-ment of exposure | Same method of ascertain-ment for cases and controls | Non-response rate | |||
| Alenezy et al., 2023 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 0 | 7 |
| Card et al., 2016 | 1 | 1 | 2 | 1 | 2 | 0 | 1 | 0 | 8 |
| D’Arienzo et al., 2000 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 0 | 7 |
| D'Arienzo et al., 2002 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 0 | 7 |
| Hammer et al., 1968 | 1 | 1 | 2 | 1 | 2 | 0 | 1 | 0 | 8 |
| Jewell and Truelove, 1972 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 0 | 7 |
| Kappelman et al., 2011 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 0 | 7 |
| Myrelid et al., 2004 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 0 | 7 |
| Pugh et al., 1979 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 0 | 7 |
| Radon et al., 2007 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 0 | 7 |
| Wasielewska et al., 2019 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 0 | 7 |
Results of meta-analysis
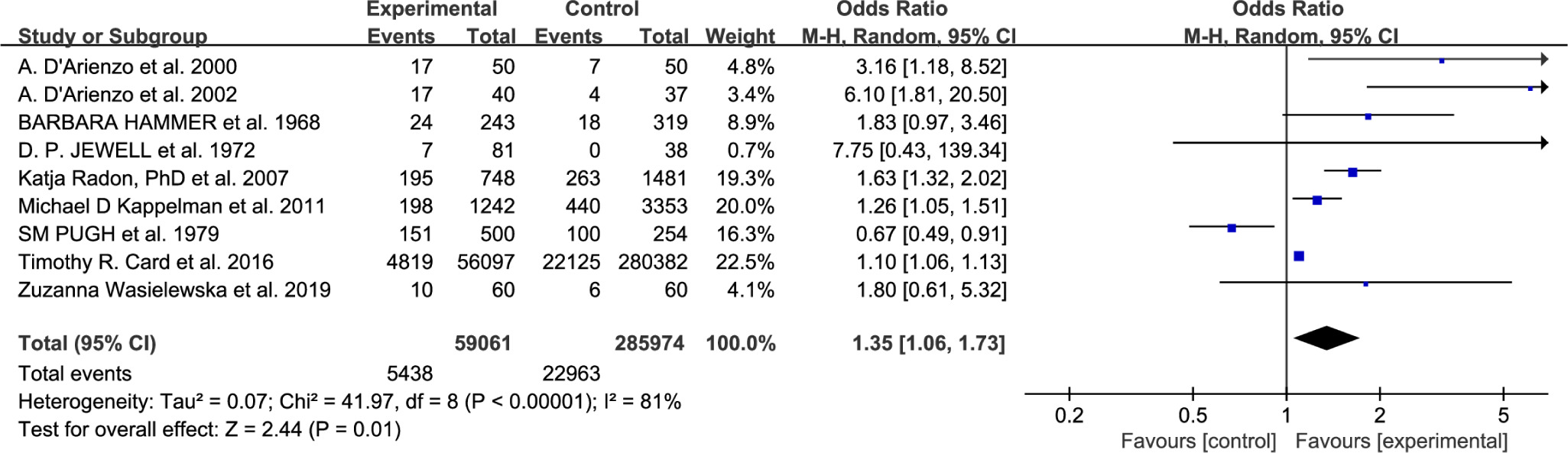
Overall, AR was more prevalent in IBD patients than in patients without IBD, with high statistical heterogeneity (X2 = 153.45, df = 10, P < 0.00001, I2 =93%, OR = 1.48 [95% CI 1.12–1.95], Z = 2.78, P = 0.005). The random effects model was applied because the outcomes revealed P ≤ 0.1 and I2 ≥ 50% (see Figure 2). The outcomes were statistically noteworthy.
Figure 2 Eleven studies’ odds ratios for the proportion of IBD patients with AR contrasted with non-IBD patients with AR are shown in a forest plot with a 95% confidence interval.
Discussion
Statement of the main conclusions
This study highlights the association between IBD and AR. AR is more likely to occur in patients with IBD. To our knowledge, this is the first meta-analysis to investigate the link between AR and IBD.
The etiology of allergy disorders and IBD has many similarities, although the precise mechanism behind their connection is yet unknown. In genetically predisposed people, an imbalance between the body’s immune system and intestinal bacteria is a crucial contributing factor.33–35 The development of immunological illnesses, particularly atopic diseases (such as AR, atopic dermatitis, and asthma), may be impacted by changes in the gut microbiota and a genetic predisposition for IBD in children.36,37 IBD and AR have similar pathogenesis, as described below. (1) Epithelial barrier: The human body must defend itself against a variety of external stimuli, including allergies, toxins, fungi, bacteria, viruses, and other pathogens. The human body has created protective epithelial barriers, such as those in the skin, lungs, and intestines, to prevent foreign antigens from breaking the immune system barrier. The nasal epithelium barrier serves as the first line of protection against airborne allergens or harmful pathogens. It is formed by cell junctions composed of tight junctions (TJ), viscous junctions, desmosomes, and half-desmosomes.38 Epithelial barrier dysfunction induces downward infiltration of risk factors and induces a nasal mucosal immune response.39 The gastrointestinal mucosa acts as a semi-permeable barrier, allowing the absorption and immune sensing of nutrients while limiting the passage of potentially harmful antigens and microorganisms. The intestinal epithelial barrier maintains intestinal integrity and immune homeostasis in a dynamic manner. This is achieved through the interaction between the structural components and molecules of the intestinal mucosa: mucus, outer layer, monolayer epithelial cells, lamina propria, and immune cells (e.g., plasma cells, dendritic cells, lymphocytes, and macrophages).40–42 There are some differences in location, structure, and partial function between nasal mucosa and intestinal mucosa, but both have similar immune functions. Airborne allergens enter principally through the passageway for the nose, and there is a situation that they may also enter the mouth and settle in the gastrointestinal tract, it is also one trigger of IBD.43 Pollen that lingers in the stomach has some remaining allergic action, according to some research.44 As a result, the epithelium interacts with the cellular immune system to serve as the body’s initial physical defense against exogenous antigens. If these epithelial barriers are damaged, allergens, pollutants, and external toxins enter the body and cause and promote inflammation to fight them.45 Flaws in the mucous membrane or epithelial cells might therefore result in a rise in the incidence of respiratory system illnesses. (such as AR, asthma, and COPD), as well as disorders of the digestive system (such as irritable bowel syndrome, IBD).17,46 AR and IBD are common mucosal inflammatory diseases.38,47 (2) Microbial alterations: The relationship between AR and IBD is explained by microbial changes. Research has demonstrated that AR patients have altered fecal flora. In addition, IBD patients’ fecal microbiomes are much less diverse than those of healthy people, and their gut bacteria are different.48 This bolsters the idea that the development of AR is influenced by the gut microbiota. In addition, IBD patients’ fecal microbiomes are much less diverse than those of healthy people, and their gut bacteria are different.49,50 Additionally, compared to healthy individuals, patients with IBD have a less stable microbiome.51 The immune system, which includes the skin, lungs, and brain, is affected by microbiome disruption. As an outcome, the “gut-skin axis,” “gut-lung axis,” and “gut-brain axis” are produced. As a result, IBD and AR cases are on the rise.29,52 (3) Immune disorders: Many researchers think that immunological abnormalities involving eosinophils, T helper cells (Th17 and Th-2), and transforming growth factor (TGF-β) might explain the complicated pathological process -causing IBD and atopic illnesses (atopic dermatitis, asthma, AR, etc.).53–56 Recent research has revealed that interleukin (IL)-17-producing Th17 cells are essential for defense. Pathogens are additionally involved in the pathogenic immune--mediated initiation and aggravation of responses, such as IBD and AR.57 IL-6, IL-23, and IL-1β stimulate the production of Th17 cells, which then secrete IL-22, IL-17, tumor necrosis factor, and proinflammatory cytokines (TNF) to recruit neutrophils and antimicrobial peptides to eliminate external infections. However, Th17 cells have a role in lesions, particularly those of the skin and airways, and are often elevated in the peripheral blood of individuals with atopic illnesses. Th17 cells may encourage neutrophilic and eosinophilic inflammation in AR, which speeds up the progression of the condition.58 Th17 cells boost immune--mediated responses and encourage IBD progression.59
Accordance and divergence from previous research
Although several studies have explored the risk of AR in patients with IBD,17,22–28,30–32 there has not been a published meta-analysis on this subject. In addition, this meta--analysis compared IBD patients with non-IBD patients, and the rigorous comparison provided strong support for the results. A Korean study showed that AR could increase the risk of developing IBD, indicating that AR and IBD were associated; however, the study did not include a control group, nor did it further explore the relationship between the two using meta-analysis.60
Effects on clinical practice
There are many similarities between AR and IBD.12–15 The findings of the meta-analysis show that individuals with IBD had a greater incidence of AR, suggesting that such people should be cautious about the risk of AR development.
Study heterogeneity
Several factors that may have contributed to the high heterogeneity of this study are as follows: (1) Among the 11 studies included, 5 used AR diagnostic questionnaires,17,25,26,30,32 one used related drugs to diagnose AR,22 and the other used clinical diagnosis combined with related tests.23,24,27,28,31 This could be one reason for the heterogeneity in the results. (2) Of the included studies, nine were in Europe17,23,25–28,30–32 and two were in North America22,24, and regional differences may be one of the reasons for the heterogeneity in study results. (3) There were differences in the diagnosis of IBD among the included studies. Four studies were described as clinical diagnoses only, and it was not determined whether corresponding histological, radiological, or radiological tests were present.22–25 It is not clear whether this leads to heterogeneity. (4) The sample size of different studies is large, while the sample size of some studies is small.17,27,28,31 This maybe lead to heterogeneity. (5) Furthermore, low-quality evidence from case-control study designs, lack of control of confounding factors in most articles. Of the included studies, five studies measured confounders such as smoking,10,22,26 dietary differences,28 regional differences (farm or city),25 and survey style (written questionnaire or telephone interview).25 None of these confounding factors changed the results. But confounders were not measured in any of the other six studies,17,24,27,30–32 which might have an impact on the results.
Strengths and limitations
The following include a few of the research’s advantages: (1) This is the first meta-analysis to research the risk of AR in IBD patients. (2) The rigorous inclusion and exclusion criteria and the elevated level of quality of research indicated by the quality evaluation of the research further supported the reliability of the findings. (3) The sample size of the literature included was large, which supports the research results. There is also a limitation of this study: there is a tight relationship between AR and IBD, we only verified the IBD increases the risk of AR, but risk of IBD in patients with AR was not explored.
Implications for future research
At present, the common pathogenesis of IBD and AR is still unclear, and further exploration of the common pathogenesis of the two is needed in the future. This may provide new ideas and new methods for the development of effective drug therapy. In addition, researchers should further investigate how to reduce the risk of AR in IBD patients and provide better treatments for those involved. It is expected that more relevant studies will be carried out in other regions in the future, with large samples and high-quality case-control studies or cohort studies to reduce sampling error. Furthermore, relevant research should be standardized to improve the level of research design and provide more reliable evidence.
Conclusion
Our findings from meta-analysis allow us to conclude that IBD and AR are connected. The occurrence of AR in people with IBD is higher than it is in individuals in general. It is possible to consider that the incidence of AR and IBD has connections and that IBD increases the risk of AR because of the associated pathologies between the two. This might serve as a foundation for estimating the risk of AR in people with IBD and further investigation into the mechanism causing their comorbidity.
Authors’ contributions
Xiongbin Gui was involved in the study’s idea and design. Lun Cai, Jie Liu, and Rongrong Yang wrote the first draft of the manuscript. Liping Wei, Huazheng Luo, and Xiongbin Gui critically revised the manuscript. All authors contributed to and approved the final version of the article.
Conflicts of interest
The authors claim that they have no financial conflicts of interest or close personal ties that may be thought to have affected the work shown in this study.
Ethical considerations
The study is only based on published literature, so an ethical declaration is not necessary.
Funding
This research was supported by the Training Plan for Thousands of Young and Middle-aged Key Teachers in Colleges and Universities of Guangxi (2020), the Project of Development and Promotion of Appropriate Medical and Health Technologies in Guangxi (Grant no. S2018114), the Guangxi Natural Science Foundation (2020GXNSFAA259020), and the National Natural Science Foundation of China (81960889).
Data availability declaration
The information in this article includes all the data that were created or analyzed throughout the investigation. The corresponding author should be contacted for any more questions.
REFERENCES
1. Hellings PW, Fokkens WJ. Allergic rhinitis and its impact on otorhinolaryngology. Allergy. 2006;61(6):656–64. 10.1111/j.1398-9995.2006.01109.x
2. Izquierdo-Domínguez A, Valero AL, Mullol J. Comparative analysis of allergic rhinitis in children and adults. Curr Allergy Asthma Rep. 2013;13(2):142–51. 10.1007/s11882-012-0331-y
3. Asher MI, Montefort S, Björkstén B, Lai CKW, Strachan DP, Weiland SK, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet. 2006;368(9537):733–43. 10.1016/S0140-6736(06)69283-0
4. Bauchau V, Durham SR. Epidemiological characterization of the intermittent and persistent types of allergic rhinitis. Allergy. 2005;60(3):350–3. 10.1111/j.1398-9995.2005.00751.x
5. Cardell L-O, Olsson P, Andersson M, Welin K-O, Svensson J, Tennvall GR, et al. TOTALL: high cost of allergic rhinitis-a national Swedish population-based questionnaire study. NPJ Prim Care Respir Med. 2016;26:15082. 10.1038/npjpcrm.2015.82
6. Testa D, Di Bari M, Nunziata M, Cristofaro GDE, Massaro G, Marcuccio G, et al. Allergic rhinitis and asthma assessment of risk factors in pediatric patients: A systematic review. Int J Pediatr Otorhinolaryngol. 2020;129:109759. 10.1016/j.ijporl.2019.109759
7. Asher MI, Stewart AW, Mallol J, Montefort S, Lai CKW, Aït-Khaled N, et al. Which population level environmental factors are associated with asthma, rhinoconjunctivitis and eczema? Review of the ecological analyses of ISAAC Phase One. Respir Res. 2010;11(1):8. 10.1186/1465-9921-11-8
8. Panwala CM, Jones JC, Viney JL. A novel model of inflammatory bowel disease: Mice deficient for the multiple drug resistance gene, mdr1a, spontaneously develop colitis. J Immunol. 1998;161(10):5733–44. 10.4049/jimmunol.161.10.5733
9. Bahn RS, Heufelder AE. Pathogenesis of Graves’ ophthalmopathy. N Engl J Med. 1993;329(20):1468–75. 10.1056/NEJM199311113292007
10. Wehkamp J, Götz M, Herrlinger K, Steurer W, Stange EF. Inflammatory bowel disease. Dtsch Arztebl Int. 2016;113(5):72–82. 10.3238/arztebl.2016.0072
11. Rosen MJ, Dhawan A, Saeed SA. Inflammatory bowel disease in children and adolescents. JAMA Pediatr. 2015;169(11):1053–60. 10.1001/jamapediatrics.2015.1982
12. Sicherer SH, Sampson HA. Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol. 2014;133(2):291–307. 10.1016/j.jaci.2013.11.020
13. Ko JK, Auyeung KK. Inflammatory bowel disease: Etiology, pathogenesis and current therapy. Curr Pharm Des. 2014;20(7):1082–96. 10.2174/13816128113199990416
14. Bernstein DI, Schwartz G, Bernstein JA. Allergic rhinitis: Mechanisms and treatment. Immunol Allergy Clin North Am. 2016;36(2):261–78. 10.1016/j.iac.2015.12.004
15. Turner D, Levine A, Escher JC, Griffiths AM, Russell RK, Dignass A, et al. Management of pediatric ulcerative colitis: joint ECCO and ESPGHAN evidence-based consensus guidelines. J Pediatr Gastroenterol Nutr. 2012;55(3):340–61. 10.1097/MPG.0b013e3182662233
16. Lee J W, Eun C S. Inflammatory bowel disease in Korea: Epidemiology and pathophysiology. Korean J Intern Med. 2022; 37(5):885–94. 10.3904/kjim.2022.138
17. Wasielewska Z, Dolinska A, Wilczynska D, Szaflarska-Poplawska A, Krogulska A. Prevalence of allergic diseases in children with inflammatory bowel disease. Postepy Dermatol Alergol. 2019;36(3):282–90. 10.5114/ada.2018.81189
18. Tzanakis NE, Tsiligianni IG, Siafakas NM. Pulmonary involvement and allergic disorders in inflammatory bowel disease. World J Gastroenterol. 2010;16(3):299–305. 10.3748/wjg.v16.i3.299
19. Rothfuss KS, Stange EF, Herrlinger KR. Extraintestinal manifestations and complications in inflammatory bowel diseases. World J Gastroenterol. 2006;12(30):4819–31. 10.3748/wjg.v12.i30.4819
20. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–84. 10.7326/M14-2385
21. Wells G A, Wells G, Shea B, Shea B, O’Connell D, Peterson J, et al. The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses, F, 2014 [C].
22. Alenezy N, Nugent Z, Herman S, Zaborniak K, Ramsey CD, Bernstein CN. Aeroallergen-related diseases predate the diagnosis of inflammatory bowel disease. Inflamm Bowel Dis. 2023;29(7):1073–9. 10.1093/ibd/izac184
23. Card TR, Langan SM, Chu TP. Extra-gastrointestinal manifestations of inflammatory bowel disease may be less common than previously reported. Dig Dis Sci. 2016;61(9):2619–26. 10.1007/s10620-016-4195-1
24. Kappelman MD, Galanko JA, Porter CQ, Sandler RS. Association of paediatric inflammatory bowel disease with other immune-mediated diseases. Arch Dis Child. 2011;96(11):1042–6. 10.1136/archdischild-2011-300633
25. Radon K, Windstetter D, Poluda AL, Mueller B, von Mutius E, Koletzko S. Contact with farm animals in early life and juvenile inflammatory bowel disease: A case-control study. Pediatrics. 2007;120(2):354–61. 10.1542/peds.2006-3624
26. Myrelid P, Dufmats M, Lilja I, Grinn C, Lannerstad O, Sjödahl R. Atopic manifestations are more common in patients with Crohn disease than in the general population. Scand J Gastroenterol. 2004;39(8):731–6. 10.1080/00365520410005955
27. D’Arienzo A, Manguso F, Scarpa R, Astarita C, D’Armiento FP, Bennato R, et al. Ulcerative colitis, seronegative spondyloarthropathies and allergic diseases: The search for a lin. Scand J Gastroenterol. 2002;37(10):1156–63. 10.1080/003655202760373362
28. D’Arienzo A, Manguso F, Astarita C, D’Armiento FP, Scarpa R, Gargano D, et al. Allergy and mucosal eosinophil infiltrate in ulcerative colitis. Scand J Gastroenterol. 2000;35(6):624–31. 10.1080/003655200750023598
29. Salem I, Ramser A, Isham N, Ghannoum MA. The gut microbiome as a major regulator of the gut-skin axis. Front Microbiol. 2018;9:1459. 10.3389/fmicb.2018.01459
30. Pugh SM, Rhodes J, Mayberry JF, Roberts DL, Heatley RV, Newcombe RG. Atopic disease in ulcerative colitis and Crohn’s disease. Clin Allergy. 1979;9(3):221–3. 10.1111/j.1365-2222.1979.tb01545.x
31. Jewell DP, Truelove SC. Reaginic hypersensitivity in ulcerative colitis. Gut. 1972;13(11):903–6. 10.1136/gut.13.11.903
32. Hammer B, Ashurst P, Naish J. Diseases associated with ulcerative colitis and Crohn’s disease. Gut. 1968;9(1):17–21. 10.1136/gut.9.1.17
33. Dixon LJ, Kabi A, Nickerson KP, McDonald C. Combinatorial effects of diet and genetics on inflammatory bowel disease pathogenesis. Inflamm Bowel Dis. 2015;21(4):912–22. 10.1097/MIB.0000000000000289
34. Guo AY, Stevens BW, Wilson RG, Russell CN, Cohen MA, Sturgeon HC, et al. Early life environment and natural history of inflammatory bowel diseases. BMC Gastroenterol. 2014;14:216. 10.1186/s12876-014-0216-8
35. Gearry RB, Richardson AK, Frampton CM, Dodgshun AJ, Barclay ML. Population-based cases control study of inflammatory bowel disease risk factors. J Gastroenterol Hepatol. 2010;25(2):325–33. 10.1111/j.1440-1746.2009.06140.x
36. Garn H, Bahn S, Baune BT, Binder EB, Bisgaard H, Chatila TA, et al. Current concepts in chronic inflammatory diseases: Interactions between microbes, cellular metabolism, and inflammation. J Allergy Clin Immunol. 2016;138(1):47–56. 10.1016/j.jaci.2016.02.046
37. Li M, Wang M, Donovan SM. Early development of the gut microbiome and immune-mediated childhood disorders. Semin Reprod Med. 2014;32(1):74–86. 10.1055/s-0033-1361825
38. Nur Husna SM, Tan H-TT, Md Shukri N, Mohd Ashari NS, Wong KK. Nasal epithelial barrier integrity and tight junctions disruption in allergic rhinitis: Overview and pathogenic insights. Front Immunol. 2021;12:663626. 10.3389/fimmu.2021.663626
39. Zhang R, Zhang L, Li P, Pang K, Liu H, Tian L. Epithelial barrier in the nasal mucosa, related risk factors and diseases. Int Arch Allergy Immunol. 2023;184(5):481–501. 10.1159/000528969
40. Vancamelbeke M, Vermeire S. The intestinal barrier: A fundamental role in health and disease. Expert Rev Gastroenterol Hepatol. 2017;11(9):821–34. 10.1080/17474124.2017.1343143
41. Salvo Romero E, Alonso Cotoner C, Pardo Camacho C, Casado Bedmar M, Vicario M. The intestinal barrier function and its involvement in digestive disease. Rev Esp Enferm Dig. 2015;107(11):686–96. 10.17235/reed.2015.3846/2015
42. Barbara G, Barbaro MR, Fuschi D, Palombo M, Falangone F, Cremon C, et al. Inflammatory and microbiota-related regulation of the intestinal epithelial barrier. Front Nutr. 2021;8:718356. 10.3389/fnut.2021.718356
43. Vutcovici M, Brassard P, Bitton A. Inflammatory bowel disease and airway diseases. World J Gastroenterol. 2016;22(34):7735–41. 10.3748/wjg.v22.i34.7735
44. Einarsson R, Renck B, Taudorf E. In vitro studies of degradation of birch and timothy pollen allergen preparations by human duodenal juice. Allergy. 1988;43(6):469–72. 10.1111/j.1398-9995.1988.tb00921.x
45. Kabashima K, Honda T, Ginhoux F, Egawa G. The immunological anatomy of the skin. Nat Rev Immunol. 2019;19(1):19–30. 10.1038/s41577-018-0084-5
46. Sugita K, Kabashima K. Tight junctions in the development of asthma, chronic rhinosinusitis, atopic dermatitis, eosinophilic esophagitis, and inflammatory bowel diseases. J Leukoc Biol. 2020;107(5):749–62. 10.1002/JLB.5MR0120-230R
47. Martini E, Krug SM, Siegmund B, Neurath MF, Becker C. Mend your fences: The epithelial barrier and its relationship with mucosal immunity in inflammatory bowel disease. Cell Mol Gastroenterol Hepatol. 2017;4(1):33–46. 10.1016/j.jcmgh.2017.03.007
48. Liu X, Tao J, Li J, Cao X, Li Y, Gao X, et al. Dysbiosis of fecal microbiota in allergic rhinitis patients. Am J Rhinol Allergy. 2020;34(5):650–60. 10.1177/1945892420920477
49. Joossens M, Huys G, Cnockaert M, De Preter V, Verbeke K, Rutgeerts P, et al. Dysbiosis of the faecal microbiota in patients with Crohn’s disease and their unaffected relatives. Gut. 2011;60(5):631–7. 10.1136/gut.2010.223263
50. Pascal V, Pozuelo M, Borruel N, Casellas F, Campos D, Santiago A, et al. A microbial signature for Crohn’s disease. Gut. 2017;66(5):813–22. 10.1136/gutjnl-2016-313235
51. Andoh A, Imaeda H, Aomatsu T, Inatomi O, Bamba S, Sasaki M, et al. Comparison of the fecal microbiota profiles between ulcerative colitis and Crohn’s disease using terminal restriction fragment length polymorphism analysis. J Gastroenterol. 2011;46(4):479–86. 10.1007/s00535-010-0368-4
52. Lee SY, Lee E, Park YM, Hong SJ. Microbiome in the gut–skin axis in atopic dermatitis. Allergy Asthma Immunol Res. 2018;10(4):354–62. 10.4168/aair.2018.10.4.354
53. Virta LJ, Ashorn M, Kolho KL. Cow’s milk allergy, asthma, and pediatric IBD. J Pediatr Gastroenterol Nutr. 2013;56(6):649–51. 10.1097/MPG.0b013e318285e9d8
54. Walker MM, Powell N, Talley NJ. Atopy and the gastrointestinal tract—A review of a common association in unexplained gastrointestinal disease. Expert Rev Gastroenterol Hepatol. 2014;8(3):289–99. 10.1586/17474124.2014.881716
55. Kotlyar DS, Shum M, Hsieh J, Blonski W, Greenwald DA. Non-pulmonary allergic diseases and inflammatory bowel disease: A qualitative review. World J Gastroenterol. 2014;20(32):11023–32. 10.3748/wjg.v20.i32.11023
56. Hemdan NY, Birkenmeier G, Wichmann G, Abu El-Saad AM, Krieger T, Conrad K, et al. Interleukin-17-producing T helper cells in autoimmunity. Autoimmun Rev. 2010;9(11):785–92. 10.1016/j.autrev.2010.07.003
57. Ueno A, Jeffery L, Kobayashi T, Hibi T, Ghosh S, Jijon H. Th17 plasticity and its relevance to inflammatory bowel disease. J Autoimmun. 2018;87:38–49. 10.1016/j.jaut.2017.12.004
58. Liu Y, Zeng M, Liu Z. Th17 response and its regulation in inflammatory upper airway diseases. Clin Exp Allergy. 2015;45(3):602–12. 10.1111/cea.12378
59. Brand S. Crohn’s disease: Th1, Th17 or both? The change of a paradigm: New immunological and genetic insights implicate Th17 cells in the pathogenesis of Crohn’s disease. Gut. 2009;58(8):1152–67. 10.1136/gut.2008.163667
60. Soh H, Lee HJ, Han K, Park S, Hong SW, Moon JM, et al. Atopic diseases are associated with development of inflammatory bowel diseases in Korea: A nationwide population-based study. Clin Gastroenterol Hepatol. 2021;19(10):2072–2081.e6. 10.1016/j.cgh.2020.07.049