
Download

ORIGINAL ARTICLE
Clinical manifestations and expression of CD18 to guide the diagnosis of leukocyte adhesion deficiency type 1: Mexico experience
Elma Isela Fuentes-Laraa, Gabriel Emmanuel Arce-Estradaa, Abner Bojalil-Cabildob, Marco Antonio Yamazaki-Nakashimadab, Sara Elva Espinosa-Padillaa, Luisa Berenise Gamez-Gonzalezc, Rosa María Nideshda Ramirez-Uribed, Omar Josue Saucedo-Ramireze, Laura Berron-Ruiza*
aImmunodeficiency Laboratory, National Institute of Pediatrics, Mexico City, Mexico
bClinical Immunology Service, National Institute of Pediatrics, Mexico City, Mexico
cChihuahua Children's Specialty Hospital, Chihuahua, Mexico
dBone Marrow Transplant Unit, The National Pediatrics Institute, México City, Mexico
eClinical Immunology Service, Children’s Hospital of Mexico “Federico Gómez,” Mexico City, Mexico
Abstract
Background: Leukocyte adhesion deficiency type 1 (LAD-1) is an inborn error of immunity characterized by a defect in leukocyte trafficking.
Methods: Patients with clinical suspicion of LAD-1 were referred to our institution. Complete blood count and flow cytometric analysis, to identify the expression of CD18, CD11b, and the lymphocyte population phenotyping, were performed, and statistical analysis was completed.
Results: We report clinical manifestations and immunological findings of six Mexican patients diagnosed with LAD-1. The diagnosis was based on typical clinical presentation, combined with laboratory demonstration of leukocytosis, and significant reduction or near absence of CD18 and its associated molecules CD11a, CD11b, and CD11c on leukocytes. We found atypical manifestations, not described in other countries, such as early-onset autoimmunity or infections caused by certain microorganisms.
Conclusions: Patients with LAD-1 may present with atypical manifestations, making flow cytometry an indispensable tool to confirm the diagnosis. We present the first report of LAD-1 patients in a Latin American country.
Key words: CD18, inborn error of immunity, infections, leukocyte adhesion deficiency type-1, leukocytosis
*Corresponding author: Laura Berrón-Ruiz, Immunodeficiency Laboratory, National Institute of Pediatrics, Av. del Imán 1, Piso 9, Torre de Investigación, Col. Insurgentes Cuicuilco, 04530, Coyoacán, Mexico City, Mexico. Email address: [email protected]
Received 18 May 2023; Accepted 4 August 2023; Available online 1 November 2023
Copyright: Fuentes-Lara EI, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Leukocyte adhesion deficiency (LAD) is an inborn error of immunity (IEI) characterized by a defect in leukocyte trafficking.1 It is divided into three types. Type 1 occurs most frequently.2 LAD-1 is an autosomal recessive disease, characterized by pathogenic variants in ITGB2 gene. This gene is located on chromosome 21 and encodes the β chain (CD18) of β2 integrins. Deficiencies or defects of CD18 affect the migration of leukocytes to the sites of inflammation or infection, making the tissues susceptible to infections. Dysregulation of the interleukin (IL)-23–IL-17 axis has been reported in LAD-1 patients, causing decreased wound healing.3
Leukocyte adhesion deficiency type 1 (LAD-1) is characterized by recurrent bacterial infections of the skin and mucosal surfaces, particularly gingivitis and periodontitis. Infections begin at birth or during the first weeks of life. Omphalitis (infection of the umbilicus) with delayed separation of the cord is typical. Skin ulcers secondary to infection may expand without healing control. Infections may be caused by Staphylococcus aureus and Pseudomonas aeruginosa. Cellulitis and necrotic abscesses, especially in the perirectal area, can occur, but the absence of the formation of pus is the most frequent observation. Neutrophilia is marked, usually 5–20 times above the normal range, reaching up to 100,000 cells/mm3 during acute infections.4
Survival of the disease without a hematopoietic stem cell transplant (HSCT) is lower by 2 years.5
Other clinical manifestations have been reported in Mexican patients with LAD-1, such as hepatosplenomegaly, gastroenteritis, pneumonia, otitis, balanoposthitis, ecthyma gangrenosum, gluteal cellulitis, oral candidiasis, urinary infection, sepsis, and infections caused by Escherichia coli, Streptococcus pneumoniae, Klebsiella pneumoniae, and cytomegalovirus. Other atypical manifestations are urachus persistence, mucosal bleeding, impaired platelet aggregation, and absent clot retraction. Hemolytic anemia stands out among autoimmunity manifestations.6–10
In a Mexican child affected by LAD-1, laboratory findings reported elevated serum levels of immunoglobulin (Ig)A, IgG, IgM, IgE and C3 and C4 fractions of the complement system.10
This was the first report on patients with LAD-1 in a Latin American country.
Materials and methods
Patients
Patients with clinical suspicion of LAD-1 were referred to our institution. Complete blood count (CBC) and lymphocyte population phenotyping were performed. The authors established clear policies to secure the privacy of patients.
Lymphocyte population phenotyping
We performed a flow cytometric analysis of controls and LAD-1 patients. Lymphocyte populations were enumerated for whole-blood samples with anticoagulant ethylenediaminetetraacetic acid (EDTA) (BD Vacutainer®; NJ, USA) and stained with the following mixtures of monoclonal antibodies (mAbs): anti-CD45-FITC/anti-CD14-PE, -anti-CD3-FITC/anti-CD19-PE/anti-CD45-PerCP, anti-CD4-FITC/anti-CD8-PE/ anti-CD3-PerCP, anti-CD3-FITC/anti-CD19-PE/anti-CD45-PerCP, and anti-CD3-FITC/anti-CD16+56-PE/anti-CD45-PerCP.
In addition, IgG1-FITC/IgG2-PE/anti-CD45-PerCP were used for isotype controls. All antibodies were purchased from BD Biosciences (San Diego, CA, USA). Samples were incubated for 20 min at room temperature in the dark. After incubation, erythrocytes were lysed by suspending the cells in 500-mL fluorescence-activated cell sorting (FACS) lysing solution (BD Biosciences) for 10 min. Cells were washed with phosphate-buffered albumin (PBA) (1% bovine serum albumin in PBS) and fixed using 1% formalin in phosphate-buffered saline solution (PBS).
Expression of CD18 and CD11b
To identify the expression of CD18 and CD11b, peripheral blood was stained with the following combination of monoclonal antibodies: anti-CD14-APC/anti-CD18-PE-Cy5/anti-CD11b-FITC. In addition, IgG1-FITC/IgG1-PE/ anti-IgG1-PE-Cy5 (Beckman Coulter, Brea, CA, USA) were used for isotype controls. Samples were incubated for 20 min at room temperature in the dark. After incubation, erythrocytes were lysed by suspending the cells in 500 ml FACS lysing solution (BD Biosciences, San Jose, CA) for 10 min. Cells were then washed with PBA (1% bovine serum albumin in PBS) and fixed using 1% formalin in PBS. Flow cytometry was performed on Arias1® (BD Biosciences). The cells were analyzed using the FlowJo 8.8 software (TreeStar®, Ashland, OR). The analysis strategy is shown in Figure 1.
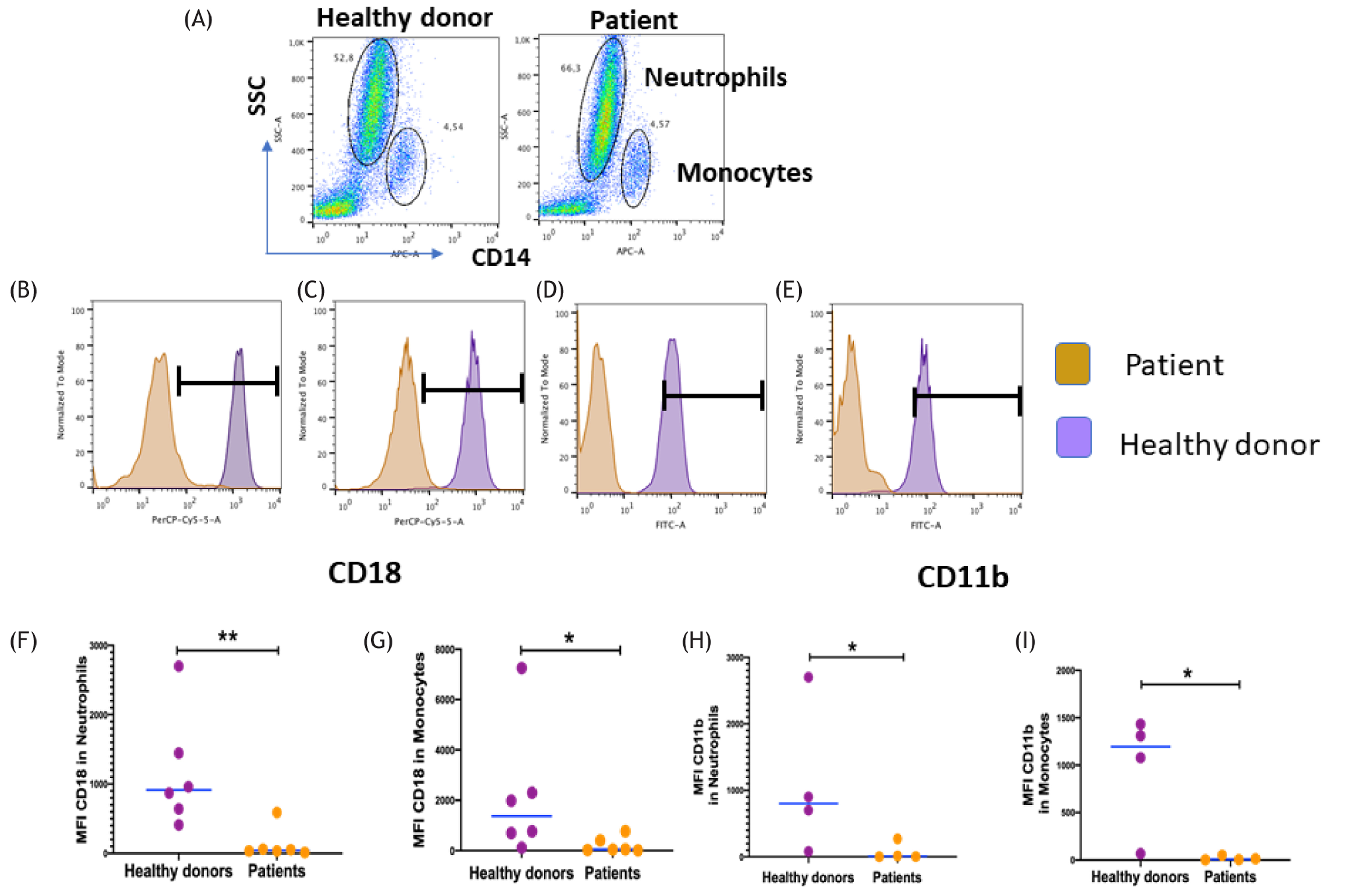
Figure 1 Analysis expression of CD18 and CD11b in neutrophils and monocytes by flow cytometry. (A) Neutrophils and monocytes were gated in CD14+ and side-scatter regions. Expression of CD18 in (B) neutrophils and (C) monocytes in patients (yellow) and healthy donors (violet). Expression of CD11b in (D) neutrophils and (E) monocytes in patients (yellow) and healthy donors (violet). The black bar shows a positive expression of CD18 or CD11b. Comparison of expression of CD18 MFI in (F) neutrophils and (G) monocytes; and that of CD11b MFI in (H) neutrophils and (I) monocytes in patients (n = 6) and healthy donors (n = 6). Statistical differences between patients and healthy donors were compared using the Mann–Whitney U test. *Significant, P = 0.05; **very significant, P = 0.01; and ***highly significant, P = 0.001. MFI = mean fluorescent intensity.
Genetic Analysis
Genetic analysis was made by either of these two methods:
-
Genomic DNA was obtained from whole blood by the salting-out method. Next-generation sequencing analysis of primary immunodeficiency genes was performed using Invitae panel. This diagnostic test evaluated 528 genes for variants that were associated with primary immunodeficiency.
-
ITGB2 (CD18 gene) mutation analysis.8
-
Genomic DNA was obtained from Epstein-Barr virus (EBV)-B cell lines with DNAzol reagent (Life Technologies, Carlsbad, NM, USA).
-
Total RNA was extracted from peripheral blood mononuclear cells with TriZOL reagent (Life Technologies) and copy DNA (cDNA) converted (SuperScript® III RT; Life Technologies). ITGB2 gene was amplified with primers spanning complete coding sequence and from genomic DNA with primers spanning exon 7.
-
The products were sequenced with ABI PRISM® Big Dye® Terminator v3.1 cycle sequencing kit (Applied Biosystems, MA, USA) according to the manufacturer instructions.
-
A search for pathogenic variants was carried out in databases (Franklin—Genoox, Varsome, and Genomenon) for predicting pathogenicity.
Statistical analysis
Statistical analysis was performed using GraphPad Prism, version 5.0 (GraphPad Software Inc., La Jolla, CA, USA). For the expression of CD18 and CD11b, the two-group comparisons were performed using the Mann–Whitney test. The results of leukocyte populations were expressed as mean value of the highest and lowest value ranges of leukocytes. P < 0.05 was considered statistically significant.
Results
Clinical and demographic data of LAD-1 patients
We report the clinical manifestations and immunological findings of six Mexican patients diagnosed with LAD-1; five were females. Age of patients at diagnosis ranged from 1 to 10 months, with onset of symptoms occurring in the first 2 weeks. The summary of clinical and demographic features of the patients is shown in Table 1.11,12 Leukocyte count is shown in Table 2.
Table 1 Clinical and demographic characteristics of patients with LAD-1.
| P1 | P2 | P3 | P4 | P5 | P6 | |
|---|---|---|---|---|---|---|
| Gender | M | F | F | F | F | F |
| Symptomatic age | 3 days | 2 months | 7 days | 9 days | 6 days | 6 days |
| Age at diagnosis | 10 months | 7 months | 5 months | 7 months | 1 month | 1 month |
| Parental consanguinity | - | - | - | + | - | - |
| Delayed umbilical cord separation | - | + | + | + | - | - |
| Superficial organ abscess | + | + | + | - | + | + |
| Deep organ abscess | - | - | + | - | - | - |
| Omphalitis | + | + | + | + | + | - |
| Diarrhea | + | - | + | - | - | - |
| Infections | Omphalitis, cytomegalovirus infection, pneumonia, urinary tract infection, gastroenteritis and sepsis | Acute otitis media | Pneumonía, otitis media, sepsis abdominal | Health care associated pneumonia and abdominal wall cellulitis in treatment | Late-onset neonatal sepsis, necrotizing enterocolitis | Late-onset neonatal sepsis, necrotizing enterocolitis |
| Hepatosplenomegaly or hepatomegaly | - | + | + | - | + | + |
| Immunoglobulins (mg/dL) | IgG 461, IgM 48.8, IgA 71.7 | IgG: 1500, IgM: 270, IgA: 119 | IgG 1380, IgA 109, IgM 360 | IgG 1510, IgM 146, IgA 212 | NA | NA |
| Microbiological isolates | E. coli multidrug-resistant, Stenotrophomona maltophilia (central venous catheter) | Klebsiella oxytoca | Acinetobacter baumannii, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Klebsiella oxytoca | E. coli, Candida albicans | NA | Enterobacter aerogenes |
NA= not available.
Table 2 Leukocytes count in six Mexican patients with LAD-1.
| Cell type | Mean (×109/L) | Range (×109/L) | Reference values |
|---|---|---|---|
| Leukocytes | 28.6** | 12–54 | 6.0–17.5 |
| Neutrophils | 21.2** | 6.2–48.6 | 1.5–6.9 |
| Monocytes | 1.49** | 0.83–3.24 | 0.15–1.28 |
| Lymphocytes | 4.46 | 1.08–7.69 | 3.4–7.6 |
| CD3+ | 3.04 | 0.83–5.45 | 2.5–5.5 |
| CD4+ | 2.12 | 0.56–3.63 | 1.6–4.0 |
| CD8+ | 0.80 | 0.15–1.80 | 0.56–1.70 |
| *CD19+ | 0.6 | 0.07–1.3 | 0.3–2.0 |
| *CD16+ + CD56+ | 0.34 | 0.2–0.48 | 0.17–1.10 |
*One case was not measured (n = 5).
**Out of range.
LAD: leukocyte adhesion deficiency.
Case 1
Clinical manifestations in 10-month-old male infant began 3 days after birth with severe omphalitis and necrosis at the infection site (Figure 2A), where Escherichia coli multidrug-resistant was isolated, with no response to treatment. Debridement was performed and granulocyte colony--stimulating factor and subcutaneous gamma globulin were administered around the wound with total remission. The patient required multiple admissions for cytomegalovirus infection, pneumonia, urinary tract infection, gastroenteritis, and sepsis treated with adequate evolution. Subsequently, the patient presented an autoimmune manifestation characterized by hemolytic anemia. An inborn error of immunity was suspected and immunophenotyping was performed by flow cytometry. T cells were elevated. Nearly no surface expression of CD18 or CD11b leukocytes could be found.
Figure 2 Cutaneous manifestations in Mexican patients with LAD-1. (A) Nonhealing wound in the umbilical area; (B) congenital umbilical hernia and omphalitis; (C) posterior thorax ulcer with isolation of Pseudomonas aeruginosa; and (D) dehiscence at the surgical sites and poor wound healing.
Diagnosis of LAD-1 was confirmed with whole exome sequencing finding a c.817G>A nucleotide substitution in exon 7 of ITGB2 gene. We sequenced the coding exonic regions of CD18 gene (ITGB2) in cDNA prepared from the patient’s peripheral blood mononuclear cells (PBMCs), finding a homozygous nucleotide substitution in exon 7 of ITGB2 gene (c.817G>A). This variant was confirmed by the sequencing of exon 7 of ITGB2 in patient’s genomic DNA (gDNA). Three HSCTs were performed, but with graft rejection. At the age of 2 years, after myeloablative conditioning based on cyclophosphamide and busulfan, the patient received umbilical cord blood (UCB) infusion with a total CD34+ of CD34 4.4×105, without evidence of engraftment. During the aplastic phase, the patient has central line infection and acute otitis media, which could be the reason of primary graft failure. A maternal haploidentical cells infusion with post-transplant cyclophosphamide depletion was performed at the age of 3 years. The patient received reduced conditioning regimen based on radiotherapy, fludarabine, and cyclophosphamide, was given cyclophosphamide for graft versus host disease (GvHD); total dose of infusion cell was CD34+ 15×106/kg, engraftment was documented on day 11 with unstable chimera. Unfortunately, the patient experienced the secondary graft failure. Third attempt with UCB transplant was performed at the age of 4 years, conditioning regimen was with total body radiotherapy, fludarabine, and cyclophosphamide. However, the patient died 3 days after infusion (CD34+ 3.4×105/kg) because of septic shock.
Case 2
A 6-month baby girl was admitted due to a delayed umbilical cord separation. She had a history of eczema at 2 months and perforated tympanic membrane because of otitis media at 4 months. Her physical examination revealed hepatosplenomegaly and a visual ulcerative lesion at umbilical scar. Laboratory tests reported microcytic hypochromic anemia and leukocytosis. Immunophenotyping by flow cytometry showed no surface expression of CD18 or CD11b leukocytes, corroborating the diagnosis of LAD-1. A paternal haploidentical HSCT was performed at 18 months of age, with alpha/beta CD19+. A reduced conditioning regimen with anti-thymocyte globulin, fludarabine, and melphalan was imparted. She died 10 days after transplantation because of infections.
Case 3
A 1-week-old female, with a history of consanguinity, had omphalitis, delayed umbilical healing, failure to thrive, hepatosplenomegaly, and abdominal sepsis. She developed pericarditis and stye in her left eye. She also presented recurrent episodes of bacterial pneumonia and bilateral suppurative otitis media complicated with secondary conductive hearing loss. Acinetobacter baumannii and Klebsiella pneumoniae were isolated from ear secretions and urine culture, respectively. Other isolation of pathogenic germs included Pseudomonas aeruginosa in stool culture and Klebsiella oxytoca in vaginal secretion. Intestinal ischemia was diagnosed, and intestinal resection was performed with placement of a colostomy tube. She developed peristomatitis and an abdominal wall abscess.
Treatment with antibiotics and perilesional gamma globulin was successful. Bacillus licheniformis was found in catheter blood culture, and later gingivitis was analyzed. Flow cytometry reported very low expression of CD11b and CD18. HSCT using stem cells from UCB was performed at 18 months of age; myeloablative conditioning with anti-thymocyte globulin, busulfan and cyclophosphamide was applied. Infusion of CD34+ 3×106/kg body weight of receptor was performed from an all identical UCB and received cyclosporine for GvHD prophylaxis. Her parents declined second transplant, and the patient was referred to palliative care.
Case 4
A 2-week-old female infant with a history of inbreeding had omphalitis with leukocytosis and neutrophilia. She presented with congenital umbilical hernia (Figure 2B), Heallthcare-associated pneumonia and she coursed with intertrigo by candidiasis, vulvar cellulitis, and Escherichia coli was isolated from umbilical secretion. In addition, Candida albicans was found in urine culture and she had a history of suppurative otitis media. High-resolution lung computed tomography (CT) revealed a ground-glass interstitial pattern image and sub-pleural cysts in the posterior lobes. She coursed with data suggestive of pulmonary vasculitis. Anti-neutrophil cytoplasmic antibodies (ANCA) were reported positive. Immunophenotyping by flow cytometry showed no surface expression of CD18 or CD11b leukocytes, corroborating the diagnosis of LAD-1. The patient did not receive HSCT as decided by her parents, and she died at home.
Case 5
A 1-year-old female infant, born from consanguineous parents, presented with dermatosis of nonspecific evolution on the face, predominantly in the right eye with a cold granuloma. A biopsy was performed and mild hyperpigmentation in the epidermis was reported. The dermis showed mild diffused fibrosis; no infectious microorganisms were identified.
At 18 months, she was diagnosed with persistent ductus arteriosus; clinical management was unsuccessful and surgical treatment was performed. The patient presented poor wound healing in the posterior thorax (Figure 2C). Pseudomonas aeruginosa was isolated on surgical site. Laboratory tests revealed moderate leukocytosis with neutrophil predominance. Flow cytometry analysis showed low levels of CD11b and CD18. The patient did not receive HSCT and she died because of pneumonia and fulminant sepsis.
Case 6
A 48-day-old female infant, born from nonconsanguineous parents, started on the sixth day of life with persistent fever. She was admitted for late neonatal sepsis. She was diagnosed with necrotizing enterocolitis, and, subsequently, she underwent intestinal resection, and a colostomy was performed. She presented dehiscence at the surgical site and poor wound healing (Figure 2D). Treatment with antibiotics and perilesional gamma globulin was successful. CBC revealed leukocytosis with neutrophil predominance. Flow cytometry analysis showed low numbers of CD11b and CD18. Invitae primary immunodeficiency panel reported a homozygous variant in ITGB2 gene c.295del (p.Ser99Profs*5). She was diagnosed with LAD-1, and died 15 days later due to infectious complications.
LAD-1 patients with irregular count numbers in their leukocyte populations and very low expression of CD18/CD11b proteins
The number of different cell populations of patients was evaluated in peripheral blood. As shown in Table 2, the absolute counts of leukocytes were high in total leukocytes, neutrophils, and monocytes, outside reference values. The total lymphocytes population was normal, within reference values. To evaluate the expression of CD18 and CD11c, staining was analyzed in a region of neutrophils and monocytes (Figure 1A). The expression of CD18 and CD11c was null in both neutrophils and monocytes, as seen in Figure 1A–1E. The expression of CD18 in six patients was significantly lower, compared to healthy controls (n = 6), in both neutrophils and monocytes (P = 0.0043 and 0.050, respectively). The expression of CD11c in four patients was significantly lower, compared to healthy controls (n = 4), in both neutrophils and monocytes (P = 0.0260 and 0.0286, respectively; Figure 1F–1I).
Discussion
Leukocyte adhesion deficiency type 1 was first described in 1979 by Hayward et al. as a separate entity among immunodeficiencies.13 Approximately 300 patients with LAD-1 have been reported globally up to 2022.14 We analyzed six patients with LAD-1 in Mexican population during 2011–2023. Recurrent, severe, and difficult-to-treat bacterial infections were the predominant clinical manifestations of these patients. Infections usually appear first in the neonatal period as omphalitis and umbilical delayed detachment. Kambli et al.15 reported delayed umbilical cord separation in only 66% of patients. Three of the six patients (50%) in our study presented delayed separation of umbilical cord. This clinical manifestation is not pathognomonic of LAD-1, but it should be suspected in patients who present it, since it is described in all case reports.5,15,16
Although autoimmune manifestations in patients with LAD-1 have been reported in adolescence or after HSCT,17 in our study we found these manifestations in one-third of the cases (n = 2) but at younger ages and without having undergone HSCT. One patient presented autoimmune hemolytic anemia that had already been reported,8 and the other presented with ANCA-positive pulmonary vasculitis. This manifestation has never been described before. Interestingly, it has been shown that CD11c expression in monocytes is decreased in patients with ANCA-associated vasculitis.18 Hence, it is important to measure this marker in patients with suspected LAD-1, especially in those with autoimmune manifestations, such as vasculitis. These autoimmune manifestations could be associated with the fact that the circulating primed neutrophils and monocytes express ANCA-antigens on the cell surface. The primed neutrophils and monocytes, adhered to the endothelium, are then activated by ANCA and release reactive oxygen radicals and lysosomal enzymes, which lead to endothelial cell injury and eventually to necrotizing inflammation.19
In 2022, Kambli et al. reported a multicenter cohort that included 106 patients with LAD-1.15 The mean white blood count (WBC) was 57×109/L (range: 16.5–167×109/L) and the mean of absolute neutrophil count (ANC) was 40×109/L (range: 11–136×109/L). In spite of the fact that our all patients had elevated WBC and ANC, we found a lower mean for these parameters, compared to this cohort study.
As described previously in Mexican population with LAD-1, we found Escherichia coli, Klebsiella pneumoniae, and cytomegalovirus infections.6,7,9,10 However, infections caused by Acinetobacter baumannii, Klebsiella oxytoca, Bacillus licheniformis, and Candida albicans have not been reported previously, even in the literature. Stenotrophomona maltophilia infection has been associated with immunocompromised posits, including certain inborn errors of immunity, but it has only been documented in one patient with LAD-1,20 so this is the second report in the literature. Fungal infections can occur in 20% of patients with LAD-1.3 We documented that fungal infections were present in 16% of our patients (n = 1).
Regarding treatment and based on our experience, subcutaneous administration of gamma globulin at infection sites has shown to improve healing and scarring processes in patients with LAD-1, as observed in the three patients, prescribed this treatment.8
Even though HSCT was possible in only three patients, the overall outcome in our study was 100% mortality. The rest did not have the clinical conditions to be subjected to HSCT.
Patients with LAD-1 undergoing HSCT have a 25% survival rate up to the age of 2 years.5 In this study, one patient with LAD-1 reached a survival age of 6 years after three HSCT. However, there are no accurate survival reports for LAD-1 patients.
Diagnosis of LAD-1 was based on typical clinical manifestations, combined with laboratory examination of leukocytosis, significant reduction or near absence of CD18 and its associated molecules CD11a, CD11b, and CD11c on leukocytes.21 Three different chains of the leukocyte integrin family (CD11a, CD11b, and CD11c) are dependent on one beta chain (CD18) for proper insertion into the cell membrane. Absence of functional CD11/CD18 integrins on leukocytes, particularly neutrophils, leads to their incapacity to adhere to the endothelium and migrate to infection sites.3,22
Leukocyte adhesion deficiency type 1 patients with the absence of beta 2 integrins succumb to infection early in life. We must consider leukocyte and neutrophil counts of patients presenting with a delayed detachment of umbilical cord, omphalitis, and severe infections. Additionally, the characterization of CD18 and CD11 levels by flow cytometry is essential for diagnosis. The expression of CD18/CD11 is accomplished by a surface staining of three colors. Staining with CD11b is performed because the enhanced adherence in response to neutrophil mediators was almost entirely dependent on leukocyte integrin, mainly CD11b, with a variable contribution from CD11a.23
Under conditions of endothelial activation, CD11a plays a major part, but all three members have a cooperative effect, hence CD11a or CD11c can also serve. There are reports where CD18/CD11 staining is performed with or without stimulus, but there are no significant differences in terms of expression;24 for this reason, we only stain under basal conditions. For CD18 staining, two clones were used (CD18 clone 7E4 IgG1 mouse Beckman Coulter and CD18 clone 6.7 IgG1 mouse BD). In two clones, expression in mean fluorescent intensity (MFI) did not show significant differences if standardized in healthy controls; for this reason, the two reagents were used with confidence. While CD11b was a single clone (BEARL IgG1 mouse; Beckman Coulter), which had a high expression as measured by MFI in healthy controls, our six patients presented a greatly decreased MFI of CD18 and CD11b, compared to healthy controls. Considering the isotype control, the expression of these integrins in neutrophils and monocytes of six patients was less than 2%, which correlated with their serious clinical manifestations.
The determination of expression of CD18 helped us to diagnose rapidly, but only two patients underwent the molecular study. We found two homozygous pathogenic variants in ITGB2 gene; variant c.295del (p.Ser99Profs*5) was not reported previously (Table 3).
Table 3 Pathogenic variants identified in ITGB2 gene in Mexican patients with LAD-1.
| Patient | Gene variant (cDNA) | Amino acid change | Nature of mutation | CD18 expression (%) | References |
|---|---|---|---|---|---|
| 1 | c.817G>A | p.Gly273Arg | Missense | 0.1 | Reported in Yaz et al.3; Yamazaki-Nakashimada et al.8 |
| 6 | c.295del | p.Ser99Profs*5 | Frameshift delins | 0.0 | New variant |
Conclusion
Leukocyte adhesion deficiency type 1 is a rare disease whose early identification based on clinical manifestations leads to a timely diagnosis. Patients with LAD-1 may present with atypical manifestations, making flow cytometry an indispensable tool to confirm the diagnosis. LAD-1 should be considered a diagnostic emergency in inborn error of immunity; without timely treatment, it results in mortality during the first few years of life. We presented the first report of patients with LAD-1 in a Latin American country.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
Elma Isela Fuentes-Lara is a beneficiary student of the LASID-Takeda Fellowship Award program. Gabriel Emmanuel Arce-Estrada was a beneficiary of the National Scholarship Program for Graduate Studies by the National Council for Science and Technology (CONACYT) from 2022 to 2023. We thank to the Hospital Infantil de México Federico Gómez for their collaboration in referring patients to our research unit.
Author Contributions
E.I.F.-L. and L.B.-R. conceived with the idea of writing this publication. E.I.F.-L., G.E.A.-E., L.B.-R.and A.B.-C. wrote the abstract, introduction and methodology. E.I.F.-L., G.E.A.-E., L.B.-R., A.B.-C. and O.J.S.-R. created the tables, graphs and images. M.A.Y.-N., S.E.E.-P., L.B.G.-G. and R.M.N.R.-U. contributed to the recruitment of patients. E.I.F.-L., G.E.A.-E., L.B.-R., A.B.-C. and M.A.Y.-N. described the cases. L.B.-R. described the phenotype of the lymphocyte populations and performed the statistical analysis. M.A.Y.-N., S.E.E.-P., and L.B.G.-G. requested the tests for genetic analysis. All authors contributed to revising the manuscript, writing the discussion and conclusions.E.I.F.-L., G.E.A.-E., and A.B.-C. accommodated the references.
REFERENCES
1. Tangye SG, Al-Herz W, Bousfiha A, Cunningham-Rundles C, Franco JL, Holland SM, et al. Human inborn errors of immunity: 2022 Update on the classification from the International Union of Immunological Societies Expert Committee. J Clin Immunol. 2022 Oct 1;42(7):1473–507. 10.1007/s10875-022-01289-3
2. Sun B, Chen Q, Dong X, Liu D, Hou J, Wang W, et al. Report of a Chinese cohort with leukocyte adhesion deficiency-I and four novel mutations. J Clin Immunol. 2019;39:309–315. 10.1007/s10875-019-00617-4
3. Yaz I, Ozbek B, Bildik HN, Tan C, Oskay Halacli S, Soyak Aytekin E, et al. Clinical and laboratory findings in patients with leukocyte adhesion deficiency type I: A multicenter study in Turkey. Clin Exp Immunol. 2021 Oct 1;206(1):47–55. 10.1111/cei.13645
4. Cano Pedroza RY, Berrón Pérez L, Espinosa-Padilla SE. Deficiencia de adhesión de leucocitos. Alergia Asma Inmunol Pediát. 2022;31(1):21–6. 10.35366/104882
5. Almarza Novoa E, Kasbekar S, Thrasher AJ, Kohn DB, Sevilla J, Nguyen T, et al. Leukocyte adhesion deficiency-I: A comprehensive review of all published cases. J Allergy Clin Immunol Pract. 2018 Jul 1;6(4):1418–20.e10. 10.1016/j.jaip.2017.12.008
6. Olaya-Vargas, Alberto, Vollbrechausen-Castelán, Lilia, Corcuera-Delgado, Celso Tomás, & Scheffler-Mendoza, Selma. (2015). Paciente con deficiencia de adhesión leucocitaria tipo 1 y doble falla primaria de injerto. Acta pediátrica de México. 2015;36(6):473–79.
7. Harris ES, Smith TL, Springett GM, Weyrich AS, Zimmerman GA. Leukocyte adhesion deficiency-I variant syndrome (LAD-Iv, LAD-III): Molecular characterization of the defect in an index family. Am J Hematol. 2012;87:311–3. 10.1002/ajh.22253
8. Yamazaki-Nakashimada M, Maravillas-Montero JL, Berrón-Ruiz L, López-Ortega O, Ramírez-Alejo N, Acevedo-Ochoa E, et al. Successful adjunctive immunoglobulin treatment in patients affected by leukocyte adhesion deficiency type 1 (LAD-1). Immunol Res. 2015 Feb 22;61(3):260–8. 10.1007/s12026-014-8619-8
9. Quero-Hernández A, Zárate AR, Tenorio RH. Deficiencia en adhesión leucocitaria tipo I. Presentación de un caso y revisión de la literatura. Rev Mex Pediatr. 2007;74(2):80–83
10. García Gaitan ME. Deficiencia de la adhesión leucocitaria tipo I. Reporte Del Primer Caso en México y Revisión de la Literatura. Universidad Nacional Autnoma de México, Mexico, City, Mexico; 1996.
11. Picard C, Al-Herz W, Bousfiha A, Casanova JL, Chatila T, Conley ME, et al. Primary immunodeficiency diseases: An update on the classification from the International Union of Immunological Societies Expert Committee for Primary Immunodeficiency 2015. J Clin Immunol. 2015 Nov 1;35(8):696–726. 10.1007/s10875-015-0201-1
12. Shearer WT, Rosenblatt HM, Gelman RS, Oyomopito R, Plaeger S, Richard Stiehm E, et al. Basic and clinical immunology lymphocyte subsets in healthy children from birth through 18 years of age: The Pediatric AIDS Clinical Trials Group P1009 study [Internet]. [cited
13. Hayward AR, Leonard J, Wood CBS, Harvey BAM, Greenwood MC, Soothill JF. Delayed separation of the umbilical cord, widespread infections, and defective neutrophil mobility. Lancet. 1979 May 26;1(8126):1099–101. 10.1016/s0140-6736(79)91786-0
14. Geroldinger-Simić M, Lehner K, Klein G, Sepp N, Jabkowski J. An adult with severe leukocyte adhesion deficiency type 1. JAAD Case Rep. 2022 Jan 1;19:1–3. 10.1016/j.jdcr.2021.10.031
15. Kambli PM, Bargir UA, Yadav RM, Gupta MR, Dalvi AD, Hule G, et al. Clinical and genetic spectrum of a large cohort of patients with leukocyte adhesion deficiency type 1 and 3: A multicentric study from India. Front Immunol. 2020 Dec 16;11:612703. 10.3389/fimmu.2020.612703
16. Gorjipour H, Chavoshzadeh Z, Fahimzad A, Hashemitari P, Darougar S. Leukocyte adhesion deficiency type 1: A case series and review of the literature. Allergy Immunol. 2019;4(1): 95–100. 10.33590/emjallergyimmunol/10314214
17. De Rose DU, Giliani S, Notarangelo LD, Lougaris V, Lanfranchi A, Moratto D, et al. Long-term outcome of eight patients with type 1 leukocyte adhesion deficiency (LAD-1): Not only infections, but high risk of autoimmune complications. Clin Immunol. 2018 Jun 1;191:75–80. 10.1016/j.clim.2018.03.005
18. Matsumoto K, Kurasawa T, Yoshimoto K, Suzuki K, Takeuchi T. Identification of neutrophil β2-integrin LFA-1 as a potential mechanistic biomarker in ANCA-associated vasculitis via microarray and validation analyses. Arthritis Res Ther. 2021 Dec 1;23(1):136. 10.1186/s13075-021-02510-1
19. Takizawa M, Maguchi S, Nakamaru Y, Miyatake Y, Fukuda S, Inuyama Y. Correlation between the levels of circulating adhesion molecules and PR3-ANCA in Wegener’s granulomatosis [Internet]. [cited 2001]. Auris Nasus Larynx. 2001;28. Available at: www.elsevier.com/locate/anl. 10.1016/S0385-8146(01)00064-5
20. Strickler A, Gallo S, King A, Rosenzweig SD. Leucocyte adhesion deficiency type 1 with developmental delay secondary to CMV infection and filiation questions. BMJ Case Rep. 2015 Apr 9;bcr2014208973. 10.1136/bcr-2014-208973
21. Uzel G, Tng E, Rosenzweig SD, Hsu AP, Shaw JM, Horwitz ME, et al. Reversion mutations in patients with leukocyte adhesion deficiency type-1 (LAD-1) [Internet]. [cited 2008]. Available from: www.bloodjournal.org. 10.1182/blood-2007-04-082552
22. Kuijpers TW, Van Lier RAW, Hamann D, De Boer M, Yin Thung L, Weening RS, et al. Leukocyte adhesion deficiency type 1/variant: Dysfunctional 2 integrins leukocyte adhesion deficiency type 1 (LAD-1)/variant A novel immunodeficiency syndrome characterized by dysfunctional 2 integrins leukocyte adhesion deficiency • bleeding tendency • integ-rins • aggregation • chemotaxis [Internet]. [cited 1997]. J Clin Invest. 1997;100. 10.1172/JCI119697
23. Mazzone A, and Ricevuti G. Leukocyte CD11/CD18 integrins: biological and clinical relevance. Haematologica. 1995;80(2):161-175.
24. Kwon WK, Choi SI, Kim HJ, Huh HJ, Kang JM, Kim YJ, et al. Flow cytometry for the diagnosis of primary immunodeficiency diseases: A single center experience. Allergy Asthma Immunol Res. 2020 Mar 1;12(2):292–305. 10.4168/aair.2020.12.2.292