
Download
ORIGINAL ARTICLE
Safety of direct oral provocation test to delabel reported mild beta-lactam allergy in infants
Francisca Cunhaa*, Inês Cunhab, Eva Gomesb
aAllergy and Clinical Immunology Department, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal
bAllergy and Clinical Immunology Department, Centro Hospitalar e Universitário do Porto, Porto, Portugal
Abstract
Background: Around 10% of people report a drug allergy and avoid some medications because of fear of allergic reactions. However, only after a proper diagnostic workup can some of these reactions be confirmed as allergic or nonallergic hypersensitivities. Beta-lactams (BLs) are the most common medication suspected of being involved in drug hypersensivity reactions (DHRs) in children. Recently, direct oral provocation tests (DPT) with BLs gained popularity within pediatric populations as a tool for delabeling children with suspected BL allergies. This study aimed to evaluate the safety of direct provocation tests in infants with mild cutaneous non-immediate reactions to BLs.
Methods: The authors retrospectively analyzed the data of 151 infants between 2015 and 2022, referred for evaluating a suspected allergy to BLs that occurred before age 24 months.
Results: The mean age of the children, including 55% male kids, at the suspected reaction was 15.9 months and the mean age at the time of the DPT was 39.6 months. In most cases, antibiotics were prescribed to treat common upper respiratory infections, such as acute otitis (54.3%) and acute tonsillitis (27.2%). Amoxicillin was considered the culprit drug in 62.9% of the cases, and the combination of amoxicillin–clavulanic acid in the case of 33.8% of children. The most frequent associated cutaneous clinical manifestations were maculopapular exanthema in 74.8% and delayed urticaria/angioedema in 25.2%. Of the 151 infants evaluated, parents of 149 infants agreed for a direct DPT, and only three had a positive test (2%). Symptoms resulting from the DPT were mild and easily treatable.
Conclusions: A direct DPT without prior tests is a safe and effective procedure to delabel BL allergy, even in infants. The authors wish to emphasize the importance of properly validating BL allergy suspicions by promoting appropriate diagnostic procedures in infants as, in most cases, DHRs can be excluded and there is no need for further therapeutic restrictions.
Key words: Beta-Lactam Allergy, Drug Hypersensitivity, Drug Provocation Test, Infants
*Corresponding author: Francisca Cunha, Allergy and Clinical Immunology Department, Centro Hospitalar e Universitário de Coimbra, Praceta Prof. Mota Pinto, 3000-075 Coimbra, Portugal. Email address: [email protected]
Received 11 April 2023; Accepted 30 November 2023; Available online 1 March 2024
Copyright: Cunha F, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Drug hypersensitivity reactions (DHRs) consist of reproducible adverse effects of drugs that if taken at therapeutic doses, clinically mimic an allergy.1–3 Around 10% of people report drug allergy and avoid some medication because of the fear of inducing allergic reactions.4 Many suspicions arise during the early years of life and persist into adulthood with a substantial impact in clinical practice because of prescription constraints. However, only a diagnostic workup confirms whether these reactions are allergic or nonallergic hypersensitivities.5 In children, beta-lactams (BLs) antibiotics are the most common medications suspected of being involved in DHRs, with non-immediate skin eruptions being their most frequent presentations in the context of treating infections.4,6 Followed by BLs, nonsteroidal anti-inflammatory drugs (NSAIDs) and non-BL antibiotics are the most common medications involved to produce DHRs in this population.1 Despite being essential for evaluating a BL allergy, a detailed history cannot predict a drug allergy by itself. Not only blood allergy tests and skin tests (STs) have suboptimal sensitivity but they are also painful and difficult to perform in children. The drug provocation test (DPT) is considered as the most accurate diagnostic test because of its high positive predictive value and negative predictive value (PPV/NPV).7–10 In the case of mild reactions, after a careful clinical history and a DPT with the suspected drug, skipping other diagnostic tests has gained popularity for the delabeling of suspected BL allergies in pediatric populations.1,6,7
Aim
The purpose of this study was to describe the population of infants referred to a specialized drug allergy clinic of a tertiary hospital, with suspected non-severe and non--immediate reactions, for evaluation of a BL allergy. We reported the results and safety of using a DPT protocol in this young age group.
Methods
This was a retrospective study (January 2015–July 2022) with collected data of 151 children who were referred for evaluation of a suspected BL allergy that occurred before the age of 24 months. The analyzed data included demographics, characteristics of the reaction, suspected drugs, and results of the performed investigation. Only children reporting non-immediate reactions were included, that is, the latency between drug intake or administration and the onset of symptoms was longer than 1 h to several hours.11,12 Patients who did not recall the timing of the reaction were excluded from the study. Other exclusion criteria were patients with suspected severe reactions, such as acute generalized exanthematous pustulosis (AGEP), Stevens–Johnson syndrome/toxic epidermal necrolysis, drug reactions with eosinophilia and systemic manifestations, and drug-mediated, organ-specific reactions; patients were also excluded from investigations if DPTs were contraindicated.13,14
Descriptive statistics included frequency and percentage of qualitative variables, and median and interquartile range or mean and standard deviation (SD) of numerical variables, according to the normality of the distribution.
Clinical History
The diagnostic investigation of suspected DHRs started by collecting a detailed clinical history, with the used protocol based on the one proposed by the European Academy of Allergy & Clinical Immunology (EAACI) Drug Allergy Interest Group and the European Network on Drug Allergy (ENDA) after it was translated to Portuguese.15,16 In anamneses, particular importance was given to the age at the time of reaction; the drug involved; the diagnosis; clinical manifestations reported during the suspected DHR; and the temporal correlation between its appearance and the administration of the suspected drug.
Drug provocation test
All tested patients reported mild cutaneous non-immediate reactions. After obtaining informed consent from parents/careers, the patients were administered diagnostic DPT with the suspected drug without previous tests. An age- and weight-adjusted dose of the suspected drug was administered according to the ENDA guidelines in a day hospital;13 the calculated dose was divided in three incremental doses that were administered at 60-min intervals, followed by a vigilance period of at least 2 h prior to medical discharge. In patients without any reaction from the first day of DPT, an extended DPT was performed. The drug was continuously administered at home on the following days, using standard doses, until the number of doses that reportedly triggered the reaction was achieved, that is, the days of drug continuation at home varied according to the timing of the suspected reaction (from 1 to 5 days).
Results
During the considered period, 151 children showed reported DHRs with mild cutaneous non-immediate reaction occurring prior to the age of 24 months, with a mean age at the reaction being 15.9 ± 5.6 months (minimum 5 months and maximum 24 months). The mean age at DPT was 39.6 ± 19.0 months, with the majority being male infants (55%). Regarding the reactive BL, amoxicillin reaction occurred in 95 (62.9%) of the cases; in 51 patients (33.8%), allergy was due to the combination of amoxicillin and clavulanic acid; and in 5 patients (3.3%), the suspected drug was cefuroxime. In 139 (92.0%) patients, the reaction was reported during the first course of antibiotic, with no previously known usage of the suspected drug. The drugs involved were prescribed for the following infections: 82 (54.3%) patients with acute otitis; 41 (27.2%) patients with acute tonsillitis; lower respiratory tract infections in 15 (9.9%) cases; urinary tract infections in 10 (6.6%) patients; and cutaneous infections in 3 (2%) cases. The reported cutaneous symptoms were maculopapular exanthema (MPE) in 113 (74.8%) patients and delayed urticarial/angioedema in 38 (25.2%) patients (Table 1). The mean period of appearance of symptoms was 4.7 ± 2.5 days of treatment (from the 1st day to the 10th day).
Table 1 Demographic data.
| Age of reaction (months) | |
|---|---|
| Mean ± SD | 15.9 ± 5.6 |
| Age of DPT (months) | |
| Mean ± SD | 39.6 ± 19.0 |
| Gender (n, %) | |
| Male | 83 (55%) |
| Female | 68 (45%) |
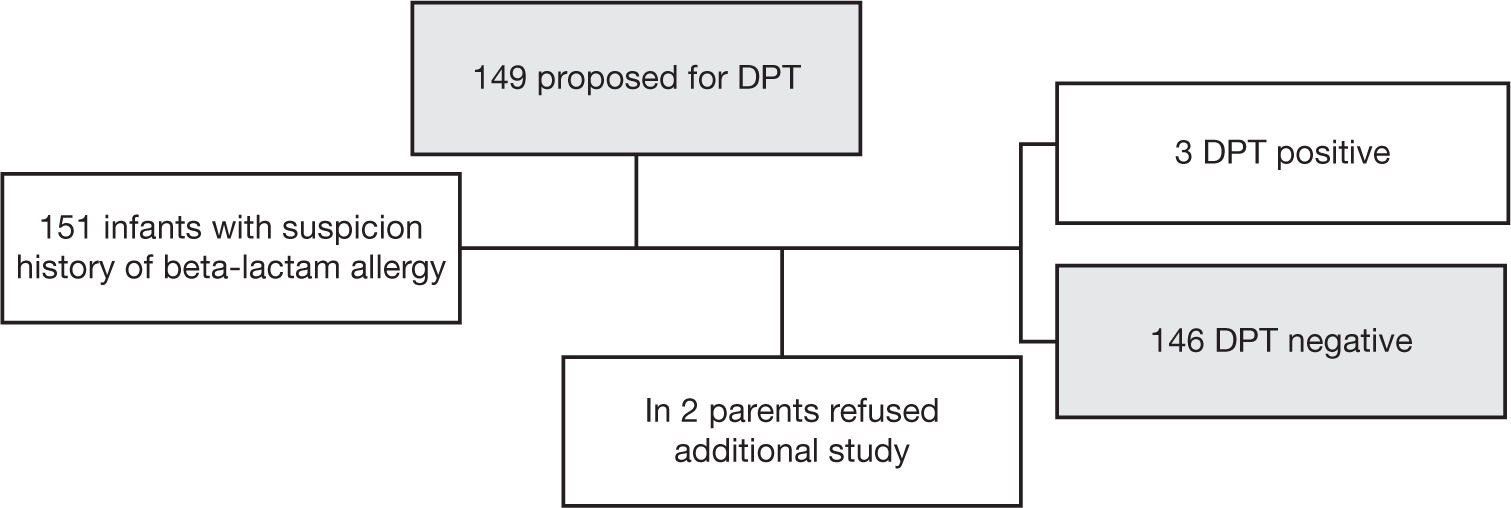
We had 151 eligible patients for direct DPT, but in case of two children, parents refused any additional studies. Of the 149 patients who completed the proposed diagnostic workup, we excluded the initial suspicion of BL allergy in 146 cases after a negative diagnostic provocation test (Figure 1). Hypersensitivity was documented by a positive DTP in three patients. Symptoms during the DPT were mild and similar to the initially described reactions; however, these appeared sooner than the initially reported reactions. In two patients, only antihistamines were used to treat reactions, but in others, antihistamines plus oral corticoids were used due to the presence of gastrointestinal symptoms, simultaneously with MPE (Table 2). Considering the negative 146 DPT results, the mean age at presentation of reaction was 15.3 ± 5.4 years. Amoxicillin was the main suspicious BL involved, and in 72.8% cases, the manifestation was MPE. The DPT was prolonged at home in 115 patients without reaction; however, among these, only three patients mentioned before showed reactions with the suspected BL.
Figure 1 Diagnostic flow chart.
Table 2 Characteristics of the population. reactions in the studied
| Diagnosis (n, %) | |
|---|---|
| Acute otitis | 82 (54.3%) |
| Acute tonsillitis | 41 (27.2%) |
| Others | 28 (18.5%) |
| Beta-lactams (n, %) | |
| Amoxicillin | 95 (62.9%) |
| Amoxicillin-clavulanic acid | 51 (33.8%) |
| Cefuroxime | 5 (3.3%) |
| Cutaneous Manifestations (n, %) | |
| Maculopapular exanthema | 113 (74.8%) |
| Urticaria/angioedema | 38 (25.2%) |
Table 3 Characteristics of infants with positive DPT.
| Gender | Male | Male | Male |
|---|---|---|---|
| Age of reaction | 17 | 12 | 18 |
| (years)* Reaction days |
4 | 5 | 2 |
| Manifestations | MPE | MPE | MPE |
| DPT | Amoxicillin | Amoxicillin | Amoxicillin/ |
| Clavulanic acid | |||
| Age of DPT (years)* | 38 | 61 | 40 |
| Day of DPT reaction | 2 | 1 | 1 |
| Manifestations | MPE | MPE + GI | MPE |
| symptoms |
*Months.
DPT: drug provocation test; GI: gastrointestinal; MPE: maculo- papular exanthema.
Discussion
Beta-lactams are the most prescribed and widely used antibiotics for treating common infections, particularly in children. Cutaneous manifestations occurring in this setting are caused by the underlying infections, but DHRs to antibiotics can trigger similar cutaneous manifestations, thus leading to diagnostic doubts. In children, such cutaneous manifestations are less commonly caused by BL hypersensitivity than in adults.17,18 In this study, we focused specifically on infants, reporting reactions before the age of 2 years. Suspected DHRs at such a young age can lead to unnecessary lifelong drug avoidance if reactions are not investigated properly.
Similar to other pediatric studies,19,20 the majority of patients who were referred to our specialized drug allergy clinic with a suspected BL allergy reported non-immediate mild cutaneous reactions, such as MPEs and urticarial exanthemas. These reactions are considered as being of low risk, particularly in children.9 Among the 149 patients administered DPT without prior diagnostic tests, only three had a positive provocation test (2%). According to the literature, positive DPT was observed in less than 10% of children.6,17,20,21
In a large study conducted by Zambonino et al., 783 children, with a median age of 6 years, were evaluated for both immediate and non-immediate DHRs to BL.22 The authors reported a confirmed allergy in 7.9% patients after a diagnostic work up, which included specific immunoglobulin E (IgE) determination, skin testing, and, if necessary, a DPT.19 In our study, we had a lower proportion of positive investigations, probably because of our population selection, that is, younger patients with only mild cutaneous non-immediate reactions that occurred before the age of 24 months. In fact, according to the literature, the probability to confirmed DHR increases with age as well as with the severity of the suspected reaction,15 being higher in the case of immediate reactions.22–24
Another large study conducted by Mill et al., comprising 818 children with a median age of 1.7 years, reported both immediate and non-immediate reactions to amoxicillin; the patients were administered direct DPT, and the proportion of positive aggravations was 5.9%.25 Despite the age of the included children being closer to those in our study, the authors considered all forms of immediate and non-immediate reactions and not only non-immediate reactions with mild cutaneous symptoms as done in the present study, which may explain the difference in confirmed diagnosis. Similar findings were reported in a study conducted by Exius et al., which included 1914 children (mean age of 1.8 years at the occurrence of reaction) with an history of benign skin reactions to amoxicillin (either immediate or non-immediate), and discovered a 5.4% positive DPT results to amoxicillin.26
In a recent study conducted by Prieto et al., addressing the utility of a single dose of DPT without any previous tests for diagnostic purposes in 194 children with mild non-immediate reactions, the proportion of positive tests was 12.4%.27 This prospective study included children aged 0–14 years, which may explain the difference in the number of confirmed reactions in our study. Interestingly, similar to our results, the authors also reported a decrease in the interval between drug administration and onset of symptoms observed in positive DPTs, compared to the original reaction. It also considered DPTs without previous skin tests a safe and useful means to assess mild non-immediate reactions in children.
A recent meta-analysis of DPT results in children with suspected hypersensivity to BL discovered that the overall prevalence of positive DPT in children with a history of mild non-immediate reactions was about 7%, and that no severe reactions occurred during DPT.28. In a recent meta-analysis done last year that included 28 studies, reporting on 8334 direct challenges, the estimated prevalence of BL hypersensitivity was 5.2% (3.7% non-immediate reactions); the frequency of severe reactions resulting from direct DPTs was very low, also supporting the idea that direct DPT is a safe and effective delabeling tool in children with suspected non-severe reactions.29
Our results demonstrated that if we only consider -clinical history, then drug allergy could be largely over diagnosed as reported by other authors,6 with a negative impact on both individual patients and public heath.30 The proportion of positive diagnosis was only 2%, which confirmed the proportion reported by other studies, considering that only children with mild cutaneous non-immediate reactions that occurred prior to the age of 2 years were included. Our data also supported the idea that in non--immediate mild cutaneous reactions, a direct DPT with the suspected drug was a safe and time-effective method to exclude false suspicions of drug hypersensitivity.7,28,30 For the diagnosis of non-immediate drug hypersensitivity, some guidelines still recommend the use of delayed-reading intradermal tests and patch tests.31,32 Nevertheless, the negative and positive predictive values of these tests in such reactions remained unclear.33,34 Thus, direct DPT with suspected drug gained popularity to study such reactions in the pediatric population in which the performance and acceptance of skin tests was challenging. In the three patients who had a documented DHR to BLs, symptoms during the DPT were mild and easily treated, though more precocious, which was in line with reports from other -studies.35,36 In fact, some working groups had included direct DPTs in their recommendations.1,31,37–40 The decision to prolong DPT at home is divergent between different studies; nevertheless, in our study, we accepted that extension had an important impact on delabeling, and was safe.
Regarding atopic background, we were not able to prove statistically the association between atopy and risk of a true drug allergy in our study. However, as recently described in the literature, it is important to highlight relationship between the presence of a positive personal and family history of atopy and an increased risk for a positive DPT.41
Regarding limitations of the present study, it was a retrospectively conducted analysis, which implied reviewing past records not intended for the purpose of the present investigation, and thus a possible recall bias by the parents about the index reaction could have happened.
In the present work, we verified a delay of 23.7 months between the age of index reaction and the age of direct DPT. As evident, sensitization loss is expected with progress in time, especially in the IgE-mediated reactions. This could be an influencing factor in delay between index reaction and work-up study. In our study, the main reaction was non-immediate reaction, attributed to a non--IgE-mediated mechanism, so the influence of such delay is not an expected relevant factor.
Owing to a highly selected studied population, considering age and clinical manifestations of the reaction, it was not possible to extrapolate data to other pediatric or adult populations or even other more complex DHRs.
Nevertheless, we considered this study as an important analysis, given the need to remove unverified BL allergy findings, especially in this age group, in which mild non--immediate cutaneous reactions were the main clinical presentations leading to a BL allergy suspicion. Such infants have an expected long life spam and would probably require these antibiotics throughout their lives. Besides, the probability of the diagnosis confirmation is quite low, making this population a prime target for BL allergy delabeling. This approach with the use of a direct DPT is more justified in infants as cooperation and acceptance of invasive diagnostic procedures. The blood allergy tests and skin tests are suboptimal and have poor diagnostic value.
Conclusion
Our work adds to the current knowledge, showing that the vast majority of pediatric patients with suspected allergy to BLs cannot be confirmed as having a true allergy upon a diagnostic investigation.41 Recent studies increasingly support the use of direct DPTs as a tool to delabel pediatric patients with suspected allergy to BLs, especially in the case of mild non-immediate reactions. We found this approach as safe and effective within the infant population. We emphasize the importance of properly validating DHRs’ suspicions in infants, as in most cases they can be excluded and there is no need for therapeutic restrictions to perpetuate to adulthood. Multi-centric studies and consensus for applying diagnostic protocols are needed to enable the vast use of such diagnostic approaches in delabeling BL allergy in this particular population.
Conflict of interest
The authors have no conflicts of interest to declare.
Declaration
The authors declare that this retrospective study has not been previously published, and isn’t being considered for publication elsewhere. Written and oral informed consents from the children’s parents were properly obtained.
Financial support
The authors did not have any financial support while carrying out this work.
REFERENCES
1. Gomes ER, Brockow K, Kuyucu S, Saretta F, Mori F, Blanca-Lopez N, et al. Drug hypersensitivity in children: Report from the pediatric task force of the EAACI Drug Allergy Interest Group. Allergy Eur J Allergy Clin Immunol. 2016;71(2):149–61. (Blackwell) 10.1111/all.12774
2. Pichler WJ. Immune pathomechanism and classification of drug hypersensitivity. Allergy Eur J Allergy Clin Immunol. 2019;74(8):1457–71. (Blackwell) 10.1111/all.13765
3. Pichler WJ Hausmann O. Classification of drug hypersensitivity into allergic, p-i, and pseudo-allergic forms. Int Arch Allergy Immunol. 2017;171(3–4):166–79. 10.1159/000453265
4. Sousa-Pinto B, Fonseca JA, Gomes ER Frequency of self--reported drug allergy: A systematic review and meta-analysis with meta-regression. Ann Allergy Asthma Immunol. 2017;119(4):362–73.e2. 10.1016/j.anai.2017.07.009
5. Warrington R, Silviu-Dan F. Drug allergy. Allergy Asthma Clin Immunol. 2011;7(S1):S10. 10.1186/1710-1492-7-S1-S10
6. Vezir E, Dibek Misirlioglu E, Civelek E, Capanoglu M, Guvenir H, Ginis T, et al. Direct oral provocation tests in non--immediate mild cutaneous reactions related to beta--lactam antibiotics. Pediatr Allergy Immunol. 2016;27(1):50–4. 10.1111/pai.12493
7. Prosty C, Copaescu AM, Gabrielli S, Mule P, Ben-Shoshan M. Pediatric drug allergy. Immunol Allergy Clin North Am. 2022;42(2):433–52. 10.1016/j.iac.2022.01.001
8. Blanca-Lopez N, Atanaskovic-Markovic M, Gomes ER, Kidon M, Kuyucu S, Mori F, et al. An EAACI task force report on allergy to beta-lactams in children: Clinical entities and diagnostic procedures. Pediatr Allergy Immunol. 2021;32(7):1426–36. 10.1111/pai.13529
9. Felix MMR, Kuschnir FC. Direct oral provocation test is safe and effective in diagnosing beta-lactam allergy in low-risk children with mild cutaneous reactions. Front Pharmacol. 2020;11:1223. 10.3389/fphar.2020.01223
10. Moral L, Caubet J-C. Oral challenge without skin tests in children with non-severe beta-lactam hypersensitivity: Time to change the paradigm? Pediatr Allergy Immunol. 2017;28:724–7. 10.1111/pai.12800
11. Romano A, Torres MJ, Castells M, Sanz ML, Blanca M. Diagnosis and management of drug hypersensitivity reactions. J Allergy Clin Immunol. 2011;127(3 Suppl):S67–73. 10.1016/j.jaci.2010.11.047
12. Romano A, Atanaskovic-Markovic M, Barbaud A, Bircher AJ, Brockow K, Caubet JC, et al. Towards a more precise diagnosis of hypersensitivity to beta-lactams—An EAACI position paper. Allergy Eur J Allergy Clin Immunol. 2020;75(6):1300–15. 10.1111/all.14122
13. Aberer W, Bircher A, Romano A, Blanca M, Campi P, Fernandez J, et al. Drug provocation testing in the diagnosis of drug hypersensitivity reactions: General considerations. Allergy Eur J Allergy Clin Immunol. 2003;58(9):854–63. 10.1034/j.1398-9995.2003.00279.x
14. Bousquet P-J, Gaeta F, Bousquet-Rouanet L, Lefrant J-Y, Demoly P, Romano A. Provocation tests in diagnosing drug hypersensitivity. Curr Pharm Design. 2008;14(27):2792-802. 10.2174/138161208786369731
15. Demoly P, Kropf R, Bircher A, Pichler WJ. Drug hypersensitivity: Questionnaire. EAACI interest group on drug hypersensitivity. Allergy. 1999 Sep 54(9):999–1003. 10.1034/j.1398-9995.1999.00247.x
16. Gomes ER, Falcão H. Hipersensibilidade a fármacos: Questionário. Rev Port Imunoalergologia. 2001;8:231–2.
17. Bierman CW, Pierson WE, Zeitz SJ, Hoffman LS, Vanarsdel PP. Reactions associated with ampicillin therapy. JAMA. 1972 May 22;220(8):1098–100. http://jama.jamanetwork.com/
18. Rebelo Gomes E, Fonseca J, Araujo L, Demoly P. Drug allergy claims in children: From self-reporting to confirmed diagnosis. Clin Exp Allergy. 2008;38(1):191–8. 10.1111/j.1365-2222.2007.02870.x
19. Rubio M, Bousquet PJ, Gomes E, Romano A, Demoly P. Results of drug hypersensitivity evaluations in a large group of children and adults. Clin Exp Allergy. 2012;42(1):123–30. 10.1111/j.1365-2222.2011.03887.x
20. Iammatteo M, Alvarez Arango S, Ferastraoaru D, Akbar N, Lee AY, Cohen HW, et al. Safety and outcomes of oral graded challenges to amoxicillin without prior skin testing. J Allergy Clin Immunol Pract. 2019;7(1):236–43. 10.1016/j.jaip.2018.05.008
21. Felix MMR, Kuschnir FC. Direct oral provocation test is safe and effective in diagnosing beta-lactam allergy in low-risk children with mild cutaneous reactions. Front Pharmacol. 2020 Aug 7;11:1223. 10.3389/fphar.2020.01223
22. Zambonino MA, Corzo JL, Muñoz C, Requena G, Ariza A, Mayorga C, et al. Diagnostic evaluation of hypersensitivity reactions to beta-lactam antibiotics in a large population of children. Pediat Allergy Immunol. 2014;25(1):80–7. 10.1111/pai.1215
23. Mirakian R, Leech SC, Krishna MT, Richter AG, Huber PAJ, Farooque S, et al. Management of allergy to penicillins and other beta-lactams. Clin Exp Allergy. 2015;45(2):300–27. 10.1111/cea.12468
24. Böhm R, Proksch E, Schwarz T, Cascorbi I. Drug hypersensitivity—-Diagnosis, genetics and prevention. Dtsch Arztebl Int. 2018;115:501–12. 10.3238/arztebl.2018.0501
25. Mill C, Primeau MN, Medoff E, Lejtenyi C, Keefe AO, Netchiporouk E, et al. Assessing the diagnostic properties of a graded oral provocation challenge for the diagnosis of immediate and non-immediate reactions to amoxicillin in children. JAMA Pediatr. 2016;170(6):e160033. 10.1001/jamapediatrics.2016.0033
26. Exius R, Gabrielli S, Abrams EM, O’Keefe A, Protudjer JLP, Lavine E, et al. Establishing amoxicillin allergy in children through direct graded oral challenge (GOC): Evaluating risk factors for positive challenges, safety, and risk of cross-reactivity to cephalosporines. J Allergy Clin Immunol Pract. 2021;9(11):4060–66. 10.1016/j.jaip.2021.06.057
27. Prieto A, Muñoz C, Bogas G, Fernández-Santamaría R, Palomares F, Mayorga C, et al. Single-dose prolonged drug provocation test, without previous skin testing, is safe for diagnosing children with mild non-immediate reactions to beta-lactams. Allergy Eur J Allergy Clin Immunol. 2021;76(8):2544–54. 10.1111/all.14800
28. Kuniyoshi Y, Tsujimoto Y, Banno M, Taito S, Ariie T, Kubota T, et al. Beta-lactam allergy and drug challenge test in children: A systematic review and meta-analysis. Pediat Res. 2023;93(1):22–30. 10.1038/s41390-022-02076-x
29. Srisuwatchari W, Phinyo P, Chiriac AM, Saokaew S, Kulalert P. The safety of the direct drug provocation test in beta lactam hypersensitivity in children: A systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2023;11(2):506–18. 10.1016/j.jaip.2022.11.035
30. Lee CE, Zembower TR, Fotis MA, Postelnick MJ, Greenberger PA, Peterson LR, et al. The incidence of antimicrobial allergies in hospitalized patients: Implications regarding prescribing patterns and emerging bacterial resistance. Arch Intern Med. 2000 Oct 9;160(18):2819–22. 10.1001/archinte.160.18.2819
31. Koosakulchai V, Sangsupawanich P, Wantanaset D, Jessadapakorn W, Jongvilaikasem P, Yuenyongviwat A. Safety of direct oral provocation testing using the-amoxicillin-2-step-challenge in children with history of non-immediate reactions to amoxicillin. World Allergy Organ J. 2021;14(7):100560. 10.1016/j.waojou.2021.100560
32. Arıkoğlu T, Kuyucu S, Caubet JC. New diagnostıc perspectives in the management of pediatrıc beta-lactam allergy. Pediat Allergy Immunol. 2022;33(3):e13745. 10.1111/pai.13745
33. Pongracic JA, Bock SA, Sicherer SH. Oral food challenge practices among allergists in the United States. J Allergy Clin Immunol. 2012;129(2):564–6. 10.1016/j.jaci.2011.09.024
34. Lezmi G, Alrowaishdi F, Bados-Albiero A, Scheinmann P, de Blic J, Ponvert C. Non-immediate-reading skin tests and prolonged challenges in non-immediate hypersensitivity to beta-lactams in children. Pediat Allergy Immunol. 2018;29(1):84–89. 10.1111/pai.12826
35. Romano A, Blanca M, Torres MJ, Bircher A, Aberer W, Brockow K, et al. Diagnosis of non-immediate reactions to β-lactam antibiotics. Allergy Eur J Allergy Clin Immunol. 2004;59(11):1153–60. 10.1111/j.1398-9995.2004.00678.x
36. Padial A, Antunez C, Blanca-Lopez N, Fernandez, TD, Cornejo-Garcia JA, Mayorga C, et al. Non-immediate reactions to β-lactams: Diagnostic value of skin testing and drug provocation test. Clin Exp Allergy. 2008;38(5):822–8. 10.1111/j.1365-2222.2008.02961.x
37. Kuruvilla M, Shih J, Patel K, Scanlon N. Direct oral amoxicillin challenge without preliminary skin testing in adult patients with allergy and at low risk with reported penicillin allergy. Allergy Asthma Proc. 2019;40(1):57–61. 10.2500/aap.2019.40.4184
38. Atakul G, Köse SS, Atay O, Boyacioglu OK, Al S. Asilsoy S, et al. Oral challenge without penicillin skin tests in children with suspected beta-lactam hypersensitivity. J Child Sci. 2022;12(1):E133–7. 10.1055/s-0042-1757151
39. Chiriac AM, Demoly P. Drug provocation tests: Up-date and novel approaches. Allergy Asthma Clin Immunol. 2013;9(1):12. 10.1186/1710-1492-9-12
40. Torres MJ, Adkinson NF, Caubet JC, Khan DA, Kidon MI, Mendelson L, et al. Controversies in drug allergy: Beta-lactam hypersensitivity testing. J Allergy Clin Immunol Pract. 2019;7(1):40–45. 10.1016/j.jaip.2018.07.051
41. Kitsos N, Cassimos D, Trypsianis G, Xinias I, Roilides E, Grivea I, et al. Drug allergy evaluation in children with suspected mild antibiotic allergy. Front Allergy. 2022;3:1050048. 10.3389/falgy.2022.1050048