
Download
ORIGINAL ARTICLE
Time effect of dupilumab to treat severe uncontrolled asthma in adolescents: A pilot study
Cristiana Indolfia, Giulio Dinardoa*, Angela Klaina, Marcella Contieria, Giuseppina Rosaria Umanoa, Alberto Decimoa, Giorgio Ciprandib, Michele Miraglia del Giudicea
aDepartment of Woman, Child and General and Specialized Surgery, University of Campania Luigi Vanvitelli, Naples, Italy
bAllergy Clinic, Casa di Cura Villa Montallegro, Genoa, Italy
Abstract
Background: Dupilumab is a new biological drug approved for the treatment of type 2 inflammatory diseases, such as asthma. Dupilumab is a fully humanized monoclonal antibody that acts against both interleukin-4 and interleukin-13 receptors. This study evaluated the time--dependent effect of dupilumab on asthma exacerbations and quality of life in adolescents with uncontrolled severe asthma.
Materials and Methods: Five adolescents suffering from uncontrolled severe asthma and treated with dupilumab were recruited. All subjects were evaluated for 4, 12, and 24 weeks after the first dose of dupilumab. Outcome measures included lung function, fractional exhaled nitric oxide, asthma control and quality of life assessed by validated questionnaires (Asthma Control Test and Asthma Control Questionnaire).
Results: The quality of life improved quickly after 4 weeks of treatment and 80% of adolescents halved the dose of inhaled corticosteroids necessary to control asthma symptoms. These results were still maintained for 24 weeks after start of the therapy. None of the patients had any asthma exacerbation during the study period.
Conclusion: Results of this study demonstrated that dupilumab was quickly effective to reduce asthma exacerbation and ameliorate quality of life in severe asthmatic adolescents.
Key words: asthma, dupilumab, children, asthma control, quality of life
*Corresponding author: G. Dinardo, Department of Woman, Child and General and Specialized Surgery, University of Campania Luigi Vanvitelli, Street Luigi de Crecchio 4, 80024, Naples, Italy. Email address: [email protected]
Received 28 March 2023; Accepted 24 May 2023; Available online 1 September 2023
Copyright: Indolfi C, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Asthma is one of the most frequent chronic respiratory diseases in children and is often associated with other conditions, such as allergic rhinoconjunctivitis1,2 and atopic dermatitis.3,4
Biological drugs represent a therapeutic innovation that has revolutionized approach toward patients with severe asthma. ‘Severe asthma’ is the asthma that is uncontrolled despite adherence to maximal optimized high-dose inhaled corticosteroids (ICSs) and long-acting beta2-agonists (LABA) treatment and management of contributing factors, or the one that worsens when high-dose treatment is reduced.5–11 Prevalence of severe childhood asthma is estimated to be around 5% among patients with asthma. 12–17
According to the Global Initiative for Asthma (GINA) 2022 guidelines, in adolescents and children with severe uncontrolled asthma or requiring frequent or continuous use of oral corticosteroids (OCSs), which corresponds to step 5 of the guidelines, the addition of a biological drug could be considered.18,19 The lowering of OCS is a favorable outcome, because OCS can have both short- and long-term negative effects in children.20
Biological drugs currently available in Italy for severe childhood asthma are omalizumab, mepolizumab, and dupilumab, although only reslizumab is approved by European Medicine Agency (EMA).21 In Italy, dupilumab is approved by Agenzia Italiana del Farmaco (AIFA) for the treatment of asthma in adults and adolescents aged ≥12 years as an add-on maintenance treatment for severe asthma with type 2 inflammation. AIFA approved dupilumab for children aged ≥12 years having severe asthma with type 2 inflammation characterized by elevated blood eosinophils and/or elevated fractional exhaled nitric oxide (FeNO), and whose condition is not adequately controlled by medium to high doses of ICSs plus another medication as a maintenance treatment. Recently, AIFA approved dupilumab also for children aged ≥6 years.22
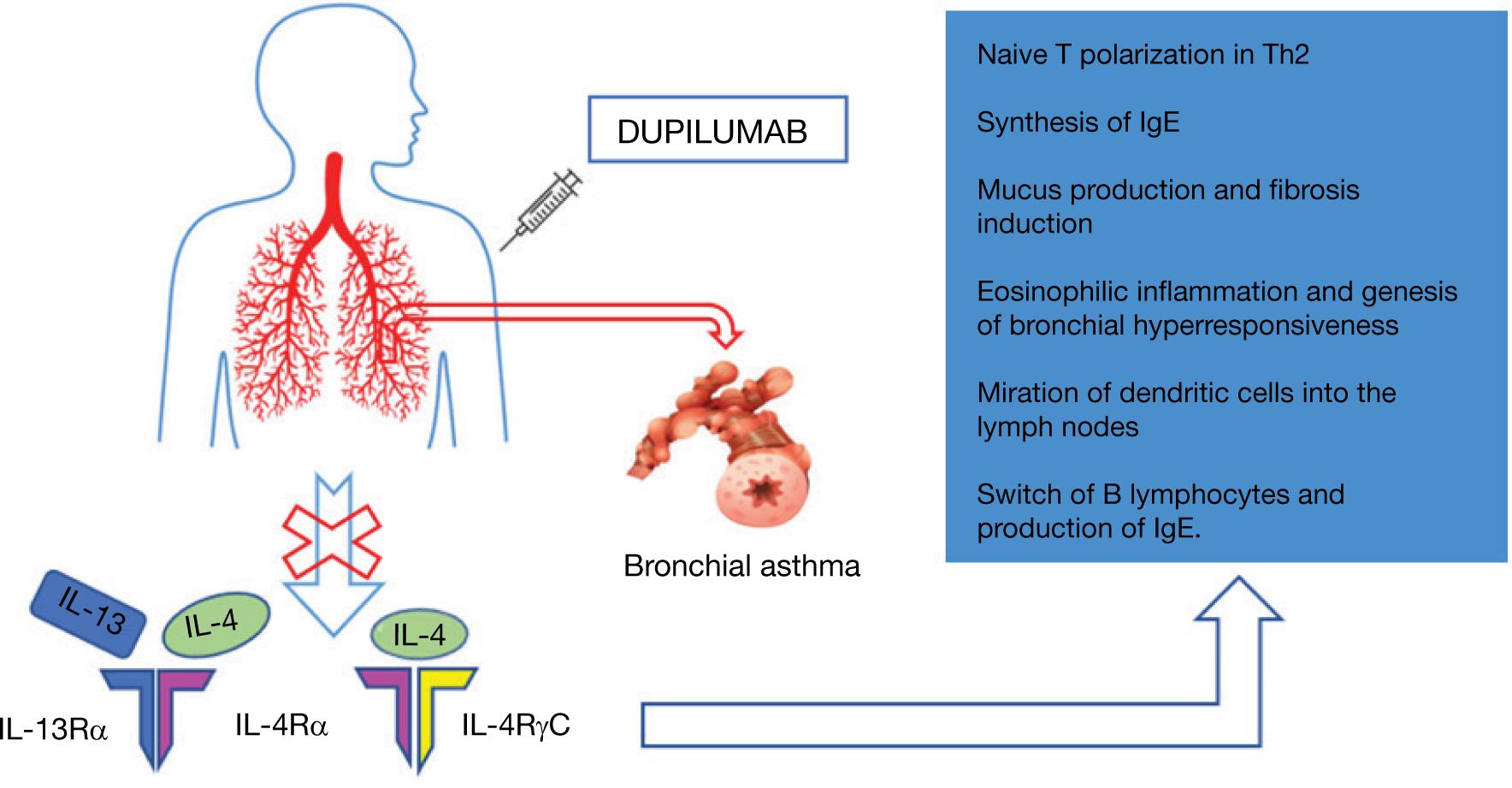
Dupilumab is a fully human monoclonal antibody that inhibits signal transduction of interleukin 4 (IL-4) through type I receptor IL-4Rα/γc, type II receptor IL-4Rα, and interleukin 13 (IL-13) through type II receptor IL-13Rα.23 IL-4 and IL-13 play a key role in the pathogenesis of helper T cell (Th2) diseases, either allergic or nonallergic, from sensitization toward environmental antigens to the maintenance of inflammation to bronchial remodeling. IL-4 is implicated in naïve T polarization in Th2 and in the synthesis of immunoglobulin E (IgE), while IL-13 has a specific role in mucus production and fibrosis induction. Both IL-4 and IL-13 influence eosinophilic inflammation and genesis of bronchial hyperresponsiveness. They also influence the collection of antigens by dendritic cells and their migration into lymph nodes, where they trigger differentiation of Th0 lymphocytes in Th2 disease in the presence of IL-4. IL-4 is also required for switching B lymphocytes and producing IgE.24,25 IL-4 and IL-13 act on R1 and R2 receptors. The R1 receptor is stimulated solely by IL-4 and is formed by two chains IL-4Rα/ϒc whereas receptor R2 is formed by two chains IL-4Rα/IL-13Rα1; therefore, both receptors have a common chain, IL4Rα (Figure 1).26,27
Figure 1 Mechanism of action of dupilumab.
Dupilumab is available as prefilled syringes for subcutaneous administration. The recommended regimen for teenagers aged 12–18 years with severe asthma and who are on OCSs, or for patients with severe asthma and having comorbid moderate-to-severe atopic dermatitis, or adults with comorbid severe chronic rhinosinusitis with nasal polyposis, is as follows: an initial dose of 600 mg (two 300-mg injections), followed by 300 mg every other week administered as subcutaneous injection. For all other patients, dupilumab regimen includes an initial dose of 400 mg (two 200-mg injections), followed by 200 mg every other week administered as subcutaneous injection.21,28
Controlling asthma is a key objective of asthma therapy. A quick and effective method for determining asthma control is to use a validated, standardized questionnaire.29 The efficacy of the Asthma Control Questionnaire (ACQ-7) and Asthma Control Test (ACT) has been assessed by several studies.29–31 Evidence suggests that ACT score closely correlates with ACQ score, lung function, asthma-related quality of life (QoL), rescue medication use, exacerbations, sleep quality, and work/school performance.32 Both ACQ-7 and ACT allow to classify significantly more patients as having uncontrolled asthma compared to the GINA criteria.33
The aim of the study was to evaluate the time--dependent effect of dupilumab on asthma exacerbations and QoL in adolescents with uncontrolled severe asthma.
Materials and Methods
Patients
We selected five adolescents suffering from uncontrolled severe asthma and treated with dupilumab. None of the enrolled patients had a history of previous use of biologic drugs. Age of the enrolled patients ranged from 12 to 18 years; all had asthma onset within the first 6 years of life and had sensitization to inhalant allergens, such as pollen or dust mites. All enrolled patients had high levels of peripheral eosinophilia (>150/mL and <1500/mL) and/or FeNO > 25 ppb. All enrolled patients had a clinical background characterized by severe asthma, with frequent exacerbations during the last year, and allergic rhinitis being treated with antihistamines and mometasone nasal spray. The subjects were treated with high doses of ICS combined with LABA and addition of montelukast.
Study Design
All the patients met eligibility criteria for starting treatment with dupilumab. Patient eligibility criteria included severe and frequent exacerbations during the last year of therapy, high levels of peripheral eosinophilia (>150/mL and <1500/mL) and/or FeNO > 25 ppb, and the need to use OCS for asthma control. Informed consent was obtained from all subjects involved in the study. Our study was a retrospective research conducted in accordance with the Declaration of Helsinki, and was approved by the Institutional Review Board (or Ethics Committee) of University of Campania “Luigi Vanvitelli.”
We conducted follow-up evaluations of patients who received dupilumab treatment at 4, 12, and 24 weeks after initiation of treatment. At each follow-up visit, we assessed asthma exacerbations, ICS dose, and asthma control using both ACT and ACQ-7. The ACT measures clinical symptoms, activity limitations, short-acting β2-agonist use, and airway narrowing. The ACQ-7 consists of seven items, which included five items for symptoms, one for rescue bronchodilator use, and one for forced expiratory volume in 1 s (Fev1% of predicted normal).
Study Endpoint
The endpoint of the study was to evaluate the time--dependent effect of dupilumab on asthma exacerbations and QoL in adolescents with uncontrolled severe asthma.
Statistical Analysis
For the construction of database and for the analysis of data, all continuous variables were tested for normality according to the Shapiro–Wilk test. Differences for not--normally distributed continuous variables were investigated by the Friedman test. Data were expressed as median and interquartile range (IQR). P < 0.05 was considered as statistically significant. All analyses were performed using GraphPad Prism version 8.0.2 for Windows (GraphPad Software, San Diego, CA, US).
Results
None of the subjects included in the study and followed had any asthma exacerbations after starting the treatment.
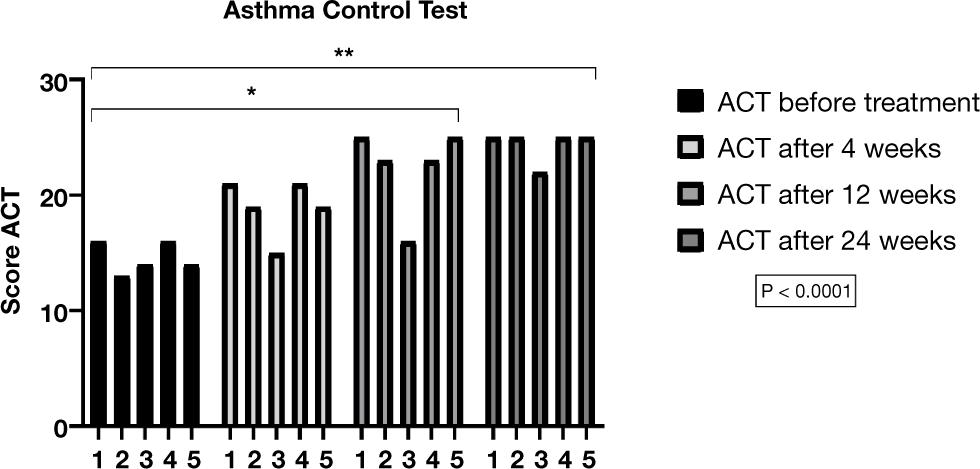
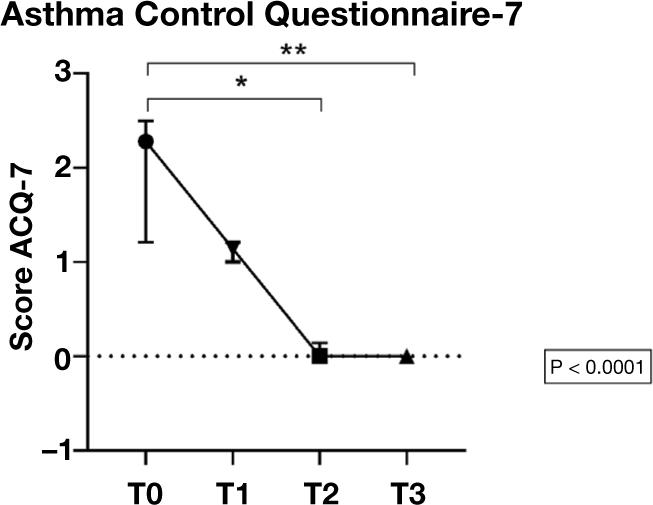
After 4 weeks of therapy, all subjects showed improvement in both ACT and ACQ-7 scores but without statistical significance. However, both ACT and ACQ-7 scores demonstrated statistically significant improvement compared to basal values after 12 and 24 weeks of treatment (Figures 2 and 3).
Figure 2 Changes in asthma control test (ACT) score before treatment and after 4, 12, and 24 weeks. *P < 0.05; **P < 0.01.
Figure 3 Changes in ACQ-7 score before treatment and after 4, 12, and 24 weeks. ACQ-7: Asthma Control questionnaire; *P < 0.05; **P < 0.01; T0: before treatment; T1: after 4 weeks; T2: after 12 weeks; T3: after 24 weeks.
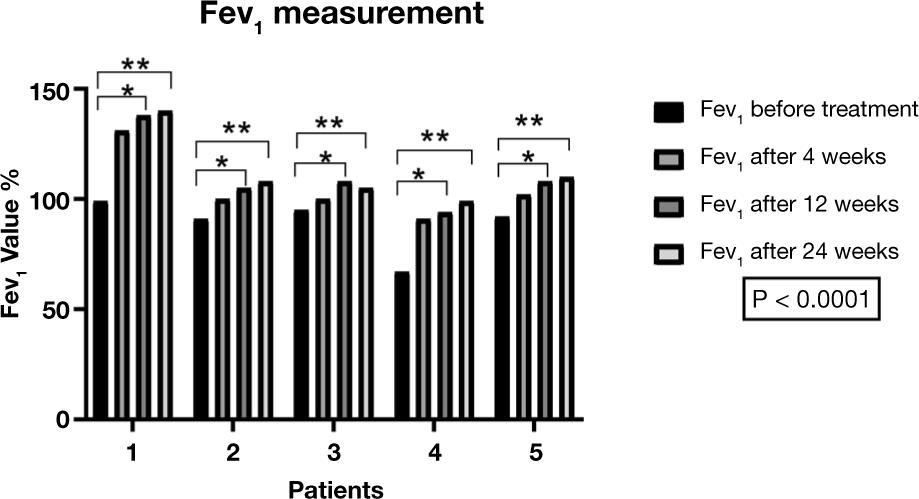
In the same manner, Fev1 demonstrated statistically significant increase versus basal values after 12 and 24 weeks of treatment (Figure 4).
Figure 4 Changes in Fev1 before and after 4, 12, and 24 weeks of treatment. Fev1: forced expiratory volume in 1 s; *P < 0.05; **P < 0.01.
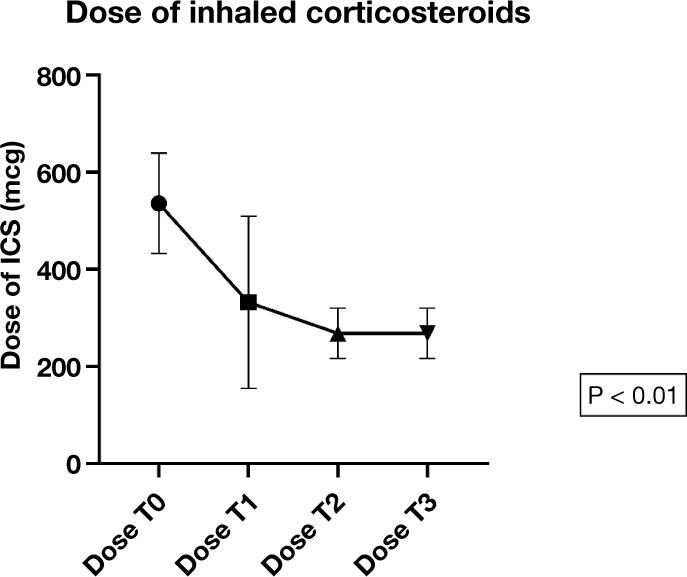
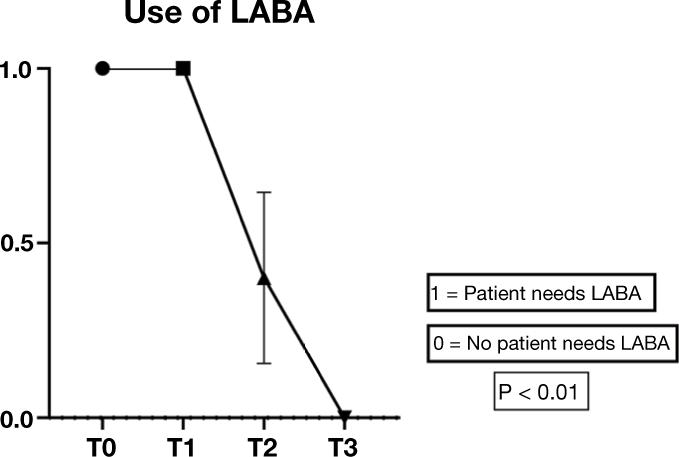
Moreover, after 4 weeks of therapy, 80% of subjects halved their ICS dose (Figure 5), and after 12 weeks, 60% of patients discontinued LABA treatment (Figure 6).
Figure 5 Changes in dose of inhaled corticosteroids (ICSs) before and after 4, 12, and 24 weeks of treatment. T0: before treatment; T1: after 4 weeks; T2: after 12 weeks; T3: after 24 weeks.
Figure 6 Changes in long-acting beta2-agonists (LABA) before and after 4, 12, and 24 weeks of treatment. T0: before treatment; T1: after 4 weeks; T2: after 12 weeks; T3: after 24 weeks.
After 24 weeks of treatment, all patients halved their ICS dose and discontinued LABA. Moreover, they achieved a good control over asthma assessed by ACT and ACQ-7 scores.
The statistical evaluation using the Friedman test at the 4-, 12-, and 24-week control was significant for all the outcomes analyzed, with P < 0.0001 for ACT and ACQ-7. For the values of Fev1, P < 0.0001, and for the data concerning the use of ICS and LABA, P < 0.01.
All endpoints were assessed by multiple comparison of Friedman's test before and after 12 and 24 weeks of treatment. We discovered that changes from baseline in ACT score at week 12 and week 24 showed statistically significant amelioration with dupilumab treatment (ACT before treatment, median 14 (3.5–16) versus ACT after 12 weeks, median 23 (19.5–25), P = 0.04. ACT before treatment, median 14 (3.5–16) versus ACT after 24 weeks, median 25 (23.5–25), P = 0.003).
The changes from baseline in ACQ-7 score at week 12 and week 24 demonstrated statistically significant amelioration with dupilumab treatment. ACQ-7 before -treatment, median 2,28 (1.14–2.49) versus ACQ-7 after 12 weeks, median 0 (0–0.14), P = 0.01. ACQ-7 before treatment, median 2,28 (1.14–2.49) versus ACQ-7 after 24 weeks, median 0 (0–0), P = 0.01.
The changes from baseline in Fev1 score at week 12 and week 24 demonstrated statistically significant amelioration with dupilumab treatment. Fev1 before treatment, median 92 (79–97) versus Fev1 after 12 weeks, median 108 (99.5–123), P = 0.04. Fev1 before treatment, median 92 (79–97) versus Fev1 after 24 weeks, median 108 (102–125), P = 0.003. We evaluated FeNO values during control to assess the level of bronchial inflammation with dupilumab therapy. We observed that, with only two exceptions, the FeNO values have stayed roughly constant over the course of the treatment because of the reduced intake of ICS; Specifically, the two patients had an increase of about 10 ppb in FeNO, compared to pre-treatment values, returning to pre-treatment values during control at 24 weeks.
Finally, none of patients had adverse effect to the treatment during the study period.
Discussion
Our data demonstrated that dupilumab ameliorated asthma control, assessed by ACQ-7 and ACT, and respiratory function assessed by Fev1 in adolescents with severe asthma during 12 weeks period. At the same time, the ICS dose halved after 4 weeks of treatment in almost all patients, and LABA dose was reduced by 60% after 12 weeks of treatment.
These findings were consistent with those reported by other investigations and showed endpoint achievement earlier compared to the results of other studies. In a retrospective study conducted by Dupin et al., comprising adult population with severe uncontrolled asthma, treated with dupilumab, after 1 year, the median Fev1 increased from 58% (47–75) to 68% (58–88) (P = 0.001), the median ACT score increased from 14 (7–16) to 22 (17–24) (P = 0.001), and the daily prednisone dose decreased from 20 mg/day (10–30) to 5 mg/day (0–7) (P = 0.001). Exacerbations per year decreased from 4 (2–7) to 1 (0–2) (P = 0.001).34
In a Japanese study conducted by Numata et al., comprising adult patients with severe asthma (10 patients received dupilumab as the first biologic and 16 patients switched to dupilumab from other biologics), during a mean follow-up period of 12.6 months, dupilumab treatment significantly reduced the number of exacerbations per year from 3.4 ± 4.1 to 1.6 ± 2.7 (P < 0.01). The ACT score significantly improved in all patients by 6 months after administration of dupilumab, but tended to worsen by 24 months in patients with previous biologic use. Adverse events included wheezing immediately after injection, hypereosinophilia, mild conjunctivitis, and relapse of chronic eosinophilic pneumonia in patients switching from benralizumab.35
In a cohort of 18 Italian patients with severe asthma (mean age 53.3 ± 12.4 years, 66.7% females), after 3 months of dupilumab therapy, ACT score improved significantly (from 15.7 ± 5.1 to 18.8 ± 4.8, P = 0.023), intake of OCSs was reduced significantly (10 (5–25) mg/day to 0 (0–5) mg/day, P = 0.0333), and FeNO levels also decreased from 25 (20–80) ppb to 21 (10.9–55.3) ppb (P = 0.0190).36 After 12 months, a statistically significant decrease was observed in the number of exacerbations from two to zero (P < 0.0068); Fev1% increased from 73.5 ± 19.5% to 87.1 ± 19.2% (P = 0.0407); and reduced intake of OCS was observed in all the patients (P < 0.0001).36
It has been demonstrated that reducing OCS intake is an achievable outcome in patient with severe uncontrolled asthma treated with dupilumab or other biologic drugs.36–38 On the other hand, reduction in ICS intake must be considered with caution, because it could lead to clinical worsening of condition. Although currently, little evidence is discovered in the literature, we were able to avoid the use of OCS therapy, and after 24 weeks of treatment, we gradually reduced the dose of ICS by half from the initial dose without clinical worsening.
A case-control study was conducted by Maspero et al. comprising 1902 patients, including 107 adolescents, with moderate-to-severe uncontrolled asthma receiving continuous treatment with ICS plus one or two other asthma medicines. Compared to placebo, changes in Fev1 at week 12 from baseline showed significant amelioration with both dupilumab 200 mg (0.37 L; 95% confidence interval [95% CI]: 0.13–0.61; P = 0.003) and 300 mg (0.27 L; 95% CI: 0.02–0.52; P = 0.037) in adolescents. In comparison to adults, adolescents showed better results in terms of lung function and proportion of severe exacerbations. By week 52, dupilumab significantly improved ACQ-5 scores, compared to placebo.37 The level of Fev1 improvement was greater in 80% of teenage patients with increased baseline Th2 biomarker levels treated with dupilumab 200 mg (0.43 L; 95% CI: 0.17–0.69; P = 0.002), compared to intention-to-treat (ITT) subgroup.
Compared to our trial, although Maspero et al. study was a case-control study and the applied questionnaire was ACQ-5, the results demonstrated similar and significant findings regarding improvement in Fev1 (both findings at 12 weeks), while improvement of ACQ-5 scores versus placebo was observed at by week 52.
In a systematic review conducted by Agache et al., including three randomized control trials (RCTs), approximately 2735 subjects aged ≥12 years were followed up for 24–52 weeks.38 Dupilumab reduced both severe asthma exacerbations (incidence rate ratio 0.51; 95% CI: 0.45–0.59) and percentage of OCS use (mean difference [MD]: −28.2 mg/day; 95% CI: 40.7–15.7). The results showed amelioration in asthma control (ACQ-5), Asthma Quality of Life Questionnaire (AQLQ) score, and use of rescue medication (puffs/die) with the following estimates: rescue medicine (MD: 0.35; 95% CI: 0.73–+0.02], AQLQ (MD: +0.28; 95% CI: 0.20–0.37), and ACQ-5 (MD: 0.28; 95% CI: 0.39–0.17). Fev1 also increased (MD: +0.15, 95% CI: +0.11–+0.18).38
In a TRAVERSE study consisting of 27 countries to assess the safety and efficacy of dupilumab in adults and adolescents with moderate-to-severe or OCSs-dependent severe asthma for 148 weeks, the most frequently reported adverse events were nasopharyngitis, injection-site erythema, and bronchitis; serious asthma exacerbations were determined in 0.5–3.6% patients and pneumonia occurred only in 0.7–2.7% patients. Rapid ameliorations were observed in pre-bronchodilator Fev1 and ACQ-5 and AQLQ scores; blood eosinophils and serum total IgE also decreased progressively.39
Dupilumab lowers the rate of severe exacerbations, enhances Fev1 and asthma control, and suppresses type 2 inflammatory biomarkers in patients with both allergic and nonallergic asthma.40 Unlike in other trials, in our study we did not notice conjunctivitis in any treated patients.41,42 Currently, we discovered no evidence to indicate the discontinuation of dupilumab therapy. In our opinion, further prospective studies are required to determine the safe discontinuation of treatment with dupilumab and other biological drugs. Our study is one of the few studies that have analyzed the time-dependent effect of dupilumab on asthmatic exacerbations, asthma control, lung function, and FeNO in adolescents.43 The limitation of our study is the less number of patients included and its retrospective design.
Conclusions
The preliminary results demonstrate that dupilumab is speedily effective in treating severe asthma in adolescents and its fast action could be useful for a better compliance to this treatment.
Author Contributions
Cristiana Indolfi: data curation, methodology, and review; Giulio Dinardo: writing, methodology, formal analysis, and investigation; Angela Klain: writing, methodology, and investigation; Marcella Contieri: writing and fund acquisition; Giuseppina Rosaria Umano: software and methodology; Alberto Decimo: supervision and resources; Giorgio Ciprandi: review and visualization; and Michele Miraglia del Giudice: conceptualization, supervision, visualization, and project administration.
Conflict of Interest
The authors declared no conflict of interest.
REFERENCES
1. Del Giudice MM, Allegorico A, Marseglia GL, Martelli A, Calvani M, Cardinale F, et al. Allergic rhinoconjunctivitis. Atenei Parm [Internet]. 2020 [cited 2022 Sep 15]. Acta Bio Medica. 2020;91(Suppl 11-S):e2020007. 10.23750/abm.v91i11-S.10310
2. Klain A, Indolfi C, Dinardo G, Decimo F, Tosca MA, Miraglia Del Giudice M, et al. Comparing available treatments for pollen-induced allergic rhinitis in children [Internet]. 2022 [cited 2022 Sep 15]. Expert Rev Clin Immunol. 2022;18(8):835–43. 10.1080/1744666X.2022.2093188
3. Galli E, Cinicola B, Carello R, Caimmi S, Brindisi G, De Castro G, et al. Atopic dermatitis. Atenei Parm [Internet]. 2020 [cited 2022 Sep 15]. Acta Bio Medica. 2020;91(Suppl 11):1–10.
4. Maiello N, Giannetti A, Ricci G, Cinicola B, Carello R, Indolfi C, et al. Atopic dermatitis and atopic march: Which link? [Internet]. 2021 Nov 29 [cited 2022 Sep 15]. Acta Biomed. 2021;92(S7):e2021525.
5. Chung KF, Wenzel SE, Brozek JL, Bush A, Castro M, Sterk PJ, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma [Internet]. 2014 Feb 1 [cited 2021 Apr 7]. Eur Respir J. 2014;43(2):343–73.
6. Castagnoli R, Marseglia A, Brambilla I, Marseglia GL, Licari A. Severe uncontrolled asthma in children: Practical approach on diagnosis and management. Minerva Pediatr. 2020, Jun 1;72(3):196–205. 10.23736/S0026-4946.20.05818-1
7. de Benedictis F, del Giudice MM, Vetrella M, Tressanti F, Tronci A, Testi R, et al. Nebulized fluticasone propionate vs. budesonide as adjunctive treatment in children with asthma exacerbation [Internet]. 2005 Jun 1 [cited 2022 Sep 13]. J Asthma. 42(5):331–6. 10.1081/JAS-200062966
8. Del Giudice MM, Pezzulo A, Capristo C, Alterio E, Caggiano S, de Benedictis D, et al. Leukotriene modifiers in the treatment of asthma in children [Internet]. 2009 [cited 2022 Sep 13]. Ther Adv Respir Dis. 2009;3(5):245–51. 10.1177/1753465809348014
9. Di Cicco ME, Leone M, Scavone M, Del Giudice MM, Licari A, Duse M, et al. Intermittent and mild persistent asthma: How therapy has changed [Internet]. 2021 Nov 29 [cited 2022 Sep 13]. Acta Biomed. 2021;92(S7):e2021523. 10.23750/abm.v92iS7.12422
10. Indolfi C, Dinardo G, Rosaria Umano G, Klain A, Contieri M, Decimo A, et al. Mometasone furoate nasal spray in Italian children with seasonal allergic rhinitis: A comprehensive assessment [Internet]. 2022 Sep 1 [cited 2022 Sep 13]. Allergol Immunopathol (Madr). 2022;50(5):61–7. 10.15586/aei.v50i5.643
11. Miraglia del Giudice M, Piacentini GL, Capasso M, Capristo C, Maiello N, Boner AL, et al. Formoterol, montelukast, and budesonide in asthmatic children: Effect on lung function and exhaled nitric oxide [Internet]. 2007 Aug [cited 2022 Sep 13]. Respir Med. 2007;101(8):1809–13. 10.1016/j.rmed.2007.02.010
12. Ahmed H, Turner S. Severe asthma in children–A review of definitions, epidemiology, and treatment options in 2019 [Internet]. 2019 Jun 1 [cited 2022 May 26]. Pediatr Pulmonol. 54(6):778–87. 10.1002/ppul.24317
13. Ciprandi G, Cioffi L, Schiavetti I, del Giudice MM, Tosca MA. Factors associated with wheezing recurrence in clinical practice [Internet]. 2022 Jun 10 [cited 2022 Jun 30]. J Asthma. 2023;60(4):843-844. 10.1080/02770903.2022.2087187
14. Marseglia GL, Manti S, Chiappini E, Brambilla I, Caffarelli C, Calvani M, et al. Chronic cough in childhood: A systematic review for practical guidance by the Italian Society of Pediatric Allergy and Immunology [Internet]. 2021 [cited 2022 Jun 30]. Allergol Immunopathol (Madr). 49(2):133–54. 10.15586/aei.v49i2.44
15. Duse M, Santamaria F, Verga MC, Bergamini M, Simeone G, Leonardi L, et al. Inter-society consensus for the use of inhaled corticosteroids in infants, children and adolescents with airway diseases [Internet]. 2021 Dec 1 [cited 2022 Jun 30]. Ital J Pediatr. 2021;47(1):1–24. 10.1186/s13052-021-01013-8
16. Tozzi AE, Armenio L, Bernardini R, Boner A, Calvani M, Cardinale F, et al. Pediatric allergy and immunology in Italy [Internet]. 2011 May [cited 2022 Jun 30]. Pediatr Allergy Immunol. 2011;22(3):267–76. 10.1111/j.1399-3038.2011.01157.x
17. Del Giudice MM, Brunese FP, Piacentini GL, Pedullà M, Capristo C, Decimo F, et al. Fractional exhaled nitric oxide (FeNO), lung function and airway hyperresponsiveness in naïve atopic asthmatic children [Internet]. 2004 [cited 2022 Sep 13]. J Asthma. 2004;41(7):759–65. 10.1081/JAS-200027862
18. Global Initiative for Asthma (GINA). GINA main report [Internet]. 2022 [cited
19. Arasi S, Costa S, Magazzù G, Ieni A, Crisafulli G, Caminiti L, et al. Omalizumab therapy in a 13-year-old boy with severe persistent asthma and concomitant eosinophilic esophagitis [Internet]. 2016 Mar 22 [cited 2022 Jun 30]. Ital J Pediatr. 2016;42(1):32. 10.1186/s13052-016-0243-x.
20. Cutrera R, Baraldi E, Indinnimeo L, Miraglia Del Giudice M, Piacentini G, Scaglione F, et al. Management of acute respiratory diseases in the pediatric population: The role of oral corticosteroids [Internet]. 2017 Mar 23 [cited 2022 Jun 30]. Ital J Pediatr. 2017;43(1):31. 10.1186/s13052-017-0348-x
21. EMA. Dupilumab European Medicines Agency. Summary of product characteristics [Internet]. [cited
22. AIFA. Agenzia Italiana del Farmaco. Annex I summary of product characteristics [Internet]. [cited
23. Harb H, Chatila TA. Mechanisms of Dupilumab [Internet]. 2020 Jan 1 [cited 2022 Jun 28]. Clin Exp Allergy. 2020;50(1):5–14. 10.1111/cea.13491
24. Hall S, Agrawal DK. Key mediators in the immunopathogenesis of allergic asthma [Internet]. 2014 [cited 2022 Jun 28]. Int Immunopharmacol. 2014;23(1):316–29. 10.1016/j.intimp.2014.05.034
25. Bagnasco D, Ferrando M, Varricchi G, Passalacqua G, Canonica GW. A critical evaluation of anti-IL-13 and anti-IL-4 strategies in severe asthma [Internet]. 2016 Aug 1 [cited 2022 Jun 28]. Int Arch Allergy Immunol. 2016;170(2):122–31. 10.1159/000447692
26. Calzavara-Pinton P, Fortina AB, Bonamonte D, Marseglia GL, Del Giudice MM, Musarra A, et al. Diagnosis and management of moderate-to-severe atopic dermatitis in adolescents. A consensus by the Italian Society of Dermatology and Venereology (SIDeMaST), the Italian Association of Hospital Dermatologists and Public Health (ADOI), the Italian Association of Hospital and Territorial Allergists and Immunologists (AAIITO), the Italian Society of Allergy, Asthma and Clinical Immunology (SIAAIC), the Italian Society of Pediatric Allergy and Immunology (SIAIP), the Italian Society of Allergologic [Internet]. 2021 Apr 1 [cited 2022 Jun 30]. Ital J Dermatol Venereol. 2021;156(2):184–97. 10.23736/S2784-8671.20.06654-7
27. Licari A, Castagnoli R, Marseglia A, Olivero F, Votto M, Ciprandi G, et al. Dupilumab to treat type 2 inflammatory diseases in children and adolescents [Internet]. 2020 Jun 1 [cited 2022 Jun 28]. Paediatr Drugs. 2020;22(3):295–310. 10.1007/s40272-020-00387-2
28. Food and Drug Administration (FDA). Dupilumab FDA prescribing information [Internet]. 2019 [cited
29. Cloutier MM, Schatz M, Castro M, Clark N, Kelly HW, Mangione-Smith R, et al. Asthma outcomes: composite scores of asthma control [Internet]. 2012 Mar [cited 2022 Jun 28]. J Allergy Clin Immunol. 2012;129(3 Suppl):S24–33. 10.1016/j.jaci.2011.12.980.
30. Juniper EF, Gruffydd-Jones K, Ward S, Svensson K. Asthma control questionnaire in children: Validation, measurement properties, interpretation [Internet]. Eur Respir J. 2010;36(6):1410–6. 10.1183/09031936.00117509
31. Dinakar C, Chipps BE, Matsui EC, Abramson SL, Irani AM, Kim JS, et al. Clinical tools to assess asthma control in children [Internet]. Pediatrics. 2017;139(1):e20163438. 10.1542/peds.2016-3438.
32. Van Dijk BCP, Svedsater H, Heddini A, Nelsen L, Balradj JS, Alleman C. Relationship between the Asthma Control Test (ACT) and other outcomes: A targeted literature review [Internet]. 2020 Apr 3 [cited 2022 Jun 28]. BMC Pulm Med. 2020;20(1):1–9. 10.1186/s12890-020-1090-5
33. Korn S, Both J, Jung M, Hbner M, Taube C, Buhl R. Prospective evaluation of current asthma control using ACQ and ACT compared with GINA criteria [Internet]. 2011 [cited 2022 Jun 28]. Ann Allergy Asthma Immunol. 2011;107(6):474–9. 10.1016/j.anai.2011.09.001
34. Dupin C, Belhadi D, Guilleminault L, Gamez AS, Berger P, De Blay F, et al. Effectiveness and safety of dupilumab for the treatment of severe asthma in a real-life French multi--centre adult cohort [Internet]. 2020 Jul 1 [cited 2022 Jun 28]. Clin Exp Allergy. 2020;50(7):789–98. 10.1111/cea.13614
35. Numata T, Araya J, Miyagawa H, Okuda K, Takekoshi D, Hashimoto M, et al. Real-world effectiveness of dupilumab for patients with severe asthma: A retrospective study [Internet]. 2022 [cited 2022 Jun 28]. J Asthma Allergy. 2022;15:395–405. 10.2147/JAA.S357548
36. Campisi R, Crimi C, Nolasco S, Beghè B, Antonicelli L, Guarnieri G, et al. Real-world experience with dupilumab in severe asthma: One-year data from an Italian named patient program [Internet]. 2021 [cited 2022 Jun 28]. J Asthma Allergy. 2021;14:575–83. 10.2147/JAA.S312123
37. Maspero JF, FitzGerald JM, Pavord ID, Rice MS, Maroni J, Rowe PJ, et al. Dupilumab efficacy in adolescents with uncontrolled, moderate-to-severe asthma: LIBERTY ASTHMA QUEST [Internet]. 2021 Aug 1 [cited 2022 Jun 28]. Allergy. 2021;76(8):2621–4. 10.1111/all.14872
38. Agache I, Song Y, Rocha C, Beltran J, Posso M, Steiner C, et al. Efficacy and safety of treatment with dupilumab for severe asthma: A systematic review of the EAACI guidelines–Recommendations on the use of biologicals in severe asthma [Internet]. 2020 May 1 [cited 2022 Jun 28]. Allergy. 2020;75(5):1058–68. 10.1111/all.14268
39. Wechsler ME, Ford LB, Maspero JF, Pavord ID, Papi A, Bourdin A, et al. Long-term safety and efficacy of dupilumab in patients with moderate-to-severe asthma (TRAVERSE): An open-label extension study [Internet]. 2022 Jan 1 [cited 2022 Jun 28]. Lancet Respir Med. 2022;10(1):11–25. 10.1016/S2213-2600(21)00322-2
40. Castro M, Corren J, Pavord ID, Maspero J, Wenzel S, Rabe KF, et al. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma [Internet]. 2018 Jun 28 [cited 2021 Apr 7]. N Engl J Med. 2018;378(26):2486–96. 10.1056/NEJMoa1804092
41. Bansal A, Simpson EL, Paller AS, Siegfried EC, Blauvelt A, de Bruin-Weller M, et al. Conjunctivitis in dupilumab clinical trials for adolescents with atopic dermatitis or asthma [Internet]. 2021 Jan 1 [cited 2022 Jun 28]. Am J Clin Dermatol. 2021;22(1):101–15. 10.1007/s40257-020-00577-1
42. Akinlade B, Guttman-Yassky E, de Bruin-Weller M, Simpson EL, Blauvelt A, Cork MJ, et al. Conjunctivitis in dupilumab clinical trials [Internet]. 2019 Sep 1 [cited 2022 Jun 28]. Br J Dermatol. 2019;181(3):459–73. 10.1111/bjd.17869
43. Dinardo G, Indolfi C, Klain A, Decimo F, Miraglia Del Giudice M. Treatment of severe asthma: fast action of dupilumab in the pediatric setting [Internet]. 2023 Apr 1 [cited 2023 Jul 10]. Minerva Pediatr;75(2):312–3. 10.23736/S2724-5276.21.06437-5