
Download
REVIEW ARTICLE
Severe bronchiolitis profiling as the first step towards prevention of asthma
Izabela Orzołeka†, Dominika Ambrożeja,b†, Heidi Makriniotic, Zhaozhong Zhuc, Tuomas Jarttid,e,f, Wojciech Feleszkoa*
aDepartment of Pediatric Pneumonology and Allergy, Medical University of Warsaw, Warsaw, Poland
bDoctoral School, Medical University of Warsaw, Warsaw, Poland
cDepartment of Emergency Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA
dPEDEGO Research Unit, University of Oulu, Oulu, Finland
eDepartment of Pediatrics and Adolescent Medicine, University of Oulu, Oulu, Finland
fDepartment of Pediatrics and Adolescent Medicine, Turku University Hospital and University of Turku, Turku, Finland
†Izabela Orzołeka and Dominika Ambrożej shared first authorships.
Abstract
Bronchiolitis is the most common respiratory infection leading to hospitalization and constitutes a significant healthcare burden. The two main viral agents causing bronchiolitis, respiratory syncytial virus (RSV) and rhinovirus (RV), have distinct cytopathic, immune response, and clinical characteristics. Different approaches have been suggested for subtyping bronchiolitis based on viral etiology, atopic status, transcriptome profiles in blood, airway metabolome, lipidomic data, and airway microbiota. The highest risk of asthma at school age has been in a subgroup of bronchiolitis characterized by older age, high prevalence of RV infection, previous breathing problems, and/or eczema. Regarding solely viral etiology, RV-bronchiolitis in infancy has been linked to a nearly three times higher risk of developing asthma than RSV-bronchiolitis. Although treatment with betamimetics and systemic corticosteroids has been found ineffective in bronchiolitis overall, it can be beneficial for infants with severe RV bronchiolitis. Thus, there is a need to develop a more individualized therapeutic approach for bronchiolitis and follow-up strategies for infants at higher risk of asthma in the future perspective.
Key words: Asthma, Bronchiolitis, Child, Virus, Wheezing
*Corresponding author: Wojciech Feleszko, Department of Pediatric Pneumonology and Allergy, Medical University of Warsaw, Warsaw, Poland. Email address: [email protected]
Received 27 October 2022; Accepted 7 February 2023; Available online 1 May 2023
Copyright: Orzolek I, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Bronchiolitis is defined as a viral infection of bronchioles and surrounding tissue. It can present as a mild illness that is safely managed as an outpatient or as a severe illness requiring hospitalization, intensive care unit (ICU) admission, and/or invasive ventilatory support.1 Bronchiolitis is the leading cause of hospitalization in children, accounting for approximately 1% of all children.2 Moreover, it also has substantial chronic airway morbidity, such as recurrent wheezing and childhood asthma.2 Depending on risk factors, approximately 30–80% of children will have subsequent asthma.3,4 Therefore, bronchiolitis and its long-term sequela has a considerable impact on the healthcare systems worldwide.5,6 Most guidelines, however, recommend only supportive care for bronchiolitis, even in the hospital setting.1
The purpose of this brief review was to open the evidence supporting distinct entities of bronchiolitis. Moreover, we wanted to discuss how they are linked to compromised long-term outcomes and treatment responses.
Viral Etiology of Bronchiolitis
Based on the past and current evidence, respiratory viral infections are the main trigger of bronchiolitis and acute wheezing episodes in children. Epidemiological data might vary, but most observational studies have identified respiratory syncytial virus (RSV) and rhinovirus (RV) as the two dominant viral triggers.7–9 The overall prevalence of RSV and RV in children under 2 years old with bronchiolitis is estimated at approximately 60 and 20%, respectively.10 During infancy the most common etiologic factor is RSV, accounting for about 60–70% of the cases.11 The hospitalization rates of RSV-induced bronchiolitis are the highest in those aged less than 3 months.12 In comparison, RV is the second most common virus in infants older than 6 months.6 Other less commonly detected viruses in children with bronchiolitis under 2 years old include human bocavirus, adenovirus, metapneumovirus, parainfluenza virus, influenza virus, and coronaviruses.10
Before the COVID-19 pandemic in 2020, seasonality of RSV and RV infections was different. In Europe, the RSV wave started in December and continued until April (peaking between January and March).13,14 RV infections, on the contrary, were present throughout the year but with the greatest prevalence during the spring and autumn.15 During the COVID-19 pandemic, a deviation from that pattern was observed with a significantly reduced number of bronchiolitis hospitalizations in Europe during winter 2020/21.16–18,19 In the subsequent winter season (i.e., winter 2021/22), the bronchiolitis cases peaked in Europe earlier, starting in November, and was approximately 2–3 weeks shorter18,20 with a similar pattern in the current 2022/23 season.20–22 A recent study observed an increase in RSV infections needing hospitalization in the current season, increased medium age of hospitalized infants, a more extended hospital stay, a more frequent need for respiratory support, and a higher frequency of patients with a history of prematurity.21 At the same time, the rate of ICU admissions and mechanical ventilation did not increase.21 Overall, studies show that compared to pre-pandemic years, hospital admissions due to bronchiolitis significantly decreased during the pandemic.16,18,23 The most likely reason is that children and caregivers did not contract respiratory viral illnesses in view of “stay at home” measures that were followed by the entire families. Other reasons focus on the possibly successful implementation of non-pharmacological interventions, the reduced use of daily care facilities, and school closures during the COVID-19 pandemic.20 Following this period of reduced bronchiolitis hospitalizations, we observed a spike in bronchiolitis cases (hospitalized or not) the subsequent year. This increase in disease severity may be related to the “immunity debt” phenomenon. This phenomenon is more prevalent in children who were raised in areas of restrictive measures and were suddenly exposed to extensive social interactions and viral infections.21
Hence, being on top of epidemiological evidence, around RSV and RV-induced infections can possibly inform healthcare services’ design and can also introduce impactful public health interventions, changing respiratory viral epidemiology should affect the distribution of healthcare resources and future public health policies.24
Clinical Characteristics and Their Link to Asthma
Expiratory breathing difficulty is a characteristic symptom of bronchiolitis and asthma. The diagnosis of bronchiolitis is made clinically. The constellation of clinical symptoms of bronchiolitis typically includes cough and signs of dyspnea as tachypnea, accessory respiratory muscles usage, and/or nasal flaring with possible decreased oxygen saturation.11 Among the other bronchiolitis features, adventitious breath sounds such as expiratory wheezing, crackles, rhonchi, and rales, hyperinflation and displaced liver may be observed in severe cases.1,25 Prodromal signs, occurring between 2 and 4 days before, usually include rhinitis, nasal congestion, and rhinorrhea.1
RV-bronchiolitis is mainly caused by species A and C. Overall, in this disease, the odds ratios (ORs) for school-age asthma are in the range of 3–10. However, allergic sensitization (OR 45) and eczema have been associated with an enhanced risk for atopic asthma inception later in childhoodss, OR up to 5.1.26–28 Conversely, the risk factors for a nonatopic phenotype of asthma by the age of 7 were RSV-induced bronchiolitis, the first episode of wheezing before the age of 1, and parental smoking ORs up to 8.1.27
Viral-dependent Pathogenesis of Bronchiolitis
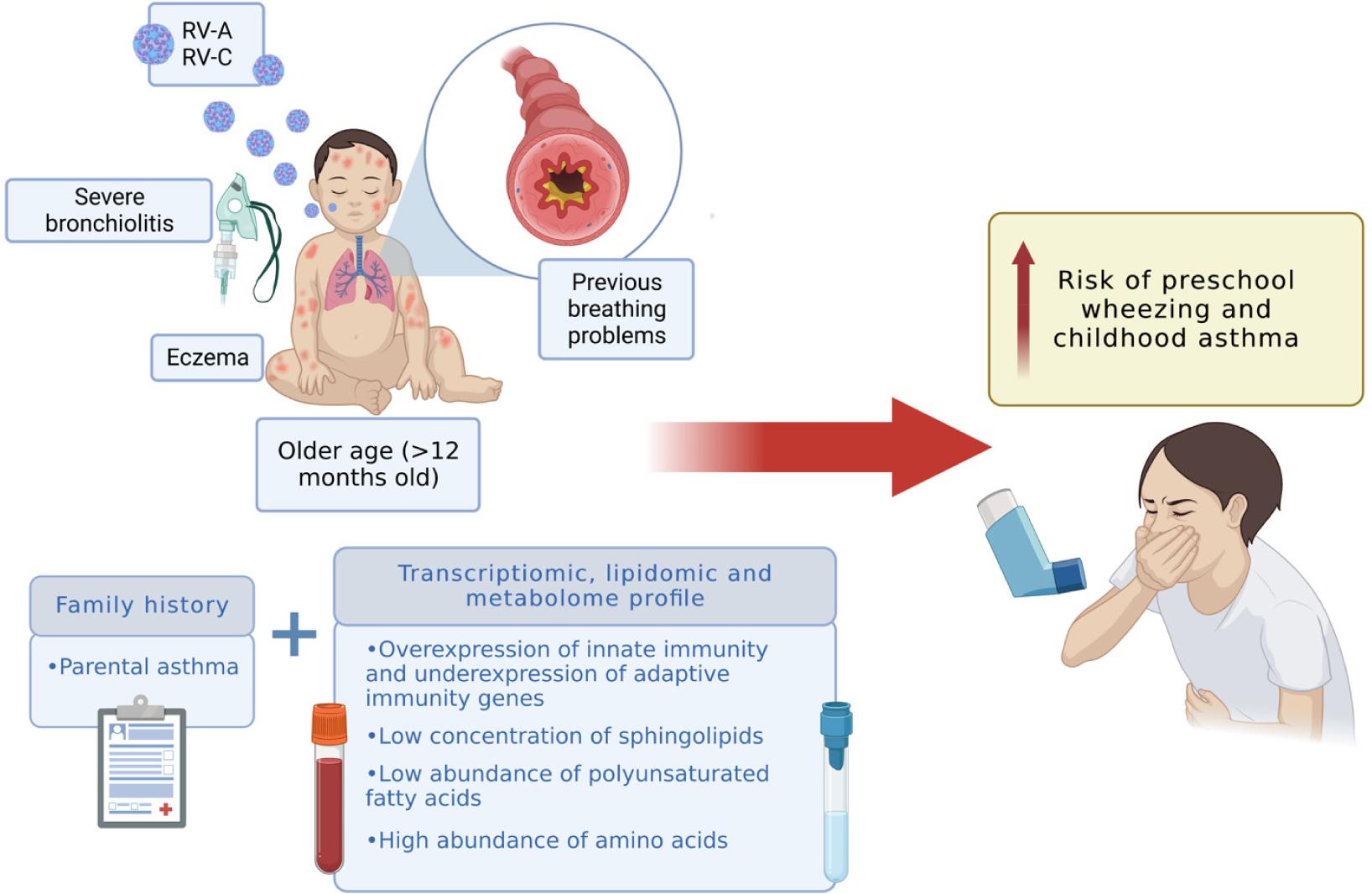
For decades bronchiolitis was regarded as a single disease based solely on the clinical presentation; however emerging data have recently demonstrated that the underlying pathomechanism of bronchiolitis is associated with specific viral etiology. Its two most common viral triggers, RSV and RV, were shown to engage a distinct host immune response and are associated with different airway injuries.29 However, with regard to asthma development, it remains unclear whether it is the early-life respiratory viral infection that initiates the abnormal chronic immune reactions in the airways or whether it is the viral-induced bronchiolitis that can serve as the marker of the underlying personal predisposition to asthma development. Most of the data supports the latter (Figure 1).25
Figure 1 Summary of personal traits, family history, metabolome, and lipidomic profile associated with a higher risk of preschool wheezing and childhood asthma. Created with BioRender.com.
Respiratory syncytial virus–induced bronchiolitis
Following an incubation period lasting about 4–6 days, the virus starts to replicate in the nasal mucosa, resulting in nasal congestion, rhinorrhea, irritability, and poor feeding.29 Further involvement of the epithelial cells of the lower respiratory tract induces secretion of antiviral interferons type I and III.25 Subsequent infiltration of immune cells (NK cells, helper CD4+, cytotoxic CD8+, and granulocytes) leads to edema, hypersecretion of mucus, sloughing of infected epithelial cells, and impaired ciliary action resulting in obstruction of bronchioles. Typical cytopathic features are syncytiums and multinuclear giant cells when infected superficial epithelial cells merge with neighboring cells before apoptosis. Cell debris and mucus make a mechanical obstruction in the airways. Inhaled air is trapped behind occluded bronchioles, leading to hyperinflation. Intraluminal obstruction causes decreased perfusion and oxygen saturation.29
Rhinovirus-induced bronchiolitis
Rhinoviruses and RSV are spread via direct contact or aerosol particles and target respiratory epithelial cells of the upper and lower airways.25 RV enhances the production of epithelial-derived cytokines such as25 interleukin (IL)-25 and IL-33, inducing type-2 immune response. Activated type-2 innate lymphoid (ILC2) cells secrete type-2 cytokines such as IL-5, IL-9, and IL-13, which generate the recruitment of eosinophils, mast, and goblet cells, and increased mucus production.30
In addition, RV has been reported to elucidate increased production of molecules involved in remodeling, fibrosis of airways, and reduction of preventive factors such as tissue inhibitor metalloproteinases (TIMPs) in vitro.31,32 A recent study reports that during a severe RV-induced bronchiolitis episode, there is an upregulated secretion of remodeling factors (e.g., TGFα, HGF, and MMP-2) in nasal washings from children below 24 months old. Thus, data indicate that RV infection in early childhood may induce a pro--remodeling milieu in airways and may result in permanent obstruction later in life.33 Moreover, RV-induced bronchiolitis in infancy has been associated with lower lung function at ages 7–9. Children with a sequel of RV infection before the age of 24 months had significantly lower z-score FEV1 values (−0.64) at ages 7–9 years than those with past RSV bronchiolitis (−0.13, P = 0.04).34
There are three RV species (A, B, C), and species C and A have been linked with more severe illness and wheezing compared to species B.30 The single nucleotide polymorphism in the CDHR3 gene (a unique receptor for RV-C) has been associated with a phenotype of more severe asthma exacerbations30 and an increased risk of childhood asthma.35,36 Additionally, variants at the 17q21 locus in children with an episode of RV bronchiolitis in infancy have been linked with a greater risk of childhood asthma OR 26.1.37 Factors predisposing to RV-wheeze in infants include aeroallergen sensitization and other atopic features such as eczema or eosinophilia.38
Risk Factors for Developing a Severe Course of the Disease
About 19% of hospitalized infants with bronchiolitis need intensive care treatment.39 The risk factors for a severe course of bronchiolitis include age below 6 weeks, prematurity, underlying chronic lung disease, congenital heart disease, immunodeficiency, and neurological disease.11 The higher risk of bronchiolitis in preterm infants is partially explained by insufficient transplacental passage of RSV-specific maternal antibodies, as it predominately occurs during the third trimester.40 Very preterm infants born before 30 weeks of gestation were found to have significantly higher hospitalization rates than late preterm (born >30 weeks of gestation) or term infants. Still, other factors can explain this, for example, increased prevalence of chronic lung disease and congenital heart defects that can add to the increased susceptibility to invasive respiratory pathogens.12,41
Severe Bronchiolitis Profiling (Molecular Differences between RSV and RV)
With the advances in high-throughput sequencing technology, attempts are underway to dissect the different populations of children with severe bronchiolitis. Differences in host immune responses to RSV and RV in infants with bronchiolitis have been first studied based on the analysis of the whole-blood RNA sequencing.42–44 RSV blood transcriptional profile was characterized by the upregulation of genes related to inflammation and innate immunity with simultaneous suppression of modules regulating adaptive immunity (such as T cells, B cells, and natural killer (NK) cells) and antimicrobial responses. In subjects with RV bronchiolitis, the downregulation of adaptive immunity genes was significantly less pronounced.43 The degree of host immune suppression genes was linked with disease severity and younger age in infants with RSV bronchiolitis.43 Interestingly, changes in transcriptome profile (overexpression of innate immunity and underexpression of adaptive immunity genes) were significant in infants who tested positive for RV but only in symptomatic subjects, in contrast with those with asymptomatic RV infection.44 RV is frequently detected in the absence of symptoms of infection in young children, varying from 14 to 50%.45–48 These findings suggest that asymptomatic RV detection likely represents the detection of viral RNA without significant activation of systemic host responses. Therefore, whole-blood transcriptional profiling of children may serve as a useful diagnostic tool to discriminate between active infection and incidental pathogen detection.44
Emerging evidence has demonstrated the contributions of the respiratory viral trigger, airway microbiome, and transcriptome in infants with bronchiolitis, mainly in the single-element “omic” approaches (such as proteomic or metabolomic analysis).49–54 Studies using nasopharyngeal airway metabolome data from inpatients with severe bronchiolitis identified their distinct metabotypes. The metabolic profile characterized by a high abundance of inflammatory amino acids and low abundance of PUFAs was associated with a higher risk for the development of recurrent wheezing and childhood asthma.55 Based on analysis of lipidomic data from upper airways of the same study group, a lower concentration of sphingolipids (e.g., sphingomyelins, ceramides) was linked with a significantly higher risk of asthma at the age of six.56 Again, based on the MARC cohort studies, the distinct endotypes within the infants with RSV and RV-induced bronchiolitis were recognized by integrating multi-“omics” data on the clinical presentation, nasopharyngeal airway microbiome, and immune response (level of expression of INF-α and IFN-γ response).57,58 Regarding RSV endotypes, the highest risk of asthma by the age of 5 years was in profile with a high percentage of parental asthma, IgE sensitization, RV coinfection, codominance of Streptococcus pneumoniae/Moraxella catarrhalis in the lung microbiome, and high epithelial INF-α and IFN-γ responses.58 In contrast, an endotype with the highest risk for asthma and recurrent wheeze among RV profiles was characterized by the high (>300 cells/mm3) serum eosinophilia, IgE sensitization, genotype RV-C infection, a predominance of M. catarrhalis in the microbiome and high type-2 cytokine response.57
A recent study showed that the airway microbiome could modify host immune responses and influence metabolic pathways associated with a higher risk of asthma. The most significant changes in host metabolic pathways (such as fatty acid and carbohydrate metabolism) in children that developed asthma 6 years after a bronchiolitis episode were driven by three major bacteria species (S. pneumoniae, Haemophilus influenzae, M. catarrhalis).59 Second, airway colonization with S. pneumoniae in infants was related to a significantly higher risk of asthma in infants with non-RV bronchiolitis, suggesting a synergistic effect of viral trigger and microbiome.59 Third, in line with previous findings, downregulated INF-α and IFN-γ host response was associated with the disease severity and long-term respiratory sequela such as asthma development.59
Moreover, another bronchiolitis research integrated the interrelations between the host response, microbial composition with its function in the airway, and their integrated role in the disease severity in infants with bronchiolitis.51 Fujiogi et al. identified several modules linked with illness severity.51 The host-type I interferon, S. pneumoniae/Staphylococcus aureus abundance, neutrophil/IL-1, T-cell regulation, microbial-branched-chain amino acid metabolism, and nicotinamide adenine dinucleotide hydrogen were the modules significantly associated with risks of positive pressure ventilation use in these infants. However, the mechanisms involved in these complex interactions still need to be further elucidated, especially as they are not reciprocally exclusive.51
These studies support the notion of bronchiolitis as a heterogeneous disease with distinct underlying mechanisms and risk for long-term sequelae (Table 1).
Table 1 Summary of differences in prevalence, clinical presentation, treatment responses and molecular distinctions between two major viral agents causing bronchiolitis—respiratory syncytial virus (RSV) and rhinovirus (RV).
| Respiratory syncytial virus (RSV) | Rhinovirus (RV) | |
|---|---|---|
| Prevalence in children under 2 years old hospitalized with bronchiolitis | Around 60%10 | Around 20%10 |
| Clinical presentation | ||
| Requirement of oxygen supplementation | More infants hospitalized with RSV bronchiolitis require oxygen7,8,64,65 | - |
| Personal history of eczema | - | More infants hospitalized with RV bronchiolitis have a personal history of eczema61,62,65,67,68 |
| Wheezing at admission | No difference has been found7,8,61–65 | - |
| Fever at admission | No difference has been found8,66 | - |
| Parental atopy | No difference has been found7,61,67,68 | - |
| Ventilation support and ICU transfer | No difference has been found7,8,61,63–65,69 | - |
| Risk of asthma following bronchiolitis episode | ||
| Risk of asthma following severe bronchiolitis | Lower risk of recurrent wheeze and childhood asthma4 | Higher risk of the development of recurrent wheezing and childhood asthma compared to RSV (OR 4.1 vs 2.7)4 |
| Factors associated with higher risk of asthma by the age 5 | Parental asthma IgE sensitization, RV coinfection Codominance of Streptococcus pneumoniae/Moraxella catarrhalis in the lung microbiome High epithelial INF-α and IFN-γ responses |
High (>300 cells/mm3) serum eosinophilia IgE sensitization RV-C infection Predominance of M. catarrhalis in microbiome High type-2 cytokine response |
| Molecular profiles | ||
| Analysis of the whole-blood RNA sequencing | Upregulation of inflammation and innate immunity genes Suppression of modules regulating adaptive immunity43 | Downregulation of adaptive immunity genes less pronounced43 |
| Analysis of microbe’s and host transcriptome | Enriched nucleic acid metabolism83 | Enriched acylation/acetylation function83 |
| Treatment | Systemic steroids not effective | Systemic steroids and beta 2-agonists found effective in short-term and long outcomes78,80,81 |
Severe Bronchiolitis Phenotypes (Clinical Differences)
Up to 30% of children with the first wheezing episode will later be diagnosed with childhood asthma and require asthma control medications.3 Clinically, the exciting profiling of bronchiolitis patients based on multi-“omic” approaches is currently unreachable to large-scale usage. Therefore, there are other attempts to stratify the children with bronchiolitis into endotypes based on the accessible clinical features to easily identify those at higher risk of subsequent asthma in daily practice.
Evaluation of a prospective multicenter cohort (MARC-30 USA) and its validation in another two cohorts (MARC-30 Finland, MARC-35), altogether with over 3000 infants, identified distinct bronchiolitis profiles (A, B, C, D). Latent class analysis investigating factors of clinical presentation such as a history of breathing problems or eczema and virological data was used. Profile A assembled older infants between 6 and 12 months with previous breathing problems, eczema, high prevalence of RV infections, and less than 1% of RSV cases. Profile B was compared to “classic bronchiolitis” characterized by low percentage of previous breathing problems, a high proportion of children with wheezing at presentation, and a high detection rate of RSV. Profile C had the most severe clinical course with significantly longer hospitalization, younger age (2–6 months old), and inadequate oral intake, while profile D had the least severe disease with no wheeze or retractions. Based on the -follow-up assessment, these bronchiolitis profiles were found to be associated with different risks of developing long-term outcomes. Profile A had a higher chance of asthma development by age 6–7 years compared with profile B (38% vs 23%). No differences in risk for subsequent asthma were found between profiles C and D.60 Furthermore, the researchers developed and validated a four-predictor model (RSV infection, history of breathing problems, history of eczema, and parental history of asthma), which helped to identify infants from the high-risk profile.60
The Clinical Impact of Severe Bronchiolitis Profiling
The primary clinical objective of severe bronchiolitis profiling is to identify characteristics associated with the onset or progression of later airway morbidities. Understanding the complex interplay between viral triggers, airway microbiome, host immune response, allergic status, and their contribution to childhood asthma is crucial. For example, colonization by S pneumoniae and non-rhino viral infection in infants correlated with a significantly higher risk of asthma at the age of 6 years.59 A recent meta--analysis comparing between virus differences in the magnitude of preschool wheeze and childhood asthma showed that the RV-bronchiolitis group was over four times more likely to develop recurrent wheeze (OR 4.1) and nearly three times more likely to develop asthma (OR 2.7) than the RSV-bronchiolitis group.4 Hence, the viral etiology of early LTRIs has a vital role in the stratification of bronchiolitis patients, which could lead to more personalized management and preventive strategies in the future perspective.60 Unfortunately, data from observational studies suggest that RSV- and RV-induced lower respiratory tract infections (LTRIs) in children under 2 years old are indifferent in terms of the clinical features present upon hospital admission, such as wheezing7,8,61–65 or fever,8,66 parental atopy,7,61,67,68 as well as ventilation support7,61,63 or ICU transfer.8,61,64,65,69 However, the requirement of oxygen supplementation7,8,64,65 seemed more common in the RSV-induced LTRIs, while a personal history of eczema was more frequently linked to the RV-induced LTRIs.61,62,65,67,68 In light of these reports, there is lacking evidence to differentiate the etiology of LTRIs between RSV and RV LTRIs based solely on patients’ clinical presentation. Thus, the more widespread rapid respiratory virus testing of children with bronchiolitis is highly anticipated, especially for RV active infection.
Treatment
Currently, most guidelines recommend limiting bronchiolitis management only to supportive care, even at the hospital setting.1 However, in some international guidelines, there is permission to perform a trial of salbutamol treatment and continue the therapy in case of good clinical response.70–73 Despite being discouraged, salbutamol and systemic corticosteroids are reported to be used against the guidelines in managing bronchiolitis in both the hospital and emergency department settings, indicating an urgent need for the revision of current guidelines.74,75 The available evidence shows that inhaled beta2-mimetics are ineffective in terms of impact on oxygen saturation, length of hospital stay, and hospitalization rate.76,77 Systemic corticosteroids failed to prove efficacy in bronchiolitis and preschool wheezing management.
However, with the growing knowledge of the heterogeneity of bronchiolitis illness, it should be noted that the majority of the studies that were conducted investigated the interventions with the one-size-fits-all approach, regardless of its viral etiology or atopic status.77 Interestingly, a more personalized approach and asthma-like treatment (with systemic corticosteroids and beta2-agonists) in infants with RV-induced bronchiolitis have improved short- and long-term outcomes. However, a robust data is still lacking.68,78,79
In a randomized clinical trial of children with bronchiolitis, treatment with prednisolone was associated with less recurrent wheezing but only in subjects with a history of eczema or RV infection.80 The researchers supported this finding in their second study, which showed that children with a high rhinovirus load particularly benefitted from prednisolone.81 In a post-hoc analysis of two clinical trials with high-dose salbutamol, it has been found that it could be more effective in a subgroup of children with bronchiolitis. The study noticed shortened hospitalization in the RV-induced bronchiolitis group who received high-dose salbutamol compared to on-demand salbutamol or placebo.78 In addition, high-dose salbutamol combined with prednisolone was associated with a longer time to the new physician-confirmed wheezing episode than prednisolone alone or placebo.78 A post-hoc analysis of two clinical trials assessing the efficacy of high-dose salbutamol alone and high-dose salbutamol combined with oral prednisolone showed that the latter treatment was associated with a longer time to the new physician-confirmed wheezing episode than prednisolone alone or placebo. Therefore, suggesting a positive long-term effect of the interaction of salbutamol with oral steroids in infants with RV bronchiolitis.78
A recent study revealed that factors predicting the administration of albuterol prior to hospital admission included older age (6–12 months), previous salbutamol use, and wheezing.82
Conclusion
In summary, the modern view of bronchiolitis assumes early subtyping into at least 2–3 major entities depending on the viral etiology, lung microbiome, and type of immunologic response, as they have different pathogenetic mechanisms and slightly different clinical pictures. Bronchiolitis subtypes are associated with different risks of subsequent asthma and may have a different response to treatment (systemic corticosteroids, beta 2-agonists). Thanks to the COVID-19 pandemic, early general virological diagnosis has gained attention and become possible, significantly supporting bronchiolitis subtyping.
Therefore, we suggest a more individualized approach to patients with bronchiolitis, such as an earlier therapeutic trial with beta 2-agonists, regardless of etiology. In the case of severe rhinovirus-induced wheezing, also consider systemic corticosteroids. However, further research is needed to adjust individualized treatment for specific subtypes and develop strategies to follow up with patients at higher risk of asthma.
Acknowledgments
None.
Conflict of Interest
The authors declare that there are no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
REFERENCES
1. Ralston SL, Lieberthal AS, Meissner HC, Alverson BK, Baley JE, Gadomski AM, et al. Clinical practice guideline: The diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134(5):e1474–502. 10.1542/peds.2014-2742
2. Mahant S, Parkin PC, Thavam T, Imsirovic H, Tuna M, Knight B, et al. Rates in bronchiolitis hospitalization, intensive care unit use, mortality, and costs from 2004 to 2018. JAMA Pediatr. 2022;176(3):270–9. 10.1001/jamapediatrics.2021.5177
3. Régnier SA, Huels J. Association between respiratory syncytial virus hospitalizations in infants and respiratory sequelae: Systematic review and meta-analysis. Pediatr Infect Dis J. 2013;32(8):820–6. 10.1097/INF.0b013e31829061e8
4. Makrinioti H, Hasegawa K, Lakoumentas J, Xepapadaki P, Tsolia M, Castro-Rodriguez JA, et al. The role of respiratory syncytial virus-and rhinovirus-induced bronchiolitis in recurrent wheeze and asthma—A systematic review and meta--analysis. Pediatr Allergy Immunol. 2022;33(3):e13741. 10.1111/pai.13741
5. Sander B, Finkelstein Y, Lu H, Nagamuthu C, Graves E, Ramsay LC, et al. Healthcare cost attributable to bronchiolitis: A population-based cohort study. PLoS One. 2021;16(12):e0260809. 10.1371/journal.pone.0260809
6. Díez-Gandía E, Gómez-Álvarez C, López-Lacort M, Muñoz-Quiles C, Úbeda-Sansano I, Díez-Domingo J, et al. The impact of childhood RSV infection on children’s and parents’ quality of life: A prospective multicenter study in Spain. BMC Infect Dis. 2021;21(1):924. 10.1186/s12879-021-06629-z
7. Mansbach JM, Clark S, Teach SJ, Gern JE, Piedra PA, Sullivan AF, et al. Children hospitalized with rhinovirus bronchiolitis have asthma-like characteristics. J Pediatr. 2016;172:202–4.e1. 10.1016/j.jpeds.2016.01.041
8. Haddadin Z, Rankin DA, Lipworth L, Suh M, McHenry R, Blozinski A, et al. Respiratory virus surveillance in infants across different clinical settings. J Pediatr. 2021;234:164–71.e2. 10.1016/j.jpeds.2021.03.036
9. Mansbach JM, Piedra PA, Teach SJ, Sullivan AF, Forgey T, Clark S, et al. Prospective multicenter study of viral etiology and hospital length of stay in children with severe bronchiolitis. Arch Pediatr Adolesc Med. 2012;166(8):700–6. 10.1001/archpediatrics.2011.1669
10. Kenmoe S, Kengne-Nde C, Ebogo-Belobo JT, Mbaga DS, Fatawou Modiyinji A, Njouom R. Systematic review and meta-analysis of the prevalence of common respiratory viruses in children < 2 years with bronchiolitis in the pre-COVID-19 pandemic era. PLoS One. 2020;15(11):e0242302. 10.1371/journal.pone.0242302
11. Smyth RL, Openshaw PJ. Bronchiolitis. Lancet. 2006; 368(9532): 312–22. 10.1016/S0140-6736(06)69077-6
12. Hall CB, Weinberg GA, Blumkin AK, Edwards KM, Staat MA, Schultz AF, et al. Respiratory syncytial virus-associated hospitalizations among children less than 24 months of age. Pediatrics. 2013;132(2):e341–8. 10.1542/peds.2013-0303
13. Wrotek A, Czajkowska M, Jackowska T. Seasonality of respiratory syncytial virus hospitalization. Adv Exp Med Biol. 2020;1279:93–100. 10.1007/5584_2020_503
14. Sirimi N, Miligkos M, Koutouzi F, Petridou E, Siahanidou T, Michos A. Respiratory syncytial virus activity and climate parameters during a 12-year period. J Med Virol. 2016;88(6):931–7. 10.1002/jmv.24430
15. Hasegawa K, Goto T, Hirayama A, Laham FR, Mansbach JM, Piedra PA, et al. Respiratory virus epidemiology among US infants with severe bronchiolitis: Analysis of 2 multicenter, multiyear cohort studies. Pediatr Infect Dis J. 2019;38(8):e180–e3. 10.1097/INF.0000000000002279
16. Grochowska M, Ambrożej D, Wachnik A, Demkow U, Podsiadły E, Feleszko W. The impact of the COVID-19 pandemic lockdown on pediatric infections—A single-center retrospective study. Microorganisms. 2022;10(1):178. 10.3390/microorganisms10010178
17. Haapanen M, Renko M, Artama M, Kuitunen I. The impact of the lockdown and the re-opening of schools and day cares on the epidemiology of SARS-CoV-2 and other respiratory infections in children—A nationwide register study in Finland. EClinicalMedicine. 2021;34:100807. 10.1016/j.eclinm.2021.100807
18. Maglione M, Pascarella A, Botti C, Ricci G, Morelli F, Camelia F, et al. Changing epidemiology of acute viral respiratory infections in hospitalized children: The post-lockdown effect. Children (Basel). 2022;9(8):1242. 10.3390/children9081242
19. Berdah L, Romain AS, Rivière S, Schnuriger A, Perrier M, Carbajal R, et al. Retrospective observational study of the influence of the COVID-19 outbreak on infants’ hospitalisation for acute bronchiolitis. BMJ Open. 2022;12(10):e059626. 10.1136/bmjopen-2021-059626
20. van Summeren J, Meijer A, Aspelund G, Casalegno JS, Erna G, Hoang U, et al. Low levels of respiratory syncytial virus activity in Europe during the 2020/21 season: What can we expect in the coming summer and autumn/winter? Euro Surveill. 2021;26(29):2100639. 10.2807/1560-7917.ES.2021.26.29.2100639
21. Brisca G, Mariani M, Buratti S, Ferretti M, Pirlo D, Buffoni I, et al. How has the SARS-CoV-2 pandemic changed the epidemiology and management of acute bronchiolitis? Pediatr Pulmonol. 2023. 10.1002/ppul.26315
22. Billard MN, Bont LJ. Quantifying the RSV immunity debt following COVID-19: A public health matter. Lancet Infect Dis. 2023;23(1):3–5. 10.1016/S1473-3099(22)00544-8
23. Guedj R, Lorrot M, Lecarpentier T, Leger PL, Corvol H, Carbajal R. Infant bronchiolitis dramatically reduced during the second French COVID-19 outbreak. Acta Paediatr. 2021;110(4):1297–9. 10.1111/apa.15780
24. Movva N, Suh M, Reichert H, Hintze B, Sendak MP, Wolf Z, et al. Respiratory syncytial virus during the COVID-19 pandemic compared to historic levels: A retrospective cohort study of a health system. J Infect Dis. 2022;226(Suppl 2):S175–S183. 10.1093/infdis/jiac220
25. Jartti T, Smits HH, Bønnelykke K, Bircan O, Elenius V, Konradsen JR, et al. Bronchiolitis needs a revisit: Distinguishing between virus entities and their treatments. Allergy. 2019;74(1):40–52. 10.1111/all.13624
26. Rubner FJ, Jackson DJ, Evans MD, Gangnon RE, Tisler CJ, Pappas TE, et al. Early life rhinovirus wheezing, allergic sensitization, and asthma risk at adolescence. J Allergy Clin Immunol. 2017;139(2):501–7. 10.1016/j.jaci.2016.03.049
27. Lukkarinen M, Koistinen A, Turunen R, Lehtinen P, Vuorinen T, Jartti T. Rhinovirus-induced first wheezing episode predicts atopic but not nonatopic asthma at school age. J Allergy Clin Immunol. 2017;140(4):988–95. 10.1016/j.jaci.2016.12.991
28. Bergroth E, Aakula M, Elenius V, Remes S, Piippo-Savolainen E, Korppi M, et al. Rhinovirus type in severe bronchiolitis and the development of asthma. J Allergy Clin Immunol Pract. 2020;8(2):588–95.e4. 10.1016/j.jaip.2019.08.043
29. Meissner HC. Viral bronchiolitis in children. N Engl J Med. 2016;374(1):62–72. 10.1056/NEJMra1413456
30. Jackson DJ, Gern JE. Rhinovirus infections and their roles in asthma: Etiology and exacerbations. J Allergy Clin Immunol Pract. 2022;10(3):673–81. 10.1016/j.jaip.2022.01.006
31. Tacon CE, Wiehler S, Holden NS, Newton R, Proud D, Leigh R. Human rhinovirus infection up-regulates MMP-9 production in airway epithelial cells via NF-{kappa}B. Am J Respir Cell Mol Biol. 2010;43(2):201–9. 10.1165/rcmb.2009-0216OC
32. Skevaki CL, Psarras S, Volonaki E, Pratsinis H, Spyridaki IS, Gaga M, et al. Rhinovirus-induced basic fibroblast growth factor release mediates airway remodeling features. Clin Transl Allergy. 2012;2(1):14. 10.1186/2045-7022-2-14
33. XuChen X, Weinstock J, Arroyo M, Salka K, Chorvinsky E, Abutaleb K, et al. Airway remodeling factors during-early-life rhinovirus infection and the effect of premature birth. Front Pediatr. 2021;9:610478. 10.3389/fped.2021.610478
34. Ruiz S, Calvo C, Pozo F, Casas I, García-García ML. Lung function, allergic sensitization and asthma in school-aged children after viral-coinfection bronchiolitis. Sci Rep. 2022;12(1):7552. 10.1038/s41598-022-11356-9
35. Everman JL, Sajuthi S, Saef B, Rios C, Stoner AM, Numata M, et al. Functional genomics of CDHR3 confirms its role in HRV-C infection and childhood asthma exacerbations. J Allergy Clin Immunol. 2019;144(4):962-71. 10.1016/j.jaci.2019.01.052
36. Bønnelykke K, Sleiman P, Nielsen K, Kreiner-Møller E, Mercader JM, Belgrave D, et al. A genome-wide association study identifies CDHR3 as a susceptibility locus for early childhood asthma with severe exacerbations. Nat Genet. 2014;46(1):51–5. 10.1038/ng.2830
37. Calışkan M, Bochkov YA, Kreiner-Møller E, Bønnelykke K, Stein MM, Du G, et al. Rhinovirus wheezing illness and genetic risk of childhood-onset asthma. N Engl J Med. 2013;368(15):1398–407. 10.1056/NEJMoa1211592
38. Jartti T, Kuusipalo H, Vuorinen T, Söderlund-Venermo M, Allander T, Waris M, et al. Allergic sensitization is associated with rhinovirus-, but not other virus-, induced wheezing in children. Pediatr Allergy Immunol. 2010;21(7):1008–14. 10.1111/j.1399-3038.2010.01059.x
39. Pelletier JH, Au AK, Fuhrman D, Clark RSB, Horvat C. Trends in bronchiolitis ICU admissions and ventilation practices: 2010–2019. Pediatrics. 2021;147(6):e2020039115. 10.1542/peds.2020-039115
40. Mammas IN, Drysdale SB, Rath B, Theodoridou M, Papaioannou G, Papatheodoropoulou A, et al. Update on current views and advances on RSV infection (Review). Int J Mol Med. 2020;46(2):509–20. 10.3892/ijmm.2020.4641
41. Stevens TP, Sinkin RA, Hall CB, Maniscalco WM, McConnochie KM. Respiratory syncytial virus and premature infants born at 32 weeks’ gestation or earlier: hospitalization and economic implications of prophylaxis. Arch Pediatr Adolesc Med. 2000;154(1):55–61.
42. Do LAH, Pellet J, van Doorn HR, Tran AT, Nguyen BH, Tran TTL, et al. Host transcription profile in nasal epithelium and whole blood of hospitalized children under 2 years of age with respiratory syncytial virus infection. J Infect Dis. 2017;217(1):134–46. 10.1093/infdis/jix519
43. Mejias A, Dimo B, Suarez NM, Garcia C, Suarez-Arrabal MC, Jartti T, et al. Whole blood gene expression profiles to assess pathogenesis and disease severity in infants with respiratory syncytial virus infection. PLoS Med. 2013;10(11):e1001549. 10.1371/journal.pmed.1001549
44. Heinonen S, Jartti T, Garcia C, Oliva S, Smitherman C, Anguiano E, et al. Rhinovirus detection in symptomatic and asymptomatic children: Value of host transcriptome analysis. Am J Respir Crit Care Med. 2016;193(7):772–82. 10.1164/rccm.201504-0749OC
45. Jansen RR, Wieringa J, Koekkoek SM, Visser CE, Pajkrt D, Molenkamp R, et al. Frequent detection of respiratory viruses without symptoms: Toward defining clinically relevant cutoff values. J Clin Microbiol. 2011;49(7):2631–6. 10.1128/JCM.02094-10
46. Rhedin S, Lindstrand A, Rotzén-Östlund M, Tolfvenstam T, Ohrmalm L, Rinder MR, et al. Clinical utility of PCR for common viruses in acute respiratory illness. Pediatrics. 2014;133(3):e538–45. 10.1542/peds.2013-3042
47. van Benten I, Koopman L, Niesters B, Hop W, van Middelkoop B, de Waal L, et al. Predominance of rhinovirus in the nose of symptomatic and asymptomatic infants. Pediatr Allergy Immunol. 2003;14(5):363–70. 10.1034/j.1399-3038.2003.00064.x
48. van den Bergh MR, Biesbroek G, Rossen JW, de Steenhuijsen Piters WA, Bosch AA, van Gils EJ, et al. Associations between pathogens in the upper respiratory tract of young children: Interplay between viruses and bacteria. PLoS One. 2012;7(10):e47711. 10.1371/journal.pone.0047711
49. de Steenhuijsen Piters WA, Heinonen S, Hasrat R, Bunsow E, Smith B, Suarez-Arrabal MC, et al. Nasopharyngeal microbiota, host transcriptome, and disease severity in children with respiratory syncytial virus infection. Am J Respir Crit Care Med. 2016;194(9):1104–15. 10.1164/rccm.201602-0220OC
50. van den Kieboom CH, Ahout IM, Zomer A, Brand KH, de Groot R, Ferwerda G, et al. Nasopharyngeal gene expression, a novel approach to study the course of respiratory syncytial virus infection. Eur Respir J. 2015;45(3):718–25. 10.1183/09031936.00085614
51. Fujiogi M, Raita Y, Pérez-Losada M, Freishtat RJ, Celedón JC, Mansbach JM, et al. Integrated relationship of nasopharyngeal airway host response and microbiome associates with bronchiolitis severity. Nat Commun. 2022;13(1):4970. 10.1038/s41467-022-32323-y
52. Rodriguez-Fernandez R, Tapia LI, Yang CF, Torres JP, Chavez-Bueno S, Garcia C, et al. Respiratory syncytial virus genotypes, host immune profiles, and disease severity in young children hospitalized with bronchiolitis. J Infect Dis. 2017;217(1):24–34. 10.1093/infdis/jix543
53. Fujiogi M, Camargo CA, Jr., Raita Y, Bochkov YA, Gern JE, Mansbach JM, et al. Association of rhinovirus species with nasopharyngeal metabolome in bronchiolitis infants: A multicenter study. Allergy. 2020;75(9):2379–83. 10.1111/all.14326
54. Brealey JC, Chappell KJ, Galbraith S, Fantino E, Gaydon J, Tozer S, et al. Streptococcus pneumoniae colonization of the nasopharynx is associated with increased severity during respiratory syncytial virus infection in young children. Respirology. 2018;23(2):220–7. 10.1111/resp.13179
55. Zhu Z, Camargo CA, Jr., Raita Y, Fujiogi M, Liang L, Rhee EP, et al. Metabolome subtyping of severe bronchiolitis in infancy and risk of childhood asthma. J Allergy Clin Immunol. 2022;149(1):102–12. 10.1016/j.jaci.2021.05.036
56. Fujiogi M, Zhu Z, Raita Y, Ooka T, Celedon JC, Freishtat R, et al. Nasopharyngeal lipidomic endotypes of infants with bronchiolitis and risk of childhood asthma: A multicentre prospective study. Thorax. 2022;7(11):1059–69. 10.1136/thorax-2022-219016
57. Raita Y, Camargo CA, Jr., Bochkov YA, Celedón JC, Gern JE, Mansbach JM, et al. Integrated-omics endotyping of infants with rhinovirus bronchiolitis and risk of childhood asthma. J Allergy Clin Immunol. 2021;147(6):2108–17. 10.1016/j.jaci.2020.11.002
58. Raita Y, Pérez-Losada M, Freishtat RJ, Harmon B, Mansbach JM, Piedra PA, et al. Integrated omics endotyping of infants with respiratory syncytial virus bronchiolitis and risk of childhood asthma. Nat Commun. 2021;12(1):3601. 10.1038/s41467-021-23859-6
59. Zhu Z, Camargo CA, Jr., Raita Y, Freishtat RJ, Fujiogi M, Hahn A, et al. Nasopharyngeal airway dual-transcriptome of infants with severe bronchiolitis and risk of childhood asthma: A multicenter prospective study. J Allergy Clin Immunol. 2022;150(4):806–16. 10.1016/j.jaci.2022.04.017
60. Fujiogi M, Dumas O, Hasegawa K, Jartti T, Camargo CA. Identifying and predicting severe bronchiolitis profiles at high risk for developing asthma: Analysis of three prospective cohorts. EClinicalMedicine. 2022;43:101257. 10.1016/j.eclinm.2021.101257
61. Takeyama A, Hashimoto K, Sato M, Sato T, Tomita Y, Maeda R, et al. Clinical and epidemiologic factors related to subsequent wheezing after virus-induced lower respiratory tract infections in hospitalized pediatric patients younger than 3 years. Eur J Pediatr. 2014;173(7):959–66. 10.1007/s00431-014-2277-7
62. Korppi M, Kotaniemi-Syrjänen A, Waris M, Vainionpää R, Reijonen TM. Rhinovirus-associated wheezing in infancy: Comparison with respiratory syncytial virus bronchiolitis. Pediatr Infect Dis J. 2004;23(11):995–9. 10.1097/01.inf.0000143642.72480.53
63. Arroyo M, Salka K, Perez GF, Rodríguez-Martínez CE, Castro-Rodriguez JA, Gutierrez MJ, et al. Phenotypical sub-setting of the first episode of severe viral respiratory infection based on clinical assessment and underlying airway disease: A pilot study. Front Pediatr. 2020;8:121. 10.3389/fped.2020.00121
64. Khuri-Bulos N, Lawrence L, Piya B, Wang L, Fonnesbeck C, Faouri S, et al. Severe outcomes associated with respiratory viruses in newborns and infants: A prospective viral surveillance study in Jordan. BMJ Open. 2018;8(5):e021898. 10.1136/bmjopen-2018-021898
65. Hasegawa K, Mansbach JM, Bochkov YA, Gern JE, Piedra PA, Bauer CS, et al. Association of rhinovirus C bronchiolitis and immunoglobulin E sensitization during infancy with development of recurrent wheeze. JAMA Pediatr. 2019;173(6):544–52. 10.1001/jamapediatrics.2019.0384
66. García-García ML, Calvo C, Moreira A, Cañas JA, Pozo F, Sastre B, et al. Thymic stromal lymphopoietin, IL-33, and periostin in hospitalized infants with viral bronchiolitis. Medicine (Baltimore). 2017;96(18):e6787. 10.1097/MD.0000000000006787
67. Jartti T, Aakula M, Mansbach JM, Piedra PA, Bergroth E, Koponen P, et al. Hospital length-of-stay is associated with rhinovirus etiology of bronchiolitis. Pediatr Infect Dis J. 2014;33(8):829–34. 10.1097/INF.0000000000000313
68. Jartti T, Lehtinen P, Vanto T, Hartiala J, Vuorinen T, Mäkelä MJ, et al. Evaluation of the efficacy of prednisolone in early wheezing induced by rhinovirus or respiratory syncytial virus. Pediatr Infect Dis J. 2006;25(6):482–8. 10.1097/01.inf.0000215226.69696.0c
69. Hasegawa K, Mansbach JM, Ajami NJ, Espinola JA, Henke DM, Petrosino JF, et al. Association of nasopharyngeal microbiota profiles with bronchiolitis severity in infants hospitalised for bronchiolitis. Eur Respir J. 2016;48(5):1329–39. 10.1183/13993003.00152-2016
70. Kirolos A, Manti S, Blacow R, Tse G, Wilson T, Lister M, et al. A systematic review of clinical practice guidelines for the diagnosis and management of bronchiolitis. J Infect Dis. 2020;222(Suppl 7):S672–S679. 10.1093/infdis/jiz600
71. Sistema General de Seguridad Social en Salud, Guíía de práctica clíínica para la evaluacióón del riesgo y manejo inicial de la neumoníía en niñños y niññas menores de 5 añños y bronquiolitis en niñños y niññas menores de 2 añños [Internet]. 2014 [cited
72. Instituto Mexicano del Seguro Social, Diagnóstico y tratamiento de bronquiolitis aguda en niñas/niños y en el primer nivel de atención [Internet]. 2015 [cited
73. Sociedad Argentina de Pediatría, Recomendaciones para el manejo de las infecciones respiratorias agudas bajas en menores de 2 años [Internet]. 2015 [cited
74. Rivera-Sepulveda AV, Rebmann T, Gerard J, Charney RL. Physician compliance with bronchiolitis guidelines in pediatric emergency departments. Clin Pediatr (Phila). 2019;58(9):1008–18. 10.1177/0009922819850462
75. House SA, Marin JR, Hall M, Ralston SL. Trends over time in use of nonrecommended tests and treatments since publication of the American Academy of Pediatrics Bronchiolitis Guideline. JAMA Netw Open. 2021;4(2):e2037356. 10.1001/jamanetworkopen.2020.37356
76. Cai Z, Lin Y, Liang J. Efficacy of salbutamol in the treatment of infants with bronchiolitis: A meta-analysis of 13 studies. Medicine (Baltimore). 2020;99(4):e18657. 10.1097/MD.0000000000018657
77. Gadomski AM, Scribani MB. Bronchodilators for bronchiolitis. Cochrane Database Syst Rev. 2014;2014(6):CD001266. 10.1002/14651858.CD001266.pub4
78. Hurme P, Homil K, Lehtinen P, Turunen R, Vahlberg T, Vuorinen T, et al. Efficacy of inhaled salbutamol with and without prednisolone for first acute rhinovirus-induced wheezing episode. Clin Exp Allergy. 2021;51(9):1121–32. 10.1111/cea.13960
79. Ambrożej D, Makrinioti H, Whitehouse A, Papadopoulos N, Ruszczyński M, Adamiec A, et al. Respiratory virus type to guide predictive enrichment approaches in the management of the first episode of bronchiolitis: A systematic review. Front Immunol. 2022;13:1017325. 10.3389/fimmu.2022.1017325
80. Lehtinen P, Ruohola A, Vanto T, Vuorinen T, Ruuskanen O, Jartti T. Prednisolone reduces recurrent wheezing after a first wheezing episode associated with rhinovirus infection or eczema. J Allergy Clin Immunol. 2007;119(3):570–5. 10.1016/j.jaci.2006.11.003
81. Jartti T, Nieminen R, Vuorinen T, Lehtinen P, Vahlberg T, Gern J, et al. Short-and long-term efficacy of prednisolone for first acute rhinovirus-induced wheezing episode. J Allergy Clin Immunol. 2015;135(3):691–8.e9. 10.1016/j.jaci.2014.07.001
82. Condella A, Mansbach JM, Hasegawa K, Dayan PS, Sullivan AF, Espinola JA, et al. Multicenter study of albuterol use among infants hospitalized with bronchiolitis. West J Emerg Med. 2018;19(3):475–83. 10.5811/westjem.2018.3.35837
83. Fujiogi M, Camargo CA, Jr., Bernot JP, Freishtat RJ, Harmon B, Mansbach JM, et al. In infants with severe bronchiolitis: Dual-transcriptomic profiling of nasopharyngeal microbiome and host response. Pediatr Res. 2020;88(2):144–6. 10.1038/s41390-019-0742-8