
Download
ORIGINAL ARTICLE
Correlation between B-cell lymphoma 6 with the balance of T helper-1/2 and severity of allergic rhinitis
Jiali Wua#, Shumei Chenb#, Xiaoyan Lib*
aDepartment of Pediatric Otolaryngology, Jiahui International Hospital, Shanghai, China
bDepartment of Otolaryngology and Head and Neck Surgery, Shanghai Children’s Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China
Abstract
Objective: Allergic rhinitis (AR) is a prevailing immune disorder affecting the nasal mucosa. B-cell lymphoma 6 (BCL6) imposes essential roles in immunity. This study probed into the serum expression of BCL6 and its effect on AR diagnosis and patients’ quality of life (QOL).
Methods: A total of 113 patients with AR including 38 cases with mild AR (MAR) and 75 cases with moderate-severe AR (MSAR) were enrolled, with 101 healthy people enrolled as control. Serum expression of BCL6 was detected by RT-qPCR and the diagnostic efficacy of BCL6 for AR was analyzed using the receiver operating characteristic curve. The proportion of T helper-1/2 (Th1/Th2) cells in CD4+ T cells in peripheral blood mononuclear cells was detected using flow cytometry. The correlation between BCL6 and Th1/Th2 cells and the effects of BCL6 expression on patients’ QOL were assessed by Pearson analysis and Mini-RQLQ questionnaire.
Results: BCL6 was downregulated in patients with AR, serum BCL6 level < 0.8450 had certain auxiliary diagnostic values for AR, and serum BCL6 level < 0.5400 could assist the diagnosis of AR severity. Th1 cell proportion in CD4+ T cells was decreased, whereas Th2 cell proportion was increased with AR severity. BCL6 was positively-linked with Th1 cells but inversely-correlated with Th2 cells in patients with AR. Patients with AR with low BCL6 expression had a poorer QOL compared with high BCL6 expression. The domains most affected by BCL6 expression were practical problems, nasal symptoms, and lacrimation.
Conclusion: Serum BCL6 is downregulated and low BCL6 expression greatly deteriorates QOL in patients with AR.
Key words: Allergic rhinitis, B-cell lymphoma 6, minirhinoconjunctivitis quality-of-life questionnaire, Pearson analysis, quality-of-life, receiver operating characteristics, T helper-1/2
*Corresponding author: Xiaoyan Li, Department of Otolaryngology and Head and Neck Surgery, Shanghai Children’s Hospital, Shanghai Jiaotong University School of Medicine, 355 Luding Road, Putuo, Shanghai 200062, China. Email address: [email protected]
#Jiali Wu and Shumei Chen contributed equally to this work.
Received 18 May 2022; Accepted 22 June 2022; Available online 1 January 2023
Copyright: Wu J, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Allergic rhinitis (AR), commonly affecting the nasal mucosa, represents a relatively homogeneous condition featured by eosinophilic inflammation owing to the immunoglobulin E (IgE)-sensitization to perennial or seasonal aeroallergens.1,2 AR, occurring with or without conjunctivitis, is normally manifested with symptoms of sneezing, nasal obstruction, rhinorrhea, and rhinocnesmus, which considerably affects the quality of life (QOL).3 AR is estimated to affect 40% of the global population, which causes huge economic burden, amounting to several billion dollars annually.4,5 The etiology of AR is interrelated to environmental, epigenetic, and genetic factors.6 Current treatment options for AR include pharmacotherapy and immunotherapy.7,8 As indicated in allergic rhinitis and its impact on asthma (ARIA) guidelines, oral antihistamines and nasal decongestants are the first-line drugs for mild to moderate AR. In more severe AR, second-line drugs such as intranasal corticosteroids or allergen immunotherapy may be used.9However, the objective measures employed for the differential diagnosis and severity evaluation of AR are still rare,10 warranting novel and potent biomarkers for AR.
T helper-1 (Th1) cells for cell-mediated immunity and T helper-2 (Th2) for humoral immunity are considered two different Th cell types with distinct cytokine patterns, and the imbalance between Th1 and Th2 cells is recognized as a vital pathological mechanism of AR.11 Indeed, AR is driven by Th2.12 The Th2 cytokine interleukin (IL)-4 facilitates class switching to the IgE antibody, which binds to the FcεRI (high-affinity IgE receptor) on mast cells. Contrastingly, Th1 reaction and the prototypic cytokine interferon (IFN)-γ could counterbalance Th2 responses, thus reducing the generation of IL-4 and IgE and ultimately inhibiting allergic sensitization.13 Regulating
Th1/Th2 balance exerts certain roles in mitigating allergic inflammatory responses in ovalbumin-elicited AR mice.14 From the aforementioned research, we can learn the paramount significance of the Th1/Th2 balance in AR.
B-cell lymphoma 6 (BCL6) is considered a sequence-specific transcriptional mediator that suppresses the target gene transcription via binding to specific DNA sequences in promoter regions.15,16 BCL6 is imperative in the development of B cells, follicular Th cells, and T regulatory cells, indicating its potential function in regulating immune responses.17–19 The transcriptional repressor BCL6 can regulate the fate of Th cells and prevent Th2-type inflammation.20 Additionally, BCL6 likely imposes multiple roles in allergic diseases that are characterized by the production of allergen-specific IgE and Th2 cytokines (IL-4, IL-5, and IL-13), and mice with germline deletion of BCL6 exhibit aggravated allergic inflammation, partly due to BCL6 deficiency in T regulatory cell populations contributing to increased Th2 cytokines and expressions of genes, such as IL1RL1, that is overexpressed in multimorbidity for rhinitis, asthma, and dermatitis.18,21 Nevertheless, the studies about the correlation of BCL6 with Th1/Th2 balance and AR severity in patients with AR are still lacking. Therefore, this study examined the expression of BCL6 in the serum and investigated its effects on AR diagnosis and patients’ QOL.
Methods
Ethics statement
This study was ratified by the ethics committee of Shanghai Children’s Hospital, Shanghai Jiaotong University School of Medicine. All participants had signed the informed consent.
Study subjects
We recruited 113 patients with AR in Shanghai Children’s Hospital, Shanghai Jiaotong University School of Medicine between January 2020 and August 2021, and additional 101 age- and sex-matched healthy people with no allergic diseases as the control group. The diagnosis of AR was conducted by the allergist based on the ARIA guidelines.22 All patients with AR were in concert with the following inclusion criteria: persistent AR; medical history and allergic symptoms (such as sneezing, rhinorrhea, nasal obstruction, and rhinocnesmus) for > 2 years; a positive skin test for Dermatophagoides farina and/or Dermatophagoides pteronyssinus (a mean wheal diameter > 3 mm) and/or positive specific IgE (> 0.35 IU/mL).
All patients were interviewed briefly and we excluded those patients with smoking, other allergic diseases, systemic steroid therapy, inflammatory or septic diseases, autoimmune diseases, pregnancy, immunotherapy, and use of antiallergic drugs within 4 weeks before the study. In addition, the demographic and clinical data of study subjects were collected, including sex, age, body mass index (BMI), disease duration, and serum total IgE levels. The patients with AR were assigned to the mild AR group (MAR group, N = 38) and moderate-severe AR group (MSAR group, N = 75) according to ARIA guidelines.22
Assessment of AR symptoms
The symptoms of all participants were scored based on the widely accepted total nasal symptom score (TNSS).23 The score was the sum of following 4 symptom scores: sneezing, rhinorrhea, nasal obstruction, and rhinocnesmus, with each symptom score recorded from 0 to 3 (0 = no symptoms, 1 = minimal and tolerable symptoms, 2 = troublesome but tolerable symptoms, and 3 = severe and intolerable symptoms). The possible obtained score of patients with AR was ranged from 0 (no symptoms) to 12 (the highest symptom intensity). The fasting venous blood was collected from the elbow of participants at enrollment, and the serum was separated within 2 h and transferred to a special cryopreservation tube in a -80°C freezer until use.
Determination of Th1 and Th2 cell levels
The peripheral blood mononuclear cells (PBMCs) were isolated from peripheral blood samples of participants by gradient density centrifugation, and the proportion of Th1 and Th2 cells in CD4+ T cells in patients with AR was analyzed by a multicolor flow cytometer using commercial human cell differentiation kits (Bio-Techne, Minneapolis, MN, USA). Briefly, after stimulation, Th cells were stained with specific fluorescent antibodies and then counted by the fluorescence-activated cell sorting flow cytometer with anti-human IFN-γ antibody and anti-human IL-4 antibody (Bio-Techne). The proportion of Th1 and Th2 cells in CD4+ T cells was calculated sequentially.
Measurement of serum IFN-γ, IL-2, IL-4, and IL-10 concentrations
Serum was isolated from the peripheral blood samples of participants. The serum levels of Th1 cell cytokines (IFN-γ and IL-2) and Th2 cell cytokines (IL-4 and IL-10) were determined using commercial human enzyme-linked immunosorbent assay kits (Bio-Techne).
Reverse transcription quantitative polymerase chain reaction (RT-qPCR)
The expression of BCL6 in PBMCs was detected utilizing RT-qPCR assay. Total RNA was extracted by the RNeasy Protect Mini kit (Qiagen, Hilden, Germany), followed by reserve transcription utilizing the PrimeScriptTM RT kit (Takara, Kyoto, Japan). Afterward, qPCR was conducted by KOD SYBR® qPCR Mix (Toyobo, Osaka, Japan). The relative expression of BCL6 was computed using the 2-ΔΔCt method,24 with glyceraldehyde-3-phosphate dehydrogenase (GAPDH) as the internal control. Primer sequences are exhibited in Table 1.
Table 1 Primer sequences.
| Gene | Forward 5'–3' | Reverse 5'–3' |
|---|---|---|
| BCL-6 | 5'-AGCAAGGCATTGGTGAAGACA-3' | 5'-ATGGCGGGTGAACTGGATAC-3' |
| GAPDH | 5'-CCCACTCCTCCACCTTTGAC-3' | 5'-CATACCAGGAAATGAGCTTGACAA-3' |
Note: BCL6, B-cell lymphoma 6; GAPDH, glyceraldehyde-3-phosphate dehydrogenase.
QOL survey of patients with AR
The impact of AR on QOL of patients was assessed by the Arabic validated version of the mini-rhinoconjunctivitis quality of life questionnaire (Mini-RQLQ), including five domains: activity, practical problems, nasal symptoms, ocular symptoms, and other symptoms. The original version of this questionnaire was designed by Juniper EF et al. in 1991,25 including 28 items. Furthermore, the Arabic version was verified by AbuRuz et al. in 2009.26 Like RQLQ, all items in Mini-RQLQ were equally weighted and the analysis was performed the same way as RQLQ.
The patients with AR were invited to answer each question using a 7-point scale (0 = not bothered, 6 = extremely bothered). The item of each domain was added to reproduce the score from 0 to 6, where 0 indicated the best QOL score and 6 indicated the worst QOL score. The questionnaires were directly analyzed from the recorded scores, and the results were exhibited as the mean score for each item in each domain and the overall QOL. The overall QOL score was estimated from the average score of all items.
Statistical analysis
SPSS 24.0 (IBM Corp. Armonk, NY, USA) and GraphPad Prism 6.01 (GraphPad Software Inc., San Diego, CA, USA) were applied for statistical analysis and graph construction. Data were displayed as mean ± standard deviation (SD) for normally distributed continuous variables; data were described as the median and interquartile range (IQR) for non-normally distributed variables, and data were expressed as number (percentage) for categorical variables. The Kolmogorov–Smirnov test was used to assess the normality of the distribution in continuous variables. When variables were normally distributed, one-way analysis of variance (ANOVA) or independent samples t-test was used for testing, otherwise, the Kruskal–Wallis H test or Mann–Whitney U test was applied. Receiver operating characteristic (ROC) curve was used to analyze the diagnostic value of BCL6 for AR and the severity of patients with AR. Pearson correlation was adopted to analyze the correlation between the serum BCL6 expression and Th1 and Th2 cells in patients with AR. The p value was obtained from a two-sided test and p < 0.05 was considered statistically significant.
Results
Clinical baseline data of participants
The quantity and clinical information of participants are shown in Table 2. The control group, MAR group, and MSAR group showed no evident difference in sex, age, BMI, and disease duration (p > 0.05). Compared with the control and MAR groups, the MSAR group had prominently elevated levels of serum total IgE, TNSS, IL-4, and IL-10, but reduced levels of IFN-γ and IL-2 (all p < 0.05).
Table 2 Clinical baseline data of participants.
| Control(n = 101) | MAR (n = 38) | MSAR(n = 75) | |
|---|---|---|---|
| Age | 29.73 ± 6.15 | 29.19 ± 7.57 | 30.66 ± 6.15 |
| Sex (Male/percentage) | 52/51.49% | 21/55.26% | 38/50.67% |
| Disease duration (years) | NA | 3.93 (3.48-4.67) | 4.57 (3.3-5.38) |
| BMI | 22.96 ± 2.18 | 22.16 ± 2.34 | 22.75 ± 1.88 |
| Serum total IgE (IU/mL) | 75.05 (59.74-94.45) | 241.72 (231.89-251.92)a | 359.25 (342.86-385.05)ab |
| TNSS | NA | 4 (3-5) | 6 (4-10)b |
| IFN-γ (ng/mL) | 6.10 (5.94-6.25) | 3.58 (2.66-4.46)a | 3.28 (2.39-3.66)ab |
| IL-2 (ng/mL) | 5.50 (4.30-6.96) | 2.87 (1.78-3.73)a | 2.55 (1.52-3.49)ab |
| IL-4 (pg/mL) | 5.67 (3.52-8.38) | 57.97 (48.14-72.57)a | 81.59 (56.90-98.46)ab |
| IL-10 (pg/mL) | 4.74 (2.10-6.52) | 56.26 (36.84-91.1)a | 71.94 (55.58-80.4)ab |
Note: MAR, mild allergic rhinitis; MASR, moderate-severe allergic rhinitis; BMI, body mass index; IgE, immunoglobulin E; TNSS, total nasal symptom score; IFN, interferon; IL, interleukin.
Data were presented as mean ± SD for normally distributed continuous variables; data were expressed as median and IQR for non-normally distributed variables, and data were shown as number (percentage) for categorical variables. a: p < 0.05 vs control group, b: p < 0.05 vs MAR group.
Diagnostic value of BCL6 for AR
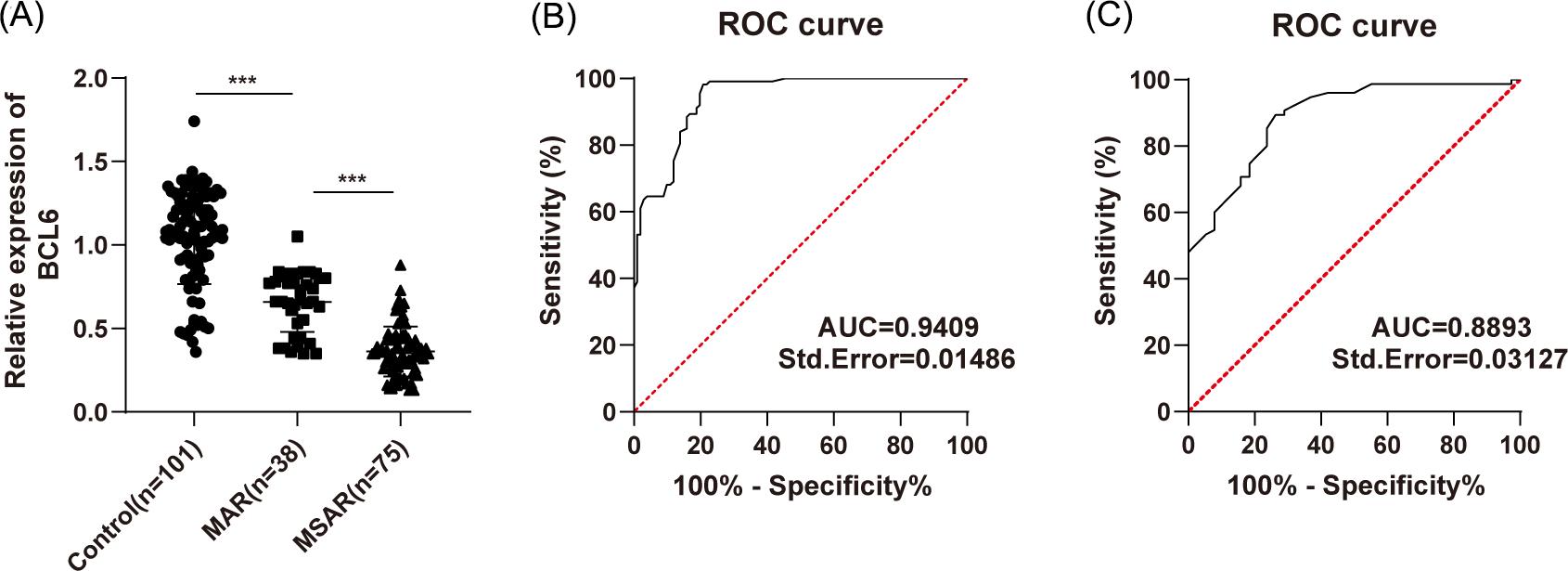
This study enrolled 113 patients with AR (38 patients with MAR and 75 patients with MSAR) and additional 101 healthy people as control, and we detected BCL6 expression in the serum by RT-qPCR, which indicated a notably reduced BCL6 expression in patients with AR compared with controls (p < 0.001, Figure 1A). Subsequently, to investigate the diagnostic value of serum BCL6 expression for AR, we plotted the ROC curve for distinguishing patients with AR from healthy people by BCL6 expression (p < 0.0001, Figure 1B). It revealed that the area under the curve (AUC) was 0.9409 and the cut-off value was 0.8450 (98.23% sensitivity and 79.21% specificity), indicating that serum BCL6 level < 0.8450 has certain auxiliary diagnostic values for AR. In addition, we interrogated the diagnostic value of serum BCL6 expression for the severity of AR and plotted the ROC curve to distinguish patients with MAR from patients with MSAR by BCL6 expression (p < 0.0001, Figure 1C). It was noted that the AUC was 0.8893 and the cut-off value was 0.5400 (89.33% sensitivity and 73.68% specificity), demonstrating that serum BCL6 level < 0.5400 could assist the diagnosis of AR severity.
Figure 1 Diagnostic value of BCL6 for AR. (A) RT-qPCR detected the serum expression of BCL6; (B) ROC analysis assessed the diagnostic efficacy of BCL6 for patients with AR; (C) ROC analysis assessed the diagnostic efficacy of BCL6 for the severity of patients with AR. One way ANOVA test was used for (A) and ROC analysis was used for (B/C). ***p < 0.001.
Correlation between BCL6 and Th1/Th2
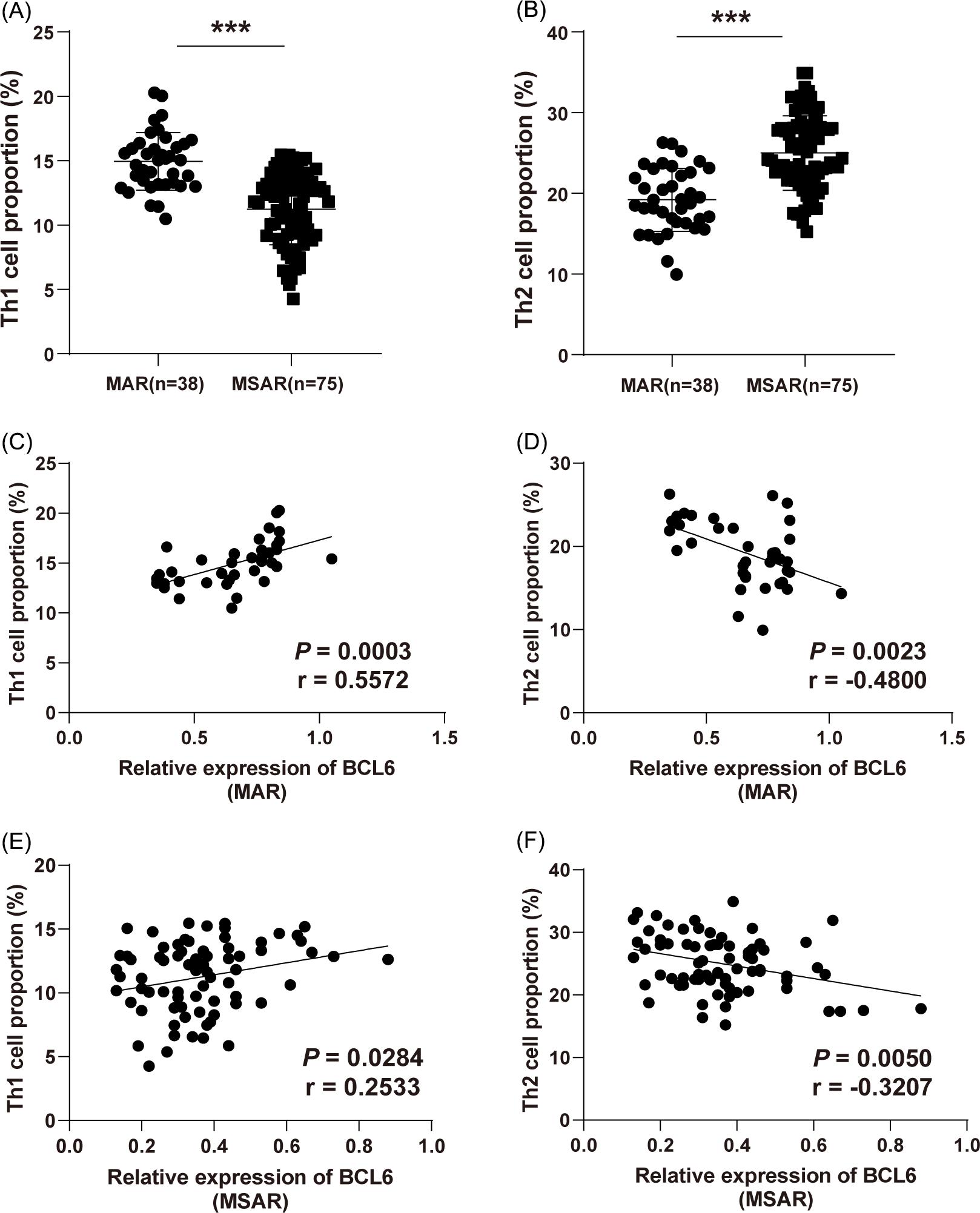
Th1/Th2 imbalance is a major contributor to the increased risk of AR,27 herein, the proportion of Th1 and Th2 cells in CD4+ T cells in PBMCs from patients with AR was detected using flow cytometry. The results revealed that the proportion of Th1 cells was decreased with AR severity, whereas the proportion of Th2 cells was raised with AR severity (Figure 2A,B). In terms of BCL6 expression in patients with MAR and MSAR, BCL6 expression was positively related to Th1 cells (r = 0.5572, p = 0.0003; r = 0.2533, p = 0.0284) (Figure 2C,E) and negatively correlated with Th2 cells (r = −0.4800, p = 0.0023; r = −0.3207, p = 0.0050) (Figure 2D,F).
Figure 2 Correlation between BCL6 and Th1/Th2. (A,B) The proportion of Th1 and Th2 cells in patients with AR; (C,D) The correlation between BCL6 and Th1/Th2 cells in patients with MAR; (E,F) The correlation between BCL6 and Th1/Th2 cells in patients with MSAR. An independent samples t-test was applied for (A/B). ***p < 0.001.
BCL6 low expression affected QOL of patients with AR
To investigate the effect of BCL6 expression on the QOL of patients with AR, we allocated patients with AR into the high and low BCL6 expression groups according to the median 0.39 (0.13–1.05) of serum BCL6 expression in patients with AR and invited patients with AR to participate in the Mini-RQLQ questionnaire. As shown in Table 3, the QOL score was 2.21 ± 0.40 in patients with AR with high BCL6 expression and 2.88 ± 0.40 in patients with AR with low BCL6 expression (p < 0.001). Among these, the domains most affected by BCL6 expression were practical problems, nasal symptoms, and lacrimation (all p < 0.01).
Table 3 BCL6 low expression affected QOL of patients with AR.
| patients with AR | P value | |||
|---|---|---|---|---|
| BCL6 high expression | BCL6 low expression | |||
| Activity limitations | Regular activity | 2.31 ± 1.33 | 2.68 ± 1.18 | 0.1138 |
| Recreational activity | 2.83 ± 1.06 | 3.16 ± 1.75 | 0.2228 | |
| Sleeping | 2.78 ± 1.26 | 3.02 ± 1.48 | 0.0962 | |
| Practical problems | Rubbing the nose/eye | 2.17 ± 1.49 | 3.53 ± 1.79 | < 0.001 |
| Blowing the nose | 1.95 ± 1.43 | 3.51 ± 1.45 | < 0.001 | |
| Nasal symptoms | Sneezing | 2.41 ± 1.40 | 3.40 ± 1.70 | < 0.001 |
| Nasal obstruction | 2.16 ± 1.46 | 3.49 ± 1.81 | < 0.001 | |
| Rhinorrhea | 2.16 ± 1.31 | 3.58 ± 1.91 | < 0.001 | |
| Ocular symptoms | Itchy eyes | 1.47 ± 1.22 | 1.61 ± 1.03 | 0.4819 |
| Eye pain | 1.34 ± 1.02 | 1.44 ± 1.13 | 0.6416 | |
| Lacrimation | 1.47 ± 1.06 | 2.01 ± 0.92 | 0.0035 | |
| Other symptoms | Fatigue | 2.34 ± 1.04 | 2.65 ± 1.36 | 0.1785 |
| Thirsty | 2.57 ± 1.09 | 2.84 ± 1.77 | 0.3209 | |
| Dysphoria | 3.10 ± 1.41 | 3.39 ± 1.57 | 0.3115 | |
| Total QOL score | 2.21 ± 0.40 | 2.88 ± 0.40 | < 0.001 | |
Note: BCL6, B-cell lymphoma 6; QOL, quality of life; AR, allergic rhinitis.
Discussion
The prevalence of AR remains growing worldwide, accompanied by an increased frequency of hypersensitive reactions to numerous allergens, and the recognized features of AR are attributed to IgE-regulated responses to various inhaled allergens and Th2 cell-triggered mucosal inflammation.6 Moreover, AR negatively impacts QOL and most patients are deeply troubled by nasal symptoms.28 BCL6 is a primary mediator of humoral immunity, which exerts a substantial role in inflammation, mainly evidenced by suppressing IL-6 expression in macrophages.16 Hence, we analyzed the diagnostic efficacy of BCL6 and the impact on QOL in patients with AR.
It is noteworthy that BCL6-deficient mice occur serious and spontaneous Th2 inflammation.29 The protein and mRNA levels of BCL6 are reduced in the nasal mucosa of AR mice and BCL6 upregulation contributes to the deactivation of NLRP3 inflammasomes and alleviation of inflammatory responses.30 Accordingly, we determined the BCL6 expression in the serum and found a decreased BCL6 expression in patients with AR, consistent with former research. A recent report has supported the diagnostic value of BCL6 in lymphomas,31 but the application of BCL6 in AR diagnosis is rarely studied. Importantly, our tests elucidated that BCL6 level < 0.8450 could assist the diagnosis of AR, and a level < 0.5400 could aid the diagnosis of AR severity.
AR is an IgE-regulated response impelled by Th2 cells and AR rats exhibit elevated levels of IgE, IL-5, and IL-13.32 The occurrence of AR is closely associated with the breakdown of the Th1/Th2 balance, during which the allergen-caused Th2 immune responses predominate over the Th1 immune responses, contributing to IgE-mediated anaphylaxis.33 Accordingly, we compared the clinical data of enrolled participants and noted that IgE, TNSS, IL-4, and IL-10 levels were increased, whereas IFN-γ and IL-2 levels were reduced in patients with AR. Moreover, our results elicited that in CD4+ T cells, Th1 cells were diminished but Th2 cells were increased as AR severity increased. Intriguingly, after long-term treatment with sublingual house dust mite drops, the children with AR exhibit elevated IL-2 and TGF-β1 but lowered IL-4 and IL-17α.34 Maintaining Th1/Th2 balance can ameliorate allergic inflammatory responses in AR.14,35 More importantly, BCL6 is necessitated for the development of follicular Th cells and it exerts inhibitory functions in Th2 cell differentiation.36 The tissue hypereosinophilia occurs with raised IL-4, IL-5, and IL-13 secretion in BCL6-silencing mice, which further indicates the involvement of BCL6 in allergy pathogenesis and the imperative roles in reducing Th2 immune responses.37 Subsequently, we noted that BCL6 was positively associated with Th1 cells but inversely linked with Th2 cells. As reported previously, BCL6 inversely regulates the dominant allergy-associated genes and allergic responses and prevents the generation of IgE and Th2 cytokines.30 BCL6 is believed to facilitate Th1 differentiation by impeding expressions of IL-5 and GATA3.38 Collectively, BCL6 might regulate AR by mediating Th1/Th2 balance.
It is currently acknowledged that the severe symptoms of AR greatly influence the QOL of patients and are related to various conditions including cognitive impairment, headache, fatigue, and sleep disturbances.39 Furthermore, the presence of nasal and ocular symptoms among AR individuals contributes to poor QOL, lowered work productivity, and elevated resource utilization.40 Given the significant changes in QOL among patients with AR, we further assessed the potential relationship between BCL6 expression and QOL. As indicated by the results, BCL6-downregulated AR individuals had a poorer QOL than BCL6-upregulated AR individuals. Among different domains of QOL, practical problems (such as rubbing the nose/eye and blowing the nose), nasal symptoms, and lacrimation were extremely affected by BCL6 expression. There is evidence to suggest that miR-205-5p knockdown might palliate the frequency of sneezing or nose-rubbing of AR mice via increasing BCL6.30 Herein, BCL6 was one of leading factors that impacted the QOL of patients with AR.
Conclusions
The present study evinced that BCL6 was weakly expressed in the serum of patients with AR and low BCL6 expression was a vital factor affecting the QOL of allergic patients. Nonetheless, this study is constrained by following limitations: (1) the study population is hospital-based, so the potential selection bias cannot be ruled out; (2) the disease status and QOL of patients with AR treated in the hospital lack the follow-up investigation, thus ignoring the long-term status of patients with AR. Herein, future experiments need to expand the sample size and further follow up on the changes in disease grade and QOL of patients with AR after receiving hospital treatment.
Statement of Ethics
This study was ratified by the ethics committee of Shanghai Children’s Hospital, Shanghai Jiaotong University School of Medicine. All participants had signed an informed consent.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
All the data generated or analyzed during this study are included in this published article.
REFERENCES
1. Rahim NA, Jantan I, Said MM, Jalil J, Abd Razak AF, Husain K. Anti-allergic rhinitis effects of medicinal plants and their bioactive metabolites via suppression of the immune system: a mechanistic review. Front Pharmacol. 2021;12:660083. 10.3389/fphar.2021.660083
2. Vardouniotis A, Doulaptsi M, Aoi N, Karatzanis A, Kawauchi H, Prokopakis E. Local allergic rhinitis revisited. Curr Allergy Asthma Rep. 2020;20(7):22. 10.1007/s11882-020-00925-5
3. Waserman S, Shah A, Avilla E. Recent development on the use of sublingual immunotherapy tablets for allergic rhinitis. Ann Allergy Asthma Immunol. 2021; 127(2):165-75. 10.1016/j.anai.2021.05.020
4. Nur Husna SM, Tan HT, Md Shukri N, Mohd Ashari NS, Wong KK. Nasal epithelial barrier integrity and tight junctions disruption in allergic rhinitis: overview and pathogenic insights. Front Immunol. 2021;12:663626. 10.3389/fimmu.2021.663626
5. Zeng Y, Song B, Gao Y, Cao W, Li J, Liu Q, et al. Cumulative evidence for association of acetaminophen exposure and allergic rhinitis. Int Arch Allergy Immunol. 2020;181(6):422-33. 10.1159/000506807
6. Choi BY, Han M, Kwak JW, Kim TH. Genetics and epigenetics in allergic rhinitis. Genes. 2021;12(12):2014. 10.3390/genes12122004
7. Bernstein DI, Schwartz G, Bernstein JA. Allergic rhinitis: mechanisms and treatment. Immunol Allergy Clin North Am. 2016;36(2):261-78. 10.1016/j.iac.2015.12.004
8. Teo CWL, Png SJY, Ung YW, Yap WN. Therapeutic effects of intranasal tocotrienol-rich fraction on rhinitis symptoms in platelet-activating factor induced allergic rhinitis. Allergy Asthma Clin Immunol. 2022;18(1):52. 10.1186/s13223-022-00695-x
9. Bousquet J, van Cauwenberge P. Allergic rhinitis and its impact on asthma (ARIA) in collaboration with the World Health Organisation. Prim Care Respir J. 2002; 11(1):18-9. 10.1038/pcrj.2002.7
10. Li L, Liu Y, Wang Q, Wang Z, Cui L, Xu Y, et al. Levels of nasal exhaled hydrogen sulfide in the general population and allergic rhinitis patients. J Clin Lab Anal. 2021;35(3):e23678. 10.1002/jcla.23678
11. Li P, Tsang MS, Kan LL, Hou T, Hon SS, Chan BC, et al. The immuno-modulatory activities of pentaherbs formula on ovalbumin-induced allergic rhinitis mice via the activation of Th1 and treg cells and inhibition of Th2 and Th17 cells. Molecules. 2021;27(1):239. 10.3390/molecules27010239
12. Kirtland ME, Tsitoura DC, Durham SR, Shamji MH. Toll-like receptor agonists as adjuvants for allergen immunotherapy. Front Immunol. 2020;11:599083. 10.3389/fimmu.2020.599083
13. Link CWM, Rau CN, Udoye CC, Ragab M, Korkmaz RU, Comduhr S,et al. IL-2-agonist-induced ifn-gamma exacerbates systemic anaphylaxis in food allergen-sensitized mice. Front Immunol. 2020;11:596772. 10.3389/fimmu.2020.596772
14. Dong F, Tan J, Zheng Y. Chlorogenic acid alleviates allergic inflammatory responses through regulating Th1/Th2 balance in ovalbumin-induced allergic rhinitis mice. Med Sci Monit. 2020;26:e923358. 10.12659/MSM.923358
15. Beguelin W, Teater M, Gearhart MD, Calvo Fernandez MT, Goldstein RL, Cardenas MG, et al. EZH2 and BCL6 cooperate to assemble CBX8-BCOR complex to repress bivalent promoters, mediate germinal center formation and lymphomagenesis. Cancer Cell. 2016; 30(2):197-213. 10.1016/j.ccell.2016.07.006
16. Li Q, Zhou L, Wang L, Li S, Xu G, Gu H, et al. Bcl6 modulates innate immunity by controlling macrophage activity and plays critical role in experimental autoimmune encephalomyelitis. Eur J Immunol. 2020;50(4):525-36. 10.1002/eji.201948299
17. Basso K, Dalla-Favera R. Roles of BCL6 in normal and transformed germinal center B cells. Immunol Rev. 2012;247(1):172-83. 10.1111/j.1600-065X.2012.01112.x
18. Koh B, Ulrich BJ, Nelson AS, Panangipalli G, Kharwadkar R, Wu W,et al. Bcl6 and Blimp1 reciprocally regulate ST2(+) Treg-cell development in the context of allergic airway inflammation. J Allergy Clin Immunol. 2020;146(5):1121-36. 10.1016/j.jaci.2020.03.002
19. Nurieva RI, Chung Y, Martinez GJ, Yang XO, Tanaka S, Matskevitch TD, et al. Bcl6 mediates the development of T follicular helper cells. Science. 2009;325(5943):1001-5. 10.1126/science.1176676
20. Sawant DV, Wu H, Kaplan MH, Dent AL. The Bcl6 target gene microRNA-21 promotes Th2 differentiation by a T cell intrinsic pathway. Mol Immunol. 2013;54(3-4):435-42. 10.1016/j.molimm.2013.01.006
21. Lemonnier N, Melen E, Jiang Y, Joly S, Menard C, Aguilar D, et al. A novel whole blood gene expression signature for asthma, dermatitis, and rhinitis multimorbidity in children and adolescents. Allergy. 2020;75(12):3248-60. 10.1111/all.14314
22. Brozek JL, Bousquet J, Agache I, Agarwal A, Bachert C, Bosnic-Anticevich S, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. 2017;140(4):950-8. 10.1016/j.jaci.2017.03.050
23. Del Cuvillo A, Santos V, Montoro J, Bartra J, Davila I, Ferrer M, et al. Allergic rhinitis severity can be assessed using a visual analogue scale in mild, moderate and severe. Rhinology. 2017;55(1):34-8. 10.4193/Rhin16.025
24. Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) method. Methods. 2001;25(4):402-8. 10.1006/meth.2001.1262
25. Juniper EF, Guyatt GH. Development and testing of a new measure of health status for clinical trials in rhinoconjunctivitis. Clin Exp Allergy. 1991;21(1):77-83. 10.1111/j.1365-2222.1991.tb00807.x
26. AbuRuz SM, Bulatova NR, Tawalbeh MI. Development and validation of the Arabic allergic rhinitis quality of life questionnaire. Saudi Med J. 2009;30(12):1577-83.
27. Malmhall C, Bossios A, Pullerits T, Lotvall J. Effects of pollen and nasal glucocorticoid on FOXP3+, GATA-3+ and T-bet+ cells in allergic rhinitis. Allergy. 2007;62(9):1007-13. 10.1111/j.1398-9995.2007.01420.x
28. Speth MM, Hoehle LP, Phillips KM, Caradonna DS, Gray ST, Sedaghat AR. Treatment history and association between allergic rhinitis symptoms and quality of life. Ir J Med Sci. 2019;188(2):703-10. 10.1007/s11845-018-1866-2
29. Sawant DV, Wu H, Yao W, Sehra S, Kaplan MH, Dent AL. The transcriptional repressor Bcl6 controls the stability of regulatory T cells by intrinsic and extrinsic pathways. Immunology. 2015;145(1):11-23. 10.1111/imm.12393
30. Zhang S, Lin S, Tang Q, Yan Z. Knockdown of miR2055p alleviates the inflammatory response in allergic rhinitis by targeting Bcell lymphoma 6. Mol Med Rep. 2021; 24(5):818. 10.3892/mmr.2021.12458
31. Marino FZ, Aquino G, Brunelli M, Scognamiglio G, Pedron S, Ronchi A, et al. High performance of multiplex fluorescence in situ hybridization to simultaneous detection of BCL2 and BCL6 rearrangements: useful application in the characterization of DLBCLs. Virchows Arch. 2021;479(3):565-73. 10.1007/s00428-021-03084-8
32. Kilic K, Sakat MS, Yildirim S, Kandemir FM, Gozeler MS, Dortbudak MB, et al. The amendatory effect of hesperidin and thymol in allergic rhinitis: an ovalbumin-induced rat model. Eur Arch Otorhinolaryngol. 2019;276(2):407-15. 10.1007/s00405-018-5222-y
33. Liu W, Ota M, Tabushi M, Takahashi Y, Takakura Y. Development of allergic rhinitis immunotherapy using antigen-loaded small extracellular vesicles. J Control Release. 2022;345:433-42. 10.1016/j.jconrel.2022.03.016
34. Zhang YZ, Luo J, Wang ZH, Wang J. Efficacy and safety of sublingual dust mite drops in children with mono-or polysensitized allergic rhinitis. Am J Otolaryngol. 2019;40(5):755-60. 10.1016/j.amjoto.2019.07.010
35. Shao YY, Zhou YM, Hu M, Li JZ, Chen CJ, Wang YJ, et al. The anti-allergic rhinitis effect of traditional Chinese medicine of shenqi by regulating mast cell degranulation and Th1/Th2 cytokine balance. Molecules. 2017; 22(3):504. 10.3390/molecules22030504
36. Bassil R, Orent W, Olah M, Kurdi AT, Frangieh M, Buttrick T, et al. BCL6 controls Th9 cell development by repressing Il9 transcription. J Immunol. 2014;193(1):198-207. 10.4049/jimmunol.1303184
37. Ogasawara T, Kohashi Y, Ikari J, Taniguchi T, Tsuruoka N, Watanabe-Takano H, et al. Allergic TH2 response governed by b-cell lymphoma 6 function in naturally occurring memory phenotype CD4(+) T cells. Front Immunol. 2018;9:750. 10.3389/fimmu.2018.00750
38. Lund R, Ahlfors H, Kainonen E, Lahesmaa AM, Dixon C, Lahesmaa R. Identification of genes involved in the initiation of human Th1 or Th2 cell commitment. Eur J Immunol. 2005;35(11):3307-19. 10.1002/eji.200526079
39. Dahanayake JM, Perera PK, Galappaththy P, Samaranayake D. Efficacy and safety of two Ayurvedic dosage forms for allergic rhinitis: Study protocol for an open-label randomized controlled trial. Trials. 2020;21(1):37. 10.1186/s13063-019-4004-1
40. Virchow JC, Kay S, Demoly P, Mullol J, Canonica W, Higgins V. Impact of ocular symptoms on quality of life (QoL), work productivity and resource utilisation in allergic rhinitis patients-an observational, cross sectional study in four countries in Europe. J Med Econ. 2011;14(3):305-14. 10.3111/13696998.2011.576039