
Download
SHORT COMMUNICATION
Positive drug provocation with beta-lactam antibiotics in children: A single test may not be enough
Luis Morala*, Sara Latorreb, Teresa Torala, Nuria Marcoc, Francisco Canalsd, María José Forniése, María Cristina Gonzáleze, Belén García-Avilésf
aPediatric Allergy and Respiratory Unit, Dr. Balmis General University Hospital, Alicante Institute for Health and Biomedical Research (ISABIAL), Alicante, Spain
bPediatrics Department, Dr. Balmis General University Hospital, Alicante, Spain
cPediatrics Department, Vega Baja Hospital, Orihuela, Spain
dPediatrics Department, Elche General University Hospital, Elche, Spain
ePediatrics Department, Elda General University Hospital, Elda, Spain
fPediatrics Department, Sant Joan d’Alacant University Hospital, Sant Joan d’Alacant, Spain
Abstract
Background: Drug provocation tests (DPTs) are considered the gold standard for diagnosing beta-lactam allergy. However, positive results tend to be mild and difficult to interpret. This study aimed to describe pediatric patients with a presumedly positive or inconclusive DPT, assess the decision to repeat the DPT, and describe its outcome.
Methods: Retrospective review of all presumedly positive or inconclusive DPTs performed in six pediatric allergy clinics from 2017 to 2019. We describe the interpretation of results, focusing on the decision to repeat the DPT and its outcome.
Results: Of 439 children challenged with a beta-lactam, 26 (5.9%) with a presumedly positive or inconclusive result were included in this study. Most were girls (n = 16, 61.5%), and the median age was 5 years (range 1–13). The initial DPT used amoxicillin (n = 13, 50.0%), amoxicillin-clavulanic acid (n = 12, 46.2%), or cefadroxil (n = 1, 3.8%). Reactions were early (n = 11, 42.3 %), delayed (n = 14, 53.8 %), or not registered (n = 1, 3.8 %), but mild in all cases. A second confirmatory DPT was proposed in 19 patients (73.1%) and performed in 17 patients (65.4%). Nine DPTs were performed from 1 day to 4 months after the first DPT, and the remaining eight took place 6 months to 2 years later. Fifteen children tolerated the drug in the second DPT: 88.2% of those reevaluated and 57.5% of the whole study group.
Conclusion: The positive predictive value of DPT may be lower than expected. Given the mildness of observed reactions, a second confirmatory DPT is warranted within a few weeks or months.
Key words: Beta-lactam antibiotics, children, diagnostic accuracy, drug provocation test, false positive reactions
*Corresponding author: Luis Moral, Pediatric Allergy and Respiratory Unit. Dr. Balmis General University Hospital. C/Pintor Baeza, 12. 03010 Alicante. Spain. Email address: [email protected]
Received 3 April 2022; Accepted 21 June 2022; Available online 1 September 2022
Copyright: Moral L, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Beta-lactam antibiotics (BLAs) are the drugs most commonly associated with hypersensitivity reactions in children. The drug provocation test (DPT) is considered the gold standard for diagnosis and helps rule out an allergy to BLA in most pediatric patients, resulting in a very low prevalence of proven allergy.1–3 BLA allergy delabeling has important implications for the patient.4 However, protocols for performing the DPT are heterogeneous, and there is marked interobserver variability in the interpretation of results.5,6 The negative predictive value of the DPT with BLA is considered high.7 The positive predictive value is also assumed to be high, but this may be affected by differences in interpretation, the presence of false positive reactions, and the low prevalence of true BLA allergy. This study aimed to describe the clinical characteristics of pediatric patients with a presumedly positive or inconclusive DPT for BLA hyper-sensitivity, assess the decision to repeat the DPT, and describe its outcome.
Materials and Methods
This retrospective observational study investigated patients aged up to 15 years who attended any of the six participating pediatric allergy clinics from January 2017 to December 2019. Patients examined for suspected BLA hypersensitivity with positive or inconclusive DPT were included in the study. The study was approved by the hospital’s research ethics committee. Data collected included details of age, gender, BLA involved, clinical features of the initial suspicious reaction, details of the first DPT (DPT-1), and results of the tests performed after DPT-1, including, if applicable, a second DPT (DPT-2). The DPT consisted of the oral administration of the suspicious BLA, usually in three incremental doses of 1/100, 1/10, and the full dose of the drug, with 1-hour intervals between doses. In some cases, the DPT was continued at the patient’s home for one or more days, as determined by the prescribing physician. For this study, the DPT was considered positive when signs or symptoms potentially related to the DPT were observed, including cases in which such an association could be deemed inconclusive. Reactions observed within the first 2 hours following administration of the BLA were considered immediate, whereas those appearing afterward were considered delayed. Exanthem and urticaria type reactions following the DPT were grouped because some cases met overlapping characteristics for both. The studies conducted following the positive DPT were decided by the attending physician, with the informed consent of the patients and their parents. When a DPT-2 was proposed, it was considered early if performed within the first 6 months following the DPT-1, and late if performed at least 6 months after.
Results
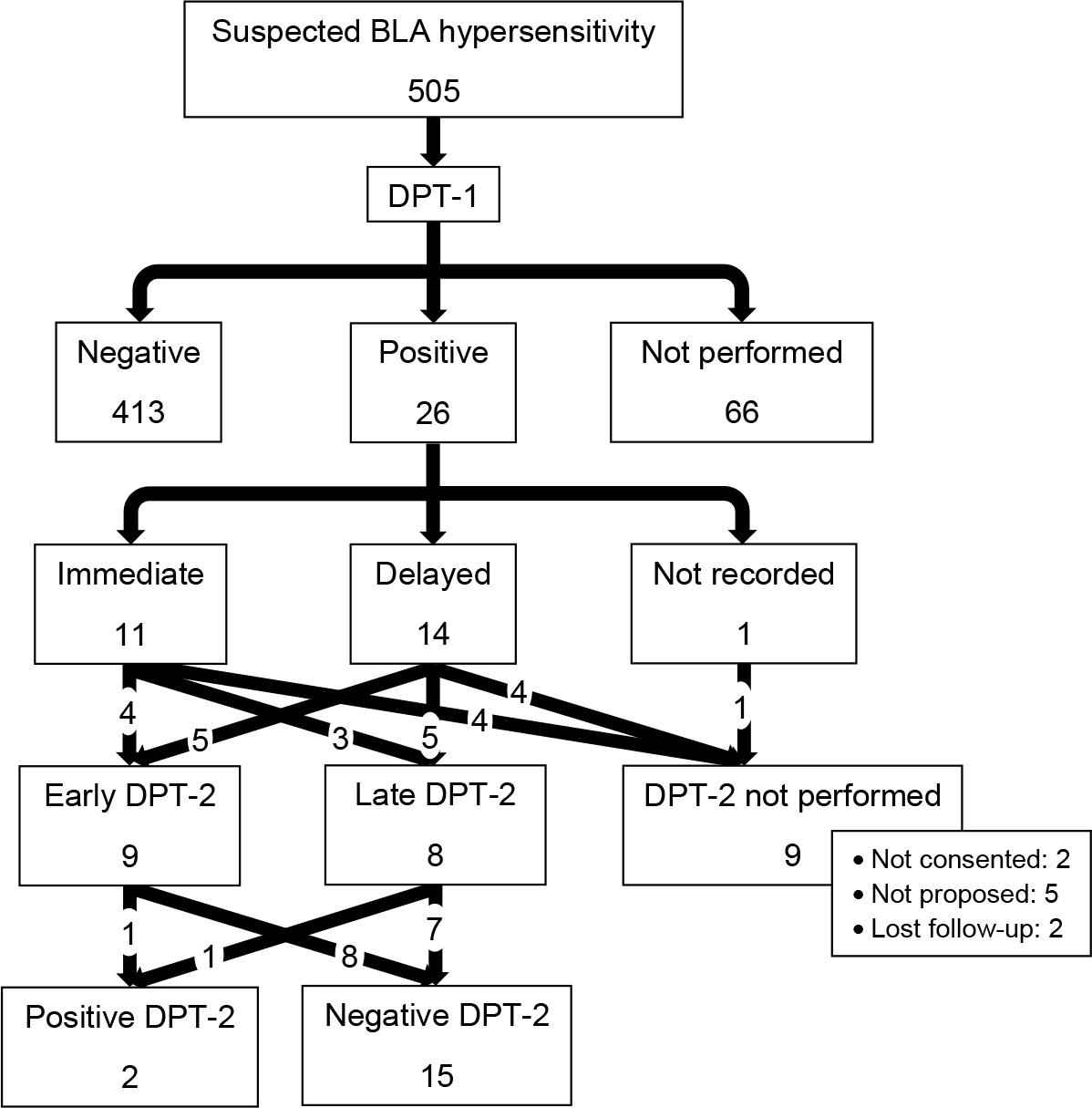
During the study period, 505 patients were evaluated for suspected BLA hypersensitivity, and 439 (86.9%) underwent a DPT (Figure 1). Of these, 26 (5.9%) had a presumedly positive or inconclusive result and were enrolled in the study. Table 1 shows the main patient characteristics and reactions following the DPT. The patients’ age ranged from 1 to 13 years (median 5), and most were girls (n = 16, 61.5%). The main reason for referral to the allergy clinic was the appearance of exanthem and/or urticaria/angioedema (n = 24, 92.3%) following administration of a BLA; no patient had anaphylaxis or other severe reactions. BLAs used for the DPT-1 were amoxicillin (n = 13, 50.0%), amoxicillinclavulanic acid (n = 12, 46.2%), and cefadroxil (n = 1, 3.8%). Reactions following the DPT-1 were immediate in 11 patients (42.3%) (six with exanthem/urticaria, three with vomiting, and two with pharyngeal pruritus), delayed in 14 patients (53.8%) (all of them with exanthem/urticaria), and not recorded in one patient (3.8%). In all cases, the reaction observed was mild and easily resolved.
Table 1 List of cases with description of studies performed and results.
| Case | Sex, age†, and BLA involved | DPT-1: symptoms | Skin tests/specific IgE following DPT-1 | Interval between DPTs, DPT-2 result |
|---|---|---|---|---|
| Clinic 1 | ||||
| 1 | Female, 2, amoxicillin | Delayed exanthem | Not performed | 4 months, NEGATIVE |
| 2 | Male, 2, amoxi-clav | Delayed exanthem | Not performed | 1 month, NEGATIVE |
| 3 | Male, 3, cefadroxil | Immediate vomiting | Not performed | 2 days, NEGATIVE |
| 4 | Female, 13, amoxicillin | Delayed exanthem | Not performed | 1 month, NEGATIVE |
| 5 | Female, 13, amoxicillin | Immediate mild urticaria | Not performed | 1 day, NEGATIVE |
| 6 | Female, 7, amoxi-clav | Immediate vomiting | Not performed | 2 weeks, NEGATIVE |
| 7 | Male, 1, amoxicillin | Delayed generalized erythema | Weak positive prick test (3–4 mm) to PPL, MDM, and amoxi-clav. Negative to penicillin, amoxicillin, and cephalosporines Negative intradermal test (immediate and delayed) with all BLAs | Proposed in 2 months, but patient did not attend the test |
| Clinic 2 | ||||
| 8 | Female, 2, amoxi-clav | Immediate vomiting | Not performed | 1 month, NEGATIVE |
| 9 | Male, 13, amoxi-clav | Delayed exanthem and hand edema | Positive skin tests to amoxicillin (14 mm) and amoxi-clav (18 mm), late reading | Not proposed |
| 10 | Female, 5, amoxi-clav | Delayed urticaria | Negative skin tests | Patient fails to attend visit 1 year later |
| Clinic 3 | ||||
| 11 | Male, 3, amoxicillin | Delayed urticaria | Negative skin tests and specific IgE | 6 months, NEGATIVE |
| 12 | Female, 2, amoxicillin | Delayed pruritic exanthem | Negative skin tests and specific IgE | 1 year, NEGATIVE |
| 13 | Male, 1, amoxi-clav | Immediate exanthem | Not performed | Patient fails to attend visit 1 month later |
| 14 | Female, 1, amoxicillin | Delayed exanthem | Negative skin tests and specific IgE | 1 year, NEGATIVE |
| 15 | Female, 1, amoxicillin | Delayed urticaria | Negative skin tests and specific IgE | Proposed within 3 months, no consent |
| 16 | Female, 13, amoxicillin | Delayed urticaria | Negative skin tests and specific IgE | 3 months, NEGATIVE |
| 17 | Female, 8, amoxicillin | Delayed localized erythema | Negative skin tests and specific IgE | 1 year later, POSITIVE: pruritic exanthem in back and foot, and vomiting 3–4 hours after test |
| Clinic 4 | ||||
| 18 | Male, 8, amoxicillin | Immediate urticarial exanthem | Negative skin tests and specific IgE | Not proposed |
| 19 | Female, 11, amoxicillin | Immediate pharyngeal pruritus | Not performed | Not proposed |
| 20 | Female, 11, amoxi-clav | Unspecified | Not performed | Not proposed |
| 21 | Male, 13, amoxicillin | Pharyngeal pruritus and immediate abdominal pain | Not performed | Not proposed |
| 22 | Male, 3, amoxi-clav | Delayed exanthem | Not performed | 3 weeks, POSITIVE: generalized rash 8 hours after test |
| Clinic 5 | ||||
| 23 | Female, 6, amoxi-clav | Immediate urticaria | Negative specific IgE | 2 years later, NEGATIVE (amoxicillin) |
| 24 | Male, 1, amoxi-clav | Immediate palpebral edema | Not performed | Almost 2 years later, NEGATIVE (amoxicillin) |
| Clinic 6 | ||||
| 25 | Female, 5, amoxi-clav | Immediate lip edema and sialorrhea | Negative skin tests and specific IgE | 1 year, NEGATIVE |
| 26 | Female, 9, amoxi-clav | Delayed pruritic exanthem | Negative skin tests and specific IgE | 6 months, NEGATIVE |
†Age in years.
Amoxi-clav, amoxicillin with clavulanic acid; BLA, beta-lactam antibiotics; DPT-1, first drug provocation test; DPT-2 second drug provocation test; MDM, minor determinant mixture; PPL, penicilloyl-polylysine.
Figure 1 Flowchart of patients attended, drug provocation tests (DPT-1 and DPT-2) performed and outcomes.
The flowchart of patients attended, DPTs performed, and outcomes is shown in Figure 1. Overall, a second DPT was performed in 17 of the 26 patients (65.4%), 15 of whom tolerated the BLA (88.2% of those reassessed with a DPT-2 and 57.7% of all the positive cases from DPT-1). Only two (11.8% of those reassessed with a DPT-2) had mild, delayed symptoms. An early DPT-2 was proposed in 11 patients, but it was only performed in 9 patients (two patients did not consent), yielding only one positive case (delayed exan-them). A late DPT-2 was proposed and performed in eight patients from 6 months to 2 years after DPT-1, again with only one positive case (delayed exanthem and vomiting). In five patients, the result of DPT-1 was taken as valid, and confirmatory tests were not considered. The remaining two patients did not attend the scheduled appointments. The results of DPT-2 in patients with immediate versus delayed reactions in DPT-1 (Table 2) were similar. Likewise, no differences were observed between patients for whom an early or a late DPT-2 was proposed. Disparate clinical decisions (regarding skin tests, specific IgE, frequency, and timing of DPT-2) after a positive DPT-1 were observed among the different pediatric allergy clinics (Table 1).
Table 2 Relationship between timing of reaction to DPT-1 and DPT-2 outcome, n (%).
| DPT-2 outcome | Type of reaction in DPT-1 | |
|---|---|---|
| Immediate (n=11) | Delayed (n=14) | |
| Positive | 0 (0.0) | 2 (14.3) |
| Negative | 7 (63.6) | 8 (57.1) |
| Patient refusal or nonattendance | 1 (9.1) | 3 (21.4) |
| Not proposed | 3 (27.3) | 1 (7.1) |
Results from 25 patients are presented, excluding one case for whom the details of DPT-1 were not known and no DPT-2 was proposed.
DPT-1, first drug provocation test; DPT-2 second drug provocation test.
Discussion
As observed in other large pediatric series, only 5.9% of our patients who attended for suspected BLA allergy had a potentially positive DPT (1-3). However, more than half the patients with a positive or inconclusive DPT-1 tolerated the BLA in DPT-2, most of which were performed within 6 months of the DPT-1. These results challenge the positive predictive value of the DPT, which might be lower than usually assumed, which would in turn further reduce the true prevalence of hypersensitivity to BLAs in the pediatric population. We are aware of only three studies that conducted a DPT-2 with BLAs in pediatric patients, in all cases at least a year following the positive DPT-1, reporting tolerance in 50% to 89% of them.3,8,9 Although the authors of these studies suggested a loss of hypersensitivity over time, none repeated the test at an early stage, which could lead to speculation regarding how many of those DPT-1 tests might have been false positives.
In adults, the main reason for a false positive in a DPT is the nocebo effect, which has been well characterized in blind, placebo-controlled challenges.10–13 The nocebo effect can provoke not only subjective symptoms but also objective signs, mainly cutaneous. This effect is poorly documented in children and adolescents, but nocebo by proxy is another possibility to be considered.14 In our series, two of the patients reported subjective symptoms and were not rechallenged, but probably they should have been. False positive reactions may also be due to the presence of pre-existing or concomitant symptoms or illnesses—usually cutaneous— which may concur, worsen, or become more apparent as a result of the special vigilance required for the test. However, there are limited reports of false positive drug-related reactions in pediatric patients.15,16 It is often difficult to classify the result as positive or negative, and it is common to find mild, unspecific, inconclusive, or different reactions than the initially suspicious ones. In view of this, we have combined potentially positive and inconclusive results in this work, due to overlapping characteristics and inherently subjective classification of DPT results. Similar questions and problems to these have been considered regarding food challenges.17–19
Positive predictive values of diagnostic tests are known to be influenced by the prevalence of the tested condition in the population that is being tested.20 Given the low prevalence of BLA hypersensitivity in children, the likelihood of a false positive DPT is significant for different reasons. Despite the limitations of our study, including its retrospective nature, small sample, and heterogeneous practices in participating clinics, we conclude that a positive BLA DPT should preferably be confirmed with a second DPT conducted within a few weeks or months. Since positive DPT rates for BLA are low, and reactions observed are rarely severe,21 the excess work required to repeat the DPT may be largely compensated by the higher diagnostic accuracy and the potential for removing a false label and averting its negative consequences. Placebo-controlled tests may be a rare and last resort when the DPT is repeatedly inconclusive or a nocebo effect is suspected.
Acknowledgements
This work won the second-best oral presentation award at the 44th Congress of the Spanish Society of Pediatric Allergy, Asthma, and Clinical Immunology (SEICAP 2020).
Conflicts of Interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
REFERENCES
1. Zambonino MA, Corzo JL, Muñoz C, Requena G, Ariza A, Mayorga C, et al. Diagnostic evaluation of hypersensitivity reactions to beta-lactam antibiotics in a large population of children. Pediatr Allergy Immunol. 2014;25(1):80–7. 10.1111/pai.12155
2. Ibáñez MD, Rodríguez del Río P, Lasa EM, Joral A, Ruiz-Hornillos J, Muñoz C, et al. Prospective assessment of diagnostic tests for pediatric penicillin allergy: From clinical history to challenge tests. Ann Allergy Asthma Immunol. 2018;121(2): 235–44.e3. 10.1016/j.anai.2018.05.013
3. Guðnadóttir GK, Jónasson G, Clausen M, Sørensen TG, Kristjánsson S. Antibiotic oral provocation challenge in children. Acta Paediatr. 2021 Dec 8. doi: 10.1111/apa.16211. Online ahead of print.
4. Lucas M, Arnold A, Sommerfield A, Trevenen M, Braconnier L, Schilling A, et al. Antibiotic Allergy Labels in Children Are Associated with Adverse Clinical Outcomes. J Allergy Clin Immunol Pract. 2019;7(3):975–82. 10.1016/j.jaip.2018.09.003
5. Romano A, Atanaskovic-Markovic M, Barbaud A, Bircher AJ, Brockow K, Caubet JC, et al. Towards a more precise diagnosis of hypersensitivity to beta-lactams — an EAACI position paper. Allergy. 2020;75(6):1300–15. 10.1111/all.14122
6. Torres MJ, Celik GE, Whitaker P, Atanaskovic-Markovic M, Barbaud A, Bircher A, et al. A EAACI drug allergy interest group survey on how European allergy specialists deal with β-lactam allergy. Allergy. 2019;74(6):1052–62. 10.1111/all.13721
7. Misirlioglu ED, Toyran M, Capanoglu M, Kaya A, Civelek E, Kocabas CN. Negative predictive value of drug provocation tests in children. Pediatr Allergy Immunol. 2014;25(7):685–90. 10.1111/pai.12286
8. Berroa F, Callero F, Fuentes-Aparicio V, Infante S, AlonsoLebrero E, Zapatero L. Rechallenge in pediatric patients diagnosed with delayed hypersensitivity to penicillins. J Investig Allergol Clin Immunol. 2013;23(5):369–70. http://www.jiaci.org/issues/vol23issue5/10-15.pdf
9. Tonson la Tour A, Michelet M, Eigenmann PA, Caubet JC. Natural History of Benign Nonimmediate Allergy to Beta-Lactams in Children: A Prospective Study in Retreated Patients After a Positive and a Negative Provocation Test. J Allergy Clin Immunol Pract. 2018;6(4):1321–6. 10.1016/j.jaip.2017.10.008
10. Lombardi C, Gargioni S, Canonica GW, Passalacqua G. The nocebo effect during oral challenge in subjects with adverse drug reactions. Eur Ann Allergy Clin Immunol. 2008;40(4):138–41. http://www.eurannallergyimm.com/cont/journals-articles/133/volume-nocebo-effect-during-oral-challenge-353allasp1.pdf
11. Bavbek S, Aydin, Sözener Z, Yüksel S. Determinants of nocebo effect during oral drug provocation tests. Allergol Immunopathol (Madr). 2015;43(4):339–45. 10.1016/j.aller.2014.04.008
12. Liccardi G, Senna G, Russo M, Bonadonna P, Crivellaro M, Dama A, et al. Evaluation of the nocebo effect during oral challenge in patients with adverse drug reactions. J Invest Allergol Clin Immunol. 2004;14(2):104–7.
13. Bizzi F, Voltolini S, Fiaschi MD, Cavanna D. Assessing clinical and psychological features: Who are patients showing a nocebo reaction during the drug challenge test? Eur Ann Allergy Clin Immunol. 2019;51(6):258–64. 10.23822/EurAnnACI.1764-1489.116
14. Czerniak E, Oberlander TF, Weimer K, Kossowsky J, Enck P. “Placebo by Proxy” and “Nocebo by Proxy” in Children: A Review of Parents’ Role in Treatment Outcomes. Front Psychiatry. 2020;11:1–10. 10.3389/fpsyt.2020.00169
15. Arik Yilmaz E, Tolga Yavuz S, Sekerel BE. Based on a patient: Dermographism should be routinely investigated before every provocation test. Allergol Immunopathol (Madr). 2013;41(1): 65–6. 10.1016/j.aller.2011.11.005
16. Raley E, Khan DA. Drug-associated inducible laryngeal obstruction complicating penicillin allergy testing. Ann Allergy Asthma Immunol. 2020;125(5):599–600. 10.1016/j.anai.2020.06.031
17. Niggemann B. When is an oral food challenge positive? Allergy. 2010;65(1):2–6. 10.1111/j.1398-9995.2009.02170.x
18. Grabenhenrich LB, Reich A, Bellach J, Trendelenburg V, Sprikkelman AB, Roberts G, et al. A new framework for the documentation and interpretation of oral food challenges in population-based and clinical research. Allergy. 2017;72(3):453–61. 10.1111/all.13049
19. de Weger WW, Sprikkelman AB, Herpertz CEM, van der Meulen GN, Vonk JM, Kamps AWA, et al. The dilemma of open or double-blind food challenges in diagnosing food allergy in children: Design of the ALDORADO trial. Pediatr Allergy Immunol. 2022;33(1):e13654 10.1111/pai.13654
20. Mischlinger J, Schernhammer E. A common trap of diagnostic tests: Disease prevalence and positive predictive value. Wien Klin Wochenschr. 2017;129(15–16):583–4. 10.1007/s00508-017-1204-0
21. Cardoso-Fernandes A, Blumenthal KG, Chiriac AM, Tarrio I, Afonso-João D, Delgado L, et al. Frequency of severe reactions following penicillin drug provocation tests: A Bayesian meta-analysis. Clin Transl Allergy. 2021;11(4):1–14. 10.1002/clt2.12008