
Download
ORIGINAL ARTICLE
Serum dual-specificity phosphatase 1 reflects decreased exacerbation risk, correlates with less advanced exacerbation severity and lower inflammatory cytokines in children with asthma
Xingqing Guo*, Chong Wang, Dong Xie, Cui Bai, Chenggang Mao, Fang Wang
Department of Pediatrics, The Affiliated Hospital of Qingdao University, Qingdao, Shandong, China
Abstract
Background: It is as fact that dual-specificity phosphatase 1 (DUSP1) regulates the T cell activation, pro-allergic response, and inflammation to engage with the pathogenesis of asthma, but its clinical role in children with asthma is unclear. The present study aimed to explore the expression of DUSP1, its association with exacerbation risk, severity, and inflammatory cytokines in children with asthma.
Method: Around 52 children with asthma-exacerbation, 50 children in asthma-remission, and 50 healthy children were chosen for the study. The serum levels of DUSP1, as well as tumor necrosis factor-α (TNF-α), interleukin (IL)-1β, IL-6, and IL-17 were detected by the enzyme-linked immunosorbent assay.
Results: The levels of DUSP1 was the highest in healthy children (median (IQR)=34.305 (25.892– 43.693) ng/mL), the second highest in children in asthma-remission (median (IQR)=21.471 (18.581–27.934) ng/mL), and the lowest in children with asthma-exacerbation (median (IQR)=13.982 (7.901–21.624) ng/mL) (P<0.001). At the same time, DUSP1 was also related to decreased asthma risk with area under curve (AUC) (95%CI) of 0.847 (0.780–0.914), and correlated with its lower exacerbation risk with AUC (95%CI) of 0.755 (0.661–0.849). Besides, DUSP1 was negatively linked with exacerbation severity (rs=–0.338, P=0.014), immunoglobulin E (rs=-0.277, P=0.047), TNF-α (rs=-0.423, P=0.002), IL-1β (rs=-0.389, P=0.004), and IL-17 (rs=-0.293, P=0.035), but not related with other disease features in children with asthma-exacerbation. Meanwhile, DUSP1 was only negatively associated with TNF-α (rs=-0.300, P=0.034) and IL-1β (rs=-0.309, P=0.029) in children in asthma-remission. However, no correlation was found in DUSP1 with inflammatory cytokines or other disease features in healthy children (all P>0.05).
Conclusion: DUSP1 reflects the reduced exacerbation risk, and associates with lower exacerbation severity and inflammatory cytokines in children with asthma-exacerbation; it also associates with inflammatory cytokines in children in asthma-remission. These findings suggest that DUSP1 may help to improve the management of asthmatic children.
Key words: acute exacerbation risk, asthmatic children, dual-specificity phosphatase 1, exacerbation severity, inflammatory cytokines
*Corresponding author: Xingqing Guo, Department of Pediatrics, The Affiliated Hospital of Qingdao University, No.16 Jiangsu Road, Qingdao 266000, China. Email address: [email protected]
Received 29 December 2021; Accepted: 5 May 2022; Available online 1 November 2022
Copyright: Guo X, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Asthma is a common chronic respiratory and inflammatory disease, which affected more than 330 million people worldwide in the year 2021.1–3 It frequently occurs in children, and causes difficulty in breathing, cough, mucus secretion, along with other symptoms.4,5 Currently, the prevention strategies against asthma include an enhanced inhaler technique and educating and creating awareness among people on asthma.6 At the same time, drugs such as inhaled corticosteroids and long-acting β2 adrenergic bronchodilators, as well as therapeutic strategies, including maintenance and reliever therapy (SMART) or combination therapies, have been recommended for asthmatic children.7,8 Despite these preventive measures and treatments, children may still present with life-threatening respiratory distress due to sudden onset of acute exacerbation asthma.4 To reduce the exacerbation risk, exploring new biomarkers to improve the management of asthmatic children is needed.
Dual-specificity phosphatase 1 (DUSP1), also called mitogen-activated protein kinase (MAPK) phosphatase-1 (MKP-1), is originally confirmed as an extracellular signal-regulated kinase (ERK)-specific phosphatase.9 It is reported that DUSP1 plays a vital role in asthmatic pathogenesis by various means. For example, DUSP1 is required for T helper (Th)1 differentiation, and the imbalance of Th1/ Th2 is essential in the pathogenesis of asthma10–12 DUSP1 acts as a negative regulator of pro-allergic response in airway epithelial cells, which are essential in the progression of asthma.13 Besides, DUSP1 inhibits the MAPK activation, and then participates in the pathogenesis of asthma by p38 and ERK1/2 pathways.14,15 Apart from the above information, DUSP1 also inhibits the activation of M1 macrophage and promotes M2 macrophage, thus mediating the anti-inflammatory effect of glucocorticoids in asthma.16,17 Based on the above information, we hypothesized that DUSP1 might be a potential biomarker for reflecting asthma severity and inflammation.
In the current study, we aimed to explore the expression of DUSP1, its correlation with the exacerbation risk, the severity degree, and inflammatory cytokines in asthmatic children.
Materials and Methods
Study participants
This was a case-control study in which a total of 52 children with asthma-exacerbation and 50 children in asthma-remission were serially chosen for the study between January 2020 and February 2021. All asthmatic children were aged from 1 to 16 years, and were diagnosed according to the criteria issued by the Global Initiative for Asthma.18 Asthma-exacerbation was defined as an acute or sub-acute attack of asthma due to airflow obstruction. Asthma-remission was defined as the absence of symptoms, and the pulmonary function restored and maintained for at least 2 months. Asthmatic children were ineligible for the study if they had complicated medical history with other respiratory diseases, autoimmune disorders, or had a prior history of cancer or hematological malignancies. In addition, the study also selected 50 healthy children in the age group of 1–16 years, receiving health examination during the same period, and were considered as health controls. The health controls were excluded from the study if they had any abnormality upon health examination, or had a history of respiratory diseases, autoimmune disorders, cancers, or hematological malignancies. The study protocol was approved by the Institutional Review Board of The Affiliated Hospital of Qingdao University. The statutory guardians of all participants provided written informed consents.
Data collection
The clinical characteristics of all participants were collected for study analysis, including the demographic characteristics, family history of asthma, eosinophil count, immunoglobulin E (IgE) level, forced expiratory volume in 1 second (FEV1) (% predicted), forced vital capacity (FVC), and inflammatory cytokines. Besides, the exacerbation severity was evaluated among children with asthma-exacerbation in accordance with the international consensus on (ICON) pediatric asthma recommendations.1
Sample collection and assessment
After recruitment, the peripheral blood samples were collected from all participants, and then the serum samples were separated by refrigerated centrifuge to detect the level of tumor necrosis factor-α (TNF-α), inter-leukin (IL)-1β, IL-6, and IL-17 by enzyme-linked immunosorbent assay (ELISA). The kits used in ELISA were as follows: Human TNF-α Quantikine ELISA Kit (Catalog no.: DTA00D), Human IL-1β Quantikine ELISA Kit (Catalog no.: DLB50), Human IL-6 Quantikine ELISA Kit (Catalog no.: D6050), and Human IL-17 Quantikine ELISA Kit (Catalog no.: D1700). All kits were purchased from R&D Systems Europe, Ltd. (Minneapolis, MN, USA). The ELISA operation was carried out in strict accordance with the manual provided by the manufacturer. Besides, the serum level of DUSP1 was also detected by ELISA using human dual specificity protein phosphatase 1 (Catalog no.: E9899h) (EIAAB SCIENCE INC, Wuhan, China), and the experimentation was consistent with the description of a previous study.19 The ELISA was performed with a triplicate experiment, and the mean value was considered as the final result.
In addition, a reverse transcription quantitative polymerase chain reaction (RT-qPCR) was performed to detect the DUSP1 mRNA expression. The total RNA was extracted by RNeasy Protect Mini Kit (Qiagen, Duesseldorf, NordrheinWestfalen, Germany), and then the reserve transcription was performed by PrimeScript™ RT reagent Kit (Takara, Dalian, Liaoning, China). After which, qPCR was realized by KOD SYBR® qPCR Mix (TOYOBO, Osaka, Kansai, Japan). The relative expression of DUSP1 was calculated using the 2-ΔΔCt method with GAPDH as an internal reference. The primers were referred to a previous study.20
Statistics
SPSS 26.0 (IBM Corp., Armonk, New York, USA) and GraphPad Prism 8.1.1 (GraphPad Software Inc., San Diego, California, USA) were used for data analysis and graph plotting, respectively. The comparisons among groups were analyzed using one-way analysis of variance test, Chi-square test or Kruskal-Wallis H rank sum test. The performance of the DUSP1 level in distinguishing the different participants was estimated using the receiver operating characteristic (ROC) curve. Associations between the variables were evaluated using Spearman’s rank correlation test, and P <0.05 was considered as statistically significant.
Results
Clinical characteristics of asthmatic children and healthy controls
A total of 52 children with asthma-exacerbation, 50 children in asthma-remission children and 50 healthy children as controls were enrolled for this study, with their characteristics shown in Table 1. The mean age of children with asthma-exacerbation, children in asthma-remission, and healthy controls were 6.1±2.8 years, 6.1±2.5 years, and 6.4±2.8 years, respectively. Also, there were 26 (50.0%), 23 (46.0%), and 18 (36.0%) female children with asthma-exacerbation, in asthma-remission, and healthy controls respectively. Moreover, no difference was found among asthmatic children and healthy controls in some clinical characteristics, including age, gender, height, weight, or family history of asthma (all P>0.05); however, the median values of eosinophil count, IgE, TNF-α, IL-1β, IL-6, and IL-17 as well as the mean values of FEV1/FVC and FEV1 (% predicted) showed differences (all P<0.001).
Table 1 Clinical characteristics of participants
| Items | Asthma-exacerbation children (N = 52) | Asthma-remission children (N = 50) | Health controls (N = 50) | P value |
|---|---|---|---|---|
| Age (years), mean±SD | 6.1±2.8 | 6.1±2.5 | 6.4±2.8 | 0.788 |
| Gender, n (%) | 0.343 | |||
| Female | 26 (50.0) | 23 (46.0) | 18 (36.0) | |
| Male | 26 (50.0) | 27 (54.0) | 32 (64.0) | |
| Height (cm), mean±SD | 115.8±16.5 | 113.8±14.6 | 120.7±18.8 | 0.111 |
| Weight (kg), mean±SD | 22.7±7.6 | 22.1±7.3 | 24.6±9.9 | 0.282 |
| Family history of asthma, n (%) | 0.332 | |||
| No | 40 (76.9) | 40 (80.0) | 44 (88.0) | |
| Yes | 12 (23.1) | 10 (20.0) | 6 (12.0) | |
| Exacerbation severity, n (%) | - | |||
| Mild | 12 (23.1) | - | - | |
| Moderate | 28 (53.8) | - | - | |
| Severe | 12 (23.1) | - | - | |
| Eosinophil count (X109/L), median (IQR) | 0.5 (0.4–0.7) | 0.2 (0.1–0.3) | 0.1 (0.1–0.1) | <0.001 |
| IgE (IU/mL), median (IQR) | 237.5 (153.4–367.5) | 74.6 (51.4–118.1) | 40.0 (23.9–54.6) | <0.001 |
| FEV1/FVC (%), mean±SD | 67.9±6.5 | 78.2±3.4 | 83.7±2.6 | <0.001 |
| FEV1(% predicted), mean±SD | 77.6±6.2 | 88.1±4.5 | 100.1±6.2 | <0.001 |
| TNF-α (pg/mL), median (IQR) | 61.1 (47.7–94.9) | 28.8 (24.2–40.7) | 20.9 (16.7–27.4) | <0.001 |
| IL-1β (pg/mL), median (IQR) | 5.5 (4.3–7.4) | 2.3 (1.5–3.0) | 1.5 (1.1–1.8) | <0.001 |
| IL-6 (pg/mL), median (IQR) | 62.7 (37.5–83.7) | 22.1 (20.1–26.0) | 12.7 (9.0–16.4) | <0.001 |
| IL-17 (pg/mL), median (IQR) | 85.0 (47.7–137.8) | 35.0 (29.3–41.1) | 21.2 (17.8–24.9) | <0.001 |
Abbreviations: SD, standard deviation; IQR, interquartile range; IgE, immunoglobulin E; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; TNF-α, tumor necrosis factor-α; IL-1β, interleukin-1 β; IL-6, interleukin- 6; IL-17, interleukin-17
DUSP1 expression in asthmatic children
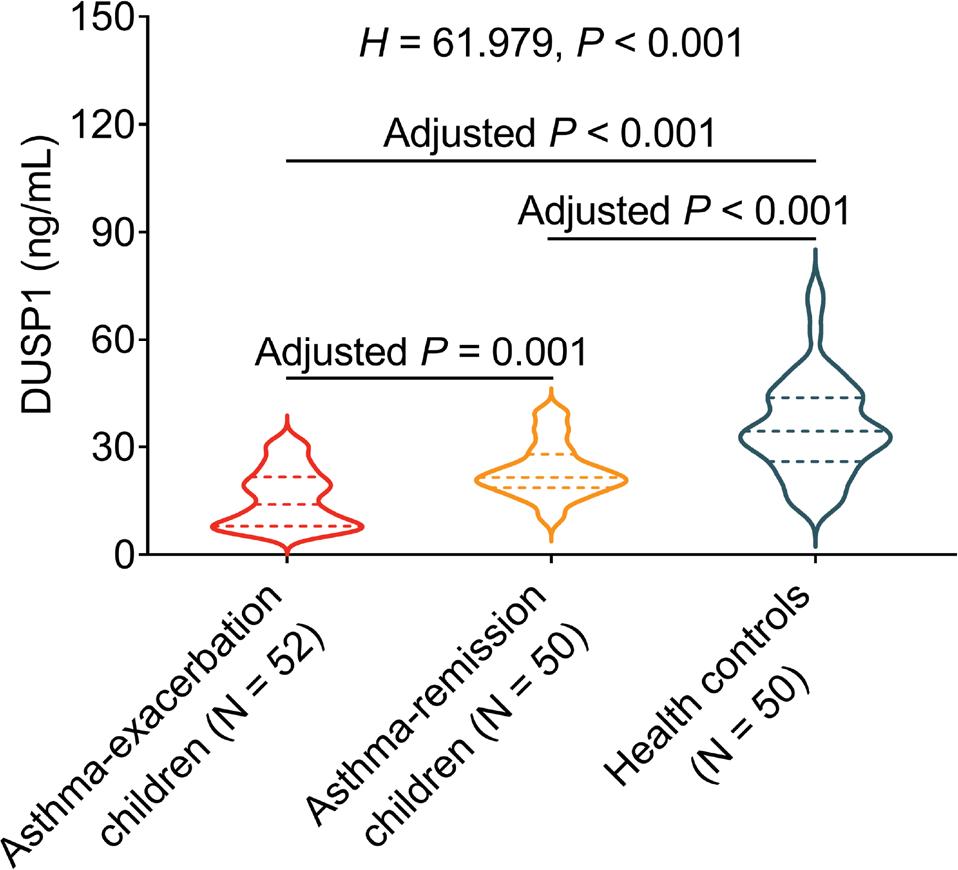
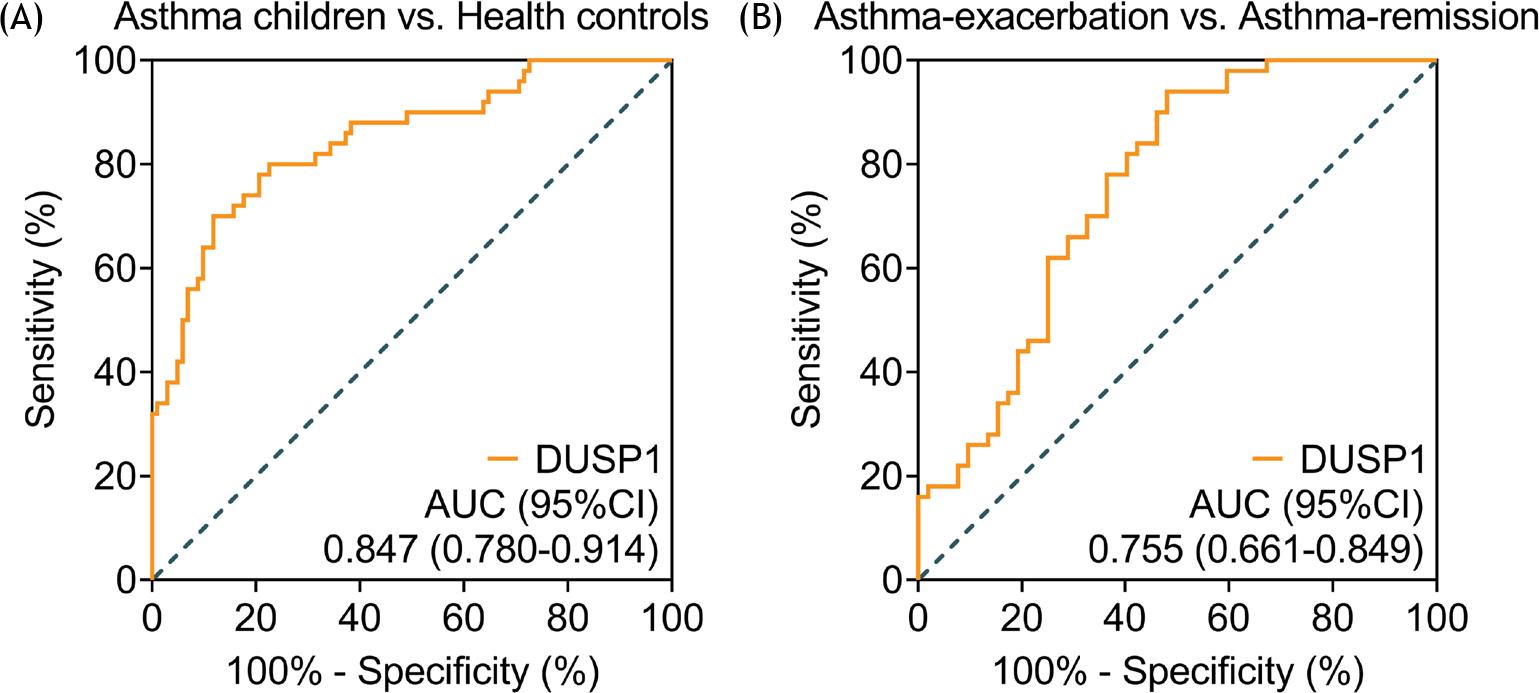
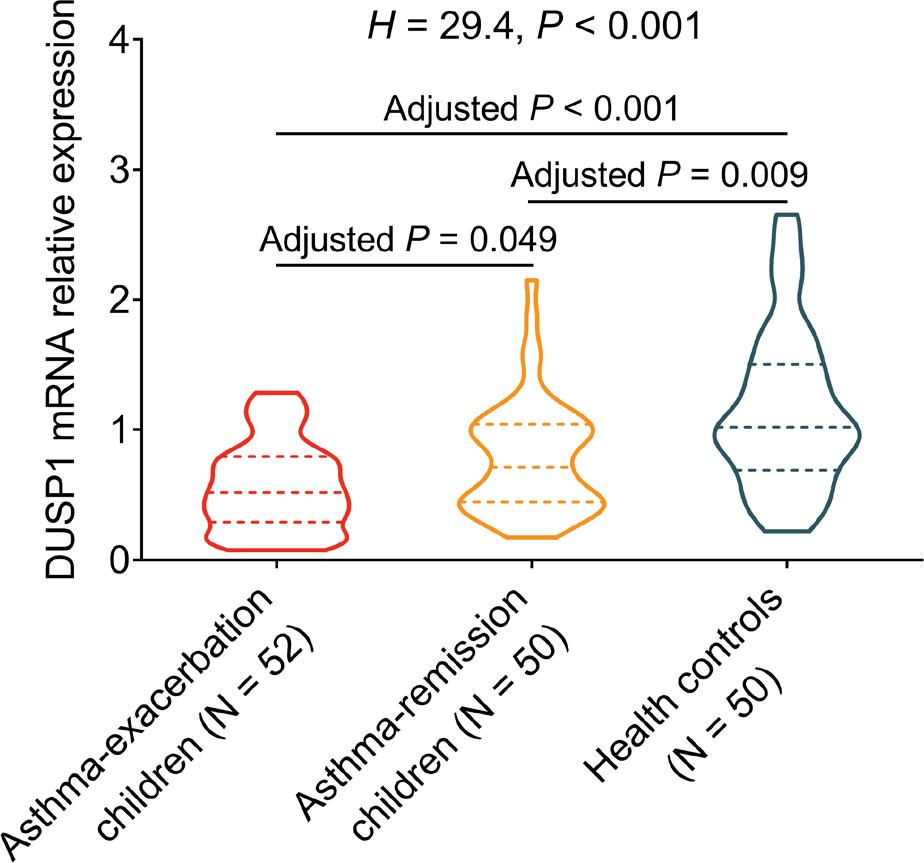
It was noted that DUSP1 was the highest in the healthy controls, the second highest among children in asthma-remission, and the lowest in children with asthma-exacerbation (P<0.001). According to multiple-comparison tests, DUSP1 was found to be decreased in children with asthma-exacerbation and children in asthma-remission than in healthy controls (both P<0.001). Besides, DUSP1 was lower among children with asthma-exacerbation than children in asthma-remission (P= 0.001) (Figure 1). Additionally, the ROC curve showed that DUSP1 had a great potential in discriminating asthmatic children from healthy controls with an AUC of 0.847, and a 95% confidence interval (CI) of 0.780–0.914; meanwhile, DUSP1 possessed a certain capability of distinguishing children with asthma-exacerbation from children in asthma-remission, the AUC (95% CI) of which was 0.755 (0.661–0.849) (Figure 2A-B). Besides, RT-qPCR was also applied to detect DUSP1 mRNA expression, which was also the lowest among children with asthma-exacerbation, followed by children in asthma-remission, and highest in healthy controls (P<0.001) (Supplementary figure 1).
Figure 1 Comparison of DUSP1 among asthma-exacerbation children, asthma-remission children, and healthy controls.
Figure 2 The ROC curve analyses. The potential of DUSP1 to discriminate: (A) asthmatic children from healthy controls and (B) asthma-exacerbation children from asthma-remission children.
Correlation of DUSP1 with exacerbation severity and inflammatory cytokines in asthmatic children
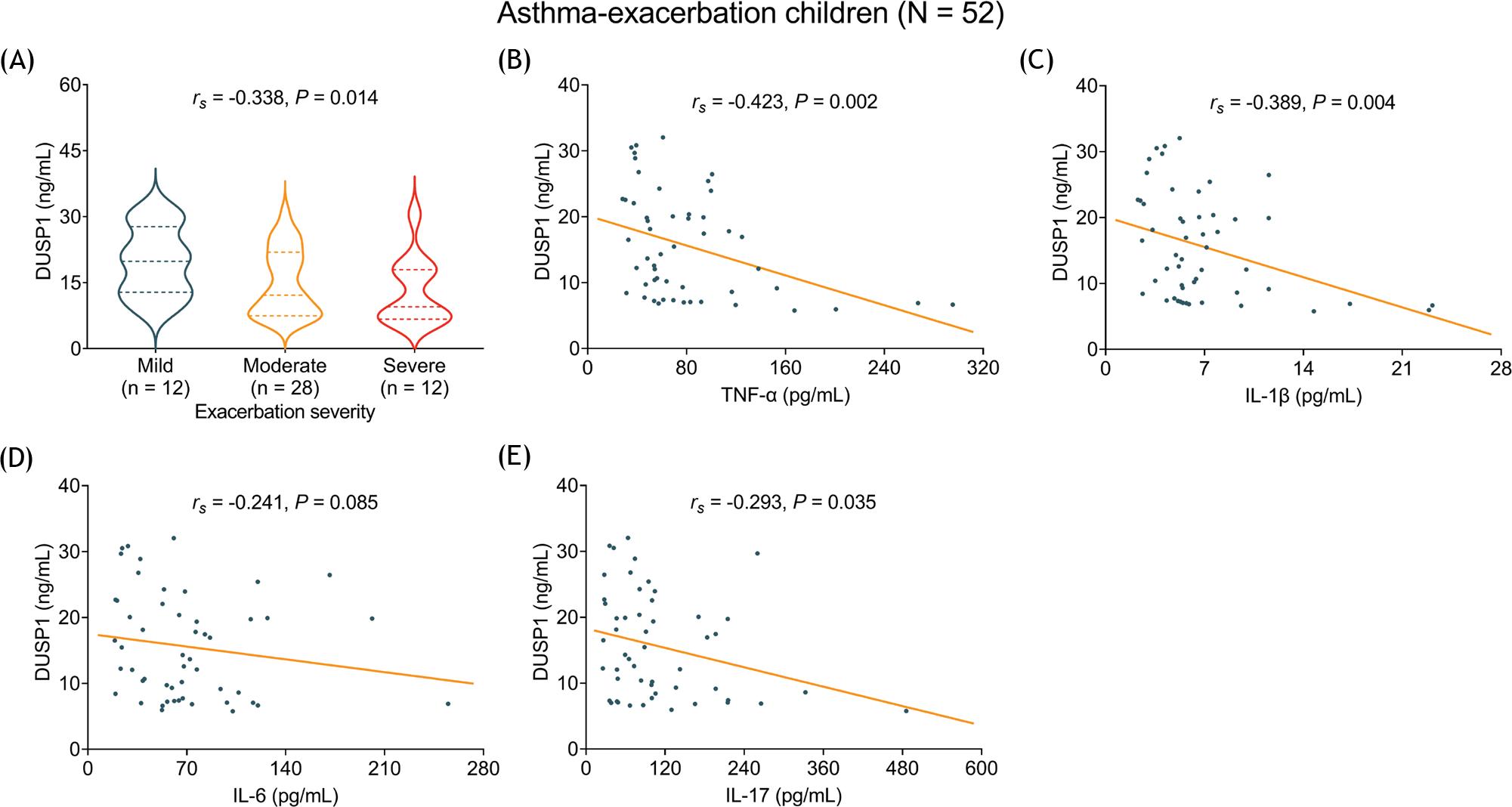
The association of DUSP1 with exacerbation severity was subsequently analyzed, and it was observed that DUSP1 was negatively associated with exacerbation severity in children with asthma-exacerbation (rs=-0.338, P=0.014) (Figure 3A). In addition, DUSP1 was negatively correlated with TNF-α (rs=-0.423, P=0.002), IL-1β (rs=-0.389, P=0.004), and IL-17 (rs=-0.293, P=0.035) in children with asthma- exacerbation. However, no correlation was observed in DUSP1 with IL-6 (rs=-0.241, P=0.085) (Figure 3B-E).
Figure 3 Correlation of DUSP1 with exacerbation severity and inflammatory cytokines. The correlation of DUSP1 with exacerbation severity: (A) TNF-α, (B) IL-1β, (C) IL-6, (D) IL-17, (E) levels in asthma-exacerbation children.
Meanwhile, DUSP1 was negatively associated with TNF-α (rs=-0.300, P=0.034) and IL-1β (rs=-0.309, P=0.029) among children in asthma-remission. However, no association was discovered in DUSP1 with IL-6 or IL-17 among children in asthma-remission, or with TNF-α, IL-1β, IL-6, or IL-17 in healthy controls (all P>0.05) (Table 2).
Table 2 Correlation of DUSP1 with inflammatory cytokines in children in asthma-remission and healthy controls
| Items | DUSP1 in asthma-remission children | DUSP1 in healthy controls | ||
|---|---|---|---|---|
| rs | P value | rs | P value | |
| TNF-α | -0.300 | 0.034 | -0.049 | 0.735 |
| IL-1β | -0.309 | 0.029 | -0.022 | 0.877 |
| IL-6 | -0.246 | 0.085 | -0.274 | 0.055 |
| IL-17 | -0.277 | 0.051 | -0.231 | 0.107 |
*DUSP1, dual-specificity phosphatase-1; TNF-α, tumor necrosis factor-α; IL-1β, interleukin-1 β; IL-6, interleukin-6; IL-17, interleukin-17
Association of DUSP1 with other disease features in asthmatic children
DUSP1 was negatively correlated with IgE among children with asthma-exacerbation (rs=-0.277, P=0.047), while no association was found in DUSP1 with eosinophil count, FEV1/FVC or FEV1 (% predicted) among children with asthma-exacerbation (all P>0.05). Additionally, no correlation was found in DUSP1 with eosinophil count, IgE, FEV1/FVC or FEV1 (% predicted) among children in asthma-remission or healthy controls (all P>0.05) (Table 3).
Table 3 Correlation of DUSP1 with disease features
| Items | DUSP1 in asthma-exacerbation children | DUSP1 in asthma-remission children | DUSP1 in healthy controls | |||
|---|---|---|---|---|---|---|
| rs | P value | rs | P value | rs | P value | |
| Eosinophil count | -0.202 | 0.151 | -0.103 | 0.478 | -0.207 | 0.150 |
| IgE | -0.277 | 0.047 | -0.134 | 0.355 | -0.077 | 0.595 |
| FEV1/FVC (%) | 0.245 | 0.080 | 0.176 | 0.222 | 0.168 | 0.242 |
| FEV1 (% predicted) | 0.157 | 0.267 | 0.194 | 0.176 | -0.023 | 0.876 |
Abbreviations: DUSP1, dual-specificity phosphatase-1; IgE, immunoglobulin E; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity
Discussion
Several previous interesting studies have investigated the DUSP1 expression in inflammation-related diseases. One study depicts that the protein expression of DUSP1 is reduced in psoriasis patients than in the controls.21 Another study reveals that DUSP1 is lower in asthmatic children compared with healthy controls.22 However, this preceding study does not investigate the level of DUSP1 between children with asthma-exacerbation and children in asthma-remission. The present study was thus conducted, and upon exploration it was found that DUSP1 was found to be the highest in healthy controls, followed by children in asthma-remission, and the lowest in children with asthma-exacerbation. The possible reasons could be that: (1) DUSP1 participated in the pathogenesis of asthma via targeting MAPK signaling, which further affected the disease development,22–24 and thus DUSP1 was lower in asthmatic children than in health controls; (2) DUSP1 is a protein with anti-inflammatory properties,25 and a higher level of inflammation could result in enhanced disease activity, and thus DUSP1 was found to be reduced in children with asthma-exacerbation than among children in asthma-remission. In addition, we also observed that DUSP1 could distinguish asthmatic children from healthy controls, and discriminate children with asthma-exacerbation from children in asthma-remission, which suggested that DUSP1 might be applied as a biomarker for the risk of asthma and asthma-exacerbation.
The exacerbation severity reflects the aggravation of asthma severity and the inflammation. According to the Global Initiative for Asthma (GINA) Strategy Report, the treatment methods of asthma patients are made based on different exacerbation severities. For instance, short-acting beta2-agonist and inhaled corticosteroids are often used for asthma patients with mild exacerbation, addon long-acting muscarinic antagonists, and azithromycin are recommended for asthma patients with moderate to severe exacerbation.26 Therefore, early identification of asthma exacerbation severity is important for guiding the treatment of asthma patients. However, the association of DUSP1 with asthma severity has not been explored yet. Therefore, this study was done and it discovered that DUSP1 was negatively associated with exacerbation severity in children with asthma-exacerbation, which could be explained by the that: DUSP1 decreases the immune response in asthma immune cells, which might subsequently suppress the chronic inflammation, further reducing exacerbation severity.14 Therefore, DUSP1 was negatively associated with exacerbation severity in asthma-exacerbation children. Furthermore, it was also found that DUSP1 was negatively correlated with IgE (a hallmark of allergic disease) in children with asthma-exacerbation, reflecting that DUSP1 might reduce the response to allergy.
According to previous studies, DUSP1 regulates the inflammation by ERK1/2 pathway and MAPK pathway,27,28 and only one study elucidates that DUSP1 potentially serves as a chronic inflammation biomarker in patients with cardiovascular disease.19 In our study, the negative correlation of DUSP1 with inflammatory cytokines was apparent in children with asthma-exacerbation, but mild in children in asthma-remission. The reasons might be that: (1) DUSP1 might suppress inflammatory and catabolic mediators by inhibiting the p38 MAPK and c-Jun N-terminal kinase signaling pathways in asthma, resulting in reduced inflammation;24 (2) since inflammation would be more obvious in asthmatic children with exacerbation than asthmatic children with remission, DUSP1 had a more evident correlation with inflammatory cytokines in children with asthma-exacerbation than in children in asthma-remission.
Although a lot of findings were identified in this study, there are still some limitations. Firstly, the sample size is not very large, and it could be expanded to improve the statistical power. Secondly, this study did not investigate the molecular mechanism of DUSP1 in asthma development and progression, thus in-vivo and in-vitro experiments might be needed in the future. Thirdly, the link between DUSP1 and its response to asthma treatment was not assessed, which could be evaluated in the subsequent study. Lastly, the current article is a case-control study, and therefore, the longitude change of DUSP1 during follow-up was not conducted.
Conclusion
In conclusion, DUSP1 reflects the decreased exacerbation risk, correlates with less advanced exacerbation severity and lower inflammatory cytokines to a certain extent in asthmatic children. These findings may prove to be a valuable information for the potency of DUSP1 as a biomarker, reflecting asthma exacerbation and inflammation.
Acknowledgements
None.
Conflict of interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
REFERENCES
1. Papadopoulos NG, Arakawa H, Carlsen KH, Custovic A, Gern J, Lemanske R, et al. International consensus on (ICON) pediatric asthma. Allergy. 2012 Aug;67(8):976–97. 10.1111/j.1398-9995.2012.02865.x
2. Papadopoulos NG, Miligkos M, Xepapadaki P. A Current Perspective of Allergic Asthma: From Mechanisms to Management. Handb Exp Pharmacol. 2022;268:69–93. 10.1007/164_2021_483
3. Chowdhury NU, Guntur VP, Newcomb DC, Wechsler ME. Sex and gender in asthma. Eur Respir Rev. 2021 Dec 31;30(162):210067. 10.1183/16000617.0067-2021
4. Trottier ED, Chan K, Allain D, Chauvin-Kimoff L. Managing an acute asthma exacerbation in children. Paediatr Child Health. 2021 Nov;26(7):438–9. 10.1093/pch/pxab058
5. Vafaee F, Shirzad S, Shamsi F, Boskabady MH. Neuroscience and treatment of asthma, new therapeutic strategies and future aspects. Life Sci. 2022 Mar 1;292:120175. 10.1016/j.lfs.2021.120175
6. Blakey J, Chung LP, McDonald VM, Ruane L, Gornall J, Barton C, et al. Oral corticosteroids stewardship for asthma in adults and adolescents: A position paper from the Thoracic Society of Australia and New Zealand. Respirology. 2021 Dec;26(12):1112–30. 10.1111/resp.14147
7. Agusti A, Fabbri L, Lahousse L, Singh D, Papi A. Single inhaler triple therapy (SITT) in asthma: Systematic review and practice implications. Allergy. 2022 Apr;77(4):1105-13. 10.1111/all.15076
8. Rogliani P, Beasley R, Cazzola M, Calzetta L. SMART for the treatment of asthma: A network meta-analysis of real-world evidence. Respir Med. 2021 Nov;188:106611. 10.1016/j.rmed.2021.106611
9. Hoppstadter J, Ammit AJ. Role of Dual-Specificity Phosphatase 1 in Glucocorticoid-Driven Anti-inflammatory Responses. Front Immunol. 2019 Jun 26;10:1446. 10.3389/fimmu.2019.01446
10. Zhang Y, Reynolds JM, Chang SH, Martin-Orozco N, Chung Y, Nurieva RI, et al. MKP-1 is necessary for T cell activation and function. J Biol Chem. 2009 Nov 6;284(45):30815–24. 10.1074/jbc.M109.052472
11. Bluestone JA, Bour-Jordan H, Cheng M, Anderson M. T cells in the control of organ-specific autoimmunity. J Clin Invest. 2015 Jun;125(6):2250–60. 10.1172/JCI78089
12. Jeong J, Lee HK. The Role of CD4(+) T Cells and Microbiota in the Pathogenesis of Asthma. Int J Mol Sci. 2021 Oct 31;22(21):11822. 10.3390/ijms222111822
13. Golebski K, van Egmond D, de Groot EJ, Roschmann KI, Fokkens WJ, van Drunen CM. EGR-1 and DUSP-1 are important negative regulators of pro-allergic responses in airway epithelium. Mol Immunol. 2015 May;65(1):43–50. 10.1016/j.molimm.2014.12.011
14. Wancket LM, Frazier WJ, Liu Y. Mitogen-activated protein kinase phosphatase (MKP)-1 in immunology, physiology, and disease. Life Sci. 2012 Feb 13;90(7–8):237–48. 10.1016/j.lfs.2011.11.017
15. Alam R, Gorska MM. Mitogen-activated protein kinase signalling and ERK1/2 bistability in asthma. Clin Exp Allergy. 2011 Feb;41(2):149–59. 10.1111/j.1365-2222.2010.03658.x
16. Pemmari A, Paukkeri EL, Hamalainen M, Leppanen T, Korhonen R, Moilanen E. MKP-1 promotes anti-inflammatory M(IL-4/IL-13) macrophage phenotype and mediates the anti-inflammatory effects of glucocorticoids. Basic Clin Pharmacol Toxicol. 2019 Apr;124(4):404–15. 10.1111/bcpt.13163
17. Yang M, Chen J, Wei W. Dimerization of glucocorticoid receptors and its role in inflammation and immune responses. Pharmacol Res. 2021 Apr;166:105334. 10.1016/j.phrs.2020.105334
18. Global Initiative for Asthma. Global strategy for asthma management and prevention. GINA report. Updated 2009. Available at http://www.ginasthma.com.
19. Khadir A, Kavalakatt S, Dehbi M, Alarouj M, Bennakhi A, Tiss A, et al. DUSP1 Is a Potential Marker of Chronic Inflammation in Arabs with Cardiovascular Diseases. Dis Markers. 2018;2018:9529621. 10.1155/2018/9529621
20. Zeng Y, Tao L, Ma J, Han L, Lv Y, Hui P, et al. DUSP1 and KCNJ2 mRNA upregulation can serve as a biomarker of mechanical asphyxia-induced death in cardiac tissue. Int J Legal Med. 2018 May;132(3):655–65. 10.1007/s00414-017-1616-4
21. Chang WJ, Niu XP, Hou RX, Li JQ, Liu RF, Wang Q, et al. LITAF, HHEX, and DUSP1 expression in mesenchymal stem cells from patients with psoriasis. Genet Mol Res. 2015 Dec 2;14(4):15793–801. 10.4238/2015.December.1.31
22. Theodorou J, Nowak E, Bock A, Salvermoser M, Beerweiler C, Zeber K, et al. Mitogen-activated protein kinase signaling in childhood asthma development and environment-mediated protection. Pediatr Allergy Immunol. 2022 Jan;33(1):e13657. 10.1111/pai.13657
23. Khorasanizadeh M, Eskian M, Gelfand EW, Rezaei N. Mitogen-activated protein kinases as therapeutic targets for asthma. Pharmacol Ther. 2017 Jun;174:112–26. 10.1016/j.pharmthera.2017.02.024
24. Peng HZ, Yun Z, Wang W, Ma BA. Dual specificity phosphatase 1 has a protective role in osteoarthritis fibroblastlike synoviocytes via inhibition of the MAPK signaling pathway. Mol Med Rep. 2017 Dec;16(6):8441–7. 10.3892/mmr.2017.7617
25. Moosavi SM, Prabhala P, Ammit AJ. Role and regulation of MKP-1 in airway inflammation. Respir Res. 2017 Aug 10;18(1):154. 10.1186/s12931-017-0637-3
26. Reddel HK, Bacharier LB, Bateman ED, Brightling CE, Brusselle GG, Buhl R, et al. Global Initiative for Asthma Strategy 2021: Executive Summary and Rationale for Key Changes. J Allergy Clin Immunol Pract. 2022 Jan;10(1S):S1-S18. 10.1016/j.jaip.2021.10.001
27. Shao LL, Gao MM, Gong JX, Yang LY. DUSP1 regulates hippo-campal damage in epilepsy rats via ERK1/2 pathway. J Chem Neuroanat. 2021 Dec;118:102032. 10.1016/j.jchemneu.2021.102032
28. Wang X, Jiang Y, Li J, Wang Y, Tian Y, Guo Q, et al. DUSP1 Promotes Microglial Polarization toward M2 Phenotype in the Medial Prefrontal Cortex of Neuropathic Pain Rats via Inhibition of MAPK Pathway. ACS Chem Neurosci. 2021 Mar 17;12(6): 966–78. 10.1021/acschemneuro.0c00567
Supplementary
Comparison of DUSP1 mRNA relative expression among asthma-exacerbation children, asthma-remission children, and healthy controls.