
Download
REVIEW ARTICLE
Psychological stress in asthma: repercussions on epigenetics-genetics, immune responses, and pulmonary function in the pediatric population
Georgia Véras de Araújo Gueiros Liraa, b*, Giselia Alves Pontes da Silvaa, Gustavo Falbo Wandalsenc, d, Emanuel Sávio Cavalcanti Sarinhoa, b
aDepartment of Pediatrics, Federal University of Pernambuco (UFPE), Pernambuco, Brazil
bCenter for Research in Allergy and Immunology at the Federal University of Pernambuco (UFPE), Pernambuco, Brazil
cDepartment of Allergy, Clinical Immunology and Rheumatology, Federal University of São Paulo (UNIFESP), São Paulo, Brazil
dDepartment of Pediatrics, Federal University of São Paulo (UNIFESP), São Paulo, Brazil
Abstract
In the assessment of childhood asthma, identifying the risk factors associated with exacerbations and broadening this view to understand psychological stress and its repercussions on the inflammatory process of asthma allow a different perspective on this biopsychosocial disease. Psychological stress, as a risk factor for the onset and noncontrol of asthma, has been increasingly evaluated from the perspective of the repercussions on the body of the stimulus generated in the hypothalamic-pituitary axis and adrenal glands, with cortisol release and immune system action. These processes trigger changes in T helper 2 cells, which polarize allergic processes, and dysfunctions in immune tolerance mechanisms, with a decrease in regulatory T cells. Genetic and epigenetic changes in β2-adrenergic and glucocorticoid receptors, with decreased response to these drugs, were also identified in studies, in addition to changes in respiratory function patterns, with worsening of obstruction and inflammation identified via decreased forced expiratory volume in one second and increased exhaled inflammatory gases in allergic asthma. Therefore, the present review sought to identify studies on the effect of personal and parental acute or chronic psychological stress, emphasizing the repercussions on genetics, epigenetics, and immune and pulmonary functional and inflammatory responses in the pediatric population.
Key words: asthma, epigenetics, immune response, lung function, stress psychological
*Corresponding author: Georgia Véras de Araújo Gueiros Lira Av. Prof. Morais Rego, 1235 – Cidade Universitária, Recife - PE, Brasil. Email address: [email protected]
Received 21 November 2021; Accepted 13 January 2022; Available online 1 March 2022
Copyright: Lira GVAG, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
The impact of asthma on the pediatric population, which has shown a growing trend in recent decades in many countries, has led to many questions and to the identification of potential risk factors for triggering asthma and clinical exacerbation.1 Environmental risk factors, climatic changes, viral respiratory infections,2–4 factors related to comorbidities, such as allergic rhinitis,5,6 behavioral factors identified by treatment nonadherence, and the psychological problems represented by, mainly, patient and carer stress are increasingly characterized as triggers of exacerbations and reasons for the lack of clinical control of asthma.7,8
The association of psychological stress with asthma has provided a different perspective of a heterogeneous and multifactorial clinical condition that biomedical assumptions solely are not able to explain, address, or manage. Urie Bronfenbrenner’s Bioecological Theory,9 grounded on the dynamic perspective of the process, person, context, and time model, allowed to expand the knowledge on the interactions between individuals and their immediate family and social environment, highlighting psychological stress as a risk factor both for the development and clinical worsening of childhood asthma.10,11
Studies have increasingly shown the influence and participation of individual and family psychological stress on the pathophysiology of asthma.12–14 Prenatal maternal stress was associated with increased production of proinflammatory cytokines detected in the umbilical cord blood, with repercussions on the fetal lung structure, causing wheezing at 2 years of age.15,16 Similarly, individual and family acute postnatal stress seems to influence the patterns of asthma-related immune responses, resulting in increased proinflammatory cytokines and clinical worsening, in addition to altering the response of inhaled corticosteroid and β2-agonist receptors.11,17
Psychological stress, when chronic and sustained, induces the release of hormones such as cortisol, which in high doses and for a prolonged time can suppress the T helper 1 (Th1) cellular immune response and exert a significant effect on humoral immunity and its effector mechanisms.17 Conversely, it is understood that the experience of psychological stress is, at any stage of life, a condition inherent to all human beings, but their ability to cope individually or through the external support of a carer can cause repercussions to the body to be attenuated or even avoided.18
The present review analyzes individual or family psychological stress as a risk factor for asthma exacerbations, highlighting the repercussions on epigenetics-genetics and immune and pulmonary functional and inflammatory responses in the pediatric population. For this purpose, searches were conducted in the PubMed/MEDLINE, Scopus, and LILACS electronic databases, with identification of original articles, published until September 2021, considered relevant to support this integrative review. The following keywords, in English and Spanish, were used: stress, psychological AND asthma; stress, psychological AND epigenesis, genetic AND asthma; stress, psychological AND asthma AND immune; stress, psychological AND asthma AND pulmonary function; stress, psychological AND asthma AND airway (resistance, obstruction, impedance, conductance, response); stress, psychological AND asthma AND airflow; stress, psychological AND asthma AND respiratory (resistance, pattern). To be included, the articles had to meet the following criteria: studies focused on human medicine, which addressed a biological, physiological, and/or pathophysiological aspect of stress, rather than having a solely psychological and/or psychosocial approach.
Psychological stress, assessment measures, and cortisol
The word stress, derived from Latin, was initially used in the 17th century to mean fatigue, tiredness, a meaning that is still found in nonacademic circles. Only in the 18th and 19th centuries did stress appear to be related to terms such as pressure, exertion, and emotional strain.19 In the twentieth century, in 1936, the Canadian physiologist Hans Selye introduced the term “stress” in the field of health to designate the general and nonspecific response of the organism to a stressor or a stressful adverse event.20
Stress is commonly defined as a condition or state in which the organism’s homeostasis is disturbed. Selye called the events that occur in response to the stress condition “general adaptation syndrome,” which has three important phases: (1) the alarm phase, in which the organism perceives the stressful stimulus; (2) the resistance phase, which consists of the organism’s attempt to adapt to the stimulus; and (3) the exhaustion phase, when the organism loses its adaptive ability and is identified as toxic.21
The perception of the stress stimulus in the environment can produce a variety of emotional, behavioral, and physiological responses in the individual. This view supports the understanding that not only the demand caused by adverse stressful events but also the way each stressful situation is interpreted, experienced, and evaluated affects an individual. The important results of this process can be measured through assessment measures that allow evaluating and measuring the effect of psychological stress on the individual.22
Assessment measures can be divided into biological measures, environmental measures (which identify stress events), and self-perceived stress measures (in which assessment instruments, in the form of questionnaires validated for different age groups, are used). The biological measures of stress have been the most advanced in recent years in the evaluation of the phenomenon, contributing to the understanding of the functioning of the organism in the face of adversities, and they can be represented by biochemical and physiological measures.23
The first biochemical measure identified was the measurement of catecholamines, especially adrenaline and norepinephrine, which are activated in the early reaction to stress but have a rapid blood circulation time. Cortisol, in turn, is considered one of the most sensitive biomarkers for the diagnosis of stress, being released in the acute phase but remaining elevated for longer.24 Because glucocorticoid receptors (GRs) are present in practically all organs and affect the functioning of the hypothalamic-pituitary-adrenal (HPA) axis, altering autonomic system and immunoregulation functions, cortisol is currently the most frequently measured hormone in studies on stress.23
Cortisol is secreted intermittently throughout the day for periods that last only a few minutes, with its highest levels occurring in the morning and lowest levels at day-end, and can be measured in plasma, sweat, urine, saliva, or hair. The biologically active form of cortisol is the free nonprotein-bound fraction, which represents approximately 10% of the plasma glucocorticoid level. Of the molecules bound to proteins (90% inactive form), 95% bind to transcortin or cortisol-binding globulin, a protein with low transport capacity and high affinity for cortisol. The remaining 5% bind to albumin, which, on the contrary, has high transport capacity and low affinity for cortisol.25
The second type of biological measure of stress is physiological, which is directly linked to the analysis of organ and tissue functioning, prioritizing the assessment of levels of wear and/or change in the functional pattern of certain body systems or structures in the face of stressful events. When chronic stress occurs, the sum of these changes can lead to the triggering of a phenomenon called increased allostatic load, which reflects the impact of the changes that the body experiences under prolonged exposure to stress, such as the impact of chronic stress on the structural conformation of the brain and lung.26,27
In parallel to the development of biological and environmental measures, innovations in self-perception instruments, through the mapping of stressors and self-measurement, have become alternative and easier ways to measure stress in clinical research.28
In studies evaluating psychological stress in the pediatric population, it is important to identify the impact of the stressful event in terms of intensity and time; in terms of the impact of stress perception and condition on the child’s intellectual, emotional, and affective development; and in terms of the availability and perception ability of adults to serve as protectors, supporters, and to help the child understand and cope with stress.29 It should thus be considered that the variety of responses to stress is mainly related to a complex and entangled network of factors associated with child development, a child’s personal relationship with a close adult, and their family and social contexts.29,30
Cortisol and the immune system
The brain is the main organ involved in the response and adaptation to stress, as it recognizes threats and determines the necessary behavioral and physiological responses. Through the senses, especially touch, hearing, and vision, stressful events in the individual’s environment are perceived, and these stimuli are connected to the emotional centers of the brain.30
The prefrontal cortex (PFC), in addition to the hippocampus and amygdala, plays an important role in regulating the stress response, and there is evidence that the left and right cerebral hemispheres perform different functions in terms of behavioral, neuroendocrine, and autonomic responses to stress stimuli, depending on the severity and duration of the stressful event. Different groups of neurons in the PFC are stimulated heterogeneously as the individual perceives stressful life events. At this time, signals are emitted to the limbic system, which is composed of the thalamus and hypothalamus, activating the sympathetic autonomic nervous system (SANS) and the HPA axis.29
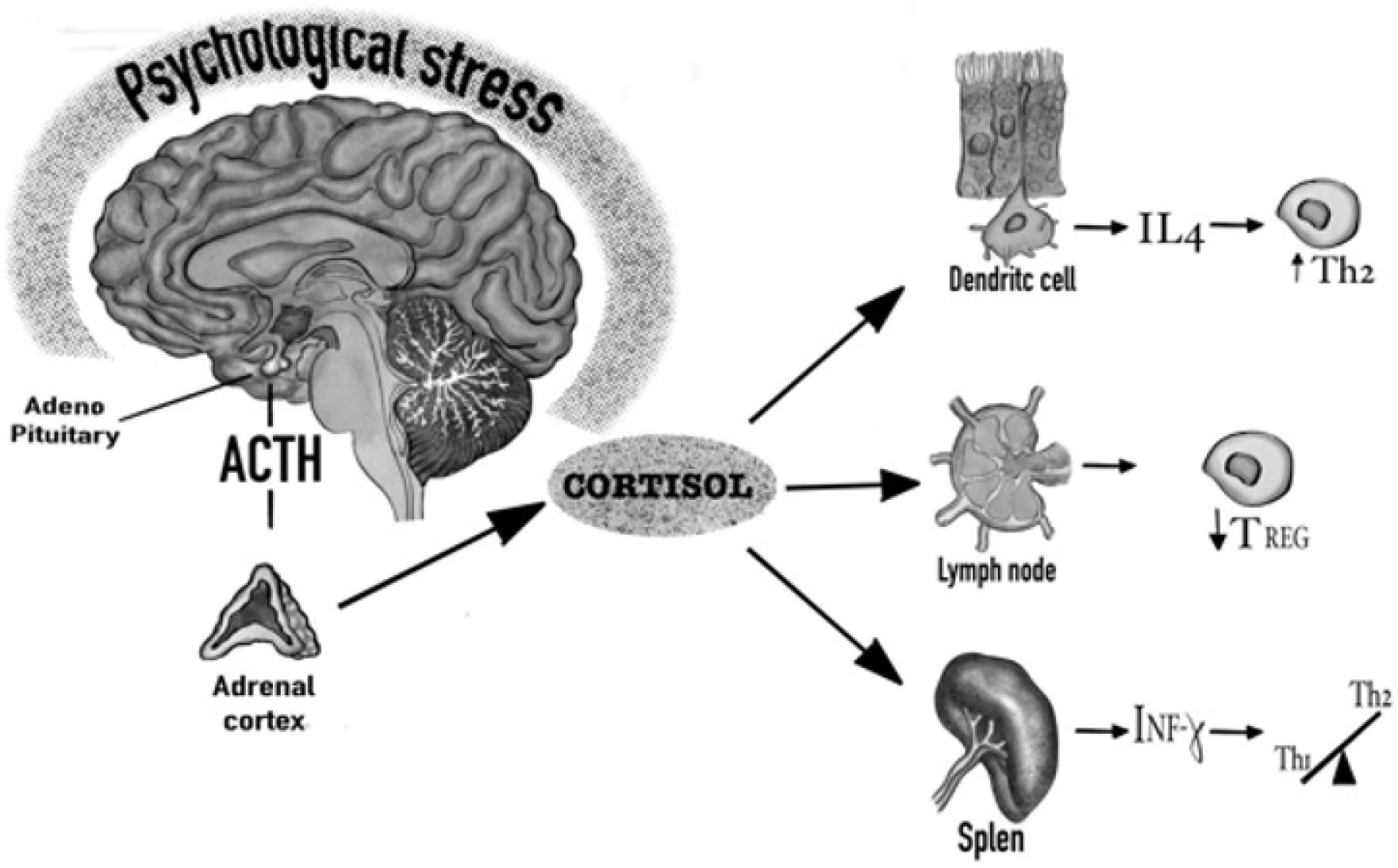
The activation of the HPA axis begins through nerve impulses originating from stress that are transmitted from the cortex to the hypothalamus. In the hypothalamus, more precisely in the locus coeruleus and paraventricular nucleus, sensory signals are processed, which induce the release of corticotropic-releasing hormone (CRH), which passes through the hypothalamic-pituitary portal system, reaching the anterior pituitary. At this site, CRH stimulates the secretion of adrenocorticotropic hormone (ACTH), which reaches the adrenal cortex via the bloodstream and induces the secretion of glucocorticoids such as cortisol (Figure 1).30
Figure 1 Stimulation of the HPA axis with release of adrenocorticotropic hormone (ACTH) by the pituitary gland and release of cortisol through the adrenal cortex. A model of interaction of cortisol with the various lymphoid and respiratory epithelium tissues, through GRs, and alterations of Th1, Th2, and Treg cells.
Glucocorticoids (GCs), along with mineralocorticoids and some sex steroids, are produced in the adrenal cortex, with the main endogenous glucocorticoid being cortisol. Cortisol is synthesized in the cortex zona fasciculata and requires cholesterol for its synthesis, which is transported to the inner mitochondrial membrane through a steroidogenic regulatory protein.31
Free cortisol has the ability to enter the target cells directly without requiring active transport. In the cytosol, cortisol binds to and activates GRs, which leads to the dissociation of heat shock proteins, allowing cortisol-GR dimerization. These dimers undergo translocation to the cell nucleus, where they activate glucocorticoid response elements in the DNA sequence, stimulating the transcription of genes regulated by glucocorticoids.31
Once cortisol exerts its activity in target cells, it is inactivated to cortisone by the microsomal enzyme 11β-hydroxysteroid dehydrogenase type 2, especially in the kidney and also in the colon and other tissues. It is important to note that cortisone also exerts glucocorticoid activity, which is, however, weaker than that of cortisol.16
Studies with animal models have shown that in stress phases, the released cortisol has the potential to bind to the GRs of dendritic cells of the respiratory epithelium of murines and promote increased release of interleukin (IL)-4, polarizing the differentiation of naïve T helper cells into Th2 cells, in addition to decreasing the concentration of CD4+FOXP3+ Treg cells in bronchial lymph nodes. In the other field of action, the spleen, there was a shift of the Th1/Th2 balance towards the Th2 responses caused by exposure to stress in mice, mainly due to the decreased expression of IFN-γ by elevated cortisol.32–34
Immunological changes were observed in individuals who were under acute and chronic influence of stressful events. Patients with posttraumatic stress disorder (PTSD) showed a significant reduction in Treg cells, both in peripheral lymph nodes and in peripheral blood mononuclear cells (PBMCs).35–37 Increased cortisol levels during psychological stress resulted in the activation of nuclear transcription factor kappa β (NF-κβ), a protein complex involved in controlling the expression of several genes linked to proinflammatory responses.38
Acute and chronic stressors also have the ability to alter mRNA expression for GRs. In T lymphocytes, GRs play a key role in regulating the expression of IL-4, IL-5, and IL-13 after exposure to allergens. Similarly, in mast cells, the expression and binding of these receptors can inhibit the release of histamine and other allergic mediators, and decrease eosinophil recruitment and activation. Therefore, changes in GRs may lead to increased expression of allergic inflammation in asthmatic patients.39
In general, changes in circulating cortisol levels are associated with an imbalance in the pattern of cytokines produced. Cortisol acting on specific immune cells generally induces suppression of the Th1 cellular immune response, exerting a significant effect on Th2 humoral immunity, with increased production of IL-4, IL-5, and IL-13, and activation of the significant immune response of allergic asthma.40
Psychological stress and asthma: genetic and epigenetic aspects
Interestingly, it has been observed that the effects of psychological stress on the human body promote changes not only in immune responses but also in epigenetics-genetics and in the response to bronchodilators and corticosteroids used in the treatment of asthma.41
There is an understanding that acute, positive, or tolerable stress does not produce long-term repercussions in the body, but when stress is chronic, it can harm the body. Chronic psychological stress can cause a counterregulatory response in lymphocyte stimulation with consequent negative regulation of the expression and/or function of GRs, leading to functional resistance to steroids.42,43 There is also evidence that psychosocial stress stimulates the production of proinflammatory cytokines in the absence of infection or injury. Table 1 describes the main studies in the pediatric population that showed the repercussions of psychological stress on genetics and epigenetics, and the changes to the receptors of the main drugs used in the treatment of asthma.8,44–47
Table 1 Repercussions of psychological stress on the genetics and epigenetics of asthma in the pediatric population.
| Study/year | Country | Study population | Population age | Main findings |
|---|---|---|---|---|
| Miller and Chen, 200644 | Canada | 77 children (59% male) with and without asthma. | Children and adolescents aged 9–18 years. | Acute and chronic stress was associated with a 9.5-fold reduced mRNA expression for the β 2-adrenergic receptor and 5.5-fold reduced expression for the glucocorticoid receptor in children with asthma. |
| Tsartsali et al., 20128 | Greece | 62 Greek children (43 boys) with asthma receiving inhaled corticosteroids. | Children and adolescents aged 5–12 years. | Single nucleotide polymorphisms (SNPs) rs1876828 and rs242941 in the corticotropin-releasing hormone receptor 1 (CRHR1) gene, T(-2C) in the promoter region of the melanocortin receptor 2 (MC2R) gene, and Bcl I restriction fragment length polymorphism in the glucocorticoid receptor (GR) gene were associated with increased baseline cortisol levels and cortisol response in stressful situations. |
| Chen et al., 201345 | USA | 516 Puerto Rican children with asthma often exposed to stressful events. | Children and adolescents aged 6–14 years. | Genetic variation in the promoter of the gene for the receptor for adenylate-cyclase activating polypeptide 1 (ADCYAP1R1). DNA methylation and single nucleotide polymorphism (SNP) in the C allele in ADCYAP1R1 were associated with asthma risk in children exposed to stressful events. |
| Ortega et al., 201346 | USA | 329 adolescents, from the 475 African-Americans selected for the study, reported stress as the main cause of exacerbations and presented with more severe asthma. | Adolescents aged over 16 years. | Genetic analysis revealed a significant difference in the distribution of genotypes among the four clusters for rs4950928, a SNP located in the CHI3L1 promoter region, the chitinase 3-like 1 gene encoding YKL-40, was observed in the context of stress and asthma severity. |
| Trump et al., 201647 | Germany | 443 mother–child pairs, a subset of the prospective mother–child cohort LINA. | Children aged up to 5 years. | Both mothers and children showed changes in DNA methylation due to stress. In children, methylation was observed in the gene of neuromedin U receptor 1 (NMUR1), a GPCR known to be involved in hypothalamic-pituitary-adrenal axis (HPA) response. |
Genetic changes can be demonstrated through the nucleotide polymorphisms of enzymes, such as adenylate cyclase, responsible for the conversion of adenosine triphosphate (ATP) into cyclic adenosine 3',5'-monophosphate (cAMP), which promotes the relaxation of airway smooth muscles and inhibits the release of bronchoconstrictor mediators by mast cells.45 Alterations can also be found in the receptors of β2-adrenergics and glucocorticoids used in the treatment of acute and chronic asthma exacerbations.44
Genetic and epigenetic variations in neurological receptors (ADCYAP1R1 and CRHR1), which regulate cortisol production in the fetus, were also associated with transplacental passage of high cortisol levels to the fetus in pregnant women who were under acute and chronic stress.8
β2-adrenergic receptors (β2ARs) and GRs are the starting points for a series of signaling pathways that regulate airway responsiveness and inflammation. In the airways, β2AR activation facilitates bronchial relaxation by smooth muscle cells. In T lymphocytes, β2ARs and GRs play important roles in regulating the expression of IL-4, IL-5, and IL-13 after allergen exposure. Thus, as changes in the mRNA of β2ARs and GRs are observed, with decreased cell expression, children with asthma may become more vulnerable to airway inflammation and bronchoconstriction after exposure to allergic triggers. In addition to these direct influences on the airways and immune function, negative regulation related to cortisol may decrease the sensitivity to β2-agonists and glucocorticoids, which are essential for effective asthma management.44,48
Abusive and unstable family relationships have the potential to trigger psychological stress between carers and children in the home environment. In this regard, the results from recent studies have shown that parental stress is prospectively associated with wheezing in childhood and that the onset of childhood asthma is more common in families with parents who have difficulty managing stress.49,50,51 In addition, there is growing evidence that stressors outside the family environment, such as exposure to violence in the community, are associated with a higher frequency of symptoms in children with asthma. Collectively, these findings suggest that in children and adolescents with asthma, the quality of life at home and family and community relationships are important determinants of health and well-being and seem to have stronger effects than other domains of life, such as academic ones.18
Another important aspect is that acute stressful events alone do not influence gene expression, but when they are added to a chronic stressful event, the strength of this association bolsters changes. Patients under psychological stress may have difficulty accurately assessing asthma symptoms and detecting clinical worsening. In addition, an individual may have health expectations and interpretations altered by stress, thus affecting the perception related to medication adherence and treatment self-management, resulting in noncontrol of asthma.52
Epigenetic disturbances in DNA methylation caused by stress are nonrandom and preferentially occur in potentiating elements that regulate more than one gene in the genome, which may contribute to the broad ramifications for child health also attributed to prenatal maternal stress.47 A meta-analysis published by Flanigan et al. examined the impact of the type of stressor and the exposure time during pregnancy. The analysis found an association between any psychological stress that occurred during prenatal care and increased persistent wheezing and current asthma in children. When considering the time of exposure to any stress, only the stress assessed in the third trimester was significantly associated with current asthma, while the assessment of stress indicators in the second trimester was significantly associated with wheezing in childhood.53
The role of the placenta also deserves special attention in future studies relating psychological stress and asthma. The traffic of information between the fetal and placental compartments is necessary for normal fetal development. Changes induced by the environment in these signaling networks may negatively influence development, impacting pulmonary organogenesis and programming future respiratory diseases. Although the mechanisms are complex and not fully understood, the functioning of the maternal and fetal HPA axis and cortisol production plays important roles. Maternal stress impairs the physiological regulation of the placenta upon exposure to fetal cortisol. For example, chronic maternal stress has been shown to decrease the regulation of placental 11-β-hydroxysteroid dehydrogenase type 2 (11β-HSD2), increase fetal exposure to cortisol, alter the fetal HPA axis development, and increase fetal cortisol.14,54
Psychological stress and immunological responses in asthma
Cortisol alters innate and adaptive immune responses in asthma, modifies the action of natural killer cells and the proliferation of T cells, promotes higher expression of the IL-2 receptor, and alters the production of interferon IFN-γ and the expression of IL-12. By suppressing immunity mediated by Th1 cells and cytokines, such as IL-12 and IFN-γ, psychological stress can alter the immune response toward a Th2 phenotype, which can aggravate and intensify airway inflammation after exposure to any inhaled antigen.55 Some studies have shown, both by the causal direction and by the temporal order of events, that when asthmatic patients are exposed to stressful events, such as participating in academic challenges, or living chronically in a low socioeconomic status (SES) environment, or with family members under chronic stress, they have higher serum eosinophil counts, a higher number of Th2 lymphocytes in response to allergic triggers, and increased in vitro production of cytokines identified in asthma, such as IL-4, IL-5, and IL-13. Stressful events also accentuate the airway inflammatory response to allergen challenges (Table 2).56–63
Table 2 Repercussions of psychological stress on the immune system in the pediatric population.
| Study/year | Country | Study population | Population age | Main findings |
|---|---|---|---|---|
| Kang et al., 199656 | USA | 35 asthmatic and 29 healthy adolescents were subjected to stress from academic tests. | Adolescents aged 14–18 years | Academic tests resulted in a significant decrease in the cytolytic activity of natural killer (NK) cells. During the final examination week, the number of CD56+ cells increased and of CD16+ cells remained similar to baseline values. There was a general increase in the CD4+/CD8+ ratio during and after the tests. |
| Kang et al., 199757 | USA | 21 asthmatic and 13 healthy adolescents subjected to stressful life events were evaluated throughout the school year. | Adolescents aged 14–18 years | The cells of asthmatic individuals released significantly more serum IL-4 and IL-5 during and after the school exam period. |
| Chen et al., 200358 | USA | 30 adolescents with persistent asthma were evaluated for the influence of socioeconomic status (SES) and stressful life events. | Adolescents aged 13–18 years | Adolescents with low SES had significantly higher IL-5 and IFN-γ levels, in addition to lower morning cortisol values, compared to the high SES group. |
| Wright et al., 200459 | USA | 499 children with a history of family members with asthma/allergies and under psychological stress. | Children in early childhood, aged 18–32 months | Increased carer psychological stress was associated with an early immune response to Der f 1 and Bla g 2 in the first 6 months after birth. Higher stress between the ages of 6 and 18 months was associated with a high total IgE level and increased TNF-α production. |
| Chen et al., 200660 | Canada | 37 children and adolescents with asthma and 39 healthy ones were evaluated for SES and stressful life events. | Children and adolescents aged 9–18 years | Children with asthma and lower SES and greater exposure to stressful life events were associated with increased production of IL-5 and IL-13 and increased eosinophils. |
| Wolf et al., 200861 | Canada | 50 children with asthma and 33 healthy children. | Children and adolescents aged 9–18 years | Asthmatic children living in an environment with parental stress had increased serum IL-4 and eosinophil cationic protein (ECP). |
| Marin et al., 200962 | Canada | 71 children with asthma and 76 healthy children exposed to acute and chronic stressful events. | Children and adolescents aged 9–18 years | Children with chronic family stress showed increased production of IL-4, IL-5, and IFN-γ. |
| Miller et al., 200963 | Canada | 67 children with asthma and 76 healthy children. | Children and adolescents aged 9–18 years | Children were more resistant to hydrocortisone’s anti-inflammatory effects on IL-5 and IFN-γ production and had higher eosinophil and ECP levels. These associations were independent of SES, exposure to cigarettes, disease severity, and use of medications. |
In the study by Marin et al., the production of inflammatory cytokines was evaluated among asthmatic individuals living in a family environment under chronic stress who experienced acute stressful life events. The results indicated that the increase in IL-4 and IL-5 production, caused by psychological stress, was associated with symptom exacerbation and clinical worsening of asthma.51
Inflammatory responses in allergic asthma are mostly caused by eosinophil infiltration and increased IgE production by stimulation of IL-4, IL-5, and IL-13 of the Th2 response pattern. In turn, regulatory T cells, which play a crucial role in the balance of this immune network by suppressing or limiting immune responses and promoting immune tolerance, appear to be impaired in prolonged periods of psychological stress, favoring imbalance and the potentiation of clinical manifestations of asthma.64
Some studies have shown that the number of Treg cells in the peripheral blood of patients with PTSD is significantly lower than that in non-PTSD subjects. It was also observed that an acute stressful event decreased the number of CD4+FOXP3+ Treg cells in human peripheral blood, which may lead to an imbalance in immune tolerance. Allergic manifestations and those of diseases related to immune disorders are more frequently observed in situations where immunological tolerance is lost.37,38
It is important to note that studies conducted in the pediatric population showed a higher expression of Th2-pattern cytokines, in addition to the release of higher serum levels of IgE and eosinophil cationic protein in the group of patients with asthma who were under the stimulus of negative emotions or situations of personal or parental stress.58,59,61,62
Psychological stress: pulmonary function and inflammation in asthma
Over time, studies have increasingly shown the repercussions of psychological stress on lung inflammation and function, with a significant decrease in forced expiratory volume in one second (FEV1) and forced vital capacity (FVC), in addition to changes in the fraction of exhaled nitric oxide (FeNO) (Table 3).65–74
Table 3 Effects of psychological stress on pulmonary function and inflammation in asthma in the pediatric population.
| Study/year | Country | Study population | Population age | Main findings |
|---|---|---|---|---|
| Miklich et al., 197365 | USA | 29 asthmatic adolescents were divided into three groups receiving mild, strong, and no emotional interventions. | Adolescents aged 11–16 years. | There was no significant difference in peak expiratory flow rate (PEFR) values between the groups; on the contrary, there was continuous shortening of the inspiration phases during strong emotional interventions. |
| Hollaender and Florin, 198266 | Germany | 14 asthmatic children and 14 healthy children were evaluated after stressful situations. | Children and adolescents aged 9–11 years. | The PEFR of asthmatic children was significantly reduced in the course of a frustrating situation and in negative emotions compared to the control group. |
| Florin et al., 198567 | Germany | 18 children with asthma and 18 healthy children were evaluated in terms of forced expiratory volume in one second (FEV1) pre- and post-test, after emotional stimuli. | Children and adolescents aged 7–12 years. | There was a significant decrease in pre- and post-bronchodilator FEV1 in the group of asthmatic children. |
| Rietveld et al., 199968 | Netherlands | 30 adolescents with asthma and 20 normal controls were evaluated for FEV1 and forced vital capacity (FVC) after stressful stimuli. | Adolescents aged 14–19 years. | Shortness of breath was greater in the asthmatic group, but there was no significant difference in FEV1 or FVC between the groups. |
| McQuaid et al., 200069 | USA | 114 children with asthma and 30 healthy controls were subjected to stressful tasks and evaluated for airway resistance. | Children and adolescents aged 9–15 years. | The entire sample showed a trend toward increased airway resistance in response to stress and a portion of asthmatic patients (22%) had an increase of more than 20% in baseline airway resistance. |
| Levy et al., 200470 | USA | 78 asthmatic children and adolescents were evaluated for allergies and pulmonary function, under stressful conditions, in different neighborhoods of the same city. | Children and adolescents aged 4–17 years. | 49 children who underwent spirometry had a mean FEV1 of 88% (median of 88%, standard deviation of 15%), and 29% of the children had FEV1 lower than 80% of the predicted value, although the values were not lower than 60% of the predicted value. |
| Chen et al., 201071 | Canada | 38 asthmatic adolescents and 23 healthy controls were evaluated regarding the fraction of exhaled nitric oxide (FeNO) levels and pulmonary function after stressful conflicts with parents. | Adolescents aged 10–20 years. | For asthmatic adolescents, there was an inverse association of SES with changes in FeNO levels in response to the conflict task, which means that as the SES decreased, greater increases in FeNO were observed. No changes in FEV1 were found in response to the conflict task. |
| Islam et al., 201172 | USA | 173 asthmatic adolescents from eight communities in Southern California were selected to reflect a broad range of exposure to air pollutants and assess lung function and interaction with parental stress. | Adolescents aged 10–18 years. | Among asthmatic adolescents from high-stress families, there were deficits in FEV1 and FVC, and they were associated with increased total oxides of nitrogen (Nox) in homes and schools. These pollutant effects were significantly larger in the high-stress compared with lower-stress households |
| Ritz et al., 201473 | USA | 39 asthmatic adolescents and 41 healthy controls were evaluated for FeNO levels and pulmonary function after stressful situations. | Adolescents older than 14 years. | Increases in FeNO levels were associated with stressful experiences in asthmatic adolescents, but there was no significant difference in FEV1. |
| Brehm et al., 201548 | Puerto Rico | 234 asthmatic patients in three cohorts subjected to stressful life events. | Children and adolescents aged 6–14 years | Puerto Rican asthmatic children and adolescents, who were highly stressed and whose mothers had a high level of stress, had a reduction in FEV1, even after bronchodilator administration. |
| Landeo-Gutierrez et al., 202074 | Puerto Rico | 678 children and adolescents were evaluated regarding psychosocial stress at home and exposure to pollutants (e.g., nitric oxide, nitrogen dioxide, total nitrogen oxides) and lung function. | Children and adolescents aged 6 to 14 years | The effects of pollutants on lung function were significantly higher among children from high-stress compared to low-stress families, after correcting for socioeconomic factors. Children who experienced a high level of stress had lower FEV1 and FVC in relation to increased environmental exposure to nitric oxide. |
An early study from 1973, which identified the physiological response of the lung in asthmatic children subjected to stressful life events, showed the involvement of the autonomic nervous system with negative emotions, leading to autonomic imbalance in asthma.65
Stressful events in the lives of asthmatic children, especially when combined with low SES, occurrence of school difficulties, alcoholism and mental illness in the family, increased the likelihood of new asthma exacerbations.48,71 Subjects experiencing chronic stress are often exposed to risk factors that lead to worse asthma control, including poverty, smoking, passive smoking, internal and external pollutants, limited access to health care or medications, reduced adherence to control medications, and a lack of care for physical well-being, affecting lung function and inflammation.64
Treatment adherence, highly necessary in chronic diseases such as asthma, is often hindered by exposure to psychological stress that carers or patients experience, in addition to the financial difficulties arising not only from the need for medication but also from the cost of reorganizing the domestic environment to reduce exposure to factors that can trigger crises.71
This review identifies some strengths and limitations that can be clarified with further studies. First, some of the limitations of review studies are that some research protocols and methods were not well described or outlined, and some studies may have been excluded because they are considered ineligible. Second, although not fully considered a limitation, by emphasizing only aspects related to psychological stress, studies that reported anxiety and depression were not included, which however allowed a detailed and exclusive view of the repercussions of psychological stress on asthma.
Despite these limitations, this review has a number of important strengths. It specifically addresses the repercussions of psychological stress on asthma, presenting epigenetic-genetic, immunological, and pulmonary function changes in a pediatric population. Finally, this review examined a variety of physiological responses relevant to stress in asthma, including HPA axis responses in the respiratory tract, for both active and passive stressors, which allows us to conclude on the different pathways by which psychological stress affects asthma.
Conclusions
The repercussions of psychological stress found in this review underscore the impact of emotional factors on the daily lives of children and adolescents with asthma, highlighting the genetic and epigenetic changes modifying, especially, the β2-adrenergic and GRs and Th2/Th1 and Treg cytokine patterns, in addition to the important repercussions on lung inflammation and function, with reduced FEV1 and increased FeNO.
Future studies would benefit from a prospective design for evaluating the causal relationships between exposure to psychological stress, hormonal dynamics of the HPA axis, and evaluation of airway cytokines in the pediatric population, following the example of animal studies. Experiencing an acute stressful life event, in addition to chronic stress, is predictive of harmful inflammatory responses that suggest that psychosocial interventions may have important biological implications for children and adolescents with asthma.
The child must be viewed in a complete and integrated way to the environment, to the family and to the historical moment in which she lives, with the psyche being the organizing core of these different aspects. Improving our understanding of which phases of psychological stress (alert, resistance, or exhaustion) are associated with the lack of clinical control of asthma and which phenotypes and endotypes of asthma may have greater repercussions shows the complexity of this topic in the approach and management of stress in the pediatric population. It is important to note that effective intervention measures, such as providing referrals to social workers or mental health professionals when appropriate, in addition to public health policies, are necessary to reduce the impact of stressful events on the lives of children and adolescents with asthma.
REFERENCES
1. Martinez FD. Childhood asthma inception and progression: role of microbial exposures, susceptibility to viruses and early allergic sensitization. Immunol Allergy Clin North Am. 2019;39(2):141–50. 10.1016/j.iac.2018.12.001
2. Duff AL, Pomeranz ES, Gelber LE, Price GW, Farris H, Hayden FG, et al. Risk factors for acute wheezing in infants and children: viruses, passive smoke, and IgE antibodies to inhalant allergens. Pediatrics. 1993;92:535-40. http://pediatrics.aappublications.org/content/92/4/535
3. Moraes LSL, Takano OA, Mallol J, Solé D. Risk factors associated with wheezing in infants. J Pediatr (Rio J). 2014;89(6):559–66. 10.1016/j.jped.2013.04.004
4. Just J, Belfar S, Wanin S, Pribil C, Grimfeld A, Duru G. Impact of innate and environmental factors on wheezing persistence during childhood. J Asthma. 2010;47(4):412–16. 10.3109/02770900903584035
5. Patra S, Singh V, Chandra J, Kumar P, Tripathi M. Diagnostic modalities for gastro-esophageal reflux in infantile wheezers. J Trop Pediatr. 2011;57(2):99-103. 10.1093/tropej/fmq056
6. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. Allergic rhinitis and its impact on asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA2LEN and AllerGen). Allergy Eur J Allergy Clin Immunol. 2008;63(Suppl. 86):8–160. 10.1111/j.1398-9995.2007.01620.x
7. Engelkes M, Janssens HM, De Jongste JC, Sturkenboom MCJM, Verhamme KMC. Medication adherence and the risk of severe asthma exacerbations: a systematic review. Eur Respir J. 2015;45(2):396–407. 10.1183/09031936.00075614
8. Tsartsali L, Papadopoulos M, Lagona E, Papadimitriou A, Kanaka-Gantenbein C, Louizou E, et al. Association of hypothalamic-pituitary-adrenal axis-related polymorphisms with stress in asthmatic children on inhaled corticosteroids. Neuroimmunomodulation. 2012;19(2):88–95. 10.1159/000329592
9. Bronfenbrenner U. Ecology of the family as a context for human development. Dev Psychol. 1986;22(6):723–42. 10.1037/0012-1649.22.6.723
10. Guttman HA. The epigenesis of the family system as a context for individual development. Fam Process. 2002;41(3):533–45. 10.1111/j.1545-5300.2002.41315.x
11. Akcan N, Bahceciler NN. Headliner in physiology and management of childhood asthma: hypothalamic-pituitary-adrenal axis. Curr Pediatr Rev. 2019;16(1):43–52. 10.2174/1573396315666191026100643
12. Bucci M, Silve S, Oh D, Harris NB. Toxic stress in children and adolescents. Adv Pediatr. 2016;63:403–28. 10.1016/j.yapd.2016.04.002
13. Lee AG, Wright RJ. Evidence establishing a link between prenatal and early-life stress and asthma development. Curr Opin Allergy Clin Immunol. 2018;18(2):148–58. 10.1097/ACI.0000000000000421
14. Lim R, Fedulov AV, Kobzik L. Maternal stress during pregnancy increases neonatal allergy susceptibility: role of glucocorticoids. Am J Physiol Lung Cell Mol Physiol. 2014;307(2):L141–L148. 10.1152/ajplung.00250.2013
15. Beijers R, Jansen J, Riksen-Walraven M, de Weerth C. Maternal prenatal anxiety and stress predict infant illnesses and health complaints. Pediatrics. 2010;126(2):e401–e409. 10.1542/peds.2009-3226
16. Gruenberg DA, Wright RJ, Visness CM, Jaffee KF, Bloomberg GR, Cruikshank WW, et al. Relationship between stress and cytokine responses in inner-city mothers. Ann Allergy Asthma Immunol. 2015;115(5):439-45. 10.1016/j.anai.2015.07.021
17. Ritz T, Ayala ES, Trueba AF, Vance CD, Auchus RJ. Acute stress-induced increases in exhaled nitric oxide in asthma and their association with endogenous cortisol. Am J Respir Crit Care Med. 2011;183(1):26–30. 10.1164/rccm.201005-0691OC
18. Garner AS. Home visiting and the biology of toxic stress: opportunities to address early childhood adversity. Pediatrics. 2013;132(Suppl):S65–S73. 10.1542/peds.2013-1021D
19. Farias FR. Sobre o conceito de estresse. Arq. bras. Psic. 1985;38(4):97–105.
20. Margis R, Picon P, Cosner AF, Silveira RDO. Stressfull life-events, stress and anxiety. R Psiquiatr. 2003;25(Suppl 1):65–74. 10.1590/S0101-81082003000400008
21. Pagliarone AC, Sforcin JM. Stress: review about the effects on the immune system. Biosaúde. 2009;11(1):57–90.
22. Chen E, Miller GE. Stress and inflammation in exacerbations of asthma. Brain Behav Immun. 2007;21(8):993–99. 10.1016/j.bbi.2007.03.009
23. Pereira ME. Medidas do estresse: uma revisão narrativa. André Faro & Marcos Emanoel Pereira. Psicologia Saúde & Doenças. 2013;14(1):101–24.
24. Elenkov IJ. Glucocorticoids and the Th1/Th2 balance. Ann N Y Acad Sci. 2004;1024:138–46. 10.1196/annals.1321.010
25. Khansari DN, Murgo AJ, Faith RE. Effects of stress on the immune system. Immunol Today. 1990;11(5):170–5. 10.1016/0167-5699(90)90069-L
26. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–96. 10.2307/2136404
27. Rosenkranz MA, Busse WW, Sheridan JF, Crisafi GM, Davidson RJ. Are there neurophenotypes for asthma? Functional brain imaging of the interaction between emotion and inflammation in asthma. PLoS One. 2012;7(8):1–12. 10.1371/journal.pone.0040921
28. Siqueira Reis R, Ferreira Hino AA, Romélio Rodriguez Añez C. Perceived stress scale. J Health Psychol. 2010;15(1):107–14. 10.1177/1359105309346343
29. Handa RJ, Weiser MJ. Gonadal steroid hormones and the hypothalamo-pituitary-adrenal axis. Front Neuroendocrinol. 2014;35(2):197–220. 10.1016/j.yfrne.2013.11.001
30. Plourde A, Lavoie KL, Raddatz C, Bacon SL. Effects of acute psychological stress induced in laboratory on physiological responses in asthma populations: a systematic review. Respir Med. 2017;127:21–32. 10.1016/j.rmed.2017.03.024
31. Barsegyan A, Mackenzie SM, Kurose BD, McGaugh JL, Roozendaal B. Glucocorticoids in the prefrontal cortex enhance memory consolidation and impair working memory by a common neural mechanism. Proc Natl Acad Sci U S A. 2010;107(38):16655–16660. 10.1073/pnas.1011975107
32. Wiley RE, Cwiartka M, Alvarez D, Mackenzie DC, Johnson JR, Goncharova S, et al. Transient corticosteroid treatment permanently amplifies the Th2 response in a murine model of asthma. J Immunol. 2004;172(8):4995–5005. 10.4049/jimmunol.172.8.4995
33. Olsen PC, Kitoko JZ, Ferreira TP, De-Azevedo CT, Arantes AC, Martins MA. Glucocorticoids decrease treg cell numbers in lungs of allergic mice. Eur J Pharmacol. 2015;747:52–8. 10.1016/j.ejphar.2014.11.034
34. Okuyama K, Dobashi K, Miyasaka T, Yamazaki N, Kikuchi T, Sora I, et al. The involvement of glucocorticoids in psychological stress-induced exacerbations of experimental allergic asthma. Int Arch Allergy Immunol. 2014;163(4):297–306. 10.1159/000360577
35. Sommershof A, Aichinger H, Engler H, Adenauer H, Catani C, Boneberg EM, et al. Substantial reduction of naïve and regulatory T cells following traumatic stress. Brain Behav Immun. 2009;23(8):1117–24. 10.1016/j.bbi.2009.07.003
36. Jergović M, Bendelja K, Vidović A, Savić A, Vojvoda V, Aberle N, et al. Patients with posttraumatic stress disorder exhibit an altered phenotype of regulatory T cells. Allergy Asthma Clin Immunol. 2014;10(1):1–9. 10.1186/1710-1492-10-43
37. Freier E, Weber CS, Nowottne U, Horn C, Bartels K, Meyer S, et al. Decrease of CD4+FOXP3+ T regulatory cells in the peripheral blood of human subjects undergoing a mental stressor. Psychoneuroendocrinology. 2010;35(5):663–73. 10.1016/j.psyneuen.2009.10.005
38. Bierhaus A, Wolf J, Andrassy M, Rohleder N, Humpert PM, Petrov D, et al. A mechanism converting psychosocial stress into mononuclear cell activation. Proc Natl Acad Sci U S A. 2003;100(4):1920–25. 10.1073/pnas.0438019100
39. Haczku A, Panettieri RA. Social stress and asthma: the role of corticosteroid insensitivity. J Allergy Clin Immunol. 2010;125(3):550–58. 10.1016/j.jaci.2009.11.005
40. Miyasaka T, Dobashi-okuyama K, Takahashi T. Allergology international the interplay between neuroendocrine activity and psychological stress-induced exacerbation of allergic asthma. Allergol Int. 2018;67(1):32–42. 10.1016/j.alit.2017.04.013
41. Rican P, American A. Current perspectives stress and asthma: novel insights on genetic, epigenetic, and immunologic mechanisms. J Allergy Clin Immunol. 2014;134(5):1009-15. 10.1016/j.jaci.2014.07.005
42. Wright RJ. Perinatal stress and early life programming of lung structure and function. Biol Psychol. 2010;84(1):46–56. 10.1016/j.biopsycho.2010.01.007
43. Bennett JM, Rohleder N, Sturmberg JP. Biopsychosocial approach to understanding resilience: stress habituation and where to intervene. J Eval Clin Pract. 2018;24(6):1339–46. 10.1111/jep.13052
44. Miller GE, Chen E. Life stress and diminished expression of genes encoding glucocorticoid receptor and beta2-adrenergic receptor in children with asthma. Proc Natl Acad Sci. 2006;103(14):5496–5501. 10.1073/pnas.0506312103
45. Chen W, Boutaoui N, Brehm JM, Han YY, Schmitz C, Cressley A, et al. ADCYAP1R1 and asthma in Puerto Rican children. Am J Respir Crit Care Med. 2013;187(6):584–88. 10.1164/rccm.201210-1789OC
46. Ortega H, Prazma C, Suruki RY, Li H, Anderson WH. Association of CHI3L1 in African-Americans with prior history of asthma exacerbations and stress. J Asthma. 2013;50(1):7–13. 10.3109/02770903.2012.733991
47. Trump S, Bieg M, Gu Z, Thürmann L, Bauer T, Bauer M, et al. Prenatal maternal stress and wheeze in children: novel insights into epigenetic regulation. Sci Rep. 2016;6:1–14. 10.1038/srep28616
48. Brehm JM, Ramratnam SK, Tse SM, Croteau-Chonka DC, Pino-Yanes M, Rosas-Salazar C, et al. Stress and bronchodilator response in children with asthma. Am J Respir Crit Care Med. 2015;192(1):47–56. 10.1164/rccm.201501-0037OC
49. Landeo-Gutierrez J, Celedón JC. Chronic stress and asthma in adolescents. Ann Allergy Asthma Immunol. 2020;125(4):393–98. 10.1016/j.anai.2020.07.001
50. Bucci M, Marques SS, Oh D, Harris NB. Toxic stress in children and adolescents. Adv Pediatr. 2016;63(1):403–28. 10.1016/j.yapd.2016.04.002
51. Hornor G. Childhood trauma exposure and toxic stress: What the PNP needs to know. J Pediatr Heal Care. 2015;29(2):191–98. 10.1016/j.pedhc.2014.09.006
52. Barnthouse M, Jones BL. The impact of environmental chronic and toxic stress on asthma. Clin Rev Allergy Immunol. 2019;57(3):427–38. 10.1007/s12016-019-08736-x
53. Flanigan C, Sheikh A, DunnGalvin A, Brew BK, Almqvist C, Nwaru BI. Prenatal maternal psychosocial stress and offspring’s asthma and allergic disease: A systematic review and meta-analysis. Clin Exp Allergy. 2018;48(4):403-14. 10.1111/cea.13091
54. Khashan AS, Wicks S, Dalman C, Henriksen TB, Li J, Mortensen PB, et al. Prenatal stress and risk of asthma hospitalization in the offspring. Psychosom Med. 2012;74(6):635–41. 10.1097/PSY.0b013e31825ac5e7
55. Liu LY, Coe CL, Swenson CA, Kelly EA, Kita H, Busse WW. School examinations enhance airway inflammation to antigen challenge. Am J Respir Crit Care Med. 2002;165(8):1062–67. 10.1164/ajrccm.165.8.2109065
56. Kang DH, Christopher LC, McCarthy DO. Academic examinations significantly impact immune responses, but not lung function, in healthy and well-managed asthmatic adolescents. Brain Behav Immun. 1996;10(2):164–81. 10.1006/brbi.1996.0015
57. Kang DH, Coe CL, McCarthy DO, Jarjour NN, Kelly EA, Rodriguez RR, et al. Cytokine profiles of stimulated blood lymphocytes in asthmatic and healthy adolescents across the school year. J Interf Cytokine Res. 1997;17(8):481–87. 10.1089/jir.1997.17.481
58. Chen E, Fisher EB, Bacharier LB, Strunk RC. Socioeconomic status, stress, and immune markers in adolescents with asthma. Psychosom Med. 2003;65(6):984–92. 10.1097/01.PSY.0000097340.54195.3C
59. Wright RJ, Finn P, Contreras JP, Cohen S, Wright RO, Staudenmayer J, et al. Chronic caregiver stress and IgE expression, allergen-induced proliferation, and cytokine profiles in a birth cohort predisposed to atopy. J Allergy Clin Immunol. 2004;113(6):1051–57. 10.1016/j.jaci.2004.03.032
60. Chen E, Hanson MD, Paterson LQ, Griffin MJ, Walker HA, Miller GE. Socioeconomic status and inflammatory processes in childhood asthma: the role of psychological stress. J Allergy Clin Immunol. 2006;117(5):1014–20. 10.1016/j.jaci.2006.01.036
61. Wolf JM, Miller GE, Chen E. Parent psychological states predict changes in inflammatory markers in children with asthma and healthy children. Brain Behav Immun. 2008;22(4):433–41. 10.1016/j.bbi.2007.10.016
62. Marin TJ, Chen E, Munch JA, Miller GE. Double-exposure to acute stress and chronic family stress is associated with immune changes in children with asthma. Psychosom Med. 2009;71(4):378–84. 10.1097/PSY.0b013e318199dbc3
63. Miller GE, Gaudin A, Zysk E, Chen E. Parental support and cytokine activity in childhood asthma: the role of glucocorticoid sensitivity. J Allergy Clin Immunol. 2009;123(4):824–30. 10.1016/j.jaci.2008.12.019
64. Landeo-Gutierrez J, Forno E, Miller GE, Celedón JC. Exposure to violence, psychosocial stress, and asthma. Am J Respir Crit Care Med. 2020;201(8):917–22. 10.1164/rccm.201905-1073PP
65. Miklich DR, Rewey HH, Weiss JH, Kolton S. A preliminary investigation of psychophysiological responses to stress among different subgroups of asthmatic children. J Psychosom Res. 1973;17(1):1–8. 10.1016/0022-3999(73)90080-9
66. Hollaender J, Florin I. Expressed emotion and airway conductance in children with bronchial asthma. J Psychosom Res. 1983;27(4):307–11. 10.1016/0022-3999(83)90053-3
67. Florin I, Freudenberg G, Hollaender J. Facial expressions of emotion and physiologic reactions in children with bronchial asthma. Psychosom Med. 1985;47(4):382–93. 10.1097/00006842-198507000-00008
68. Rietveld S, Van Beest I, Everaerd W. Stress-induced breathlessness in asthma. Psychol Med. 1999;29(6):1359–66. 10.1017/S0033291799008958
69. McQuaid EL, Fritz GK, Nassau JH, Lilly MK, Mansell A, Klein RB. Stress and airway resistance in children with asthma. J Psychosom Res. 2000;49(4):239–45. 10.1016/S0022-3999(00)00173-2
70. Levy JI, Welker-Hood LK, Clougherty JE, Dodson RE, Steinbach S, Hynes HP. Lung function, asthma symptoms, and quality of life for children in public housing in Boston: a case-series analysis. Environ Heal A Glob Access Sci Source. 2004;3:1–12. 10.1186/1476-069X-3-13
71. Chen E, Strunk RC, Bacharier LB, Chan M, Miller GE. Socioeconomic status associated with exhaled nitric oxide responses to acute stress in children with asthma. Brain Behav Immun. 2010;24(3):444–50. 10.1016/j.bbi.2009.11.017
72. Islam T, Urman R, Gauderman WJ, Milam J, Lurmann F, Shankardass K, et al. Parental stress increases the detrimental effect of traffic exposure on children’s lung function. Am J Respir Crit Care Med. 2011;184(7):822–27. 10.1164/rccm.201104-0720OC
73. Ritz T, Trueba AF, Simon E, Auchus RJ. Increases in exhaled nitric oxide after acute stress: association with measures of negative affect and depressive mood. Psychosom Med. 2014;76(9):716–25. 10.1097/PSY.0000000000000118
74. Landeo-Gutierrez J, Marsland AL, Acosta-Pérez E, Canino G, Celedón JC. Exposure to violence, chronic stress, asthma, and bronchodilator response in Puerto Rican children. Ann Allergy Asthma Immunol. 2020;124(6):626–27.e1. 10.1016/j.anai.2020.03.005