
Download




ORIGINAL ARTICLE
D-dimer concentrations in acute urticaria in children
Janusz Zaryczańskia, Agnieszka Ochaba*, Magdalena Ochabb, Anna Zaryczańskac, Zenon Brzozad, Agata Chobota
aDepartment of Pediatrics, Institute of Medical Sciences, University of Opole, Opole, Poland
bFaculty of Automatic Control, Electronics and Computer Science, Silesian University of Technology, Gliwice, Poland
cDermatology Students’ Scientific Circle in the Department of Dermatology, Venereology and Allergology, Medical University of Gdansk, Gdańsk, Poland
dDepartment of Internal Diseases, Institute of Medical Sciences, University of Opole, Opole, Poland
Abstract
Introduction: Urticaria is a clinical entity presenting as wheals, angioedema, or both simultaneously. Elevated D-dimer levels were reported in the course of chronic spontaneous urticaria. Data regarding D-dimer levels in acute urticaria in children are limited.
Objectives: To assess potential associations between duration of glucocorticosteroid (GCS) therapy and D-dimer concentrations in children with acute urticaria.
Patients, materials, and methods: Hospital records of 106 children (59 females), aged 5.57 ± 4.91 years, hospitalized in 2014–2018 were analyzed retrospectively. The study group consisted of pediatric patients admitted to the hospital due to severe acute urticaria resistant to antihistaminic treatment that was ordered in the ambulatory care (out-patient clinic). Patients were divided into subgroups: no GCS treatment, short-duration treatment (up to 5 days) and long-duration treatment (6 and more days) GCS treatment. Simultaneously, patients received antihistaminic drugs. D-dimer level and other inflammatory factors such as white blood cell (WBC) count, platelet (PLT) count, and C-reactive protein (CRP) in each group were analyzed.
Results: The D-dimer level was elevated in 51% of cases. In the subgroup with longer GCS treatment, D-dimer concentration was significantly higher in comparison to patients with a shorter GCS course. There were no differences in the distribution of CRP, PLT, and WBC concentrations between these subgroups.
Conclusions: In the studied group of children, there was a tendency for higher D-dimer levels in patients, who required a longer GCS treatment. This finding is hypothesis-generating and requires further investigation to confirm if D-dimers can be used as a prognostic factor in acute urticaria in children.
Key words: acute urticaria, children, pediatrics, D-dimers, glucocorticosteroids
*Corresponding author: Agnieszka Ochab, M.D. Department of Pediatrics University Hospital in Opole, Al. Witosa 26, 45-401 Opole, Poland. Email address: [email protected]
Received 29 March 2020; Accepted 5 June 2020; Available online 2 January 2021
Copyright: Janusz Zaryczański, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Urticaria is a clinical entity presenting as either wheals (elevated, itchy, and erythematous bumps or plaques on the skin), angioedema, or both simultaneously. Development of urticarial wheals is also known as hives.1,2 This entity is very much diversified in terms of clinical symptoms, pathogenesis, and time of occurrence. The underlying cause of the disease is associated with activation of the mast cells which release histamine, platelet-activating factor (PAF), and other mediators. This results in activation of the sensory nerves, vasodilatation, plasma extravasation, and cell recruitment to urticarial lesions.2
Acute urticaria is characterized by complete resolution of the symptoms within 6 weeks. Manifestation lasting longer than 6 weeks is classified as chronic urticaria. Urticaria is a common skin condition, with a lifetime prevalence of 2–6%. The highest incidence has been observed in children, who in great majority suffer from acute urticaria. Chronic urticaria is more common in the adult population; it is nevertheless a much less frequent condition, with a prevalence of 0.1–3%.3
The exact cause of acute urticaria remains idiopathic in 80–90% of patients. The most commonly reported causes of this disease in the pediatric population include viral infections (Adenovirus, Enterovirus, Respiratory Syncytial Virus, Cytomegalovirus, Epstein–Barr Virus), bacterial infections, (Streptococcus pyogenes, Helicobacter pylori, Mycoplasma pneumoniae), or less commonly parasitic infections. A small percentage of cases of acute urticaria in children may be associated with drug ingestion. Drug-induced urticaria can be distinguished into two types: (i) an allergic reaction—which may be, for example, associated with beta-lactam antibiotics hypersensitivity—and (ii) non-immunologically mediated reactions, most commonly related to non-steroidal anti-inflammatory drugs (NSAIDs) or beta blockers that may trigger direct mast cell degranulation. Lastly, certain foods such as milk, eggs, or nuts may provoke the onset of urticaria, and it is usually associated with an allergic reaction.2,3 In exceptional clinical cases, allergy testing may be performed. The mainstay of managing acute urticaria is the detection and elimination of the trigger factor. In addition to that first-line therapy is composed of second-generation antihistamine drugs. In case of lack of clinical response, severe pruritus, or distinct impairment of patient’s quality of life, the dose of antihistamine drug can be increased up to four-fold. First generation antihistamine drugs should be avoided due to their high risk of side effects. In case of severe course of the disease and/or antihistamine drug resistance, the administering of systemic glucocorticosteroids (GCS) for several days (prednisolone 0.5–1 mg/kg of body weight per day) should be considered.4
D-dimers are fibrin degradation products, composed of two D fragments connected by a double covalent bond. Increased serum concentration of D-dimer is observed when simultaneous clotting and fibrinolysis take place. Nevertheless, elevated D-dimer level is not pathognomonic of thromboembolic processes.5 Measurement of D-dimer level is useful in diagnosing deep vein thrombosis, pulmonary embolism, and disseminated intravascular coagulation.6 In addition, elevated D-dimer level is also reported in autoimmune diseases concerning granulocytes and eosinophils including: juvenile idiopathic synovitis, bullous pemphigoid, psoriasis, and vasculitis diseases such as polyarteritis nodosa or Henoch–Schönlein purpura.7,8 Increased level of D-dimer level in the course of chronic spontaneous urticaria was also disclosed.9–12
To the best of our knowledge there were no reports concerning D-dimer assay in diagnostic and therapeutic management of acute urticaria in pediatric population.
Aims
Based on the above information, we hypothesized that assessing D-dimer levels in children with acute urticaria may be potentially useful in the management algorithm of these patients. Therefore, this study aimed to analyze associations between the duration of GCS therapy in hospitalized, pediatric patients with acute urticaria, and the D-dimer concentrations.
Material and Methods
Patients
Our retrospective study included all patients who were hospitalized in the Department of Pediatrics of the University Clinical Hospital in Opole, Poland from the beginning of 2014 until the end of 2018 due to acute urticaria, who did not respond to first-line therapy administered as outpatient care. By response to first-line treatment, we understand significant resolution of skin lesions and reduction of pruritus after administration of second-generation antihistamine drugs. Only children with the most severe course of urticaria were admitted to the hospital (the severity of skin lesions was assessed in the outpatient clinic with Visual Analogue Scale). The study group consisted of 106 children aged between 3 months and 17 years—the characteristics of the groups are shown in Table 1.
Table 1 Characteristics of the study group and the subgroups depending on the duration of glucocorticosteroid (GCS) treatment. Values presented as means ± standard deviations.
| Whole study Group (subgroups I–III) | Subgroup I. No GCS treatment | Subgroup II. GCS for 1–5 days | Subgroup III. GCS for ≥ 6 days | |
|---|---|---|---|---|
| Number of patients | 106 | 16 | 64 | 26 |
| Sex: male/female | 47/59 | 5/11 | 34/30 | 8/18 |
| Age (years) | 5.57 ± 4.91 | 4.91 ± 4.81 | 4.71 ± 4.38 | 8.12 ± 5.47 |
| D-dimers (ng/ml) | 1811 ± 3512 | 901 ± 687 | 1243 ± 1347 | 2896 ± 5454 |
| CRP (mg/l) | 8.45 ± 18.4 | 14.4 ± 32.1 | 7.37 ± 15.9 | 5.47 ± 7.62 |
| PLT (103/μl) | 339 ± 104 | 322 ± 102 | 337 ± 93.5 | 351 ± 129 |
| WBC (103/μl) | 12.1 ± 4.53 | 11.8 ± 5.58 | 11.9 ± 4.8 | 12.9 ± 3.01 |
| Days on steroid treatments | 3.84 ± 3.22 | 0 ± 0 | 2.88 ± 1.23 | 8.58 ± 2.18 |
In accordance with the guidelines established by the European Academy of Allergy and Clinical Immunology (EAACI), Global Allergy and Asthma European Network (GA2LEN), and The World Allergy Organization (WAO),2 during hospitalization the treatment with antihistamine drugs was maintained and GCS therapy was instituted: patients intravenously received prednisolone 0.5–1 mg/kg/day or other dose-equivalent corticoids. In the study, 90 patients were treated with GCSs: 74.4% of them received hydrocortisone intravenously at a dose of 5–10 mg per 12-hour period, 27.8% received methylprednisolone intravenously at a dose of 1 mg/kg/day, and 6.7% received dexamethasone intravenously at a dose of 0.3 mg/kg/day. Steroid therapy was discontinued along the remission of the skin lesions. Almost a quarter of them (24.4%) continued the therapy with prednisone (0.5–1 mg/h/day) at home.
Methods
The data retrieved from the medical records and included in the analysis were as follows: sex, age, white blood cell count (WBC) (103/μl), platelet count (PLT) (103/μl), C-reactive protein (CRP) (mg/l), and D-dimer concentrations (evaluated using immunoturbidimetric technique; ng/ml). All laboratory tests were included in the standard care, and were performed in the central laboratory of the University Clinical Hospital in Opole. D-dimer concentration was measured on the day of admission as a routine procedure at the Department. The threshold for the positivity of D-dimer concentration was 1000 ug/ml. In case of increased D-dimer level, as a routine we performed a re-evaluation on the seventh day of hospitalization. The local ethical committee indicated that as it was a retrospective analysis of medical records, this study did not require a separate acceptance of the committee as well as no consent forms had to be signed by parents/caregivers and the patients.
Statistical analysis
Statistical analysis was performed using the computing environment R; additional software packages were taken from the Bioconductor project. Descriptive statistics for continuous variables were presented as mean values and standard deviations. The normality of data distribution was checked by the Shapiro–Wilk test. Due to not normal distribution, for comparison the Mann–Whitney U-test was employed. Kruskal–Wallis test, which is a non-parametric alternative of the one-way ANOVA, was applied to determine if there was a difference in distribution between the three independent groups (according to the GCS therapy duration). Wilcoxon signed-rank test was used to compare two subgroups treated with GCS for varied periods of time. Correlation analysis was performed by Spearman correlation test after removing outliers based on IGR Score. Significance for results of all statistical analyses was assumed at p < 0.05.
Results
The research included all children who were admitted to the Department of Pediatrics of the University Clinical Hospital in Opole, Poland in the years 2014–2018 due to acute urticaria, who did not respond to first-line therapy (second-generation antihistamine drugs) administered as an outpatient care. The study group consisted of 106 children (59 females) aged between 3 months and 17 years (mean 5.57 ± 4.91 years).
The age difference between male children and female children was not statistically significant. There was an evident predominance of the youngest children among those children admitted to our hospital with the diagnosis of acute urticaria (Figure 1). The mean concentration of D-dimers in the whole study group was 1810 ± 3512 ng/ml (ranging from 192 to 25 750 ng/ml) (Figure 2; top). The D-dimer level was elevated in 51% of the cases. After dividing patients into three subgroups based on the GCS treatment (without GCS, GCS up to 5 days, and GCS for 6 days or more), we found no statistically significant differences in the distribution of concentrations of CRP (p = 0.99), PLT (p = 0.91), and WBC (p = 0.35). There was also no statistically significant difference in the D-dimers concentrations (p = 0.09), even after the analysis by gender (boys, p = 0.775 and girls, p = 0.09) respectively (Figure 4; boys – left panel and girls – right panel). Nevertheless, the comparison of two subgroups treated with GCS for varied periods of time, revealed that those children that required longer GCS therapy had significantly higher D-dimer levels (1354 ng/ml vs. 602 ng/ml, p = 0.048) (Figure 3). This difference was significant in the female group of patients (p = 0.046), and was not detected in boys (Figure 4; boys – left panel and girls – right panel).
Figure 1 Histogram of patients’ age distribution in the analyzed population.
Figure 2 Visualization of differentiation of analyzed factors: D-dimer, CRP, WBC and PLT.
Figure 3 D-dimer level with no glucocorticosteroid treatment, short-duration treatment, and long-duration treatment.
Figure 4 D-dimer level with no glucocorticosteroid treatment, short-duration treatment, and long-duration treatment in subpopulation of boys (left panel) and girls (right panel).
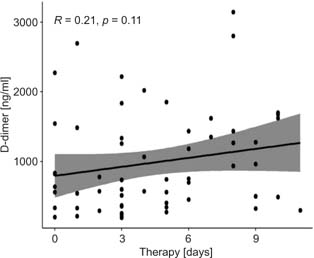
Analysis of correlations showed no significant relations between concentrations of D-dimers, CRP or PLT, and the GCS treatment (r = 0.21, p = 0.11; r = 0.03, p = 0.75; and r = 0.03, p = 0.77) (Figure 5) respectively.
Figure 5 Correlation between D-dimer level and the duration of glucocorticosteroid treatment.
Discussion
The association between urticaria and increased procoagulant activity has recently been largely investigated.13
The immune system, inflammation, and blood coagulation comprise interrelated, complementary components of a protective immunological response. Interactions between dysfunctions of the immune system and coagulation processes have been repeatedly reported in autoimmune and immune-mediated skin diseases, and the molecular background of these interactions has been profoundly investigated. Pro-inflammatory cytokines such as interleukin-1, interleukin-6, and tumor necrosis factor (TNF) might trigger the release of procoagulant mediators and decrease the activity of natural anticoagulants. On the other hand, higher activity of coagulation, confirmed by detection of the prothrombotic proteases, might result in overexpression of pro-inflammatory cytokines.14,15
In the literature, the simultaneous involvement of immune response, inflammation, and blood coagulation have been primarily associated with chronic, autoimmune processes.7 Our findings may suggest that these interactions also play a role in acute diseases, and a thorough analysis of the background of this phenomenon raises the opportunity for improving diagnostic and therapeutic management of acute urticaria.
At present, there is no laboratory test that could be useful in assessing the severity of acute urticaria, or the prognosis of this disease course. To the best of our knowledge, this study is one of the first publications considering the analysis of the D-dimer level in young patients with this diagnosis. We demonstrated a tendency for higher D-dimer concentrations in children with acute urticaria, who required a longer time of GKS treatment. The results of our investigation indicate that assessment of the D-dimer concentration in acute urticaria may potentially be helpful in facilitating the decision regarding the introduction of systemic steroid therapy. Nevertheless, this observation requires further investigation.
Takahashi et al. observed significant elevation of the D-dimer level which rapidly subsided in accordance with the treatment and with the resolution of skin changes. Nevertheless, the association between the dysregulation of the immune system and the increased concentration markers of coagulation pathway activation has been poorly investigated in the pediatric population.
In the literature, the interplay between inflammatory process and coagulation has been often elucidated by the example of chronic urticaria. Kasperska-Zajac et al. emphasized their significant role in the pathogenesis of chronic spontaneous urticaria and considered the influence of particular cytokines as crucial in determining the activity and the severity of the disease.16,17
According to recent reports, chronic urticaria is associated with both increased D-dimer concentration, as well as an elevated VII factor level and elevated F1+2 level. The concentration of D-dimer level in chronic urticaria has even been considered a marker for disease activity and response to treatment.12,18,19
These observations lead to the conclusion that the tissue factor pathway may be involved in the pathogenesis of this entity. Despite the fact that these parameters decrease during omalizumab treatment and within the remission of clinical symptoms, a limited number of studies resulted in exclusion of blood clotting tests in the diagnostic management of chronic urticaria.20 Furthermore, coagulation disturbances were confirmed in isolated cases of Henoch–Schönlein purpura.8 Elevated markers of hypercoagulability have also been detected in other types of vasculitis such as Kawasaki disease and eosinophilic granulomatosis with polyangitis.21,22 The correlation between elevated D-dimer level and the severity of the diseases was a subject of numerous studies. Nevertheless, data are too limited to draw definite conclusions or to demonstrate the exact pathomechanism of this phenomenon.
Recently, there has been a growing interest on procoagulant activity in patients with acute urticaria. It is considered that elevated level of D-dimers in acute urticaria can be explained by a simultaneous stimulation of the coagulation processes and the fibrinolysis processes, resulting from the activity of the enzymes released by granulocytes, which are involved in leukocytoclastic vasculitis.23,24 A comparable increase of the D-dimer level was observed in leukocytoclastic vasculitis in the course of Henoch–Schönlein purpura, chronic spontaneous urticaria, or connective tissue diseases such as juvenile idiopathic arthritis in children in the Polish population.25–27 It should be emphasized that in all of these entities, granulocytes play an essential role in the inflammatory process.
The strength of this study lies in the large number of patients and the originality of this investigation. The main limitation of this study is the discrepancy in the number of patients in each subgroup—a small number of patients did not receive GKS treatment, because only non- respondents to ambulatory treatment were hospitalized. Moreover, duration of symptoms before biological assay varied in particular patients. These may be the reasons that the revealed differences did not reach statistical significance.
Conclusions
In conclusion, this study showed higher D-dimer concentrations in children, especially girls, who required longer GCS treatment due to acute urticaria. This finding is hypothesis-generating. The question as to whether there is a future possibility to estimate the prognosis of acute urticaria course and to assess the need of adding GCS to antihistamine therapy based on the D-dimer concentration in children remains open and requires further research.
Conflict of interest
The authors declare that there is no conflict of interest to disclose.
Funding
This study was partially financed by the University of Opole grant IMS17. The authors convey their thanks to them.
REFERENCES
1. Nowicki RJ, Śpiewak R. Diagnostyka pokrzywek. In: Kruszewski J, Nowicki RJ, Śpiewak R, editors. Pokrzywki. Rozpoznawanie i leczenie. Warsaw: Medycyna Praktyczna; 2011, p. 45–56.
2. Zuberbier T, Aberer W, Asero R, Abdul Latiff AH, Baker D, Ballmer-Weber B, et al. The EAACI/GA2LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy. 2018;73(7):1393–414. 10.1111/all.13397
3. Tsakok T, Du Toit G, Flohr C. Pediatric urticaria. Immunol Allergy Clin North Am. 2014;34:117–39. 10.1016/j.iac.2013.09.008
4. Zuberbier T, Aberer W, Asero R, Bindslev-Jensen C, Brzoza Z, Canonica GW, et al. The EAACI/GA 2 LEN/EDF/WAO guideline for the definition, classification, diagnosis, and management of urticaria: the 2013 revision and update. Allergy. 2014;69:868–87. 10.1111/all.12313
5. Walczak B, Demkow U, Fijałkowska A. Metody oznaczania ste¸żenia D-dimerów przydatne w diagnostyce żylnej choroby zakrzepowo-zatorowej. Pneumonol Alergol Pol. 2009;77(3):264–70.
6. Rośniak–Bąk K, Łobos M. Przydatność kliniczna i diagnostyczna oznaczeń D–dimeru w różnych stanach chorobowych. Folia Medica Lodz. 2016;43:69–91.
7. Cugno M, Borghi A, Garcovich S, Marzano AV. Coagulation and skin autoimmunity. Front Immunol. 2019;10:1407. 10.3389/fimmu.2019.01407
8. Yilmaz D, Kavakli K, Ozkayin N. The elevated markers of hypercoagulability in children with Henoch–Schönlein purpura. Pediatr Hematol Oncol. 2005;22:41–8. 10.1080/08880010590896251
9. Criado PR, Antinori LCL, Maruta CW, Reis VMS. Evaluation of D-dimer serum levels among patients with chronic urticaria, psoriasis and urticarial vasculitis. An Bras Dermatol. 2013;88(3):355–60. 10.1590/abd1806-4841.20131532
10. Hansen C. Leukocytoclastic vasculitis mistaken for chronic idiopathic urticaria. J Case Rep. 2018;6:32–5.
11. Borzova E, Grattan CEH. Urticarial vasculitis. In: Griffiths CEM, Barker J, Bleiker T, Chalmers R, Creamer D, editors. Rook’s textbook of dermatology. 9th ed., Jon Wiley & Sons, Ltd, Chichester 2016, p. 1–6.
12. Kasperska-Zajac A, Brzoza Z, Rogala B. D-dimer plasma concentration in chronic urticaria patients with positive autologous serum intradermal test. Adv Clin Exp Med. 2007;16(1):65–8.
13. Zhu H, Liang B, Li R, Li J, Lin L, Ma S, et al. Activation of coagulation, anti-coagulation, fibrinolysis and the complement system in patients with urticaria. Asian Pacific J Allergy Immunol. 2013;31(1):43.
14. Esmon CT. Crosstalk between inflammation and thrombosis. Maturitas. 2004;61(1–2):122–31. 10.1016/j.maturitas.2008.11.008
15. Levi M, Van Der Poll T. Two-way interactions between inflammation and coagulation. Trends Cardiovas Med. 2005;15(7):254–9. 10.1016/j.tcm.2005.07.004
16. Grzanka R, Damasiewicz-Bodzek A, Kasperska-Zajac A. Interplay between acute phase response and coagulation/fibrinolysis in chronic spontaneous urticaria. Allergy Asthma Clin Immunol. 2018;14(1):27. 10.1186/s13223-018-0255-8
17. Kasperska-Zajac A, Sztylc J, Machura E, Jop G. Plasma IL-6 concentration correlates with clinical disease activity and serum C-reactive protein concentration in chronic urticaria patients. Clin Exp Allergy. 2011;41(10):1386–91. 10.1111/j.1365-2222.2011.03789.x
18. Ghazanfar MN, Thomsen SF. D-dimer as a potential blood biomarker for disease activity and treatment response in chronic urticaria: a focused review. Eur J Dermatol. 2018;28(6):731–5.
19. Farres MN, Refaat M, Melek NA, Ahmed EE, Shamseldine MG, Arafa NA. Activation of coagulation in chronic urticaria in relation to disease severity and activity. Allergol Immunopathol (Madr). 2015;43(2):162–7. 10.1016/j.aller.2014.04.002
20. Asero R, Marzano AV, Ferrucci S, Cugno M. D-dimer plasma levels parallel the clinical response to omalizumab in patients with severe chronic spontaneous urticaria. Int Arch Allergy Immunol. 2017;172(1):40–4. 10.1159/000453453
21. Akazawa H, Ikeda U, Yamamoto K, Kuroda T, Shimada K. Hypercoagulable state in patients with Takayasu’s arteritis. Thromb Haemost. 1996;76(5):712–16. 10.1055/s-0038-1650353
22. Marzano A, Tedeschi A, Rossio R, Fanoni D, Cugno M. Prothrombotic state in churg-strauss syndrome: a case report. J Investig Allergol Clin Immunol 2010;20(7):616–19.
23. Takahashi T, Minami S, Teramura K, Tanaka T, Fujimoto N. Four cases of acute infectious urticaria showing significant elevation of plasma D-dimer level. J Dermatol. 2018;45(8):1013–16. 10.1111/1346-8138.14481
24. Baek YS, Jeon J, Kim JH, Oh CH. Severity of acute and chronic urticaria correlates with D-dimer level, but not C-reactive protein or total IgE. Clin Exp Dermatol. 2014;39(7):795–800. 10.1111/ced.12413
25. Zaryczański J. D–dimery w plamicy Schőnleina–Henocha dzieci. Pediatr Pol. 2002;9:761.
26. Zaryczański J. D-dimery u dzieci chorych na młodzieńcze przewlekłe zapalenie stawów. Reumatologia. 1999;37:376–82.
27. Zaryczański J. D–dimery w chorobach tkanki łącznej u dzieci. Pediatr Prakt. 2002;10(1):65.