
Download
ORIGINAL ARTICLE
Effectiveness of topical intranasal curcumin in the experimentally induced allergic rhinitis model in rats (revised)
Erbay Demira*, Muhsin Kotenb, Fatma Elif Usturalı Keskinc, Canan Eryıldızd, Selis Gülseven Güvene
aDepartment of Otorhinolaryngology, Independent Investigator, Istanbul, Türkiye
bDepartment of Otorhinolaryngology, Kirklareli Training and Research Hospital, Kırklareli, Türkiye
cDepartment of Pathology, Trakya University Hospital, Edirne, Türkiye
dDepartment of Medical Microbiology, Trakya University Hospital, Edirne, Türkiye
eDepartment of Otorhinolaryngology, Trakya University Hospital, Edirne, Türkiye
Abstract
Curcumin, a flavonoid derived from turmeric, has demonstrated antioxidant, anti-inflammatory, and antiallergic effects. This study evaluated the therapeutic efficacy of intranasal curcumin in an allergic rhinitis (AR) rat model. Forty rats were randomized into four groups: a sham control, an AR model with no treatment (negative control), an AR model treated with intranasal mometasone furoate (positive control), and an AR model treated with intranasal curcumin. Allergic symptoms (sneezing, itching, nasal discharge) were evaluated by both unblinded and blinded observers. Serum Ovalbumin (OVA)-specific IgE levels were measured using ELISA. Nasal mucosal histopathology (edema, cilia loss, goblet cell hyperplasia, inflammation, eosinophilia) was assessed by light microscopy. Intranasal curcumin significantly improved histopathological findings and reduced allergic symptoms, with efficacy comparable to steroid treatment. It alleviates AR symptoms and inflammation, suggesting a promising, low-cost alternative for AR management.
Key words: allergic rhinitis, anti-inflammatory effects, histopathological improvement, IgE Modulation, intranasal curcumin
*Corresponding author: Erbay Demir, Department of Otorhinolaryngology, Independent Investigator, Istanbul, Türkiye. Email address: [email protected]
Received 1 February 2026; Accepted 3 February 2026; Available online 1 March 2026
Note: This article is an updated version of the original submission: Demir E, Koten M, Usturalı Keskin FE, Eryıldız C, Gülseven Güven S. Effectiveness of topical intranasal curcumin in the experimentally induced allergic rhinitis model in rats. Allergol. Immunopathol. (Madr). 2026;54(1):1–7. 10.15586/aei.v54i1.1468
Copyright: Demir E et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Bullet Point Summary
-
Intranasal curcumin was associated with reduction in allergic rhinitis (AR) symptoms, including sneezing, itching, and nasal discharge in an experimental rat model.
-
Histopathological examination demonstrated improvements in mucosal inflammation, cilia preservation, and goblet cell hyperplasia in curcumin-treated animals compared with untreated allergic controls.
-
Curcumin treatment led to a decrease in OVA-specific IgE levels, although not statistically significant, suggesting potential systemic immunomodulatory effects.
-
The study suggests that curcumin may represent a potentially safe, cost-effective, and accessible alternative to standard therapies like mometasone furoate for AR.
-
Daily intranasal administration of curcumin showed consistent improvements in symptom scores over multiple time points.
-
The findings suggest that intranasal curcumin may warrant further investigation in preclinical and clinical settings to better define its potential role in AR management.
Introduction
Allergic rhinitis (AR) is an immunoglobulin E (IgE)-mediated chronic inflammatory disease of the nasal mucosa. This condition presents with nasal symptoms including congestion, rhinorrhea, pruritus, and sneezing, triggered by allergen exposure.1,2 Prevalence of allergic rhinitis is estimated to be between 10 and 20% of the population.3 Its high prevalence translates to a significant economic burden, impacting healthcare systems and productivity.4
Experimental animal models of AR utilize various allergens, such as ovalbumin (OVA), Japanese cedar pollen, Staphylococcal enterotoxin B, Schistosoma mansoni egg antigen, toluene 2,4-diisocyanate, and house dust mites. Following the successful establishment of an AR model, experimental animals exhibit the hallmark symptoms: rhinorrhea, pruritus, and sneezing.
Flavonoids constitute a class of plant-derived compounds exhibiting antioxidant, anti-inflammatory, and antiallergic activities.5,6 Extensive use of Curcuma longa (turmeric) is evident in the ancient Indian medical system known as “Ayurveda.” The initial isolation of curcumin, the major bioactive flavonoid responsible for the plant’s yellow coloration, occurred two centuries ago. In 1910, the structure of curcumin (diferuloylmethane) component was determined. Research findings consistently demonstrate its anti-inflammatory and antioxidant effects, signifying its therapeutic promise in the treatment of numerous allergic, inflammatory, and chronic conditions.7–12 Curcumin demonstrates a dose-dependent, irreversible inhibitory effect on antigen-induced mast cell degranulation, consequently mitigating IgE-mediated allergic reactions.13
This study investigates the efficacy of intranasal curcumin in an experimental AR rat model to assess its impact on rhinitis symptoms, nasal mucosal histopathology, and serum allergen-specific IgE levels.
Materials and Methods
This study was conducted at the Experimental Animals Unit, and approval from the Local Ethics Committee of Animal Experiments was obtained in accordance with the Helsinki Declaration for animal experiments (Approval number: 2018.03.04/date: 30.03.2018). A total of 40 female Sprague–Dawley rats (200–250 g) aged 10–12 weeks were utilized for this study. The rats were kept in a 12-h light/dark cycle at 19-21°C with 50% humidity. Animals were allowed food and water ad libitum.
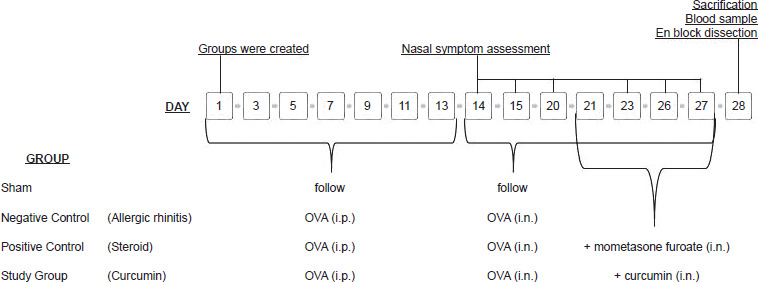
The Sham group received no intervention. The Negative Control (allergic rhinitis) group was designed as an AR model and received no treatment. The Positive Control (steroid) and Study (curcumin) groups, also designed as AR models, received intranasal steroid and intranasal curcumin, respectively (Figure 1).
Figure 1 Working plan. OVA: Ovalbumin, i.p.: Intraperitoneally, i.n.: Intranasally
The symptoms in the rats were observed on Day 1. The Sham group consisted of healthy animals receiving no intervention. Subsequently, anesthesia was achieved with xylazine 10 mg/kg (Xylazinbio 2% 50 mL, Bioveta) and ketamine 40 mg/kg (Ketasol 10% 10 mL, Richter Pharma AG). Then, the animals were weighed and assigned tail numbers. Groups were selected randomly.
Sensitization and provocation
An antigen solution was prepared using 1 mL physiological saline 0.9% (SF, saline), 1 mg OVA (Grade VI, Sigma-Aldrich Chemical Co., St. Louis, MO), and 10 mg aluminum hydroxide as adjuvant. The solution was given to the rats in the Negative Control, the Positive Control, and the Study groups via intraperitoneal administration every 2 days, with a total of 7 injections over 13 days (Days 1, 3, 5, 7, 9, 11 and 13).14
During the 14 days following sensitization, 0.04 g OVA was dissolved in 2 mL SF to obtain a 2% (w/v) OVA-SF solution every day. This solution was administered to the 30 sensitized animals in the Negative Control, the Positive Control, and the Study groups by means of a micropipette as 25 µL in each nostril (50 µL for each rat), thereby creating an AR model using intranasal provocation with OVA in sensitized rats.15
Treatment
Intranasal administration of OVA continued throughout the study, furthermore, both the positive control and study groups received daily intranasal treatment from Days 21 through 28. Intranasal treatments were administered 1 h before the OVA was given. Daily administrations followed a consistent schedule. A daily dose of 0.1 mL mometasone furoate (Nazoster®, Santa Farma Drug Industry, Istanbul, Türkiye, 50 µg per spray, equivalent to 50 µg per nostril) was administered to each nostril of rats in the positive control group using a micropipette [14]. The rats in the study group were given curcumin solution (200 mg/mL) prepared using distilled water. Using a micropipette, 20 µL of this solution was administered in each nostril twice a day.16,17 Fresh solutions were prepared each day for the study.
Assessment of symptoms
Clinical observations were independently performed by two blinded observers. A clinical assessment was conducted focusing on the key symptoms of AR: sneezing, nasal itching, and nasal discharge. Data was collected through assessments performed on Days 1, 14, 15, 20, 23, 26, and 27. Post intranasal OVA administration, each rat was isolated in an individual cage for a 10-min acclimation period before undergoing a 10-min observation. Symptom scores were determined using a four-point scale, as illustrated in Table 1. Symptoms were individually assessed and assigned a score from 0 to 3, reflecting their intensity.17,18 A total score ≥5 was considered to reflect a successful AR model.19
Table 1 Symptom scoring system for assessment of nasal itching, sneezing, and nasal discharge in the experimental rat model of allergic rhinitis.
| 0 point | 1 point | 2 point | 3 point | |
|---|---|---|---|---|
| No. of nasal itching motion (scratches) (time/minute) | None | 2 | 4–6 | >6 |
| No. of sneezes (time/10 min) | None | 1–3 | 4–9 | ≥10 |
| Amount of nasal flow | None | In a nostril | Outside nostril | Overflowing both nostrils |
Measurement of IgE levels
Intracardiac blood samples of 2–4 cc were collected under anesthesia before animals were sacrificed. Whole blood samples were collected using EDTA as an anticoagulant and centrifuged at 3000 rpm for approximately 20 min. Supernatants were collected in Eppendorf tubes carefully and stored at −40–80°C. OVA-specific IgE measurements were performed using the ELISA method (Rat OVA-Specific IgE ELISA Kit/96 Tests, MyBioSource, Inc., USA).
Histopathological examination
Decapitation, performed under ketamine/xylazine anesthesia (40 mg/kg/10%, 10 mg/kg/2%), euthanized the rats 24 h after their last drug dose. Following decapitation, the eyes, skin, muscles, brain, pituitary gland, and lower jaw were dissected. The residual specimen (nasal cavity, paranasal sinuses, and conchae), resected en bloc, received thorough lavage with 10% formalin before placement in individual containers containing 400 cc of the same fixative. Tissue specimens were preserved in 10% formalin for 48 h. Decalcification of the bone tissue was subsequently achieved through a 36-hour immersion in 10% formic acid. Transverse sections were obtained from decalcified heads.20 Microtomy was employed to generate 4–5 μm sections after dehydration and paraffin embedding. The staining protocol utilized hematoxylin and eosin (H&E). These same histological procedures were also applied to the Sham and Negative Control groups, which did not receive drug doses.
Edema, vascular congestion, cilia loss, increase in goblet cells, inflammation and increase in eosinophils were scored through light microscopy examination.21–23 The semiquantitative assessment employed a four-point scale: 0 for no change, 1 for mild change (minimal focal change), 2 for considerable change (moderate diffuse involvement), and 3 for significant change (marked and extensive change). All evaluations were performed independently by two pathologists blinded to group allocation.
Statistical analysis
The sample size was determined to be 10 rats per group, based on a projected large effect size (0.58) for the primary outcome, alpha of 0.05, and a power of 0.80. Results were expressed as mean ± standard deviation, median (interquartile range) and number (%). Normal distribution suitability of the data was evaluated by the Shapiro–Wilk test. Data showing normal distribution across groups were compared using one-way ANOVA (with Tukey’s HSD post-hoc test if significant) and Kruskal–Wallis tests (with Bonferroni-corrected Mann–Whitney U post-hoc tests, if significant). Before-and-after group comparisons used paired t-tests when normality held, and Wilcoxon tests when it did not. Categorical data was compared using a chi-square test. Statistical analysis was performed using the SPSS 20.0 (License No: 10240642) package program. A P-value <0.05 was assumed for statistical significance.
Results
Histological findings
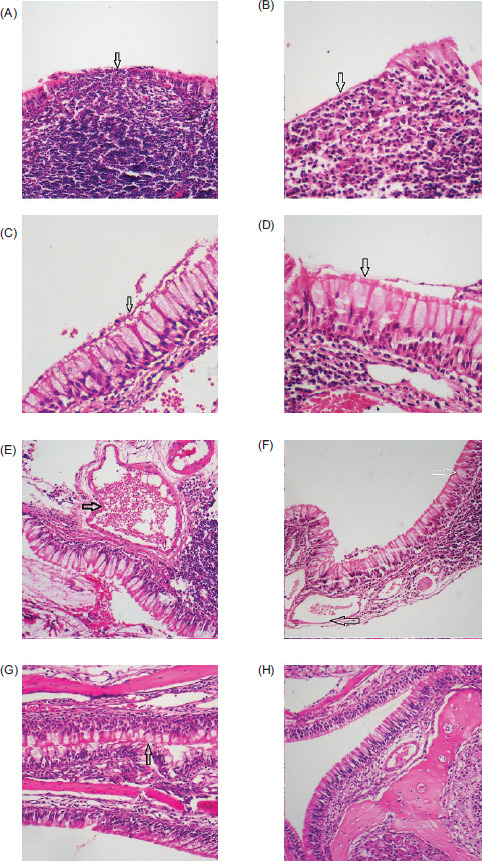
In the Negative Control group, increased goblet cells and cilia loss were observed in the respiratory epithelium, increased inflammatory cells with lymphocyte dominance and eosinophils were noted in lamina propria, and vascular congestion and edema were detected in connective tissue (Figure 2). A comparative analysis revealed statistically significant elevations (P < 0.05) in edema (P = 0.007), vascular congestion (P = 0.006), cilia loss (P = 0.003), goblet cell numbers (P = 0.007), and inflammatory response (P = 0.041) in the Negative Control group compared to the Sham group. No significant differences were observed between the Study and Sham groups, or between the Study and Positive Control groups.
Figure 2 Histopathological examination. (A) Inflammatory cells infiltrating epithelium in the Negative Control group (HEx100). (B) Inflammation and small number of eosinophils are observed in the Study group (HEx200). (C) Increased goblet cells and cilia loss in the Negative Control group (HEx400). (D) Significantly decreased cilia loss in the Study group (HEx400). (E) Increased vascular congestion in the Negative Control group (HEx200). (F) Significantly reduced congestion (black arrow) and mildly increased goblet cells (white arrow) in the Study group (HEx100). (G) Little increase in goblet cells and no inflammation observed in the Positive Control group (HEx200). (H) Normal mucosa in the Sham group (HEx100).
Statistical analysis revealed no significant differences (P > 0.05) in edema, vascular congestion, cilia loss, increase in goblet cells, inflammation, or eosinophil increase between the Study and Positive Control groups. Edema, vascular congestion, cilia loss, and eosinophil increase showed no statistically significant difference between the Study and Sham groups (P = 0.214, P = 0.078, P = 0.113, P = 0.054).
Assessment of symptom scores
Prior to treatment, all rats administered intranasal OVA demonstrated a rise in the classic symptoms of AR, namely sneezing, nasal pruritus, and nasal discharge. By Day 20, all rat groups except the Sham group exhibited symptom scores of 5 or greater, thereby confirming the successful establishment of an allergic rhinitis model.
Throughout the assessment period, the Sham group rats consistently presented with a symptom score of zero. The negative control group received only intranasal OVA commencing on Day 20, exhibiting a progressive increase in symptom scores across all assessments. Conversely, post-intranasal treatment, a progressive decline in symptom scores was observed in both the positive control and study groups across all observations.
Intranasal treatment resulted in statistically significant decreases in symptom scores for the positive control and study groups (P = 0.004 in each group). Post-study symptom score analysis revealed no significant difference between the positive control and study groups (P = 1.000).
Serum IgE results
A decrease in OVA-specific IgE levels was observed in the curcumin group relative to the AR group, nevertheless, this reduction was not statistically significant (P = 0.81). The analysis of the current study revealed no statistically significant difference in outcomes between the positive control and study groups (P = 0.996). A summary of the results is provided in Table 2.
Table 2 Comparative histopathological findings, symptom scores, and serum ovalbumin-specific IgE levels across Sham, Negative Control, Positive Control, and Study groups.
| Sh (n = 10) n (%) | NC (n = 10) n (%) | PC (n = 10) n (%) | S (n = 10) n (%) | ||
|---|---|---|---|---|---|
| Edema | None | 6 (60) | 0 (0) | 9 (90) | 8 (80) |
| Mild | 4 (40) | 7 (70) | 0 (0) | 1 (10) | |
| Moderate | 0 (0) | 3 (30) | 1 (10) | 1 (10) | |
| Severe | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Vascular congestion | None | 7 (70) | 0 (0) | 2 (20) | 2 (20) |
| Mild | 2 (20) | 5 (50) | 4 (40) | 6 (60) | |
| Moderate | 1 (10) | 1 (10) | 2 (20) | 2 (20) | |
| Severe | 0 (0) | 4 (40) | 2 (20) | 0 (0) | |
| Cilia loss | None | 8 (80) | 0 (0) | 6 (60) | 5 (50) |
| Mild | 1 (10) | 2 (20) | 4 (40) | 5 (50) | |
| Moderate | 1 (10) | 7 (70) | 0 (0) | 0 (0) | |
| Severe | 0 (0) | 1 (10) | 0 (0) | 0 (0) | |
| Goblet cell increase | None | 7 (70) | 0 (0) | 3 (30) | 1 (10) |
| Mild | 3 (30) | 6 (60) | 6 (60) | 6 (60) | |
| Moderate | 0 (0) | 3 (30) | 1 (10) | 2 (20) | |
| Severe | 0 (0) | 1 (10) | 0 (0) | 1 (10) | |
| Inflammation | None | 0 (0) | 0 (0) | 6 (60) | 4 (40) |
| Mild | 6 (60) | 1 (10) | 2 (20) | 2 (20) | |
| Moderate | 4 (40) | 7 (70) | 1 (10) | 1 (10) | |
| Severe | 0 (0) | 2 (20) | 1 (10) | 3 (30) | |
| Eosinophil increase | None | 1 (10) | 0 (0) | 7 (70) | 6 (60) |
| Mild | 8 (80) | 4 (40) | 2 (20) | 3 (30) | |
| Moderate | 1 (10) | 5 (50) | 1 (10) | 1 (10) | |
| Severe | 0 (0) | 1 (10) | 0 (0) | 0 (0) | |
| Symptom scores [median (interquartile range)] | Day 14 | 0 (0–0) | 1 (0–2) | 1 (1.0–1.25) | 1 (0.0–1.25) |
| Day 15 | 0 (0–0) | 3 (1–4) | 2 (2–4.5) | 3 (1–4) | |
| Day 20 | 0 (0–0) | 5.5 (5–6.25) | 6 (5–6.25) | 5 (5–6) | |
| Day 23 | 0 (0–0) | 6 (5–6.25) | 2.5 (1–3.25) | 3 (2–4.25) | |
| Day 26 | 0 (0–0) | 6 (6–7) | 2.5 (1.75–3) | 3 (2–4.25) | |
| Day 27 | 0 (0–0) | 7 (6-8) | 2 (1–2) | 2.5 (2–3.25) | |
| Ovalbumin-specific (ng/mL) (mean ± standard deviation) | - | 8.6290 ± 3.96236 | 4.5120 ± 2.21493 | 4.8640 ± 4.23142 | |
Sh: Sham group; NC: Negative Control group; PC: Positive Control group; S: Study group.
Discussion
Intranasal steroids demonstrate efficacy across the spectrum of AR symptoms, while exhibiting a reduced incidence of systemic adverse effects compared to alternative agents.24,25 Alternatively, the anti-allergic properties of curcumin and other flavonoids are still under investigation. We used an AR rat model to explore the antiallergic effects of curcumin in this study.
An AR guinea pig model was developed by Thakare et al.26 using OVA. Curcumin (100 and 200 mg/kg) and montelukast (10 mg/kg) were administered orally to the animal subjects. The results demonstrated a statistically significant decrease in sneezing and itching symptoms among subjects administered 200 mg/kg of curcumin. Furthermore, a reduction in nasal discharge and watery eyes was observed. Zhang et al.27 developed an OVA-induced AR model in mice. Researchers found that both 100 and 200 mg/kg doses of curcumin, given by gavage, significantly reduced sneezing and itching.
Acar et al.16 compared the effectiveness of intranasal curcumin versus a group treated with intranasal azelastine and a Sham group. Their study concluded that the rats in the group treated with intranasal curcumin showed significantly less sneezing, itching noses, runny noses, and watery eyes. However, a detailed analysis revealed no statistically significant difference in symptom relief between intranasal curcumin and intranasal azelastine. The study by Acar et al. also reported that curcumin significantly lessened itching, sneezing, and nasal discharge among the treated rats. In addition, there was no significant difference in symptom score reduction between mometasone furoate and curcumin.
In previous studies, histopathological examination of experimental animals revealed that intranasal curcumin lessened the inflammatory cell infiltration, vascular proliferation, and epithelial goblet cell metaplasia in the nasal mucosa.16,26,28 In the present study, mirroring previous research, intranasal steroids and curcumin significantly reduced edema, cilia loss, inflammation, and eosinophil increase. Although there was a decrease in vascular congestion with curcumin, the difference was not statistically significant. A slight, but measurable, elevation in goblet cell numbers was detected, potentially indicative of irritation or infection. The current study found no statistically significant differences in histopathological outcomes between the intranasal curcumin and steroid treatments. However, the absence of a curcumin-only healthy control group limits the ability to distinguish potential local irritant effects of the formulation from changes related to the AR model itself. Future studies could include a group receiving intranasal OVA without prior sensitization to better assess goblet cell changes.
Studies using ovalbumin-induced AR models in mice and guinea pigs showed that 200 mg/kg of oral curcumin significantly reduced OVA-specific IgE levels.26,27 Moreover, some published studies have demonstrated that different flavonoids decrease serum OVA-specific IgE levels, including with intranasal application.23
The present study found no statistically significant difference in OVA-specific IgE levels between the steroid and study groups. Compared to the Negative Control group, both groups showed lower OVA-specific IgE levels. Nonetheless, a statistically significant difference was observed solely between the positive and negative control groups. Once sensitization is induced, sIgE levels—although a reduction supports Th2 inhibition—have limited clinical relevance compared to clinical and histological findings.
The findings of the current study demonstrate a reduction in sneezing, nasal itching, and rhinorrhea among AR patients following intranasal curcumin administration, aligning with previous research. Consistent with the literature, we observed that intranasal curcumin treatment resulted in significantly improved histopathological features of the nasal mucosa, and the inflamed tissue showed signs of healing.
In a randomized double-blind study of 241 patients with AR, which compared 5 mg of curcumin daily to a placebo over 2 months, the curcumin group showed improved symptoms and nasal airflow.11 Strong evidence from multiple studies confirms the significant immunomodulatory and antiallergic effects of curcumin.29 The present study suggests that intranasal curcumin could offer a promising alternative treatment for AR in the future, showing potential in its effects.
Conclusion
This study suggests that intranasal curcumin could be a viable alternative to steroid nasal sprays for AR, effectively reducing symptoms and showing comparable improvements in tissue samples. The reduction in allergy symptoms (sneezing, itching, rhinorrhea) and nasal inflammation seen with curcumin highlights its potential therapeutic value. Observed histopathological and symptomatic improvements support prior research showing curcumin’s anti-inflammatory and immunomodulatory effects. Because of its accessibility, affordability, and safety, intranasal curcumin may be a promising addition to, or replacement for, standard treatments. Further investigation, including human clinical trials, is necessary to validate its long-term effectiveness, identify optimal dosing, and assess its place within standard AR management.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Author Contributions
All authors contributed equally to this article.
Conflicts of Interest
Authors have no conflicts of interest to disclose any relationships or activities.
Funding
This study was supported by the Trakya University Scientific Research Fund (decision number: TÜBAP-2018/329).
REFERENCES
1 Nagai H, Teramachi H, Tuchiya T. Recent advances in the development of anti-allergic drugs. Allergol Int. 2006;55(1):35–42. 10.2332/allergolint.55.35
2 Varshney J, Varshney H. Allergic rhinitis: An overview. Indian J Otolaryngol Head Neck Surg. 2015;67(2):143–9. 10.1007/s12070-015-0828-5
3 Brozek JL, Bousquet J, Baena-Cagnani CE, Bonini S, Canonica GW, Casale TB, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 revision. J Allergy Clin Immunol. 2010;126(3):466–76. 10.1016/j.jaci.2010.06.047
4 Blaiss MS, Hammerby E, Robinson S, Kennedy-Martin T, Buchs S. The burden of allergic rhinitis and allergic rhinoconjunctivitis on adolescents: A literature review. Ann Allergy Asthma Immunol. 2018;121(1):43–52.e3. 10.1016/j.anai.2018.03.028
5 Kahraman A, Serteser M, Koken T. Flavonoidler. Kocatepe Tıp Dergisi. 2002;3(1):98138. 10.18229/ktd.98138
6 Kumar S, Pandey AK. Chemistry and biological activities of flavonoids: An overview. ScientificWorldJournal. 2013;2013: 162750. 10.1155/2013/162750
7 Aggarwal BB, Harikumar KB. Potential therapeutic effects of curcumin, the anti-inflammatory agent, against neurodegenerative, cardiovascular, pulmonary, metabolic, autoimmune and neoplastic diseases. Int J Biochem Cell Biol. 2009;41(1):40–59. 10.1016/j.biocel.2008.06.010
8 Bhattacharyya S, Mandal D, Sen GS, Pal S, Banerjee S, Lahiry L, et al. Tumor-induced oxidative stress perturbs nuclear factor-kappaB activity-augmenting tumor necrosis factor-alpha-mediated T-cell death: Protection by curcumin. Cancer Res. 2007;67(1):362–70. 10.1158/0008-5472.CAN-06-2583
9 Shishodia S, Sethi G, Aggarwal BB. Curcumin: Getting back to the roots. Ann N Y Acad Sci. 2005;1056:206–17. 10.1196/annals.1352.010
10 Srivastava RM, Singh S, Dubey SK, Misra K, Khar A. Immunomodulatory and therapeutic activity of curcumin. Int Immunopharmacol. 2011;11(3):331–41. 10.1016/j.intimp.2010.08.014
11 Wu S, Xiao D. Effect of curcumin on nasal symptoms and airflow in patients with perennial allergic rhinitis. Ann Allergy Asthma Immunol. 2016;117(6):697–702.e1. 10.1016/j.anai.2016.09.427
12 Xiao Y, Xia J, Wu S, Lv Z, Huang S, Huang H, et al. Curcumin inhibits acute vascular inflammation through the activation of heme oxygenase-1. Oxid Med Cell Longev. 2018;2018:3295807. 10.1155/2018/3295807
13 Lee JH, Kim JW, Ko NY, Mun SH, Her E, Kim BK, et al. Curcumin, a constituent of curry, suppresses IgE-mediated allergic response and mast cell activation at the level of Syk. J Allergy Clin Immunol. 2008;121(5):1225–31. 10.1016/j.jaci.2007.12.1160
14 Sagit M, Polat H, Gurgen SG, Berk E, Guler S, Yasar M. Effectiveness of quercetin in an experimental rat model of allergic rhinitis. Eur Arch Otorhinolaryngol. 2017;274(8):3087–95. 10.1007/s00405-017-4602-z
15 Altıntoprak N, Kar M, Acar M, Berkoz M, Muluk NB, Cingi C. Antioxidant activities of curcumin in allergic rhinitis. Eur Arch Otorhinolaryngol. 2016;273(11):3765–73. 10.1007/s00405-016-4076-4
16 Acar M, Muluk NB, Yigitaslan S, Cengiz BP, Shojaolsadati P, Karimkhani H, et al. Can curcumin modulate allergic rhinitis in rats? J Laryngol Otol. 2016;130(12):1103–9. 10.1017/S0022215116008999
17 Wen WD, Yuan F, Wang JL, Hou YP. Botulinum toxin therapy in the ovalbumin-sensitized rat. Neuroimmunomodulation. 2007;14(2):78–83. 10.1159/000107422
18 Senturk E, Yildirim YS, Dogan R, Ozturan O, Guler EM, Aydin MS, et al. Assessment of the effectiveness of cyclosporine nasal spray in an animal model of allergic rhinitis. Eur Arch Otorhinolaryngol. 2018;275(1):117–24. 10.1007/s00405-017-4786-2
19 Assanasen P, Baroody FM, Rouadi P, Naureckas E, Solway J, Naclerio RM. Ipratropium bromide increases the ability of the nose to warm and humidify air. Am J Respir Crit Care Med. 2000;162(3 Pt 1):1031–7. 10.1164/ajrccm.162.3.9912055
20 Herbert RA, Janardhan KS, Pandiri AR, Cesta MF, Miller RA. Nose, larynx, and trachea. Boorman’s Pathology of the Rat. Elsevier. 2018. pp. 391–435. 10.1016/B978-0-12-391448-4.00022-8
21 Ercan I, Cakir BO, Başak T, Ozbal EA, Sahin A, Balci G, et al. Effects of topical application of methotrexate on nasal mucosa in rats: A preclinical assessment study. Otolaryngol Head Neck Surg. 2006;134(5):751–5. 10.1016/j.otohns.2005.11.046
22 Bousquet J, Jacot W, Vignola AM, Bachert C, Van Cauwenberge P. Allergic rhinitis: A disease remodeling the upper airways? J Allergy Clin Immunol. 2004;113(1):43–9. 10.1016/j.jaci.2003.09.047
23 Avincsal MO, Ozbal S, Ikiz AO, Pekcetin C, Güneri EA. Effects of topical intranasal doxycycline treatment in the rat allergic rhinitis model. Clin Exp Otorhinolaryngol. 2014;7(2):106–11. 10.3342/ceo.2014.7.2.106
24 Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008;63 Suppl 86:8–160. 10.1111/j.1398-9995.2007.01620.x
25 Gupta R, Fonacier LS. Adverse effects of nonsystemic steroids (inhaled, intranasal, and cutaneous): A review of the literature and suggested monitoring tool. Curr Allergy Asthma Rep. 2016;16(6):44. 10.1007/s11882-016-0620-y
26 Thakare VN, Osama MM, Naik SR. Therapeutic potential of curcumin in experimentally induced allergic rhinitis in guinea pigs. Int Immunopharmacol. 2013;17(1):18–25. 10.1016/j.intimp.2013.04.025
27 Zhang N, Li H, Jia J, He M. Anti-inflammatory effect of curcumin on mast cell-mediated allergic responses in ovalbumin-induced allergic rhinitis mouse. Cell Immunol. 2015;298(1–2): 88–95. 10.1016/j.cellimm.2015.09.010
28 Subhashini, Chauhan PS, Kumari S, Kumar JP, Chawla R, Dash D, et al. Intranasal curcumin and its evaluation in murine model of asthma. Int Immunopharmacol. 2013;17(3):733–43. 10.1016/j.intimp.2013.08.008
29 Owaga EE, Mponda J, Nyang’inja RA. Nutrigenomic approach in understanding the antiallergic effects of curcumin. Asian J Biomed Pharma Sci. 2014;4(31):1. 10.15272/ajbps.v4i30.487