
Download
ORIGINAL ARTICLE
Pragmatic management of acute cough in children and adolescents: an updated position paper by the Italian Society of Pediatric Allergy and Immunology (SIAIP)
Sara Mantia†, Amelia Licarib,c†, Michele Miraglia del Giudiced, Maria Angela Toscae, Giorgio Ciprandif*, Gianluigi Marsegliab,c
aUnit of Pediatrics, Department of Human Pathology in Adult and Developmental Age “Gaetano Barresi, “University of Messina, Messina, Italy
bPediatric Unit, Department of Clinical, Surgical, Diagnostic, and Pediatric Sciences, University of Pavia, Pavia, Italy
cPediatrics, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy
dDepartment of Woman and Child and General and Specialized Surgery, University of Campania Luigi Vanvitelli, Naples, Italy
eAllergy Center, IRCCS Istituto Giannina Gaslini, Genoa, Italy
fAllergy Clinic, Casa di Cura Villa Montallegro, Genoa, Italy
Abstract
Background: Cough is one of the most common and distressing symptoms in pediatric practice and represents a major cause of medical consultation, parental anxiety, and inappropriate medication use. Although most acute cough episodes are benign and self-limiting, they can significantly affect child’s sleep, school performance, and quality of life. The COVID-19 pandemic and subsequent changes in infection patterns and immune responses have further highlighted the need to update the existing clinical guidance.
Objective: This joint position paper by the Italian Society of Pediatric Allergy and Immunology (SIAIP) aims to provide a pragmatic, evidence-based update on the management of acute and post-viral cough in children and adolescents, integrating recent scientific advances and real-world clinical experiences.
Methods: A multidisciplinary board of experts from SIAIP critically reviewed the literature published from 2019 to 2025 and updated the previous 2019 SIAIP document. The group achieved consensus on diagnostic and therapeutic recommendations through structured discussion and iterative revision.
Results: The document emphasizes a stepwise approach to pediatric acute cough, starting with careful history-taking, clinical evaluation, and reassurance. Non-pharmacological measures—hydration, nasal saline irrigation, and avoidance of irritants—remain the first-line management. Pharmacological therapy may be considered in selected cases where cough is particularly distressing or significantly interferes with sleep; peripherally acting, nonsedative antitussives represent a reasonable option in terms of efficacy and safety. Centrally acting antitussives and unnecessary antibiotics should be avoided. Standardized, high-quality natural medical devices—with appropriate supporting evidence—represent a valid option. Honey-based preparations can be considered as complementary options. The paper also discusses new insights into cough pathophysiology, particularly the role of airway sensory hypersensitivity and neurogenic inflammation, which are paving the way for mechanism-based treatments.
Conclusions: This position paper provides an updated, pragmatic framework for the management of acute and post-viral cough in children and adolescents. It promotes rational drug use, integration of non-pharmacological and complementary measures, and awareness of emerging therapeutic targets. A mechanism-driven, individualized, and family-centered approach is advocated to improve clinical outcomes and quality of life for pediatric patients.
Key words: acute cough, children, levodropropizine, management, natural remedies, post-viral cough, position paper
*Corresponding Author: Giorgio Ciprandi, MD, Via P. Boselli 5, 16146 Genoa, Italy. Email address: [email protected]
Received 17 October 2025; Accepted 22 December 2025; Available online 1 May 2026
†Both are first co-authors.
Copyright: Manti S, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Cough is both a symptom and a clinical sign, triggered by a reflex mediated through a complex neuronal pathway. It serves a fundamental physiological role in clearing the airways of accumulated material, usually because of overload of secretion (the so-called post-nasal drip), less frequently to foreign body, or inhalation of irritants. Cough may also occur in association with the conditions such as asthma, gastroesophageal reflux disease (GERD), or because of vagal stimulation.
Cough can be classified according to its duration or clinical characteristics. Acute cough, defined as lasting for <1 month, is extremely common in childhood. Clinically, cough may be clinically described as wet, typically associated with mucus hypersecretion, or dry, mainly because of airway irritation. Moreover, its acoustic features may help to differentiate types, such as bitonal, whooping, barking, or hollow cough.
It is important to emphasize that cough generally represents a physiological protective mechanism, allowing the clearance of secretions, irritants, or foreign material from the airways. Therefore, as with fever, it should not be suppressed indiscriminately; in fact, an ineffective cough, especially when centrally inhibited, may be of little clinical benefit or even counterproductive.
From an epidemiological perspective, acute cough represents the most frequent complaint in primary care. The most common cause is upper respiratory tract infection (URTI), usually of viral origin—the so-called post-viral cough.1 To provide guidance in clinical practice, the Italian Society of Pediatric Allergy and Immunology (SIAIP) in 2019 published a systematic review on the pharmacological management of acute cough in children and adolescents,2 which also included a diagnostic algorithm. However, that document preceded the COVID-19 pandemic, and substantial new evidence has since become available.
For these reasons, the SIAIP recognized the need to update and expand the previous position paper, involving additional national and international scientific societies. A dedicated scientific board was established to revise the document and provide an updated, evidence-based reference for clinicians. The present position paper aims to summarize the most recent knowledge and offer a practical tool for the management of acute cough in children and adolescents.
Acute Cough: Clinical Aspects
Acute cough affects virtually all children and typically occurs several times per year.3,4 It represents the most frequent cause of new consultations in primary care and is also a common cause of unscheduled visits to emergency departments and out-of-hours services.5 However, cough is a nonspecific symptom, and a wide range of etiologies must be considered. In daily practice, the most common triggers of acute cough are respiratory infections, mainly involving the upper airways, inhalation of irritants, foreign bodies, and exposure to allergens in children with asthma (Table 1). Although, in the majority of cases, cough is self-limiting and related to viral infections, it markedly increases parental anxiety and disrupts family sleep.6 In school-age children, cough interferes with classroom activities and sports, thereby compromising school performance, physical exercise, and rest, and it may even result in school absenteeism.
Table 1 Causes of acute cough in children
| Causes | Suggestive findings |
|---|---|
| Environmental pulmonary toxicants | Exposure to tobacco smoke or environmental pollutions |
| URTIs | Rhinorrhea (anterior and posterior “post-nasal drip”); swollen nasal mucosa; fever; sore throat; nasal discharge; and nasal congestion |
| Croup | URTI-like prodrome; barky cough; stridor; nasal flaring; chest retractions; and tachypnea |
| Epiglottitis | Abrupt onset; fever; irritability; marked anxiety; stridor; respiratory distress; drooling; and toxic appearance |
| Bacterial tracheitis | Stridor; barky cough; fever; respiratory distress; and toxic appearance |
| Bronchiolitis | Rhinorrhea; first episode of respiratory distress associated with cough; crackles and/or wheezing; dyspnea; polypnea; increased respiratory effort manifested as nasal flaring, grunting, use of accessory muscles or intercostal and/or subcostal chest wall retractions; low oxygen (O2) saturation levels and apnea; changes in skin color; feeding difficulties; lethargy; and, rarely fever |
| Pneumonia | Fever; cough; tachypnea; dyspnea; Hypoxemia; increased work of breathing (e.g., chest retractions, nasal flaring, and head bobbing); and decreased or abnormal breath sounds on auscultation (e.g., crackles, rales, crepitation, wheeze, and rhonchi) |
| Foreign body | Sudden onset of coughing; wheezing; stridor (high-pitched); difficulty in breathing; drooling; gagging; vomiting; and dysphonia or cyanosis |
| COVID-19 | Nasal congestion and rhinorrhea; sore throat; fever; chest tightness; tachypnea; wheezing; crackles; and hypoxia |
Children with acute cough often require close parental supervision and care, leading to work absence and reduced productivity. This impact is further amplified when younger siblings are also affected or when multiple episodes occur during the same winter season. Consequently, families frequently resort to natural remedies in an attempt to relieve symptoms.7,8 These practices are not always supported by evidence and may contribute to inappropriate medication use, including unnecessary antibiotics. Overall, acute cough imposes a considerable burden not only on children but also on their families and society because of its direct and indirect costs.9,10
The COVID-19 pandemic, while having a devastating impact on global health systems, also provided an unprecedented “natural experiment” for respiratory infections.11–13 It clearly emphasized that every infectious episode is accompanied by an inflammatory response that underlies the main systemic and respiratory symptoms. Lockdowns, use of masks, hand hygiene campaigns, and social distancing markedly reduced the circulation of common respiratory viruses during the first pandemic phases. This was reflected in the almost complete disappearance of bronchiolitis and a dramatic fall in other acute respiratory infections in many countries.14,15 As these non-pharmacological interventions were progressively relaxed, a rapid and sometimes pronounced rebound of respiratory infections was observed, often with atypical seasonality and clustering of cases. This phenomenon has been attributed, at least in part, to a “gap” in immune training because of reduced exposure to pathogens, particularly in younger children who had never previously encountered common respiratory viruses.
Within this changing epidemiological landscape, the clinical expression of acute and post-infectious cough appears to be evolving. Children may present with cough associated with different viral patterns and co-infections, and some episodes seem more intense or prolonged than in the pre-COVID era. In addition, heightened parental concern about respiratory symptoms, often driven by fear of SARS-CoV-2 infection, has led to earlier medical consultations and, in some settings, to increased pressure for diagnostic tests and pharmacological treatments. These elements underline the need to reappraise the approach to post-viral cough, considering both inflammatory nature of symptoms and new patterns of viral circulation.7
Taken together, these observations reinforce the importance of updated, evidence-based strategies for the assessment and management of acute cough in children and adolescents. Clinicians are now required to balance the reassurance that most acute coughs are benign and self-limited with the recognition of potential red flags, while at the same time avoiding unnecessary investigations and inappropriate pharmacological interventions.
Acute Cough: Practical Management
The present document summarizes and discusses updated knowledge and evidence on the pathophysiology and treatment of acute cough. In addition, it revises the previously proposed practical algorithm for the clinical management of children and adolescents with acute cough. A specific novelty of this position paper is the formal inclusion of selected non-pharmacological remedies. Because the aim was to reflect real-life management, it was not possible to ignore the widespread interest of parents and many physicians in “natural” products, which are often perceived as both effective and safe. Several reviews have re-examined this topic, selecting studies according to predefined evidence-based criteria.16–18 Overall, the literature shows that only a limited number of substances are supported by sufficiently robust evidence to warrant recommendation in clinical practice. Further well-designed studies, particularly in real-life settings, are therefore needed to provide convincing data on their efficacy and safety.
Causes of Acute Cough in Children
In children, acute cough in children is most commonly caused by acute viral infections, including common colds, acute bronchitis, bronchiolitis, croup, influenza, and post-viral cough or by exposure to environmental pulmonary toxicants. However, acute cough may also be less common, but leads to potentially serious conditions, such as asthma exacerbations, pneumonia, or foreign body aspiration.
The main causes of acute cough in childhood are summarized in Table 1.
Algorithm-Based Approach to Acute Cough
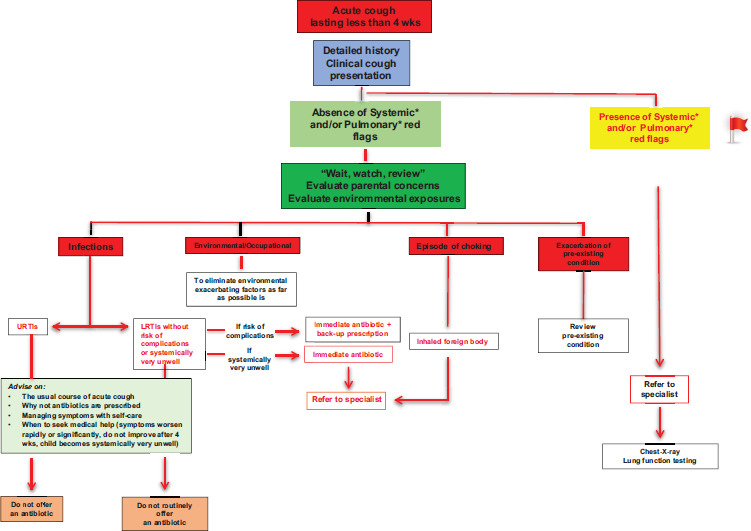
Algorithm for the management of acute cough provides a structured framework to guide clinical reasoning and ensure an evidence-based, stepwise evaluation. The approach begins with a detailed medical history, a thorough physical examination, and an assessment of cough quality (Figure 1).
Figure 1 Flow chart of acute cough assessment for children in absence of systemic and/or pulmonary flags
In most cases, acute cough in children results from viral URTIs and resolves spontaneously without complications. Nevertheless, a meticulous history remains essential to avoid missing or delaying the diagnosis of potentially serious underlying disorders. Key aspects to investigate include the child’s age, the duration and onset of cough, its qualitative features, possible triggers, associated symptoms or signs, and particular attention on red flags as outlined in Figure 2.
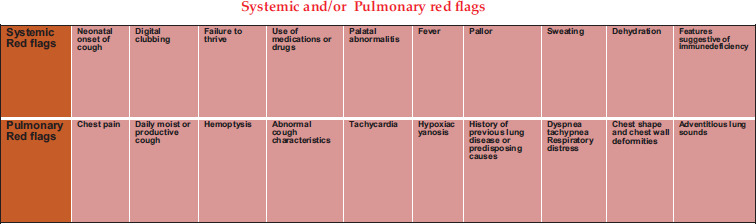
Figure 2 Red flags for severe acute cough.
Children should always be examined for systemic or pulmonary abnormalities (Table 2). The absence of such findings supports the likelihood of a benign, self-limiting cause, whereas the presence of fever, respiratory distress, abnormal auscultatory findings, or systemic involvement warrants further investigation. In addition, parental expectations and modifiable exacerbating factors, such as exposure to tobacco smoke, biomass fuels, indoor allergens, or outdoor air pollution, should also addressed, regardless of the suspected etiology.
Table 2 List of systemic and pulmonary red flags.
| Systemic red flags | Neonatal onset of cough | Digital clubbing | Failure to thrive | Use of medications or drugs | Craniofacial, palatal abnormalities | Fever | Pallor | Sweating | Dehydration | Features suggestive of immune deficiency | Neuromuscular disorder |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pulmonary red flags | Chest pain | Coughing is progressive, daily moist or productive cough | Hemoptysis | Abnormal cough characteristic | Tachycardia | Hypoxia cyanosis | History of previous lung disease or predisposing causes | Dyspnea tachypnea respiratory distress | Chest shape and chest wall deformities | Adventitious lung sounds | Coughing initiates suddenly with a choking episode, swallowing difficulties |
When “cough pointers” are identified, they may indicate specific acute disorders requiring targeted investigation and management (Figure 2). Importantly, in children, the quality and temporal pattern of cough often provide valuable diagnostic clues. As a pragmatic rule, dry cough usually reflects an irritative or inflammatory process involving the airways or adjacent structures, whereas wet cough is more consistent with productive cough because of postnasal drip, or less frequently a mucus hypersecretion, or impaired mucociliary clearance (Table 3).
Table 3 Quality of cough and suggested underlying causes or contributing factors.
| Quality of cough | Suggested underlying causes or contributing factors |
|---|---|
| Barking or brassy cough or honking | Croup, tracheomalacia, and habit cough |
| Paroxysmal (with/without whoop) | Pertussis and parapertussis |
| Staccato, dry cough | Mycoplasma pneumoniae, Chlamydia pneumoniae; post-viral cough syndrome, cough variant asthma |
| Wet cough | Protracted bacterial bronchitis, pneumonia, bronchiectasis, cystic fibrosis, primary ciliary dyskinesia |
Dry cough frequently accompanies infections such as pertussis, pertussis-like illness, post-viral cough syndrome, Mycoplasma pneumoniae or Chlamydia pneumoniae infections. These conditions are typically characterized by a paroxysmal, sometimes spasmodic cough, often associated with other features of respiratory infection, including pharyngitis. An infectious cause should be particularly suspected when there is a history of close contact with symptomatic individuals. Pertussis and pertussis-like illness must be considered even in fully immunized children, as partial vaccine failure is a recognized phenomenon.
Dry and paroxysmal cough, in the absence of wheeze, chest tightness, or dyspnoea may represent the predominant manifestation of cough-variant asthma (CVA). Episodes commonly occur in response to typical asthma triggers, such as cold air, weather changes, exercise, and exposure to outdoor or indoor pollutants. Because patients with CVA often exhibit variable expiratory airflow limitation and bronchial hyperresponsiveness, they tend to benefit from standard asthma therapies, particularly inhaled corticosteroids.18 Early diagnosis and appropriate treatment may delay progression to classic asthma in predisposed individuals. Conversely, children who have experienced CVA but have never wheezed and have no other evidence of atopy appear to have a very low risk of developing asthma.19
A barking or brassy cough, particularly when associated with stridor and hoarseness, is highly suggestive of croup. In contrast, a sudden onset of cough accompanied by wheeze, stridor, respiratory distress, or additional symptoms, such as drooling, gagging, vomiting, and dysphonia, or cyanosis raises strong suspicion of foreign body aspiration, which requires urgent assessment.
A dry cough present since birth should prompt consideration of congenital airway malformation, such as tracheomalacia, especially when associated with failure to thrive, stridor, dyspnea, respiratory distress, recurrent lower respiratory tract infections (LRTI), or dysphagia.19
Habit cough (also referred to as habit-tic cough, psychogenic cough, somatic cough disorder, or functional cough) occurs when psychological distress manifests as a cough. It is typically a dry, often harsh cough that usually begins after a viral URTI.20 It is predominantly a daytime phenomenon, occurring many times per minute with a strikingly regular pattern, and it tends to diminish when the child is distracted or asleep, although complete absence at night is relatively uncommon. The frequent presence of additional somatic complaints, such as throat or chest pain, breathlessness, hyperventilation, palpitations, headache, nausea, or vomiting, may lead to extensive (and sometimes unnecessary) investigations.20
Similarly, vocal tics can manifest as a dry cough, often accompanied by throat-clearing and and other stereotyped vocalizations, and may form part of a generalized tic disorder.20
A wet cough is usually indicative of productive cough due to postnasal drip or less frequently a mucus hypersecretion, or impaired mucociliary clearance.21 Persistent wet secretions associated with bacterial infection may suggest protracted bacterial bronchitis (PBB), which is characterized by: (i) chronic wet cough lasting for more than 4 weeks; (ii) absence of specific pointers to alternative causes of wet cough; and (iii) resolution of symptoms following a 2–4-week course of appropriate oral antibiotics. The most common pathogens are Haemophilus influenzae, Streptococcus pneumoniae, and Moraxella catarrhalis.22
Whenever possible, clinicians should directly listen to, and, when feasible, record the cough during the visit to corroborate the history. It is important to remember that cough quality and pattern can change over time; for example, a dry cough may evolve into a wet cough as airway secretions increase.
A cautious interpretation is therefore essential, as cough characteristics alone are not sufficiently specific to distinguish reliably between common causes of acute cough in children.23 Cough description should always be integrated with the overall clinical context and considered as one component, rather than the sole determinant, of diagnostic decision-making.
Therapeutic Management of Acute Cough
The therapeutic management of acute cough in children should be pragmatic and evidence-based, with the primary goal of relieving discomfort and improving quality of life (QoL) while avoiding unnecessary or potentially harmful treatments. Since most cases are of viral and self-limiting origin, reassurance, parental education, and symptom severity monitoring remain the cornerstones of care. Non-pharmacological measures, such as adequate hydration, nasal saline irrigation, humidified air, and avoidance of irritants, such as tobacco smoke, should always represent the first-line approach.8
The inappropriate use of antibiotics or systemic corticosteroids should be strongly discouraged, as these agents provide no benefit in uncomplicated viral coughs and may contribute to antimicrobial resistance or adverse effects.24 Likewise, centrally acting antitussives, such as codeine, dextromethorphan, or cloperastine, have limited efficacy and safety concerns, including sedation and respiratory depression, and should not be used in children.25
The main therapeutic strategies are summarized in Table 4.
Table 4 Therapeutic options for the management of acute and post-viral cough in children.
| Therapeutic category | Examples of active substances | Mechanism of action | Evidence and indications | Comments/safety considerations |
|---|---|---|---|---|
| Non-pharmacological measures | Hydration, humidified air, nasal saline irrigation, environmental control | Maintain mucosal hydration and mucociliary clearance; reduce cough triggers | First-line in all children with acute viral cough | Simple, safe, cost-effective; universally recommended |
| Peripheral antitussives | Levodropropizine | Inhibits cough reflex via modulation of peripheral sensory (C-fiber) activity | Suggested efficacy in acute post-viral cough by real word evidence; improves sleep and QoL | Nonsedative; well-tolerated; suitable from age ≥2 years |
| Central antitussives | Codeine, dextromethorphan, cloperastine, butamirate | Suppress cough center in medulla | No consistent benefit in children; potential toxicity | Contraindicated or not recommended for children aged <12 years; risk of sedation, respiratory depression |
| Mucolytics/expectorants | Ambroxol, acetylcysteine, carbocysteine, guaifenesin | Alter mucus viscosity or secretion | Insufficient evidence in children; may induce vomiting or paradoxical cough | Avoid in children aged <2 years; limited role overall |
| Anti-inflammatory therapy | Corticosteroids (systemic or inhaled) | Reduces airway inflammation | Only indicated for specific conditions (asthma, croup) | No role in simple viral cough |
| Natural/plant-based medical devices | Plantago lanceolata, Grindelia robusta, Thymus vulgaris, Helichrysum italicum, Althea officinalis, Hedera helix | Forms a protective mucosal barrier; demulcent, antioxidant effects | May reduce cough frequency and throat irritation; modest benefit in post-viral cough | Variable quality and standardization; use only certified formulations |
| Medical devices containing complex botanical substances with honey | Grindelia, Helichrysum, Plantago Biological honey | Demulcent, antioxidant, anti-inflammatory, and reduces reflex sensitivity | Evidence of reducing cough duration and severity | Contraindicated in infants aged <12 months (for honey) |
| Honey and glycerol-based products | Honey, honey + glycerol syrups | Demulcent and antioxidant; soothes throat and reduces reflex sensitivity | Limited or no clinical evidence supports honey- and glycerol-based products in children aged >1 year | Contraindicated in infants aged <12 months (risk of botulism); adjunctive role only |
| Emerging pharmacological agents | P2X3 antagonists (gefapixant, eliapixant), transient receptor potential (TRP) channel modulators, NK1 receptor antagonists | Target vagal afferent hypersensitivity and neurogenic inflammation | Promising results in adults with chronic refractory cough | Not yet approved for pediatric use; potential future options |
Pharmacological Management of Acute and Post-Viral Cough
The pharmacological management of acute cough in children should be reserved for selected cases, such as where the symptom significantly interferes with sleep, feeding, or daily activities. As cough is a physiological reflex essential for airway clearance, the goal of therapy is not suppression per se, but modulation of excessive or distressing cough that persists beyond the acute viral phase.25
Pharmacological intervention becomes appropriate when cough is frequent, and disturbing, especially at night, and when the physical examination and clinical context exclude serious underlying conditions. In these cases, treatment may be aimed at reducing cough reflex hypersensitivity, which can persist after viral infections because of residual airway inflammation and neurogenic activation. Post-viral cough is often sustained by peripheral sensory nerve hyperexcitability, leading to exaggerated cough responses to minimal stimuli.26
In this setting, peripherally acting antitussives, are preferable to central cough suppressants. Unlike codeine or dextromethorphan, which inhibit the cough center and may depress respiratory drive, peripheral agents act by modulating afferent C-fiber activity in the airways, thereby reducing cough frequency without abolishing the protective reflex.24 This mechanism allows for symptom control while preserving airway defense, a key consideration in pediatric patients.
Recent Italian real-world studies have offered preliminary support to this approach. In a large observational multicenter primary-care study, children with post-viral cough treated with levodropropizine experienced a rapid improvement in cough intensity, sleep quality, and the overall well-being. Benefits were generally observed within 5–7 days, and the treatment was well tolerated, with only mild, self-limited adverse events.17,24 The study offers real-world evidence that is consistent with the efficacy and safety of peripheral, non-opioid antitussives in pediatric acute and post-viral cough, although confirmation from controlled trials is needed. Centrally acting antitussives, including codeine, cloperastine, butamirate, and dextromethorphan, lack robust evidence of efficacy in children and carry unfavorable safety profiles (sedation, respiratory depression, and risk of misuse). Their use is strongly discouraged by international agencies, such as European Medicines Agency (EMA) and Food Drug Administration (FDA), in the pediatric population.17
Other classes of agents, such as mucolytics and expectorants, have not demonstrated consistent benefit in randomized pediatric studies and may cause paradoxical worsening of cough or vomiting in young children. Their use should be avoided, particularly in children aged <2 years, where the cough reflex and mucociliary clearance are still immature.
Overall, when pharmacological treatment is indicated, peripherally acting nonsedative agents represent the most appropriate choice. Their use should always be individualized, considering age, symptom burden, and tolerance, and integrated with non-pharmacological measures and environmental control. Such a targeted approach ensures both symptom relief and physiological protection, aligning with the principles of rational, evidence-based pediatric respiratory care.24
Emerging Perspectives in Pharmacological Cough Modulation
Recent advances in cough pathophysiology have highlighted the complex interplay between airway inflammation, epithelial injury, and neurogenic sensitization, leading to persistent cough even after the resolution of infection. This condition, often referred to as post-viral, is characterized by a transient hypersensitivity of vagal afferent pathways, resulting in an exaggerated cough response to otherwise innocuous stimuli, such as talking, cold air, or mild irritants.24 In children, prolonged cough may be in rare cases neurogenic (sensory neuropathic) in origin.27
Mucosal dehydration and mechanical stimuli, caused by pharyngeal dripping of viscous nasal mucus, viruses, bacteria, inflammatory mediators, and irritant substances, play a decisive role in triggering the urge to cough and sustaining URTI-associated acute cough.28
Viral respiratory infections induce the release of pro-inflammatory cytokines, prostaglandins, and neuropeptides (such as substance P and calcitonin gene-related peptide), which enhance the excitability of sensory nerve endings in the airways. This leads to upregulation of transient receptor potential (TRP) channels, particularly transient receptor vannilloid 1 (TRPV1), TRPA1, and transient receptor melastatin 8 (TRPM8), on vagal afferents. These receptors serve as molecular “sensors” for chemical and mechanical stimuli, and their heightened activation contributes to cough reflex hypersensitivity. Understanding these mechanisms has paved the way for innovative targeted pharmacological approaches.29,30
Among these, P2X3 receptor antagonists (e.g., gefapixant and eliapixant) have emerged as a new class of neuromodulatory agents capable of suppressing pathological cough hypersensitivity by selectively blocking adenosine 5′-triphosphate (ATP)-mediated activation of vagal sensory fibers. In adults with refractory or unexplained chronic cough, gefapixant has shown significant reduction in cough frequency and severity, although its use is currently limited by dose-related taste disturbance.31 Pediatric data are still lacking, but these compounds represent a promising future direction for the management of chronic or post-infectious cough unresponsive to conventional therapy.
Other research efforts are focusing on TRP channel modulators, neurokinin-1 (NK1) receptor antagonists, and neuromodulators of the vagal pathway, aiming to restore normal cough threshold without impairing airway defense. Experimental compounds targeting TRPV1 and TRPA1 channels have demonstrated antitussive potential in preclinical studies by reducing sensory neuron excitability and inflammatory signaling.32
Although these approaches are not yet approved for pediatric use, they illustrate a paradigm shift in cough treatment, from empirical symptom suppression toward pathophysiology-driven modulation of cough reflex hypersensitivity. Future studies in children and adolescents will be essential to clarify the safety, dosing, and long-term impact of these agents as well as their integration into multimodal treatment strategies that combine pharmacological, environmental, and behavioral interventions.
Taken together, these advances reinforce the concept that the management of cough, especially post-viral, should evolve from a symptomatic to a mechanism-based approach, aimed at restoring airway sensory homeostasis and preventing chronicity.
Non-Pharmacological and Natural Remedies
In pediatric clinical practice, non-pharmacological and natural remedies are frequently used to manage acute and post-viral cough. Their popularity reflects both parental preference for “natural” therapies and the desire to avoid unnecessary pharmacological interventions. However, despite their widespread use, the scientific evidence supporting these treatments remains limited, and many available products differ widely in formulation, concentration, and quality.8
Non-pharmacological management includes a range of simple yet effective supportive measures, such as ensuring adequate hydration, maintaining ambient humidity, promoting nasal patency through saline irrigation, and eliminating environmental irritants (e.g., tobacco smoke, biomass fuels, and air pollutants). These interventions help to maintain mucociliary clearance and reduce cough reflex activation, and should be universally recommended as the first step in management for all children with acute cough.24
Beyond these general measures, numerous herbal extracts and natural products have been investigated for their potential soothing, demulcent, or mucosal protective effects. The SIAIP Task Force on Nutraceuticals and Medical Devices has recently reviewed the most commonly used natural preparations for pediatric cough, such as formulations based on Plantago lanceolata, Grindelia robusta, Helichrysum italicum, Thymus vulgaris, Althea officinalis, Hedera helix, and honey.25 These compounds often act via non-pharmacological mechanisms, forming a protective film over the inflamed mucosa, thus reducing irritation and local inflammation. In URTI-associated acute cough, mucosal dehydration and mechanical stimuli from viscous postnasal drip, pathogens, and inflammatory mediators play a decisive role; the barrier action of these agents helps to counteract exactly these processes. Many are classified as medical devices rather than drugs, as their action is primarily physical, rather than systemic.
Among these natural options, honey is the best studied and most consistently effective. Several randomized controlled trials (RCTs) and meta-analyses have shown that a single evening dose of honey can reduce nocturnal cough frequency and improve sleep quality in children aged >1 year.8 Honey exerts a demulcent and antioxidant effect, stimulating salivary secretion and coating the upper airway mucosa, thereby diminishing cough reflex sensitivity. However, it is important to emphasize that honey must not be administered to infants aged <12 months because of the risk of infant botulism.
A high-quality specific polysaccharide–resin–saponins–honey-based medical device, specifically formulated for the treatment of post-viral acute cough, has been demonstrated in a pediatric RCT to be superior to placebo in nocturnal and more intense cough, and to carbocysteine in all the items of the cough score adopted in the study to evaluate night and day cough.28
There are other medical devices based on combinations of plant extracts (e.g., Thymus vulgaris L., Althaea officinalis L., and Hedera helix L.), and some of these products are often combined with glycerol, malt extract, or hyaluronic acid, which provide additional emollient and humectant effects, facilitating mucosal hydration and comfort. However, differences in botanical source, extraction process, and degree of standardization among products can significantly influence clinical outcomes. Thus, standardization, quality control, and transparency of composition are essential prerequisites for their rational use.17 The remark on “transparency of composition” does not apply to substance-based medical devices because their full qualitative and quantitative composition is already disclosed to the competent notified body during the certification process. Adequate quality is a mandatory prerequisite for product choice.
It is also important to stress that “natural” does not always mean “safe.” Adverse effects are rare but can occur, as is the case with medicines, particularly in children with allergies. In addition, effectiveness is not guaranteed. For this reason, natural products should be recommended only when documented literature evidence supports their use. As a result, in the case of acute URTI-related cough, only high-quality products with sound evidence of efficacy may be a valuable therapeutical option. When selected appropriately, they can reduce symptom perception, improve family satisfaction, and limit unnecessary use of synthetic drugs. Their integration into standard care should follow the same evidence-based criteria applied to conventional treatments: correct indication, appropriate dosing, defined treatment duration, and ongoing monitoring of response.17
Ultimately, non-pharmacological and natural remedies represent a valuable component of a holistic, patient-centered approach to pediatric cough management. Their judicious use, guided by evidence, safety, and parental expectations, can complement pharmacological options within a rational, tiered treatment strategy designed to minimize overtreatment while maintaining patient comfort and airway protection.
Conclusions and Future Directions
Cough remains one of the most frequent and distressing symptoms in pediatric practice, representing a leading cause of medical consultation, parental anxiety, and inappropriate medication use. Although most cases are benign and self-limiting, acute cough may significantly impair sleep, school performance, and the overall family well-being.
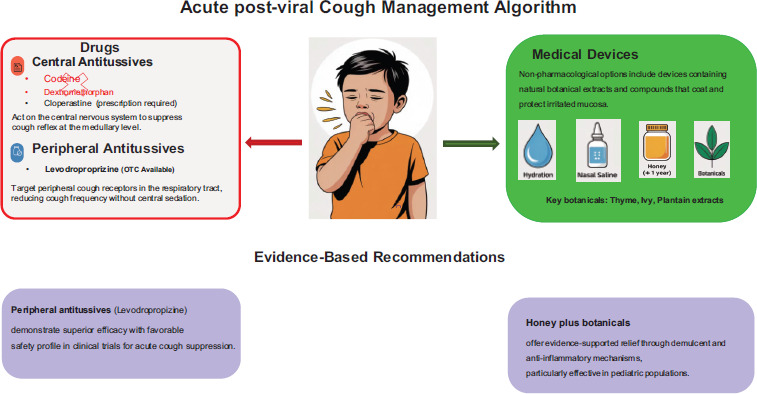
A rational, evidence-based approach should therefore guide management, as schematically represented in Figures 2–4 for the general overview and management of post-viral and non-post-viral acute cough. Careful clinical assessment and parental reassurance are often sufficient, with non-pharmacological measures, such as adequate hydration, nasal saline irrigation, and avoidance of irritants, constituting the first therapeutic step. Pharmacological therapy may be considered in selected cases in which cough becomes particularly distressing or interferes with sleep; in this context, peripherally acting, nonsedative antitussives can represent a reasonable option in terms of efficacy and safety. Centrally acting agents and unnecessary antibiotics should be avoided. In parallel, the use of standardized natural medical devices or honey-based preparations may be contemplated, with careful consideration of their composition and supporting evidence.
Figure 3 Algorithm for managing children with post-viral acute cough.
Beyond symptomatic control, there is growing awareness that post-viral cough often involves airway sensory hypersensitivity and neurogenic inflammation. This evolving concept opens new perspectives for mechanism-based treatments, including modulators of vagal afferent pathways, such as P2X3 antagonists or TRP channel inhibitors, which could represent future therapeutic options once adequately validated for pediatric use.
To advance the field, large multicenter real-world studies are needed to assess the efficacy, safety, and long-term outcomes of current pharmacological and non-pharmacological strategies. The development of validated clinical tools, including objective cough monitoring systems and parent-reported outcome measures, will allow more accurate evaluation of treatment effects in children.
Ultimately, the management of acute and post-viral cough in childhood should evolve from an empirical, symptom-based approach toward a mechanism-driven, individualized model that combines scientific evidence, clinical judgment, safety profile, and family-centered care. Such an approach will ensure not only more rational use of medicines but also improved QoL and better health outcomes for children and their families. In this context, natural remedies also could be a useful and safe approach but only if using medical device and products with adequate scientific evidence, as documented for a multicomponent medical device containing honey, Plantago lanceolata, Grindelia robusta, and Helichrysum italicum.33,34
In conclusion, the management of children with acute cough should be personalized and based on safe, mainly concerning sedative effects, and effective drugs and medical devices with well-documented literature.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Author Contributions
This study was a collaboration of all the authors.
Conflicts of Interests
The authors declared that they had no competing interests.
Funding
The publication was supported by the Italian Society of Pediatric Allergy and Immunology (SIAIP).
REFERENCES
1 Finley CR, Chan DS, Garrison S, Korownyk C, Kolber MR, Campbell S, et al. What are the most common conditions in primary care? Systematic review. Can Fam Physician. 2018;64(11):832–40.
2. Marseglia GL, Manti S, Chiappini E, Brambilla I, Caffarelli C, Calvani M, et al. Acute cough in children and adolescents: A systematic review and a practical algorithm by the Italian Society of Pediatric Allergy and Immunology. Allergologia Immunopathol. 2021;49(2):155–69. 10.15586/aei.v49i2.44
3 Brodlie M, Graham C, McKean MC. Childhood cough. BMJ. 2012;344:e1177. 10.1136/bmj.e1177
4 Chang AB. Pediatric cough: Children are not miniature adults. Lung 2010;188(Suppl 1):S33–40. 10.1007/s00408-009-9166-2
5 Irwin RS, Baumann MH, Bolser DC, Boulet LP, Braman SS, Brightling CE, et al. Diagnosis and management of cough executive summary: ACCP evidence-based clinical practice guidelines. Chest 2006;129:1S–23. 10.1378/chest.129.1_suppl.1S
6 Marchant JM, Newcombe PA, Juniper EF, Sheffield JK, Stathis SL, Chang AB. What is the burden of chronic cough for families? Chest 2008;134:303–9. 10.1378/chest.07-2236
7 Manti S, Tosca MA, Licari A, Brambilla I, Foiadelli T, Ciprandi G, et al. Cough remedies for children and adolescents: Current and future perspectives. Paediatr Drugs. 2020;22(6):617–34. 10.1007/s40272-020-00420-4
8 Ciprandi G, Tosca MA. Non-pharmacological remedies for post-viral acute cough. Monaldi Arch Chest Dis. 2021;92(1): monaldi.2021.1821. 10.4081/monaldi.2021.1821
9 Leontari K, Lianou A, Tsantes AG, Filippatos F, Iliodromiti Z, Boutsikou T, et al. Pertussis in early infancy: Diagnostic challenges, disease burden, and public health implications amidst the 2024 resurgence, with emphasis on maternal vaccination strategies. Vaccines (Basel). 2025;13(3):276. 10.3390/vaccines13030276
10 Rao S, Gross RS, Mohandas S, Stein CR, Case A, Dreyer B, et al. Postacute sequelae of SARS-CoV-2 in children. Pediatrics. 2024;153(3):e2023062570. 10.1542/peds.2023-062570
11 Oesterle TS, Kolla B, Risma CJ, Breitinger SA, Rakocevic DB, Loukianova LL, et al. Substance use disorders and telehealth in the COVID-19 pandemic era: A new outlook. Mayo Clin Proc. 2020;95(12):2709–18. 10.1016/j.mayocp.2020.10.011
12 Lacombe A, Quintela I, Liao YT, Wu VCH. Food safety lessons learned from the COVID-19 pandemic. J Food Saf. 2021;41(2):e12878. 10.1111/jfs.12878
13 Assi M, Abbas S, Nori P, Doll M, Godbout E, Bearman G, et al. Infection prevention and antimicrobial stewardship program collaboration during the COVID-19 pandemic: A window of opportunity. Curr Infect Dis Rep. 2021;23(10):15. 10.1007/s11908-021-00759-w
14 Desai AD, Lavelle M, Boursiquot BC, Wan EY. Long-term complications of COVID-19. Am J Physiol Cell Physiol. 2022;322(1):C1–11. 10.1152/ajpcell.00375.2021
15 Onyeaka H, Anumudu CK, Al-Sharify ZT, Egele-Godswill E, Mbaegbu P. COVID-19 pandemic: A review of the global lockdown and its far-reaching effects. Sci Prog. 2021;104(2):368504211019854. 10.1177/00368504211019854
16 Murgia V, Ciprandi G, Votto M, De Filippo M, Tosca MA, Marseglia GL. Natural remedies for acute post-viral cough in children. Allergol Immunopathol (Madr). 2021;49(3):173–84. 10.15586/aei.v49i3.71
17 Ciprandi G. Natural anti-tussive products for children and adolescents: Darkness and shadow. Minerva Pediatr (Torino). 2025 (in press). 10.23736/S2724-5276.25.07848-6
18 Cox JK, Lockey R, Cardet JC. Cough-variant asthma: A review of clinical characteristics, diagnosis, and pathophysiology. J Allergy Clin Immunol Pract. 2025;13(3):490–8. 10.1016/j.jaip.2024.11.005
19 Galway NC, Shields MD. The child with an incessant dry cough. Paediatr Respir Rev. 2019;30:58–64. 10.1016/j.prrv.2018.08.002
20 Liu NM, Chadwick CL, Gupta A. Habit cough in children. Paediatr Child Health. 2023; 23(4):85–118. 10.1016/j.paed.2023.01.004
21 Gilchrist FJ. An approach to the child with a wet cough. Paediatr Respir Rev. 2019;31:75–81. 10.1016/j.prrv.2018.11.002
22 Kantar A, Chang AB, Shields MD, et al. ERS statement on protracted bacterial bronchitis in children. Eur Respir J. 2017;50(2):1602139. 10.1183/13993003.02139-2016
23 Bisballe-Müller N, Chang AB, Plumb EJ, Oguoma VM, Halken S, McCallum GB. Can acute cough characteristics from sound recordings differentiate common respiratory illnesses in children? : A comparative prospective study. Chest. 2021;159(1):259–69. 10.1016/j.chest.2020.06.067
24 Marseglia GL, Veraldi D, Ciprandi G. Management of children with acute post-viral cough: A primary care experience with levodropropizine. Minerva Pediatr (Torino). 2025;77(4):281–7. 10.23736/S2724-5276.24.07691-2
25 Ciprandi G, Nutraceutical and Medical Device Task Force of the Italian Society of Pediatric Allergy, Immunology (SIAIP). Natural anti-tussive products for children and adolescents: Darkness and shadow. Minerva Pediatr (Torino). Published online June 13, 2025. 10.23736/S2724-5276.25.07848-6
26 Marseglia GL, Ciprandi G. Levodropropizine for children and adolescents with acute post-viral cough: An evidence-based choice. Minerva Pediatr (Torino). 2024;76(6):758–66. 10.23736/S2724-5276.24.07638-9
27 Suyo MM, Covington C. An unusual case of chronic cough in a pediatric patient. Ann Allergy Asthma Immunol. 2022;129(5):S160–1. 10.1016/j.anai.2022.08.974
28 Murgia V, Manti S, Licari A, De Filippo M, Ciprandi G, Marseglia GL. Upper respiratory tract infection-associated acute cough and the urge to cough: New insights for clinical practice. Pediatr Allergy Immunol Pulmonol. 2020;33(1):3–11. 10.1089/ped.2019.1135
29 Bonvini SJ, Belvisi MG. Cough and airway disease: The role of ion channels. Pulm Pharmacol Ther. 2017;47:21–8. 10.1016/j.pupt.2017.06.009
30 Mazzone SB, Undem BJ. Vagal afferent innervation of the airways in health and disease. Physiol Rev. 2016;96(3):975–1024. 10.1152/physrev.00039.2015
31 Smith JA, Kitt MM, Morice AH, et al. Gefapixant, a P2X3 receptor antagonist, for the treatment of refractory or unexplained chronic cough: A randomised, double-blind, controlled, parallel-group, phase 2b trial. Lancet Respir Med. 2020;8(8):775–85. 10.1016/S2213-2600(19)30471-0
32 Grace MS, Bonvini SJ, Belvisi MG, McIntyre P. Modulation of the TRPV4 ion channel as a therapeutic target for disease. Pharmacol Ther. 2017;177:9–22. 10.1016/j.pharmthera.2017.02.019
33 Canciani M, Murgia V, Caimmi D, Anapurapu S, Licari A, Marseglia GL. Efficacy of Grintuss pediatric syrup in treating cough in children: A randomized, multicenter, double blind, placebo-controlled clinical trial. Ital J Pediatr. 2014;40:56. 10.1186/1824-7288-40-56
34 Cohen HA, Hoshen M, Gur S, Bahir A, Laks Y, Blau H. Efficacy and tolerability of a polysaccharide-resin-honey based cough syrup as compared to carbocysteine syrup for children with colds: A randomized, single-blinded, multicenter study. World J Pediatr 2017;13(1):27–33. 10.1007/s12519-016-0048-4