
Download
RESEARCH ARTICLE
Recurrent pediatric mast cell-mediated angioedema: a retrospective case series and reflection on classification
Martha Jimenez-Freitesa,b*, Rosa Jimenez-Feijooa,b, Jaime Lozano-Blascoa,b, Adrianna Machinena-Speraa,b, Olga Dominguez-Sancheza,b, Monica Piquer-Giberta,b, Maria del Mar Folque-Gimeneza,b, Gilda Yanez-Lemaa, Montserrat Alvaro-Lozanoa,b
aPediatric Allergology and Clinical Immunology Department, Hospital Sant Joan de Déu, Barcelona, Spain
bStudy Group for Allergic Diseases in Childhood and Adolescence, Institut de Recerca Sant Joan de Déu (IRSJD), Barcelona, Spain
Abstract
Background: Mast cell-mediated angioedema (MC-AE) is an increasingly recognized entity in pediatric allergy, distinct from bradykinin-mediated and allergic angioedema. Despite its clinical relevance, pediatric data remain limited and classification remains challenging in the absence of validated biomarkers.
Objective: To describe the clinical presentation, diagnostic workup, and therapeutic outcomes of a pediatric case series with recurrent MC-AE without wheals.
Methods: A retrospective review was conducted comprising pediatric patients with recurrent angioedema without urticaria, evaluated at a tertiary pediatric allergy unit in Barcelona between January 2021 and November 2024. Inclusion required ≥2 episodes, no wheals, and follow-up ≥12 months. Data collected included demographics, clinical features, laboratory evaluation, treatment response, and outcomes.
Results: Seven children (six females, median age at onset 6 years) met inclusion criteria. All had superficial, well-demarcated, self-limiting angioedema, most commonly periorbital. C1-inhibitor studies were normal, excluding hereditary angioedema. All responded to high-dose second-generation antihistamines; corticosteroids were used transiently in moderate/severe episodes. No patients required biologics or hospital admission. Basophil activation was positive in 1/6 tested patients. Episode frequency decreased during follow-up.
Conclusion: Pediatric MC-AE appears to represent a clinically identifiable phenotype characterized by recurrent superficial swelling, normal complement testing, and consistent antihistamine responsiveness. These findings support mechanism-oriented classification frameworks and highlight the importance of timely recognition to optimize management.
Key words: antihistamines, biomarkers, chronic urticaria, diagnosis, histaminergic angioedema, mast cell-mediated angioedema, pediatric angioedema
*Corresponding author: Martha Jimenez-Freites, Pediatric Allergology and Clinical Immunology DepartmentHospital Sant Joan de DéuPasseig Sant Joan de Déu, 208950 Esplugues de Llobregat, Barcelona, Spain. Email address: [email protected]
Received 2 December 2025; Accepted 23 March 2026; Available online 1 July 2026
Copyright: Jimenez-Freites M, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Mast cell-mediated angioedema (MC-AE) is increasingly recognized as a distinct clinical entity in pediatric patients. It is typically characterized by recurrent, sudden-onset swelling of the skin or mucosa, often affecting the face, lips, eyelids, extremities, or upper airway and is usually responsive to antihistamines or corticosteroids.1,2 Historically labeled as “histaminergic” angioedema, recent expert consensus has recommended adopting terminology that reflects its underlying pathophysiology, namely, mast cell-driven inflammation.3
Although well described in adults, pediatric data remain limited, particularly when angioedema occurs without urticaria.4,5 We report a retrospective pediatric case series of MC-AE and discuss its diagnostic and therapeutic implications in light of evolving classification frameworks.
Methods
We conducted a retrospective review of pediatric patients with recurrent angioedema without wheals evaluated at the Allergology and Clinical Immunology Department of Hospital Sant Joan de Déu, Barcelona, Spain. The study was approved by the institutional Ethics and Research Committee (27/05/2021, protocol EOM 20-21).
Inclusion criteria included age <18 years, at least two documented episodes of angioedema without concomitant wheals, and a minimum follow-up of 12 months. Diagnosis of MC-AE was established based on recurrent superficial swelling without urticaria, normal complement C4 levels, normal C1-inhibitor (C1-INH) antigenic and functional values, normal baseline serum tryptase, and consistent clinical response to second-generation H1 antihistamines and/or adrenaline.
Complement studies (C4, C1-INH antigenic levels, and C1-INH functional activity) were performed during asymptomatic periods using standardized laboratory assays (immunoturbidimetric measurement for C4 and C1-INH antigen; and chromogenic functional assay for C1-INH activity). Baseline serum tryptase was measured using automated fluoroenzyme immunoassay methods.
Bradykinin-mediated angioedema was excluded based on normal complement parameters and absence of clinical features suggestive of hereditary angioedema (HAE), including recurrent abdominal pain, laryngeal edema without antihistamine responsiveness, prolonged episode duration, and family history of C1-INH deficiency.5
All patients underwent structured clinical evaluation, including detailed history of potential triggers and targeted allergic work-up when indicated clinically. This included skin prick testing and/or specific immunoglobulin E (IgE) determination in selected patients. No IgE-mediated trigger explaining isolated recurrent angioedema was identified.
Basophil activation testing (BAT) was performed in five patients using an indirect assay in which patient serum was incubated with donor basophils. Basophil activation was assessed by the upregulation of cluster of differentiation 63 (CD63 cells) using flow cytometry. Results were interpreted according to laboratory reference thresholds. No allergen-specific stimulation was performed.
Seven patients met the inclusion criteria.
Results
Population characteristics
Seven children (six females), aged 4–14 years, were included in the study. The median age at symptom onset was 6 years (interquartile range [IQR]: 4–12 years), and the median age at specialist assessment was 12 years (IQR: 9–14 years). The median diagnostic delay between onset and evaluation by a specialist was 3 years (IQR: 0–6) and is summarized in Table 1.
Table 1 Clinical, laboratory, and treatment characteristics of pediatric patients with mast cell–mediated angioedema (MC-AE).
| Patient | Sex | Age at onset (years) | Age at assessment (years) | Episode frequency before treatment | Episode frequency during follow-up | Duration untreated | Duration treated | Main locations | Emergency visits | Adrenaline use | Response time to adrenaline | Antihistamine dose | Corticosteroids | Total IgE (kU/L) | Sensitizations | C4 (mg/L) | C1-INH antigenic (mg/dL) | C1-INH functional (%) | Basal tryptase (μg/L) | BAT result | Time since lastattack |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 12 | 15 | ~10/year | Weekly at peak | 20–30 min to 5 days | 1–3 days | Tongue, lips, uvula | Yes | No | — | Up-dosed bilastine (20 mg/12h; 10 mg/6h) | Oral and IM corticosteroids (40 mg oral; IM in ED), rapid response (minutes) | Not performed | No | 165 | 30 | 101 | Not performed | Not performed | >1 year |
| 2 | F | 6 | 9 | 2–3/week | 2–3/month | 24 hours | <24 hours | Eyelids | No | No | — | Rupatadine 10 mg up to 3/day | Oral corticosteroids | 238 | No | 101 | 27 | 99 | 4.88 | Negative | Months |
| 3 | F | 4 | 14 | 10–16/year | 2–3/year | 1–3 days | 1–2 hours | Feet, eyelids | No | No | — | Rupatadine 10 mg/day | No | 52 | No | 151 | 29 | 97 | 7.18 | Negative | >3 years |
| 4 | F | 14 | 14 | 1/month | Remission | 1–3 days | <1 Hour | Lips, eyelids, hands, knee | Yes | No | — | Ebastine 20 mg/day | No | 941 | Wallnut, Halzelnut | Not performed | Not performed | Not performed | 3.9 | Negative | >3 years |
| 5 | M | 12 | 12 | ~10 in 6 months | 1–3/year | 10-12hrs | 1-2 Hours | Eyelids, tongue | Yes | No | — | Rupatadine 10 mg up to 3/day | No | <1 | Dust mite | 446 | 30 | Not performed | 1.10 | Positive | >2year |
| 6 | F | 6 | 7 | 6/year | 1 episode in 3 months | 24 hours | <1 hour | Eyelids | No | No | — | Cetirizine 5 mg as needed | Occasional oral corticosteroids | Not performed | No | 186 | Not performed | Not performed | Not performed | Negative | >1 year |
| 7 | F | 4 | 10 | 4–5/year | 1–2/year | Minutes to <24 hours | Minutes to < 2 hours | Facial, upper airway | Yes | Yes | <30 min | Bilastine 20 mg up to 3/day | Oral and IM corticosteroids (40 mg oral; IM in ED), rapid response (minutes) | 57 | No | 189 | 26 | 92 | 1.48 | Negative | >1 year |
Three children had concomitant atopic conditions (mild atopic dermatitis or allergic rhinitis). None had chronic urticaria, autoimmune disorders, previous anaphylaxis, or documented food or drug allergies.
Clinical presentation
All children presented with well-demarcated, non-pitting, transient angioedema. The periorbital region was most frequently affected,6,7 followed by the lips and extremities. One patient developed tongue and pharyngeal edema following dental manipulation, requiring emergency department evaluation and intramuscular epinephrine. Clinical improvement occurred within minutes, with near-complete resolution within the first hour. The patient subsequently underwent additional dental procedures using the same local anesthetic without recurrence of clinical manifestations. Latex exposure was also continued without adverse reactions. No temporal or reproducible association with medications or materials used during the procedure was identified.
No systemic involvement or hospitalizations occurred after specialist assessment. Episodes typically lasted for 12–24 h when untreated and resolved more rapidly (6–12 h) with second-generation H1 antihistamines. Short course of systemic corticosteroids was administered for moderate-to-severe episode in three patients, with resolution within hours. Four children achieved disease control on standard antihistamine dosing, whereas three required dose escalation. During follow-up episode, frequency decreased in all patients. No child required biologic therapy or bradykinin-targeted treatment.
Diagnostic evaluation
All patients underwent a standardized diagnostic work-up, including detailed clinical history, physical examination, laboratory assessment, and evaluation of therapeutic response. The diagnostic approach aimed to exclude bradykinin-mediated angioedema, allergic triggers, and systemic mast cell disorders.
Complement parameters were within laboratory reference ranges in all patients. C4 levels ranged from 101 to 446 mg/L (reference range: 100–400 mg/L), with a median value of 176 mg/L. C1-INH antigenic levels ranged from 26.0 to 30.0 mg/dL (reference range: 22.0–45.0 mg/dL), and C1-INH functional activity ranged from 92% to 101% (reference range: 70–130%).
Baseline serum tryptase levels ranged from 1.10 to 7.18 µg/L (reference range: <11.4 µg/L), with a median value of 3.9 µg/L. No patient showed clinical or laboratory features suggestive of cutaneous or systemic mastocytosis. BAT was performed in six patients. One patient demonstrated a positive result. No allergen-specific stimulation was used. Total IgE levels ranged from <1 to 941 kU/L (reference range: 0–250 kU/L). Sensitization to allergens was identified in two patients but showed no temporal association with angioedema episodes. Targeted allergic evaluation, including skin testing or specific IgE if indicated clinically, did not reveal a consistent allergic trigger.
Autoimmune screening (anti-nuclear antibody [ANA], anti-double-stranded DNA [dsDNA], thyroid antibodies, and thyroid-stimulating hormone [TSH]), performed in selected patients, was unremarkable.
Treatment and follow-up
All children were treated with second-generation H1 antihistamines. Four achieved control on standard dosing, whereas three required dose escalation. Short courses of systemic corticosteroids were used in moderate-to-severe episodes in three patients. One patient required intramuscular epinephrine for airway involvement. No intubation was required. Follow-up ranged from 12 months to >3 years. Episode frequency decreased in all patients. No hospitalization occurred after initial specialist evaluation.
No patient required biologics or bradykinin-targeted therapy. Although omalizumab has demonstrated efficacy in refractory MC-AE,4,6–8 it was not necessary in this cohort.
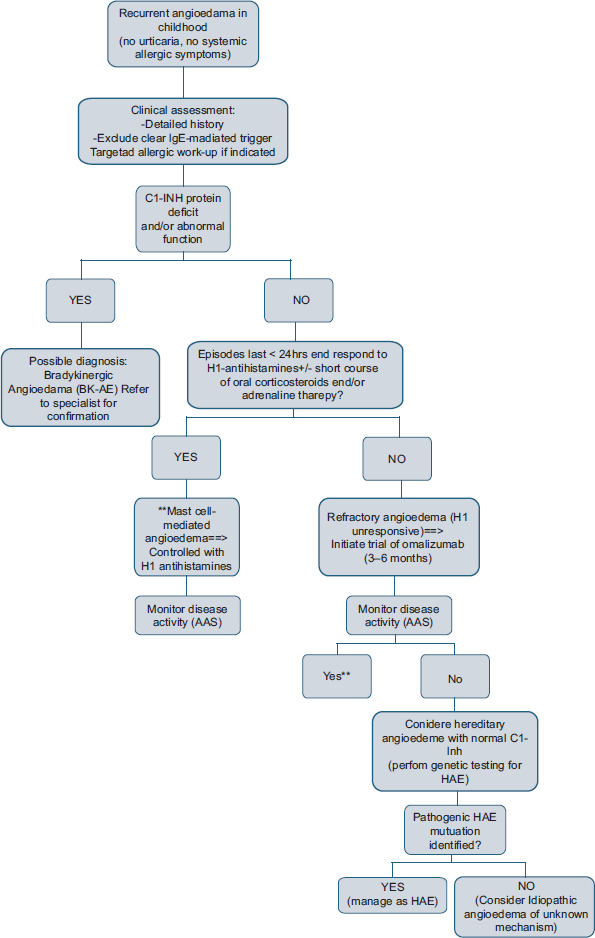
A stepwise diagnostic algorithm is summarized in Figure 1.
Figure 1 Diagnostic algorithm for pediatric recurrent angioedema without wheals. Stepwise evaluation based on exclusion of bradykinin-mediated forms and confirmation of mast cell-mediated AE. Clinical clues (such as duration, family history, and site of involvement), complement studies (C1-INH function and level), and treatment response (antihistamines, corticosteroids, and omalizumab) guide classification.
Discussion
This pediatric case series highlights key features of MC-AE as a clinically recognizable phenotype. All patients displayed recurrent superficial swelling with consistent antihistamine response. These findings were in line with recent proposals advocating for mechanism-driven classification beyond traditional symptom-based terminology.3,4
Clinically, MC-AE must be distinguished from bradykinin-mediated angioedema, particularly HAE, given its potential severity and different therapeutic implications. In our series, none of the patients met clinical or laboratory criteria for HAE: had normal C4 and C1-INH levels, no family history suggestive of hereditary disease, and no history of abdominal attack or prolonged laryngeal involvement.5,7 The relatively short duration of episodes, their superficial localization, and the prompt therapeutic response further support a mast cell-driven mechanism.1,2
The use of response to second-generation H1-antihistamines as part of diagnostic approach remains central in clinical practice. As proposed by Ferrer et al.,1 a stepwise strategy based on exclusion of bradykinin pathways followed by therapeutic response can guide classification in the absence of biomarkers. Indeed, although laboratory markers, such as BAT or tryptase, were explored, their diagnostic sensitivity remained limited.6 Our findings were consistent with this observation: only one patient demonstrated a positive BAT, while the remaining laboratory evaluations were unremarkable.
Interestingly, our cohort demonstrated a female predominance and a wide age distribution at onset, partially differing from previously reported pediatric series, such as Migliarino et al., where a more balanced gender distribution was described.2 These differences may reflect referral patterns, sample size variability, or a broader clinical spectrum of MC-AE in childhood.
The observed median diagnostic delay of 3 years underlines the challenges in recognizing MC-AE. This delay probably reflects ongoing uncertainty in differentiating histaminergic from bradykinin-mediated forms and may contribute to delayed referral to specialized care.
Notably, none of our patients required escalation of omalizumab despite its reported efficacy in refractory MC-AE.8 This observation supports the generally manageable characteristic of pediatric MC-AE under optimized antihistamine therapy, in contrast to chronic spontaneous urticaria with angioedema, where long-term control may be more challenging.9
This study has several limitations. The sample size was small and reflected the rarity in pediatric populations. The retrospective, single-center design could limit generalizability. Genetic testing for factor XII-associated angioedema was not systematically performed. BAT was not available to all patients and remained investigational. In addition, no validated quality-of-life instruments were used. Despite these limitations, the consistency of clinical features, laboratory findings, and therapeutic responses provided relevant real-world insight into this under-recognized phenotype.
Overall, our findings contribute to the growing body of evidence supporting mechanism-oriented classification of angioedema. International initiatives, such as the definition, acronyms, nomenclature, and classification of angioedema (DANCE) consensus, emphasize the importance of distinguishing mast cell-mediated forms from bradykinin-mediated forms on pathophysiological grounds.3 While larger prospective studies are needed, our series provides pediatric-specific clinical data aligned with this evolving framework.
Conclusion
This pediatric case series supports the recognition of MC-AE as a clinically identifiable phenotype characterized by recurrent superficial swelling, normal complement testing, and consistent response to antihistamines. A mechanism-oriented framework may enhance diagnostic clarity and aligns with emerging international consensus recommendations. Earlier specialist evaluation may help reduce diagnostic delay and improve clinical management.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Author Contributions
Martha Jimenez-Freites contributed to study conception and design, data collection, data analysis, and manuscript drafting.Rosa Jimenez-Feijoo, Jaime Lozano-Blasco, Adrianna Machinena-Spera, Olga Dominguez-Sanchez, Monica Piquer-Gibert, Maria del Mar Folque-Gimenez, and Gilda Yanez-Lema contributed to data collection and critical revision of the manuscript.Montserrat Álvaro-Lozano supervised the study, contributed to study design, and critically revised the manuscript. All authors approved the final version of the manuscript.
Conflict of Interest
The authors had no conflict of interest related to the content of this manuscript.
Funding
This research received no external funding.
REFERENCES
1 Ferrer M, Rodriguez-Garijo N, Sabaté-Brescó M. Medical algorithm: Diagnosis and management of histaminergic angioedema. Allergy. 2023 Feb;78(2):599-602. 10.1111/all.15618. Epub 2022 Dec 15.
2 Migliarino V, Zago A, Martelossi C, Barbi E, Giangreco M, Berti I, et al. Natural History of Pediatric Idiopathic Histaminergic Angioedema: A Retrospective Monocentric Study. Children. 2025 May 1;12(5). 10.3390/children12050600
3 Reshef A, Buttgereit T, Betschel SD, Caballero T, Farkas H, Grumach AS, et al. Definition, acronyms, nomenclature, and classification of angioedema (DANCE): AAAAI, ACAAI, ACARE, and APAAACI DANCE consensus. J Allergy Clin Immunol. 2024 Aug 1;154(2):398–411.e1. 10.1016/j.jaci.2024.03.024
4 Caballero T, Ferrer M, Guilarte M. Classification and treatment of angioedema without wheals: A Spanish Delphi consensus. Am J Clin Dermatol. 2023 Jan 1;24(1):135–41. 10.1007/s40257-022-00735-7
5 Maurer M, Magerl M, Betschel S, Aberer W, Ansotegui IJ, Aygören-Pürsün E, et al. The International WAO/EAACI guideline for the management of hereditary angioedema—The 2021 revision and update. Allergy Eur J Allergy Clin Immunol. 2022 Jul 1;77(7):1961–90.
6 Bindke G, Gehring M, Wieczorek D, Kapp A, Buhl T, Wedi B. Identification of novel biomarkers to distinguish bradykinin-mediated angioedema from mast cell-/histamine-mediated angioedema. Allergy Eur J Allergy Clin Immunol. 2022 Mar 1;77(3):946–55. 10.1111/all.15013
7 Buttgereit T, Vera C, Aulenbacher F, Church MK, Hawro T, Asero R, et al. Patients with chronic spontaneous urticaria who have wheals, angioedema, or both, differ demographically, clinically, and in response to treatment—Results From CURE. J Allergy Clin Immunol Prac. 2023 Nov 1;11(11):3515–25.e4. 10.1016/j.jaip.2023.08.020
8 Goswamy VP, Lee KE, McKernan EM, Fichtinger PS, Mathur SK, Viswanathan RK. Omalizumab for treatment of idiopathic angioedema. Ann Allergy Asthma Immunol. 2022 Nov 1;129(5):605–11.e1. 10.1016/j.anai.2022.07.017
9 Sabaté-Brescó M, Rodriguez-Garijo N, Azofra J, Baeza ML, Donado CD, Gaig P, et al. A comparative study of sex distribution, autoimmunity, blood, and inflammatory parameters in chronic spontaneous urticaria with angioedema and chronic histaminergic angioedema. J Allergy Clin Immunol Prac. 2021 Jun 1;9(6):2284–92. 10.1016/j.jaip.2021.03.038