
Download
ORIGINAL ARTICLE
Reduced baseline lung function in asymptomatic and symptomatic infants with recurrent asthma-like symptoms
Javier Mallola*, Viviana Aguirre-Camposanoa, Gustavo Falbo Wandalsenb
aDepartment of Paediatric Respiratory Medicine, Hospital and CRS El Pino, University of Santiago de Chile (USACH)
bDivision of Allergy, Clinical Immunology, and Rheumatology, Department of Paediatrics, Federal University of São Paulo (UNIFESP), São Paulo, Brazil
Abstract
Background: Recurrent asthma-like symptoms (RALS) in infants, defined as three or more physician-diagnosed episodes of wheezing and cough in the past 12 months, are the most common clinical presentation of asthma during the first two years of life. During exacerbations, patients may experience severe episodes and often require emergency department visits or hospitalisation. However, there is limited information on lung function (LF) during symptomatic periods compared to asymptomatic periods and in healthy controls.
Methods: The baseline LF of 264 infants aged < 15 months with RALS (94 symptomatic and 170 asymptomatic) was measured using rapid thoracic compression from the raised volume technique, and 44 healthy infants were included as the control group. The measurements were converted to z-scores for analysis and comparison.
Results: The mean LF was significantly lower in symptomatic than in asymptomatic infants. Additionally, LF in the asymptomatic group was significantly lower than that in healthy infants. Tobacco smoking during pregnancy, frequent wheezing episodes (≥7), and family history of asthma were significantly associated with a higher proportion of abnormal FEV0.5 (z-score < −1.64) across the entire group of RALS infants.
Conclusion: Infants with RALS exhibit markedly reduced LF during symptomatic episodes. Furthermore, even when asymptomatic, they exhibit substantially lower LF than normal infants. These functional features support the notion that LF deficits are present very early in life in infants with RALS. This may also help explain the high prevalence of frequent and severe episodes observed in infants with RALS in clinical practice. © 2026 Codon Publications. Published by Codon Publications.
Key words: airway narrowing, infants, lung function, recurrent asthma-like symptoms, spirometry
*Corresponding author: Javier Mallol, Department of Paediatric Respiratory Medicine, Hospital CRS El Pino, Ave. Alberto Hurtado 13560 Santiago, Chile. Email address: [email protected]
Received 18 November 2025; Accepted 10 January 2026; Available online 1 May 2026
Copyright: Mallol J, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Recurrent asthma-like symptoms (RALS) in infants, characterised by recurrent episodes of wheezing and coughing, constitute a highly prevalent condition and represent the most common clinical manifestation of asthma during the first two years of life. This condition constitutes a significant burden of medical consultations, frequent medication use, and a high prevalence of emergency department visits and hospital admissions, as reported in large international, population-based studies.1,2 In addition, long-term follow-up studies have shown that suffering from RALS in the first two years of age, particularly if infants have decreased LF, bronchial hyperresponsiveness (BHR), and frequent or severe wheezing episodes, is linked to a higher risk of asthma, BHR, low LF, and chronic obstructive pulmonary disease (COPD) later in life.3-8
In infants with RALS, the baseline LF is reduced compared to that in healthy infants, as measured by spirometry using raised volume rapid thoracoabdominal compression (RVRTC) or other techniques.4,8–12 This finding of reduced LF early in infants with RALS supports the concept of an airway structural/functional disturbance that begins in the foetal stage or very early after birth.3–6,13–15 Although the standard practice is to assess LF in RALS infants when they are asymptomatic, measuring LF during symptomatic episodes may broaden the information about their respiratory status and eventually help physicians with disease classification and therapeutic decision making. However, there is little information on LF measured using infant spirometry during the symptomatic period.16 Further airway narrowing in infants with RALS when symptomatic would be a plausible explanation for the high prevalence of severe clinical expression (severe episodes, visits to the Emergency Department, and hospitalisation) in this group of patients1,2 when they become respiratory symptomatic. This knowledge may have clinical and preventive implications for the early management of infants with RALS. The present study aimed to describe and compare the spirometric baseline LF in symptomatic and asymptomatic infants with RALS and healthy infants.
Methods
This cross-sectional retrospective study describes the baseline spirometric LF data of 264 infants diagnosed with RALS who were monitored at our outpatient respiratory clinic between 2005 and 2012. Their LF was consecutively measured using the RVRTC technique, spirometry from now on, and following the ERS/ATS recommendations.17 The recorded parameters for analysis were forced vital capacity (FVC), forced expiratory volume at 0.5 s (FEV0.5), forced expiratory flow at 50% and 75% of FVC (FEF50 and FEF75), FEF25–75%, and FEV0.5/FVC.
At the time of measurement, 94 patients were symptomatic, while 170 were asymptomatic; all measurements were conducted at the Department of Paediatric Respiratory Medicine, Hospital El Pino, Santiago de Chile, and the control group consisted of 44 healthy infants. Patients were treated with inhaled corticosteroids (budesonide 200 mcg/day or equivalent) and inhaled salbutamol as needed.None of the patients were receiving oral corticosteroids, theophylline, or leukotriene receptor antagonists.
The asymptomatic group consisted of infants with RALS without upper respiratory tract infection (common cold), coryza/rhinorrhoea, cough/wheezing, or other respiratory symptoms in the 4 weeks preceding testing and at the clinical examination, as determined by a paediatric respiratory physician on the day of the measurement. The RALS symptomatic infant group consisted of infants who had mild-to-moderate respiratory symptoms (coryza, cough/wheezing) that started in the previous 7 days, as reported by the mother and confirmed by a paediatric respiratory physician on the measurement day. Infants with symptoms occurring within the preceding four weeks but not in the last seven days were not tested until at least one symptom-free month had elapsed, ensuring a clear separation between symptomatic and asymptomatic groups at the time of RVRTC assessment.
All infants in both the symptomatic and asymptomatic groups had normal pulse oximetry and no respiratory distress or fever. In the symptomatic group, gentle suction of the nostrils after normal saline (0.9%) solution was performed before testing, when necessary. Viral testing was not conducted due to limited availability, as testing resources were prioritised exclusively for hospitalised infants at that time. The control group consisted of forty-four healthy, full-term infants without any known chronic or acute respiratory disease and without upper or lower respiratory symptoms in the four weeks preceding testing. Infants were recruited from routine health checkups and vaccination clinics.
Infants with severe wheezing, recovering from pneumonia or other lower respiratory infections, suffering from chronic illnesses affecting the lungs, hospitalised in the past three months, or using systemic corticosteroids in the past four weeks were excluded. Inhaled beta-agonists were withheld 12 hours before the measurements, while inhaled corticosteroids were continued as prescribed by physicians.
This study was approved by the Scientific Ethics Committee of the Chilean Ministry of Health and the Southern Metropolitan Health Service in Santiago, Chile. Written informed consent was obtained from all parents, who were present throughout the entire procedure.
Lung function testing
Lung function measurements were performed by the same physicians, who were familiar with the patients’ medical histories, six hours postprandial, while sleeping under sedation with chloral hydrate (70–90 mg/kg), and using the spirometry technique, as described in detail elsewhere.18 Briefly, a facemask was positioned over the infant’s face, covering the mouth and nose, while keeping the neck slightly extended during the procedure, with the mouth slightly open and a gentle anterior jaw thrust19 to facilitate as much lung insufflation and forced expiration through the mouth as possible. Lung inflation pressure was set at 30 cm H2O, and after delivering several sequential inflations to that lung volume, and when a respiratory pause was evident, thoracic compression was initiated, and a series of manoeuvres were performed using an increasing range of jacket pressures (30–110 cm H2O)17 until there was no further increase in flows with subsequent increases in jacket pressure (flow limitation). The best curve was selected from three reproducible curves as the single best-shaped curve with the highest sum of FVC and FEF25–75%; the values from that curve were computed for analysis.16–18 Abnormal LF was defined as a z-score < -1.64 for any of the studied spirometry parameters and categorised as normal/abnormal for the analysis.
We hypothesised that asymptomatic infants with RALS have reduced baseline LF, which further deteriorates during symptomatic episodes without reaching normal levels during asymptomatic periods. With our current sample sizes (264 infants with RALS and 44 healthy controls), there is an 84.5% likelihood of finding a significant difference in LF between groups when a real difference, specifically a medium effect size (Cohen’s d = 0.5), is present.
Statistical analysis
Descriptive statistics were used to analyse categorical variables, and logarithmic transformations were applied to variables that were not normally distributed. Values for FVC, FEV0.5, FEF50, FEF75, FEF25–75%, and FEV0.5/FVC in the three study groups were converted to z-scores using the equations of Jones et al.20 and analysed with non-para-metric statistics (Mann–Whitney, Kruskal–Wallis tests) and ANOVA with Welch’s t-test, which allows for unequal variances and group sizes. In the entire group of RALS infants (n = 264), analysis of variance was used to assess differences in z-scores of FVC, FEV0.5, FEF50, FEF75, FEF25–75%, and FEV0.5/FVC based on factors such as sex, family history of asthma, current maternal tobacco smoking, maternal smoking during pregnancy, second-hand tobacco exposure at home, admissions for acute lower respiratory infection, and frequent wheezing episodes (≥7). The proportions of infants with abnormal LF in the asymptomatic and symptomatic groups were compared using the chi-square test.
The association of abnormal FEV0.5 in the whole RALS group (symptomatic and asymptomatic pooled) with factors such as sex, family history of asthma, current maternal tobacco smoking, exposure to second-hand tobacco smoke at home, maternal smoking during pregnancy, and frequent wheezing (≥7) was assessed using a multivariable stepwise logistic regression model. The variables included in the model were selected based on clinical relevance and p-values < 0.10 in the univariate analysis. Model diagnostics included the Hosmer–Lemeshow test for goodness of fit and checks for multicollinearity. To account for multiple comparisons, the Bonferroni correction was applied to the six spirometric parameters (adjusted alpha = 0.008). Missing data were handled via listwise deletion and were less than 5% for all variables.
The results for LF parameters were expressed as z-scores and 95% confidence intervals (95% CI), whereas the anthropometric variables (age, weight, and height) were reported as the mean and 95% CI. In the whole RALS group, the prevalence of variables such as family history of asthma, tobacco exposure during pregnancy and at home, birth weight less than 2500 g, and frequent previous wheezing episodes (≥7) was expressed as a percentage(%) and 95% CI. Analysis was performed using statistical software, and p-values < 0.05 were considered statistically significant.
Results
There was no significant difference in the male-to-female ratio between the symptomatic (63/31; 2:1) and asymptomatic groups (113/57; 2:1), and the difference in the proportion of males between the symptomatic (67.0%) and asymptomatic (66.5%) groups was not significant. The control group was matched by sex, resulting in a 22:22 male-to-female ratio. The anthropometric characteristics of the three groups are shown in Table 1. There were no significant differences in the anthropometric variables between symptomatic and asymptomatic infants. All the infants were Hispanic.
Table 1 Anthropometric characteristics of the three groups.
| RALS | ||||||
|---|---|---|---|---|---|---|
| Healthy infants (n=44) | Symptomatic (n=94) | Asymptomatic (n=170) | ||||
| Mean | 95% CI | Mean | 95% CI | Mean | 95% CI | |
| Age (weeks) | 35.6 | 27.9–43.3 | 60.9 | 55.8–66.1 | 60.3 | 56.8–63.9 |
| Weight (kg) | 8.0 | 7.3–8.6 | 10.1 | 9.7–10.4 | 10.2 | 9.9–10.4 |
| Height (cm) | 67.9 | 65.4–70.3 | 74.8 | 73.5–76.0 | 75.1 | 74.2–76.0 |
| Birth weight (g) | 3365 | 3226–3504 | 3427 | 3328–3529 | 3399 | 3329–3469 |
| Birth height (cm) | 50 | 49.4–50.5 | 49.9 | 49.5–50.3 | 50.2 | 49.9–50.5 |
| Birth weight/height ratio | 67.2 | 64.9–69.5 | 68.5 | 66.9–70.1 | 67.5 | 66.4–68.6 |
RALS: recurrent asthma-like symptoms.
Lung function was significantly lower in the symptomatic RALS group than in the asymptomatic group (p < 0.0001); in turn, LF in asymptomatic infants was significantly lower than in the healthy control group (p < 0.0001). Z-scores for each spirometric parameter in the three groups are shown in Table 2.
Table 2 Spirometry values for healthy, symptomatic, and asymptomatic infants with RALS, z-scores mean (95% confidence interval).
| RALS | ||||
|---|---|---|---|---|
| Healthy infants n=44 | Symptomatic n = 94 | Asymptomatic n = 170 | Pa,b | |
| zFVC | 0.35 (0.02–0.68) | −1.30 (-1.57 to −1.03) | −0.60 (−0.80 to −0.40) | <0.0001 |
| zFEV0.5 | 0.40 (0.07–0.72) | −1.71 (−1.99 to −1.43) | −0.50 (−0.72 to −0.28) | <0.0001 |
| zFEF50% | −0.35 (−0.70–0.00) | −2.03 (−2.34 to −1.72) | −0.66 (−0.87 to −0.46) | <0.0001 |
| zFEF75% | −0.01 (−0.32–0.30) | −2.15 (−2.52 to −1.78) | −0.75 (−0.97 to −0.53) | <0.0001 |
| zFEF25-75% | −0.11 (−0.41–0.18) | −2.27 (−2.62 to −1.92) | −0.64 (−0.88 to −0.41) | <0.0001 |
| zFEV0.5/FVC | 0.01 (−0.25–0.27) | −0.58 (−0.87 to −0.28) | 0.26 (0.07 to 0.46) | <0.0001 |
RALS, recurrent asthma-like symptoms; z, z-scores; FVC, forced vital capacity; FEV0.5, forced expiratory volume at 0.5 seconds; FEF50%, forced expiratory flow at 50% of FVC; FEF75%, forced expiratory flow at 75% of FVC; FEF25-75%, forced expiratory flow between 25% and 75% of FVC; and FEV0.5/FVC. a: ANOVA, Welch’s test, asymptomatic vs. healthy control: p<0.0001; b: asymptomatic vs. symptomatic group: p<0.0001 (for all six spirometry parameters).
The mean number of wheezing episodes in infants with RALS was 6.92 (95% CI, 6.56–7.28), and 46.5% (95% CI, 40.30– 52.24) had seven or more episodes in the past 12 months. In addition, 26.9% (95% CI, 21.90–32.55) were exposed to smoking during pregnancy, 57.6% (95% CI, 51.55–63.39) were exposed to second-hand tobacco at home, and 76.1% (95% CI, 70.64–80.88) had a family history of asthma.
Lung function
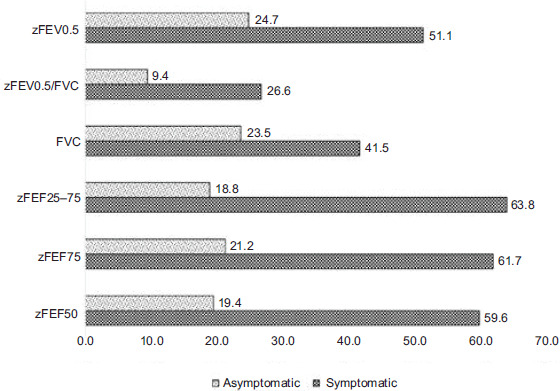
The proportion of infants with abnormal LF in the symptomatic group was approximately 2–3 times higher than that in the asymptomatic group for most spirometric parameters (p < 0.001), as shown in Figure 1, with a significant proportion of asymptomatic infants with RALS exhibiting abnormal LF. It is worth noting that all infants with RALS, both asymptomatic and symptomatic, had FVC values above the lower limit of normal (LLN; −1.64 SD). No adverse events, including vomiting, tachycardia, or hypoxaemia, were observed during or after the LF measurements. After adjusting for sex, height, birth weight under 2500 g, and admissions, the factors significantly associated with abnormal zFEV0.5 in infants with RALS were smoking during pregnancy (OR 4.26, 95% CI 2.10–8.65), family history of asthma (OR 2.26, 95% CI 1.08–4.72), and frequent wheezing episodes (≥ 7 episodes) in the past year (OR 2.84, 95% CI 1.62–4.99); sex (male) was not significantly associated with abnormal LF (OR 0.87, 95% CI 0.39–2.23, p = 0.842).
Figure 1 Proportion (%) of symptomatic and asymptomatic RALS infants with abnormal lung function (z-scores < -1.64). RALS, recurrent asthma-like symptoms; z, z-scores; FVC, forced vital capacity; FEV0.5, forced expiratory volume at 0.5 seconds; FEF50%, forced expiratory flow at 50% of FVC; FEF75%, forced expiratory flow at 75% of FVC; FEF25-75%, forced expiratory flow between 25% and 75% of FVC; and FEV0.5/FVC.
Discussion
This study demonstrated that symptomatic infants with RALS exhibited a marked reduction in LF compared to asymptomatic infants with RALS. Furthermore, infants with asymptomatic RALS had significantly lower LF than healthy controls. This supports the notion that airway obstruction in early life is dynamic and is aggravated during episodes of respiratory symptoms. These findings align with the concept that airway impairment is an early and persistent feature of RALS, as it can be detected as early as the first few weeks of life and is present before any asthma-like episode occurs.3,14 Our results add to the growing evidence that airway narrowing and hyperresponsiveness may originate prenatally, contributing to the early onset of asthma and potentially chronic obstructive pulmonary disease (COPD) later in life.4–7 Previous studies have shown that infants with a history of RALS have baseline impairments in forced expiratory flows during clinically asymptomatic periods.3,4,8–12 However, few studies have shown how much lung function is affected during symptomatic episodes16 in infants with RALS or how many of them have abnormal lung function (below the lower limit of normal) in the absence of respiratory symptoms.
Our results extend these observations by quantifying this marked additional decline, highlighting the functional impact of acute respiratory symptoms in a population already at risk. Furthermore, the high proportion of RALS infants with abnormal LF, even when they are asymptomatic, may have important clinical implications because airways with a previously reduced calibre are more susceptible to narrowing.
The limited information on LF in infants and older children with asthma during symptomatic periods is perhaps because most laboratories prefer to perform LF measurements when patients are asymptomatic. However, this may be clinically relevant, as found in the present study, where symptomatic infants were two to three times more likely to exhibit abnormal LF values than asymptomatic infants. This underlying airway dysfunction in infants with RALS, even when asymptomatic, may partly explain the high prevalence of severe episodes, ED visits, and admission during asthma-like symptom exacerbations.1,2,21,22
Our findings have important clinical implications, particularly the marked decrease in LF in infants with RALS during symptomatic periods and the lower lung function compared to healthy infants in the group of asymptomatic RALS infants. This outcome of underlying airway narrowing in infants with RALS may explain why common colds or acute viral respiratory infections result in a significant decrease in their expiratory flow rates,16 which in turn would explain the increased frequency and severity of wheezing episodes and exacerbations in infants with RALS associated with colds. A significant further decline in parameters such as FEV0.5 and FEF25–75% during symptomatic episodes points to clinically relevant bronchial obstruction related to the higher frequency and severity of wheezing episodes. Given the early onset and persistence of LF impairment in these patients, proactive monitoring and management of RALS could decrease the frequency and severity of wheezing episodes in the short term and may help prevent long-term respiratory outcomes. Repeated and severe episodes of RALS contribute to long-term respiratory functional impairment,22–26 even if symptoms are not always evident. Our results suggest that measuring LF during symptomatic periods may increase diagnostic sensitivity and assist in identifying infants who may benefit from early therapeutic and preventive interventions.
This study identified key early life risk factors independently associated with abnormal LF, such as prenatal tobacco exposure, parental asthma, and frequent wheezing episodes (≥7). These factors were consistent across symptomatic and asymptomatic infants with RALS and aligned with existing literature relating them to more frequent and severe episodes of wheezing during the first year of life at the community level,1,2,21,22 asthma development, and reduced LF later in life.23–27 Although wheezing episodes increase with age, lung function was analysed using age-adjusted z-scores, and the association between ≥7 episodes and abnormal lung function persisted, indicating a true symptom burden rather than an age effect. Parental asthma is a key criterion for predicting and diagnosing asthma in infants and preschool children using the Asthma Predictive Index (API).28 Infants with RALS and a family history of asthma showed significantly lower LF, reinforcing the diagnostic and predictive value of the API. Early identification of this high-risk group could lead to more targeted management and follow-up. We have confirmed previous findings that infants with RALS and parental asthma have a notably lower LF,3 as measured by spirometry (RVRTC), as well as by tidal LF measurements.29
The present study shows that prenatal exposure to tobacco derivatives is strongly associated with a higher proportion of infants with abnormal LF in infants with RALS, corroborating prior evidence of the detrimental impact of nicotine and other derivatives present in cigarettes, such as CO and tar, on foetal lung development, causing impaired airway growth, increased bronchial reactivity, and epigenetic alterations linked to asthma susceptibility, which may even have their origin in the grandparents.30–33 The proportion of infants with abnormal LF was more than twice as high among those exposed to maternal smoking during pregnancy. In addition, smoking during pregnancy is strongly associated with a higher prevalence of RALS during the first year of life.34 The latter reinforces tobacco smoke as a harmful determinant of structural/functional modifications of the intrauterine airway in infants exposed to prenatal maternal smoking.
A high number of wheezing episodes (≥ seven/year) was significantly associated with abnormal LF, suggesting that an increased frequency of wheezing episodes contributes to progressive airflow limitation in this group of patients, which is predicted by elevated FENO.9 supporting the notion that early therapeutic intervention using specific antiasthma medications for the management of RALS could potentially help preserve LF in these patients. However, it is important to consider that in infants with RALS receiving ICS as part of real-world routine care, several important factors, such as heterogeneous treatment initiation, limited adherence and inhalation technique, parental concern about the use of ICS, and underlying phenotypic heterogeneity of RALS, may affect therapeutic response, indicating the need for earlier, phenotype-guided, and better-supported therapeutic strategies. Therefore, the persistence of RALS and impaired lung function in treated infants should not be interpreted as evidence of therapeutic failure of ICS per se, but rather as a reflection of the complexity, variability, and limitations of real-world management in this age group.
These findings underscore the importance of properly managing wheezing episodes in infants with RALS to mitigate the frequency and severity of episodes and, eventually, long-term respiratory complications later in life.
Infants with RALS share multiple features with older children diagnosed with asthma, including clinical features, persistent LF impairment, airway hyperreactivity, and responses to environmental triggers. Reluctance to classify recurrent asthma-like symptoms in infants may delay the timely diagnosis and treatment of asthma, as suggested by the current GINA guidelines for the diagnosis of asthma in young children.35 Our findings support the need to reconsider this nomenclature, recognising that many of these infants meet the biological and clinical criteria for asthma. Labelling and managing RALS as early asthma could improve outcomes by prompting earlier interventions.
Strengths and Limitations
This study had several limitations. Its retrospective, cross-sectional design allows the identification of associations but precludes causal inference and assessment of longitudinal changes in lung function. Nevertheless, this study provides a robust characterisation of baseline lung function at a critical early life stage, thereby establishing a foundation for future prospective investigations of lung function trajectories. Although lung function was assessed at a single time point per infant, the primary objective was to characterise baseline lung function in relation to recurrent asthma-like symptoms early in life, which is a clinically relevant and under-described stage of the disease. Spirometry using the raised volume rapid thoracic compression (RVRTC) technique in infants with recurrent wheezing has several limitations, despite its recognised utility. Technical and physiological issues remain to be investigated, as reported by the International Consensus on RVRTC.17 Factors that may influence the measurement outcomes are those related to the inherent physiological characteristics of the chest wall and infant airways that may introduce uncertainties, that is, the degree of airway dynamic compression, its variability at different ages, the possibility of not reaching flow limitation during compression, the significant component given by chest-wall high flexibility during infancy, the effect of the upper airway as a resistor, the effect of different levels of sedation or idiosyncratic sedation effects, increased stomach air (stomach insufflation), among others. These complexities, along with the extensive and time- consuming measurements and inherent variability, are factors that likely explain, in part, the scarcity of studies using spirometry (RVRTC) in infants with RALS.
Another possible limitation is that spirometry parameters were converted to z-scores using widely employed reference equations,20 based on infants from the United States. Therefore, regional and ethnic differences in growth and lung development may limit their applicability to Chilean or Latin American infants; however, this remains to be proven. Furthermore, the absence of reference prediction equations specific to Chilean or Latin American infants, combined with the widespread use of Jones’ equations in multiple infant lung function studies across this region and others, supports the appropriateness of applying these equations to our patients with RALS and healthy controls.
Although lung function results were standardised for age and body size, residual confounding related to age-dependent symptom burden and cumulative respiratory exposures cannot be excluded in this cross-sectional analysis. However, it should be considered that our findings describe early baseline lung function differences associated with RALS, rather than age-dependent progression, underscoring the need for longitudinal studies beginning earlier in life. Another possible limitation was that physicians measuring lung function were not blinded to the prior clinical history; however, symptoms were assessed using a stan-dardised questionnaire, and lung function measurements were obtained using objective, protocol-driven methods, limiting potential observer bias. To minimise the likely seasonal effects, RVRTC testing was performed throughout the year, and the observed associations were not driven by the clustering of measurements in specific months.
Our results of LF measurements using the RVRTC technique in infants with RALS may have been affected by measurement variability. However, we have reported low intra-subject variability for spirometric parameters in infants with RALS using this technique (FVC = 2.9% (95% CI 2.6–3.2); FEV0.5 = 2.2% (95% CI 1.9–2.5); FEF50% = 3.7% (95% CI 3.3–4.1); FEF75% = 5.9% (95% CI 5.2–6.6); and FEF25–75% = 3.3% (95% CI 2.9–3.7)), demonstrating the high reproducibility of the spirometric parameters measured using RVRTC.18 Converting to z-scores using validated reference equations would also help reduce the variance due to growth-related differences and improve the comparability.
Size-unbalanced groups, such as those in this study, may limit the statistical certainty of the spirometric comparisons. However, with our current sample sizes (260 infants with RALS and 44 healthy controls), the design would be adequate for a medium effect size. In the context of spirometry, this means that there is an 84.5% likelihood of finding a significant difference in LF between groups when a real difference exists, specifically a medium effect size (Cohen’s d = 0.5). Thus, the sample size provided adequate power (>84%) to detect medium effect sizes in the LF comparisons.
The advantages of our study are the inclusion of both symptomatic and asymptomatic RALS infants, along with a healthy control group, all from the same centre and assessed using a standardised spirometric protocol. As previously noted, the application of z-scores for lung function comparisons enhances the robustness of our findings, and the identification of both modifiable and non-modifiable risk factors associated with abnormal lung function further adds to the study value. Additionally, this study identified that tobacco smoking during pregnancy is a strong predictor of abnormal expiratory flows (FEV0.5 and FEF25–75%) in RALS infants. The latter would be helpful for clinicians in their level of awareness when looking after RALS infants whose mothers smoked during pregnancy, as a large proportion of those infants would have abnormal expiratory flows, as found in the present study. However, this proportion may increase notably during symptomatic periods, eventually resulting in severe bronchial obstruction.
There is very little information showing the marked decrease in LF that we found in infants with RALS during exacerbation of their asthma-like symptoms.16 The results of measurements during symptomatic periods potentially amplify the detectable deficits. Measuring LF during symptomatic periods helps capture obstruction-related changes and supports the concept that airway obstruction in early life is dynamic and exacerbated during episodes of respiratory distress.
Infants with RALS share several risk factors for asthma, and this study, which shows significant LF impairment, especially when symptomatic, could help reevaluate the diagnosis of asthma in infants with RALS. The widespread impact of asthma at all ages on public health, society, the economy, and quality of life suggests that now is the right time to classify RALS as infant asthma. Persisting in excluding RALS in infants from asthma diagnosis is no longer justifiable. Advances in understanding the foetal origins of asthma,6,13,31,33 along with the availability of reliable diagnostic and predictive tools for early life,28 demand an urgent reappraisal of current clinical classification practices. Evidence from longitudinal cohort studies clearly shows that infants with RALS and reduced lung function are at higher risk of developing asthma, COPD, and long-term pulmonary function deficits.4,23–27 Health policies and paediatric respiratory guidelines should incorporate this knowledge by promoting early recognition, standardised assessment, and targeted intervention strategies for RALS in infancy.
Most epidemiological, biological, clinical, and functional expressions of asthma in older children and adults are also present in infants. Thus, an essential window of time for proper treatment and management may be lost because of nomenclature, resulting in unnecessary delays in diagnosis, adequate study, and treatment of these asthmatic infants. Perhaps a different and more appropriate management approach may ameliorate the ominous clinical and functional outcomes of RALS in infancy, childhood, and adulthood. A more proactive, asthma-oriented management approach may be warranted even at this early stage of disease, particularly during the first 12–18 months of age, a critical window during which RALS typically present with the highest frequency and greatest severity of episodes.1,2 Potential strategies include reducing early viral exposure (e.g. delaying nursery attendance in high-risk infants), improving early recognition of severe RALS phenotypes, strengthening perinatal tobacco control interventions, and optimising inhaled therapy through appropriate particle size selection and inhalation technique. Such measures may help modify adverse clinical and functional trajectories from infancy to later life.
Conclusion
This study shows that infants with recurrent asthma-like symptoms (RALS) already have a significant deficit in their LF, even when they are asymptomatic, with a further marked reduction when symptomatic. The results indicate that the LF deficit in infants with RALS occurs very early in life, supporting the idea that airway functional impairment may exist before birth. The connection between prenatal tobacco exposure, family history of asthma, and frequent wheezing with abnormal LF emphasises the need for early identification and intervention in high-risk patients. Such early LF impairment is likely to contribute to the high rates and severity of respiratory exacerbations observed in clinical practice among infants with RALS.
Acknowledgements
We are grateful to the parents and infants who participated in this study. Additionally, we appreciate the valuable collaboration and assistance provided by the staff of the Department of Paediatric Respiratory Medicine, Hospital CRS El Pino.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Author Contributions
All authors contributed equally to this article.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to research, authorship and/or publication of this article.
Funding
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
1 Mallol J, García-Marcos L, Solé D, Brand P; EISL Study Group. International prevalence of recurrent wheezing during the first year of life: variability, treatment patterns and use of health resources. Thorax. 2010;65:1004–1009. 10.1136/thx.2009.115188
2 Mallol J, Solé D, García-Marcos L, Rosario N, Aguirre V, Chong H, et al. Prevalence, severity, and treatment of recurrent wheezing during the first year of life: a cross-sectional study of 12,405 Latin American infants. Allergy Asthma Immunol Res. 2016;8:22–31. 10.4168/aair.2016.8.1.22
3 Hallas HW, Chawes BL, Rasmussen MA, Arianto L, Stokholm J, Bønnelykke K, et al. Airway obstruction and bronchial reactivity from age 1 month until 13 years in children with asthma: a prospective birth cohort study. PLoS Med. 2019;16:e1002722. 10.1371/journal.pmed.1002722
4 Owens L, Laing IA, Zhang G, Le Souëf PN. Infant lung function predicts asthma persistence and remission in young adults. Respirology. 2017;22:289–294. 10.1111/resp.12901
5 Bisgaard H, Nørgaard S, Sevelsted A, Chawes BL, Stokholm J, Mortensen EL, et al. Asthma-like symptoms in young children increase the risk of COPD. J Allergy Clin Immunol. 2021;147:569–576.e9. 10.1016/j.jaci.2020.05.043
6 Guerra S, Lombardi E, Stern DA, Sherrill DL, Gilbertson-Dahdal D, Wheatley-Guy CM, et al. Foetal origins of asthma: a longitudinal study from birth to age 36 years. Am J Respir Crit Care Med. 2020;202:1646–1655. 10.1164/rccm.202001-0194OC
7 Martinez FD. Early-life origins of chronic obstructive pulmonary disease. N Engl J Med. 2016;375:871–878. 10.1056/NEJMra1603287
8 O’Brian AL, Lemanske RF Jr, Evans MD, Gangnon RE, Gern JE, Jackson DJ. Recurrent severe exacerbations in early life and reduced lung function at school age. J Allergy Clin Immunol. 2012;129:1162–1164. 10.1016/j.jaci.2011.11.046
9 Elliott M, Heltshe SL, Stamey DC, Cochrane ES, Redding GJ, Debley JS. Exhaled nitric oxide predicts persistence of wheezing, exacerbations, and decline in lung function in wheezy infants and toddlers. Clin Exp Allergy. 2013;43:1351–1361. 10.1111/cea.12171
10 Borrego LM, Stocks J, Leiria-Pinto P, Peralta I, Romeira AM, Neuparth N, et al. Lung function and clinical risk factors for asthma in infants and young children with recurrent wheeze. Thorax. 2009;64:203–209. 10.1136/thx.2008.099903
11 Lanza FC, Wandalsen GF, Dos Santos AM, Solé D. Bronchodilator response in wheezing infants assessed by the raised volume rapid thoracic compression technique. Respir Med. 2016;119:29–34. 10.1016/j.rmed.2016.08.013
12 Llapur CJ, Martínez TM, Coates C, Tiller C, Wiebke JL, Li X, et al. Lung structure and function of infants with recurrent wheeze when asymptomatic. Eur Respir J. 2009;33:107–112. 10.1183/09031936.00106607
13 Henderson AJ, Warner JO. Fetal origins of asthma. Semin Fetal Neonatal Med. 2012;17:82–91. 10.1016/j.siny.2012.01.006
14 Turner S, Fielding S, Mullane D, Cox DW, Goldblatt J, Landau L, et al. A longitudinal study of lung function from 1 month to 18 years of age. Thorax. 2014;69:1015–1020. 10.1136/thoraxjnl-2013-204931
15 Turner S. Antenatal origins of reduced lung function—but not asthma? Respirology. 2016;21:574–575. 10.1111/resp.12794
16 Mallol J, Aguirre V, Wandalsen G. Common cold decreases lung function in infants with recurrent wheezing. Allergol Immunopathol (Madr). 2010;38:110–114. 10.1016/j.aller.2009.10.001
17 American Thoracic Society; European Respiratory Society. ATS/ERS statement: raised volume forced expirations in infants: guidelines for current practice. Am J Respir Crit Care Med. 2005;172:1463–1471. 10.1164/rccm.200408-1141ST
18 Mallol J, Aguirre VL, Wandalsen G. Variability of the raised volume rapid thoracic compression technique in infants with recurrent wheezing. Allergol Immunopathol (Madr). 2005;33:74–79. 10.1157/13072917
19 Morris MG. Nasal versus oronasal raised volume forced expirations in infants—a real physiologic challenge. Pediatr Pulmonol. 2012;47:780–794. 10.1002/ppul.22509
20 Jones M, Castile R, Davis S, Kisling J, Filbrun D, Flucke R, et al. Forced expiratory flows and volumes in infants. Normative data and lung growth. Am J Respir Crit Care Med. 2000;161:353–359. 10.1164/ajrccm.161.2.9903026
21 Bisgaard H, Szefler S. Prevalence of asthma-like symptoms in young children. Pediatr Pulmonol. 2007;42:723–728. 10.1002/ppul.20644
22 Levine H, Leventer-Roberts M, Hoshen M, Mei-Zahav M, Balicer R, Blau H. Healthcare utilization in infants and toddlers with asthma-like symptoms. Pediatr Pulmonol. 2019;54:1567–1577. 10.1002/ppul.24429.
23 Heikkilä P, Korppi M, Ruotsalainen M, Backman K. Viral wheezing in early childhood as a risk factor for asthma in young adulthood: a prospective long-term cohort study. Health Sci Rep. 2022;5:e538. 10.1002/hsr2.538
24 Goksör E, Åmark M, Alm B, Ekerljung L, Lundbäck B, Wennergren G. High risk of adult asthma following severe wheezing in early life. Pediatr Pulmonol. 2015;50:789–797. 10.1002/ppul.23071.
25 Duijts L, Granell R, Sterne JA, Henderson AJ. Childhood wheezing phenotypes influence asthma, lung function and exhaled nitric oxide fraction in adolescence. Eur Respir J. 2016;47:510–519. 10.1183/13993003.00718-2015
26 Ruotsalainen M, Piippo-Savolainen E, Hyvärinen MK, Korppi M. Adulthood asthma after wheezing in infancy: a questionnaire study at 27 years of age. Allergy. 2010;65:503–509. 10.1111/j.1398-9995.2009.02212.x
27 Ma H, Li Y, Tang L, Peng X, Jiang L, Wan J, et al. Impact of childhood wheezing on lung function in adulthood: a meta-analysis. PLoS One. 2018;13:e0192390. 10.1371/journal.pone.0192390
28 Castro-Rodríguez JA, Forno E, Padilla O, Casanello P, Krause BJ, Borzutzky A. The asthma predictive index as a surrogate diagnostic tool in preschoolers: analysis of a longitudinal birth cohort. Pediatr Pulmonol. 2021;56:3183–3188. 10.1002/ppul.25592
29 de Gouveia Belinelo P, Collison AM, Murphy VE, Robinson PD, Jesson K, Hardaker K, et al. Maternal asthma was associated with reduced lung function in male infants in a combined analysis of the BLT and BILD cohorts. Thorax. 2021;76:996–1001. 10.1136/thoraxjnl-2020-215526.
30 Gibbs K, Collaco JM, McGrath-Morrow SA. Impact of tobacco smoke and nicotine exposure on lung development. Chest. 2016;149:552–561. 10.1378/chest.15-1858
31 Miller RL, Lawrence J. Understanding root causes of asthma: perinatal environmental exposures and epigenetic regulation. Ann Am Thorac Soc. 2018;15(Suppl 2):S103–S108. 10.1513/AnnalsATS.201706-514MG.
32 Accordini S, Calciano L, Johannessen A, Benediktsdóttir B, Bertelsen RJ, Bråbäck L, et al. Prenatal and prepubertal exposures to tobacco smoke in men may cause lower lung function in future offspring: a three-generation study using a causal modelling approach. Eur Respir J. 2021;58:2002791. 10.1183/13993003.02791-2020
33 Gatford KL, Wooldridge AL, Kind KL, Bischof R, Clifton VL. Pre-birth origins of allergy and asthma. J Reprod Immunol. 2017;123:88–93. 10.1016/j.jri.2017.07.002
34 Garcia-Marcos L, Mallol J, Solé D, Brand PL; EISL Study Group. International study of wheezing in infants: risk factors in affluent and non-affluent countries during the first year of life. Pediatr Allergy Immunol. 2010;21:878–888. 10.1111/j.1399-3038.2010.01035.x
35 Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention: diagnosis of asthma in children five years and younger. 2025 GINA Strategy Report. Accessed 2025 Nov 5. Available from: https://ginasthma.org/2025-gina-strategy-report/