
Download
ORIGINAL ARTICLE
Delayed-type drug hypersensitivity reactions in a tertiary adult allergy clinic: A 5-year cohort study
Makbule Seda Bayrak Durmaza*, Begüm Görgülü Akına, Fikriye Kalkana, Betül Özdel Öztürka, Şadan Soyyiğitb
aDepartment of Immunology and Allergic Diseases, Ankara Bilkent City Hospital, Ankara, Turkey
bDivision of Allergy and Clinical Immunology, Ankara Bilkent City Hospital, School of Medicine, Ankara Yildirim Beyazit University, Ankara, Turkey
Abstract
Background and Objectives: Delayed-type drug hypersensitivity reactions (DHRs) range from maculopapular eruptions to severe cutaneous adverse reactions (SCARs). Provocation tests are unsafe in SCARs, so diagnosis depends on history, making regional data important for identifying high-risk drugs. This study aimed to retrospectively assess the clinical features and test results of patients with delayed-type DHRs in our clinic.
Materials and Methods: Adults ≥18 years with DHRs, evaluated at our clinic between 2019 and 2025, were included in this retrospective observational study. Patients with Types I–III reactions or incomplete records were excluded. Eligible cases were identified through retrospective review of medical records. Clinical data, laboratory findings, and patch and/or drug provocation test results were obtained from medical files.
Results: Thirty-three patients were included, of which 57.6% were females, and the median age was 40 years (19–70). The most common phenotype was maculopapular exanthem (n = 15, 45.5%), followed by fixed drug eruption (FDE) (n = 8, 24.2%). Seven patients (21.2%) had SCAR, including toxic epidermal necrolysis (TEN, n = 3), Stevens–Johnson syndrome (SJS, n = 1), SJS/TEN overlap (n = 1), drug-related eosinophilia and systemic symptoms (n = 1), and generalized bullous FDE (n = 1). Six patients (18.2%) required hospitalization, four of whom were managed in an intensive care or burn unit. Seventeen patients (51.5%) had a single likely culprit drug, while the remaining patients were taking multiple medications. Antimicrobials (41.3%), particularly beta-lactam antibiotics, and nonsteroidal anti-inflammatory drugs (NSAIDs, 29.3%), were the most frequently implicated drug groups. Nine patients underwent diagnostic testing (patch testing n = 6, delayed intradermal testing n = 3), with four positive results.
Conclusions: Antibiotics, especially beta-lactam antibiotics and NSAIDs, were the leading culprit drugs. Polypharmacy complicates culprit identification, particularly in SCAR cases, underscoring the need for cautious prescribing and avoidance of unnecessary medications.
Key words: beta-lactam antibiotics, drug hypersensitivity, severe cutaneous adverse reactions
*Corresponding author: Bayrak Durmaz Makbule Seda, Department of Immunology and Allergic Diseases, Ankara Bilkent City Hospital, Ankara, Turkey. Email address: [email protected]
Received 17 November 2025; Accepted 9 February 2026; Available online 1 July 2026
Copyright: Durmaz MSB, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Delayed-type drug hypersensitivity reactions (DHRs) are immune-mediated adverse drug reactions that occur more than 6 h after exposure, in contrast to immediate IgE-mediated allergies.1,2 These reactions, driven by drug-specific T lymphocytes, correspond to Gell and Coombs Type IV hypersensitivity.1,3 Clinically, they range from benign eruptions, such as maculopapular exanthem (MPE), fixed drug eruption (FDE), allergic contact dermatitis (ACD), and symmetrical drug-related intertriginous and flexural exanthema (SDRIFE), to life-threatening severe cutaneous adverse reactions (SCARs), including Stevens–Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), SJS/TEN overlap, drug reaction with eosinophilia and systemic symptoms (DRESS), generalized bullous FDE (GBFDE), and acute generalized exanthematous pustulosis (AGEP).1,4–10 SCARs are associated with widespread epidermal necrosis, mucosal injury, multiorgan involvement, and mortality rates of up to 50%.11,12
Almost any medication can provoke a delayed-type DHR. However, retrospective studies consistently implicate beta-lactam and sulfonamide antibiotics, aromatic anticonvulsants (e.g., carbamazepine), nonsteroidal anti-inflammatory drugs (NSAIDs), antigout agents (e.g., allopurinol), and certain antivirals as frequent culprits across the spectrum of delayed reactions.1,4,11–13 Regional prescribing patterns, genetic predispositions (such as HLA-B58:01 or HLA-B15:02), and population-specific susceptibilities significantly influence reaction prevalence and severity.1,11,14 Therefore, real-world epidemiologic data is essential for contextualizing risk and guiding preventive strategies.
Identifying the responsible drug in delayed DHRs, particularly in SCARs, remains challenging, as these unpredictable reactions often occur in patients receiving multiple concomitant medications.15,16 Because re-exposure may trigger severe or even fatal relapse, drug provocation testing (DPT) is contraindicated in SCARs.4,17 Diagnosis, therefore, relies primarily on a detailed clinical history and validated criteria, supplemented by patch or delayed intradermal testing (IDT) when considered safe.10,17,18 In vitro assays and genetic testing may provide complementary information, but are limited and nonstandardized.
Despite advances in understanding pathogenesis and risk prediction, regional data on the clinical spectrum and causative drugs in delayed-type DHRs remain scarce. To address this gap, we retrospectively analyzed adult patients diagnosed with delayed-type DHRs in our tertiary allergy clinic over the past 5 years. Our goal was to characterize clinical phenotypes, identify the most frequent culprit drugs, and evaluate skin testing results (including patch and delayed intradermal readings) to inform safer drug use and allergy management.
Materials and Methods
Study design and patient selection
This retrospective observational study was conducted at the Adult Allergy and Immunology Clinic of a tertiary referral hospital over 5 years (2019–2025). The study included adult patients (≥18 years) diagnosed with delayed-type (Type IV) DHRs, including MPE, FDE, SDRIFE, DRESS, GBFDE, SJS/TEN, and AGEP. Additionally, patients with ACD due to drug exposure during the same period were included. Diagnosis was established based on a compatible clinical presentation, a temporal relationship with the suspected culprit drug(s), and fulfillment of published diagnostic criteria, including the RegiSCAR (Registry of Severe Cutaneous Adverse Reactions) criteria for DRESS, consensus definitions for SJS/TEN, and the EuroSCAR (European Study of Severe Cutaneous Adverse Reactions) score for AGEP.19–21 Disease severity in SJS/TEN patients was assessed using the Severity of Illness Score for Toxic Epidermal Necrolysis (SCORTEN).22 Exclusion criteria were incomplete medical documentation, uncertain diagnoses, or nonimmunologic reactions to drugs (e.g., drug intolerance or expected side effects). Cases with alternative explanations for the eruption (such as infection-related exanthema or an autoimmune disease flare) were also excluded. Eligible cases were identified through a systematic review of electronic medical records of patients evaluated during the study period.
Data collection
Clinical data were extracted from electronic medical records using a standardized data collection form. Information captured included demographic characteristics (age and sex), comorbidities, clinical phenotype, suspected culprit drug(s), latency between drug exposure and reaction onset, and relevant laboratory findings. For SCARs, outcome measures such as recovery status, sequelae, and mortality were recorded. In DRESS cases, diagnostic certainty was assessed using the RegiSCAR scoring system.19 In patients with SJS/TEN, disease severity was assessed using the SCORTEN prognostic score.22
Diagnostic work-up
Skin testing was selectively performed in patients in whom identification of the culprit drug was clinically relevant, feasible, and considered safe, based on reaction severity, clinical phenotype, availability of a testable formulation, and patient consent. In patients with non-severe delayed-type reactions, patch testing and/or delayed intradermal testing were preferred when the suspected drug was deemed essential or likely to be needed in the future. In cases with a history of SCARs, diagnostic testing was restricted to patch testing at reduced concentrations and only performed when the potential benefit outweighed the risks, in accordance with international recommendations.
Accordingly, all cases were reviewed by an allergy specialist, and the most likely suspected culprit drug(s) were identified based on the temporal relationship and clinical judgment. When diagnostic testing was indicated, skin testing (including patch testing and delayed IDT) aided in identifying the causative agent, in accordance with international consensus recommendations.15,23 All skin tests were performed at least 6 weeks to 6 months after complete resolution of the cutaneous adverse drug reaction.24 Patch tests were performed according to the procedures recommended by the European Society of Contact Dermatitis (ESCD) and the International Contact Dermatitis Research Group (ICDRG).25 The suspected drugs were tested either in their commercial form, diluted to 30% or as pure substances diluted to 10%, in petrolatum or water. For patients with a history of SCARs such as SJS/TEN or DRESS, lower concentrations were used for safety reasons.24 Patch materials were applied under occlusion on the upper back (and, when appropriate, on the previously affected site) using Finn Chambers®. Readings were performed at 48 and 72 h, with an additional delayed reading at 7 days in selected cases.24–26 Results were interpreted according to ICDRG/ESCD scoring criteria, classifying reactions as negative, doubtful (?), irritant (IR), or positive (+, ++, +++) based on erythema, infiltration, papules, or vesicles.25 Negative (vehicle) controls were included in all cases.25 IDT were performed using sterile, injectable formulations of the suspected drug, diluted sequentially (10–4, 10–3, 10–2, 10–1) in normal saline. A small volume (0.04 mL) was injected intradermally into the volar forearm. Tests were initially read at 20 min to exclude immediate-type reactions and subsequently at 24, 48, and 72 h, with a final reading at 7 days to detect delayed hypersensitivity responses.24 Positive results were defined as an indurated erythematous papule or plaque at the injection site compared with negative controls. In selected cases, testing for safe alternative antibiotics (e.g., drug provocation or graded challenge) was performed according to the established international protocols.27
Assessment and scoring systems
The RegiSCAR scoring system was applied for the diagnosis of DRESS. This system is based on a combination of clinical and laboratory parameters, including fever, lymphadenopathy, eosinophilia, atypical lymphocytes, organ involvement, and the duration and resolution of symptoms, allowing classification of cases as possible, probable, or definite.19
Disease severity in patients with SJS/TEN was assessed using the SCORTEN, a validated prognostic tool incorporating seven independent risk factors: age >40 years, presence of malignancy, heart rate >120 beats/min, initial epidermal detachment >10% of body surface area, serum urea >10 mmol/L, serum glucose >14 mmol/L, and serum bicarbonate <20 mmol/L.22 SCORTEN scores of 0–1 are associated with an estimated mortality rate of approximately 3%, 2 points with 12.3%, 3 points with 35.4%, 4 points with 58%, and scores of 5–7 with mortality rates approaching 90%.
Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Ethics Committee (Approval No. TABED 1-25-1115).
Statistical analysis
Statistical analyses were primarily descriptive, in line with the retrospective observational study design. Continuous variables were summarized as median and range, and categorical variables as frequencies and percentages. Comparisons between SCAR and non-SCAR groups were performed for selected clinically relevant outcomes (hospitalization and systemic corticosteroid use) using Fisher’s exact test, given the small sample size. A P-value <0.05 was considered statistically significant. All analyses were performed using SPSS version 28.
Results
Patient demographics and clinical characteristics
A total of 33 patients were included in the analysis, of which 19 (57.6%) were females. The median age was 40 years (range 19–70). Sixteen patients (48.5%) had at least one comorbidity. A family history of drug allergy was reported in one of the 30 patients with available data (3.3%). This patient had a family history of beta-lactam antibiotic allergy and developed MPE after amoxicillin–clavulanate.
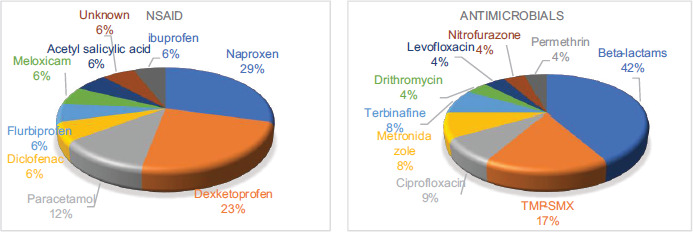
Seventeen patients (51.5%) were exposed to a single suspected culprit drug, while 16 (48.5%) had concomitant intake of multiple agents. When analyzed by the total number of implicated drugs, antimicrobial agents and NSAIDs were the most frequently suspected classes (Figure 1). The median latency between drug exposure and reaction onset was 5 days (range 1–42).
Figure 1 Distribution of suspected antimicrobial and nonsteroidal anti-inflammatory drug subgroups among delayed-type drug hypersensitivity reactions. The figure illustrates the internal distribution within the two most frequently implicated drug categories. Percentages were calculated based on the total number of suspected drugs, as multiple agents could be implicated in a single patient. Beta-lactam antibiotics: cefuroxime axetil (n = 2), amoxicillin–clavulanate (n = 2), ampicillin–sulbactam (n = 1), ceftriaxone (n = 1), cefazolin (n = 1), cefixime (n = 1), cefpodoxime (n = 2). NSAIDs, nonsteroidal anti-inflammatory drugs; TMP–SMX, trimethoprim–sulfamethoxazole.
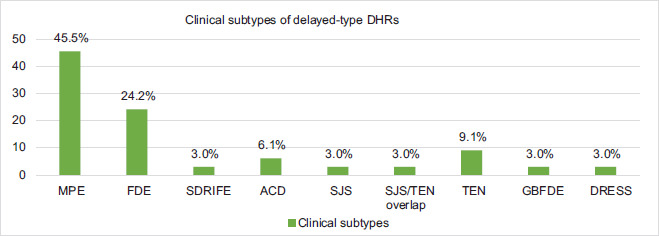
The most common clinical phenotype was MPE (n = 15, 45.5%), followed by FDE (n = 8, 24.2%). Seven patients (21.2%) experienced SCARs, including TEN (n = 3), SJS (n = 1), SJS/TEN overlap (n = 1), DRESS (n = 1), and GBFDE (n = 1). Six patients (18.2%) required hospitalization, four of whom were admitted to an intensive care or burn unit. An overview of patient demographics and clinical characteristics is provided in Table 1, and the distribution of clinical phenotypes is shown in Figure 2.
Figure 2 Distribution of clinical subtypes of delayed-type drug hypersensitivity reactions among the study patients. DHRs, drug hypersensitivity reactions; MPE, maculopapular exanthem; FDE, fixed drug eruption; SDRIFE, symmetrical drug-related intertriginous and flexural exanthema; ACD, allergic contact dermatitis; TEN, toxic epidermal necrolysis; SJS, Stevens–Johnson syndrome; DRESS, drug reaction with eosinophilia and systemic symptoms; GBFDE, generalized bullous fixed drug eruption.
Table 1 Demographic and clinical characteristics of patients with non-SCAR and SCAR reactions (n = 33).
| Characteristics | Non-SCAR (n = 26) | SCAR (n = 7) |
|---|---|---|
| Female sex, n (%) | 14 (53.8) | 5 (71.4) |
| Age, years, median (range) | 39 (19–70) | 47 (22–66) |
| Reaction type, n (%) | ||
| Non-SCAR | ||
| Maculopapuler exanthem | 15 (45.5) | |
| Fixed drug eruption | 8 (24.2) | |
| SDRIFE | 1 (3.0) | |
| Allergic contact dermatitis | 2 (6.1) | |
| SCAR | ||
| SJS/TEN (including overlap forms) | 5 (15.2) | |
| DRESS | 1 (3.0) | |
| GBFDE | 1 (3.0) | |
| Latency from drug exposure to symptom onset (days), median (range) | 5 (1–14) | 10 (5–42) |
| Treatment | ||
| Systemic corticosteroids, n (%) | 4 (15.3) | 7 (100.0) |
| IVIG treatment, n (%) | 0 (0.0) | 2 (28.6) |
| Patients hospitalized | 0 (0.0) | 6 (85.7) |
| Intensive care/burn unit required | 0 (0.0) | 4 (57.1) |
| Single suspected culprit drug, n (%)# | 16 (61.5) | 1 (14.3) |
| Multiple suspected drugs, n (%)# | 10 (38.5) | 6 (85.7) |
| Suspected culprit drug categories, n (%)* | ||
| Antimicrobials | 10 (25.6) | 13 (68.4) |
| NSAIDs (including paracetamol) | 14 (35.9) | 3 (15.8) |
| Cardiovascular agents | 5 (12.8) | 0 (0.0) |
| Radiocontrast media | 3 (7.6) | 0 (0.0) |
| Muscle relaxants | 2 (5.1) | 0 (0.0) |
| Others | 5 (12.8) | 3 (15.8) |
| Underwent patch/IDT testing | 9 (34.6) | 0 (0.0) |
| Positive skin test result, n (% of tested) | 4 (15.3) | 0 (0.0) |
Percentages are calculated within each group (Non-SCAR and SCAR) unless otherwise specified.
*Percentages were calculated based on the total number of suspected drugs, as some patients were exposed to more than one implicated agent.
#Multiplicity of suspected culprit drugs refers to the number of implicated agents per patient. Continuous variables are presented as median (range).
SCAR, severe cutaneous adverse reaction; SDRIFE, symmetrical drug-related intertriginous and flexural exanthema; SJS, Stevens–Johnson syndrome; TEN, toxic epidermal necrolysis; DRESS, drug reaction with eosinophilia and systemic symptoms; GBFDE, generalized bullous fixed drug eruption; IVIG, intravenous immunoglobulin; IDT, intradermal test.
Diagnostic work-up
Diagnostic testing was performed in 9 out of 33 patients (27.3%). Among these, four patients had positive skin test results confirming the suspected culprit drug, while five had negative results. Following negative patch test results, two patients (one with MPE and one with FDE) underwent diagnostic drug provocation testing (DPT). The DPT was negative in the MPE case, whereas it elicited a positive reaction to naproxen in the FDE case, confirming it as the causative drug.
In the remaining 24 patients (72.7%), diagnostic testing was not performed due to patient refusal (n = 6, 18.2%), an ongoing refractory period (n = 6, 18.2%), the acute phase of the reaction (n = 3, 9.1%), or lack of indication when a safe alternative drug was available (n = 9, 27.3%). No in vivo diagnostic testing was performed in SCAR patients because of safety concerns and limited clinical indication. Detailed characteristics of patients who underwent diagnostic testing are presented in Table 2.
Table 2 Characteristics and test results of patients who underwent diagnostic testing (n = 9).
| Case | Age/ Sex | Clinical reaction | Suspected culprit drug(s) | Diagnostic test(s) performed | Test result(s) |
|---|---|---|---|---|---|
| 1 | 50 F | MPE | Paracetamol Dexketoprofen | Paracetamol 5% PT# + DPT Dexketoprofen 1% PT# + DPT | Negative Negative |
| 2 | 67 F | MPE | RCM (iodinated contrast) | Iohexol (1/10 dilution), Delayed IDT | Negative |
| 3 | 25 F | MPE | RCM (gadolinium contrast) | Gadobutrol (1/10 dilution) Delayed IDT | Negative |
| 4 | 33 F | MPE | RCM (iodinated contrast) | Iohexol (1/10 dilution), Delayed IDT | Positive |
| 5 | 68 M | MPE | Colchicine AllopurinolDiclofenac | Colchicine 1% PT# Allopurinol PT#Diclofenac 2% PT# | PositiveNegative Negative |
| 6 | 67 F | MPE | Tizanidine ASAParacetamol | Tizanidine PT ASA 5% PT#Paracetamol 5% PT# | Negative NegativeNegative |
| 7 | 68 M | FDE | Naproxen Ranitidine Darifenasin Thiocolchicoside | Naproxen 10% PT*,# + DPT Ranitidine 30% PT*,# + DPT Darifenasin 30% PT*,# + DPT Thiocolchicoside 30% PT*,# + DPT | Positive Negative Negative Negative |
| 8 | 19 F | ACD | Asiaticoside(Centella asiatica extract) | Asiaticoside PT | Negative |
| 9 | 22 M | ACD | Nitrofurazone | Nitrofurazone PT | Positive |
Age in years. *, lesional and non-lesional testing; #, test preparation in petrolatum; F, female; M, male; MPE, maculopapular exanthem; FDE, fixed drug eruption; ACD, allergic contact dermatitis; RCM, radiocontrast media; ASA, acetylsalicylic acid; PT, patch test; DPT, drug provocation test; IDT, intradermal test.
Subgroup analyses
Non-SCAR groups
Among the 15 patients with MPE, a single suspected culprit drug was identified in nine cases (60%), while the remaining patients had exposure to multiple suspect medications. The median latency between drug exposure and symptom onset in MPE was 6 days (range 1–25). Eight MPE patients (53.3%) were females. All MPE cases followed a mild-to-moderate clinical course and resolved with drug withdrawal and symptomatic treatment; none required hospitalization. Patch testing was performed in six MPE patients and yielded positive results in two cases (33.3%), confirming the culprit drug (Table 2).
Eight patients were diagnosed with FDE. Lesions were localized and recurred at identical sites upon reexposure. A single culprit drug was identified in five patients, while three had multiple suspected agents. NSAIDs were the most frequently implicated drug class (75%), with naproxen suspected in four cases. Patch testing was performed in three FDE patients and confirmed drug causality in one case. Following negative patch test results, two patients (one with MPE and one with FDE) underwent cautious DPT. The MPE patient had a negative DPT, whereas the FDE patient had a positive challenge to naproxen, identifying it as the causative agent.
One patient was diagnosed with SDRIFE. This 31-year-old male developed pruritic, symmetric erythematous lesions approximately 3 days after dexketoprofen intake, without systemic involvement. The eruption resolved after drug discontinuation and treatment with topical corticosteroids and oral antihistamines. Paracetamol was tolerated as a safe alternative during follow-up.
Two patients were diagnosed with ACD. The suspected agents were Asiaticoside (Centella asiatica extract) and nitrofurazone, with patch testing confirming drug causality in one case (nitrofurazone) (Table 2).
In patients with non-SCAR reactions, a total of 39 suspected culprit drugs were identified, reflecting exposure to more than one implicated agent in several cases. NSAIDs were the most frequently suspected drug class (35.9%), including naproxen (n = 4), dexketoprofen (n = 3), paracetamol (n = 2), ibuprofen (n = 1), flurbiprofen (n = 1), meloxicam (n = 1), acetylsalicylic acid (n = 1), and diclofenac (n = 1). Antimicrobial agents accounted for 25.6% of suspected drugs and included beta-lactam antibiotics such as cefuroxime axetil (n = 2), amoxicillin–clavulanate (n = 1), and ampicillin–sulbactam (n = 1), as well as TMP–SMX (n = 2), terbinafine (n = 2), nitrofurazone (n = 1), and permethrin (n = 1).
Other implicated drug classes included cardiovascular agents (12.8%), such as ticagrelor (n = 1), metoprolol (n = 1), atorvastatin (n = 1), spironolactone (n = 1), and perindopril (n = 1); radiocontrast media (7.6%), including iohexol (n = 2) and gadobutrol (n = 1); and muscle relaxants (5.1%), namely thiocolchicoside (n = 1) and tizanidine (n = 1). Miscellaneous agents (12.8%) included hydroxychloroquine (n = 1), colchicine (n = 1), allopurinol (n = 1), famotidine (n = 1), and asiaticoside (C. asiatica extract) (n = 1).
SCAR groups
Seven patients (21.2% of the cohort) experienced SCARs, including three cases of TEN and one each of SJS, SJS/TEN overlap, DRESS, and GBFDE (Figure 2). The most frequently implicated drug class in SCARs was fluoroquinolone antibiotics (n = 4, 57%), followed by beta-lactam antibiotics (n = 2, 29%) and trimethoprim–sulfamethoxazole (TMP–SMX) (n = 2, 29%). Other suspected agents included metronidazole, dexketoprofen, naproxen, carbamazepine, and sulfasalazine.
All three TEN cases, the SJS/TEN overlap case, and the single SJS case required hospitalization, with four of these five patients managed in an intensive care or burn unit. The median SCORTEN score among patients with TEN or SJS/TEN overlap was 3 (range 2–4), corresponding to an estimated mortality risk of approximately 35–60%. All SCAR patients received systemic corticosteroid therapy (intravenous prednisolone) and comprehensive supportive care, including wound management and fluid and electrolyte replacement. Two TEN patients received intravenous immunoglobulin (IVIG) (IVIG; 1–2 g/kg/day for 3–5 days) in addition. The single SJS case, attributed to ceftriaxone and dirithromycin, followed a milder course and improved with systemic and topical corticosteroid therapy. No fatalities occurred in the study cohort. Detailed clinical characteristics, suspected culprit drugs, and management strategies are summarized in Table 3.
Table 3 Clinical details of severe cutaneous adverse reactions (n = 7).
| Case | Age/Sex | SCAR diagnosis | Suspected culprit drug(s) | Severity score | Hospitalization | Treatment |
|---|---|---|---|---|---|---|
| 1 | 51/M | SJS | Ceftriaxone Dirithromycin | Not assessed | Ward | IV corticosteroids supportive care |
| 2 | 66/F | SJS/TENoverlap | Ciprofloxacin MetronidazoleHyoscine-N-butylbromide | SCORTEN = 2 | ICU | IV corticosteroids supportive care |
| 3 | 54/F | TEN | CefpodoximeLevofloxacin | SCORTEN = 4 | ICU/Burn unit | IV corticosteroids, supportive care, IVIG |
| 4 | 29/M | TEN | Ciprofloxacin Metronidazole NSAID (unknown)Carbamazepine | SCORTEN = 2 | ICU/Burn unit | IV corticosteroids, supportive care, IVIG |
| 5 | 25/F | TEN | Amoxicillin–clavulanate Cefazolin | Not assessed | ICU/Burn unit | IV corticosteroids, supportive care |
| 6 | 47/F | DRESS | Sulfasalazine Dexketoprofen TMP–SMX | RegiSCAR5 (probable) | Ward | IV corticosteroids, topical corticosteroids, and supportive care |
| 7 | 22/F | GBFDE | Cefpodoxime Naproxen TMP–SMX | – | None | Oral corticosteroids, topical corticosteroids |
SCAR, severe cutaneous adverse reaction; M, male; F, female; SJS, Stevens–Johnson syndrome; TEN, toxic epidermal necrolysis; DRESS, drug reaction with eosinophilia and systemic symptoms; GBFDE, generalized bullous fixed drug eruption; SCORTEN, severity-of-illness score for TEN; RegiSCAR, European SCAR Consortium score; ICU, intensive care unit; IVIG, intravenous immunoglobulin; TMP–SMX, trimethoprim–sulfamethoxazole; IV, intravenous.
The DRESS case involved a 47-year-old female who developed generalized erythema, facial edema, and eosinophilia (RegiSCAR score = 5, indicating a probable diagnosis). The reaction was attributed to sulfasalazine and TMP–SMX, and the patient achieved complete recovery with systemic corticosteroids and topical therapy.
The GBFDE case was a 22-year-old male who presented with sharply demarcated bullous lesions recurring at previously affected sites after exposure to cefpodoxime, naproxen, and TMP–SMX. Clinical improvement was observed following withdrawal of the suspected drugs and treatment with oral and topical corticosteroids.
In accordance with international safety guidelines, no in vivo diagnostic testing (patch or intradermal testing) was performed in SCAR cases because of the risk of inducing a severe relapse. Causality assessment was therefore based on the temporal relationship between drug exposure and symptom onset, clinical judgment, and established drug–reaction associations.
Comparison with non-SCAR groups
Compared to non-SCAR patients, those with SCARs had significantly higher rates of hospitalization (85.7% vs 0%, p < 0.001) and a greater need for systemic corticosteroid therapy (100% vs 20%, p < 0.001). The median latency from drug exposure to symptom onset was longer in SCAR reactions (10 days, range: 5–42) than in non-SCAR reactions (5 days, range: 1–14).
Discussion
In this 5-year retrospective cohort, delayed-type DHRs exhibited a broad clinical spectrum ranging from mild exanthematous eruptions to SCARs. Beta-lactam antibiotics and NSAIDs were the predominant culprit groups, consistent with previous studies.28–32 These agents are the leading causes of benign exanthematous eruptions, while polypharmacy, present in nearly half of our patients, complicates causality assessment, particularly in severe cases. This observation highlights a recurrent challenge in clinical pharmacovigilance, where multiple concomitant drugs can obscure true attribution.
MPE and FDE emerged as the predominant non-SCAR phenotypes in our cohort, a pattern consistent with previous studies reporting these entities as the most common manifestations of delayed-type DHRs.28–31 The prominent role of antimicrobial agents, particularly beta-lactam antibiotics and TMP–SMX, also aligns with findings from the cohorts in Iran and Mexico, underscoring the widespread use of these agents and their potential to induce delayed DHRs.28,33 NSAIDs constituted a major group of suspected triggers in our cohort, consistent with previous studies identifying this class as a common cause of delayed-type DHRs. The frequent implication of NSAIDs supports existing evidence that these agents are among the leading contributors to maculopapular and other non-immediate cutaneous eruptions, reflecting both their widespread use and established immunogenic potential.28,32,34,35 Overall, our findings are in line with global data reporting NSAIDs as the second most common drug group implicated in delayed-type DHRs.28,32
Less frequently observed phenotypes in our cohort included SDRIFE and ACD, both representing localized, T-cell-mediated delayed hypersensitivity reactions.5,8,9 SDRIFE typically presents with symmetric, well-demarcated erythema in flexural or intertriginous areas following systemic drug exposure, without mucosal or internal organ involvement.8,9 In our series, one patient developed SDRIFE 3 days after dexketoprofen intake, which resolved rapidly after drug withdrawal and topical corticosteroid treatment. Although beta-lactam antibiotics, particularly amoxicillin, are the most common triggers, NSAIDs have also been implicated, as illustrated by our case.9 Two patients developed ACD due to topical preparations: one from a C. asiatica-containing herbal cream and another from nitrofurazone ointment. Both exhibited localized eczematous lesions confined to application sites. Patch testing confirmed nitrofurazone hypersensitivity, while the C. asiatica case was diagnosed clinically. These findings highlight that both topical and systemic drugs can induce localized delayed-type reactions through similar immune mechanisms. Although typically mild and self-limiting, recognizing such patterns is essential to avoid reexposure and to guide the selection of safe alternative therapies.
Approximately one-fifth of patients in our cohort experienced SCARs, including SJS, TEN, DRESS, and GBFDE. Consistent with global epidemiological data, antibiotics emerged as the most frequently implicated drug group, followed by NSAIDs and antiepileptic agents, in line with the findings from international SCAR registries.12,36,37 Sulfasalazine and TMP–SMX, both well-established inducers of DRESS, were each implicated in one severe case.38 All patients with SCARs required active systemic treatment and a substantial requirement for hospitalization or intensive care support, reflecting the severity of these reactions. Despite a median SCORTEN score of 3, no fatalities were observed, which may be attributable to early recognition and adherence to evidence-based management protocols. Although high-risk drugs traditionally associated with SCARs, such as aromatic anticonvulsants and allopurinol, were infrequently identified in our cohort—likely reflecting local prescribing patterns—multicenter studies consistently identified these agents as primary inducers of SJS/TEN and DRESS.12 Consequently, pharmacogenetic screening remains essential in populations where these drugs are commonly prescribed.29
Compared to non-severe reactions, SCAR patients exhibited significantly greater morbidity, requiring systemic therapy and prolonged hospitalization. While MPE and FDE resolved after culprit withdrawal and topical corticosteroids, SCARs necessitated multidisciplinary management, high-dose corticosteroids, and, in some cases, IVIG. These findings underscore the value of early diagnosis and guideline-driven therapy in mitigating mortality.
In vivo diagnostic testing contributed substantially to confirmation in non-severe reactions but remained limited.39 Nine patients (27.3%) underwent patch or delayed IDT, four of whom were positive, and these figures are in line with published positivity ranges for non-immediate reactions.4 Patch tests are generally highly specific but only moderately sensitive, while delayed IDT can improve sensitivity at the expense of a small risk. Negative results do not exclude causality, and diagnostic yield varies by phenotype, tending to be higher in AGEP and DRESS and lower in SJS/TEN.4,39 Current international guidance therefore advocates a structured, stepwise diagnostic approach, beginning with meticulous clinical history and timing analysis, followed by patch or delayed intradermal testing when safe and appropriate, while drug provocation testing is contraindicated in SCARs due to the risk of severe relapse.4,17,23
In SCAR, where drug provocation is contraindicated, identification of the culprit relies on expert clinical judgement and temporal relationships. Polypharmacy is a major obstacle: many SCAR patients receive several drugs concurrently (e.g., combinations including antibiotics, NSAIDs, or anticonvulsants), which increases both risk and diagnostic uncertainty.29 This underscores the need for rational prescribing and medication stewardship.
Several limitations of this study warrant consideration. The relatively small sample size and single-center, retrospective design restrict the generalizability of the findings and may have led to the underrepresentation of certain phenotypes or culprit drugs. For instance, no AGEP cases were observed, and only one allopurinol-induced reaction was recorded, likely reflecting local prescribing patterns. Additionally, maculopapular exanthema cases were proportionally fewer in our cohort. This may be explained by the fact that our tertiary centre mainly receives referrals of more severe cases, leading to a relative underrepresentation of mild forms. Furthermore, reliance on medical record documentation introduces a risk of information bias. Despite careful data verification, details such as precise latency periods or complete concomitant medication lists were occasionally incomplete. Another important limitation is the lack of a gold-standard diagnostic tool for most delayed-type DHRs, particularly SCARs. In our cohort, causality assessment primarily relied on clinical judgment and established diagnostic criteria, as reexposure challenges were ethically unsafe and in vitro assays (e.g., lymphocyte transformation test or ELISpot) were unavailable. Consequently, some culprit identifications remain presumptive, an inherent limitation shared by most real-world allergy studies. This uncertainty may contribute to unnecessary drug avoidance and highlights the continuing need for validated, accessible confirmatory methods.
Despite these limitations, this study provides valuable real-world evidence on both severe and non-severe delayed-type DHRs in adults. By combining clinical phenotyping with confirmatory testing (patch testing, delayed IDT, and DPT) in a subset of patients, we contribute to the limited body of data on diagnostic yield in non-immediate drug allergies. These findings demonstrate the practical value of these diagnostic tools when appropriately applied in clinical practice. Importantly, our results underscore the role of polypharmacy as a major confounder in both the development and diagnosis of DHRs. Multiple concomitant medications were common, particularly among SCAR cases, and frequently obscured accurate drug attribution. This observation reinforces the importance of rational prescribing and improved medication stewardship to minimize unnecessary exposure and diagnostic ambiguity.
In summary, antibiotics, especially beta-lactam antibiotics, and NSAIDs were the most frequent culprits of delayed-type DHRs, while SCARs represented about one-fifth of cases and are of particular clinical importance due to their potentially high mortality and severe clinical course. Polypharmacy emerged as a significant confounder, both in the development and diagnosis of reactions. A structured, stepwise diagnostic approach combining thorough history, selective testing, and multidisciplinary evaluation remains critical. Future research should prioritize the development of reliable in vitro assays and broader pharmacogenetic screening for high-risk drugs. Continued regional surveillance is essential to refine diagnostic algorithms and promote personalized, evidence-based management of DHRs.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that ChatGPT (OpenAI) was used solely for language editing and grammar improvement. The scientific content, interpretation, and conclusions of the manuscript were developed entirely by the authors. All references have been manually verified for accuracy and relevance.
Author Contributions
All authors contributed equally to this article.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
None.
REFERENCES
1 Chu MT, Chang WC, Pao SC, Hung SI. Delayed drug hypersensitivity reactions: Molecular recognition, genetic susceptibility, and immune mediators. Biomedicines. 2023;11(1):177. 10.3390/biomedicines11010177
2 Lehloenya RJ, Peter JG, Copaescu A, Trubiano JA, Phillips EJ. Delabeling delayed drug hypersensitivity: How far can you safely go? J Allergy Clin Immunol Pract. 2020;8(9):2878–95.e6. 10.1016/j.jaip.2020.07.005. Erratum In: J Allergy Clin Immunol Pract. 2021;9(1):603. 10.1016/j.jaip.2020.10.024. Erratum in: J Allergy Clin Immunol Pract. 2022;10(2):651. 10.1016/j.jaip.2021.12.002
3 Gell PGH, Coombs RRA. Clinical aspects of immunology. Oxford: Blackwell Science; 1963.
4 Copaescu A, Gibson A, Li Y, Trubiano JA, Phillips EJ. An updated review of the diagnostic methods in delayed drug hypersensitivity. Front Pharmacol. 2021;11:573573. 10.3389/fphar.2020.573573
5 Tramontana M, Hansel K, Bianchi L, Sensini C, Malatesta N, Stingeni L. Advancing the understanding of allergic contact dermatitis: From pathophysiology to novel therapeutic approaches. Front Med (Lausanne). 2023;10:1184289. 10.3389/fmed.2023.1184289
6 Tanno LK, Calderon MA, Smith HE, Sanchez-Borges M, Sheikh A, Demoly P; Joint Allergy Academies. Dissemination of definitions and concepts of allergic and hypersensitivity conditions. World Allergy Organ J. 2016;9:24. 10.1186/s40413-016-0115-2
7 Riedl MA, Casillas AM. Adverse drug reactions: Types and treatment options. Am Fam Physician. 2003;68(9):1781–90.
8 Schuler AM, Smith EH, Chaudet KM, Bresler SC, Gudjonsson JE, Kroshinsky D, et al. Symmetric drug-related intertriginous and flexural exanthema: Clinicopathologic study of 19 cases and review of literature. J Cutan Pathol. 2021;48(12):1471–9. 10.1111/cup.14090
9 Durmaz MSB. Simetrik, ilaç ilişkili intertriginöz ve fleksural ekzantem. Turkiye Klinikleri Immunol Allergy-Special Topics. 2025;18(1):54–8.
10 Barbaud A, Goncalo M, Mockenhaupt M, Copaescu A, Phillips EJ. Delayed skin testing for systemic medications: Helpful or not? J Allergy Clin Immunol Pract. 2024;12(9):2268–77. 10.1016/j.jaip.2024.06.047
11 Lee EY, Knox C, Phillips EJ. Worldwide prevalence of antibiotic-associated Stevens–Johnson syndrome and toxic epidermal necrolysis: A systematic review and meta-analysis. JAMA Dermatol. 2023;159(4):384–92. 10.1001/jamadermatol.2022.6378
12 Tempark T, John S, Rerknimitr P, Satapornpong P, Sukasem C. Drug-induced severe cutaneous adverse reactions: Insights into clinical presentation, immunopathogenesis, diagnostic methods, treatment, and pharmacogenomics. Front Pharmacol. 2022;13:832048. 10.3389/fphar.2022.832048
13 De A, Rajagopalan M, Sarda A, Das S, Biswas P. Drug reaction with eosinophilia and systemic symptoms: An update and review of recent literature. Indian J Dermatol. 2018;63(1): 30–40. 10.4103/ijd.IJD_582_17
14 Mockenhaupt M. Introduction: Classification, terminology, epidemiology, and etiology of cutaneous adverse drug reactions. In: Shear NH, Dodiuk-Gad RP, editors. Advances in diagnosis and management of cutaneous adverse drug reactions: Current and future trends. Cham: Springer; 2019. pp. 3–20.
15 Demoly P, Adkinson NF, Brockow K, Castells M, Chiriac AM, Greenberger PA, et al. International consensus on drug allergy. Allergy. 2014;69(4):420–37. 10.1111/all.12350
16 Khan DA, Banerji A, Blumenthal KG, Phillips EJ, Solensky R, White AA, et al. Drug allergy: A 2022 practice parameter update. J Allergy Clin Immunol. 2022;150(6):1333–93. 10.1016/j.jaci.2022.08.028
17 Rive CM, Bourke J, Phillips EJ. Testing for drug hypersensitivity syndromes. Clin Biochem Rev. 2013;34(1):15–38.
18 Barbaud A, Collet E, Milpied B, Assier H, Staumont D, Avenel-Audran M, et al. A multicentre study to determine the value and safety of drug patch tests for the three main classes of severe cutaneous adverse drug reactions. Br J Dermatol. 2013;168(3):555–62. 10.1111/bjd.12125
19 Kardaun SH, Sidoroff A, Valeyrie-Allanore L, Halevy S, Davidovici BB, Mockenhaupt M, et al. Variability in the clinical pattern of cutaneous side-effects of drugs with systemic symptoms: Does a DRESS syndrome really exist? Br J Dermatol. 2007;156(3):609–11. 10.1111/j.1365-2133.2006.07704.x
20 Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L, Roujeau JC. Clinical classification of cases of toxic epidermal necrolysis, Stevens–Johnson syndrome, and erythema multiforme. Arch Dermatol. 1993;129(1):92–6.
21 Sidoroff A, Halevy S, Bavinck JN, Vaillant L, Roujeau JC. Acute generalized exanthematous pustulosis (AGEP)—A clinical reaction pattern. J Cutan Pathol. 2001;28(3):113–9. 10.1034/j.1600-0560.2001.028003113.x
22 Bastuji-Garin S, Fouchard N, Bertocchi M, Roujeau JC, Revuz J, Wolkenstein P. SCORTEN: A severity-of-illness score for toxic epidermal necrolysis. J Invest Dermatol. 2000;115(2):149–53. 10.1046/j.1523-1747.2000.00061.x
23 Brockow K, Garvey LH, Aberer W, Atanaskovic-Markovic M, Barbaud A, Bilo MB, et al. Skin test concentrations for systemically administered drugs: An ENDA/EAACI Drug Allergy Interest Group position paper. Allergy. 2013;68(6):702–12. 10.1111/all.12142
24 Barbaud A, Gonçalo M, Bruynzeel D, Bircher A; European Society of Contact Dermatitis. Guidelines for performing skin tests with drugs in the investigation of cutaneous adverse drug reactions. Contact Dermatitis. 2001;45(6):321–8. 10.1034/j.1600-0536.2001.450601.x
25 Johansen JD, Aalto-Korte K, Agner T, Andersen KE, Bircher A, Bruze M, et al. European Society of Contact Dermatitis guideline for diagnostic patch testing: Recommendations on best practice. Contact Dermatitis. 2015;73(4):195–221. 10.1111/cod.12432
26 Fonacier L, Bernstein DI, Pacheco K, Holness DL, Blessing-Moore J, Khan D, et al. Contact dermatitis: A practice parameter update 2015. J Allergy Clin Immunol Pract. 2015;3(3 Suppl):S1–39. 10.1016/j.jaip.2015.02.009
27 Aberer W, Bircher A, Romano A, Blanca M, Campi P, Fernandez J, et al. Drug provocation testing in the diagnosis of drug hypersensitivity reactions: General considerations. Allergy. 2003;58(9):854–63. 10.1034/j.1398-9995.2003.00279.x
28 Farshchian M, Ansar A, Zamanian A, Rahmatpour-Rokni G, Kimyai-Asadi A, Farshchian M. Drug-induced skin reactions: A 2-year study. Clin Cosmet Investig Dermatol. 2015;8:53–56. 10.2147/CCID.S75849
29 Peter JG, Lehloenya R, Dlamini S, Risma K, White KD, Konvinse KC, Phillips EJ. Severe delayed cutaneous and systemic reactions to drugs: A global perspective on the science and art of current practice. J Allergy Clin Immunol Pract. 2017;5(3):547–63. 10.1016/j.jaip.2017.01.025
30 Huang HY, Luo XQ, Chan LS, Cao ZH, Sun XF, Xu JH. Cutaneous adverse drug reactions in a hospital-based Chinese population. Clin Exp Dermatol. 2011;36(2):135–41. 10.1111/j.1365-2230.2010.03922.x
31 Mockenhaupt M. Epidemiology of cutaneous adverse drug reactions. Chem Immunol Allergy. 2012;97:1–17. 10.1159/000335612
32 Al-Ahmad M, Edin J, Musa F, Rodriguez-Bouza T. Drug allergy profile from a national drug allergy registry. Front Pharmacol. 2021;11:555666. 10.3389/fphar.2020.555666
33 Hernández-Salazar A, Rosales SP, Rangel-Frausto S, Criollo E, Archer-Dubon C, Orozco-Topete R. Epidemiology of adverse cutaneous drug reactions: A prospective study in hospitalized patients. Arch Med Res. 2006;37(7):899-902. 10.1016/j.arcmed.2006.03.010
34 Souissi A, Fenniche S, Benmously R, Ben Jannet S, Marrak H, Mokhtar I. Study of the cutaneous drug reactions in a teaching hospital in Tunis. Tunis Med. 2007;85(12):1011–5.
35 Patel RM, Marfatia YS. Clinical study of cutaneous drug eruptions in 200 patients. Indian J Dermatol Venereol Leprol. 2008;74(4):430. 10.4103/0378-6323.42883
36 Guzman AI, Paliza AC. Epidemiology of severe cutaneous adverse drug reactions in a university hospital: A five-year review. J Med Univ Santo Tomas. 2018;2(1):171–84. 10.35460/2546-1621.2017-0031
37 Badar Uddin U, Zeenat Un N. Cutaneous adverse drug reactions to antibiotics: How much is the extent of the problem? JOJ Dermatol Cosmet. 2023;5(4):555666. 10.19080/JOJDC.2023.05.555666
38 Stirton H, Shear NH, Dodiuk-Gad RP. Drug reaction with eosinophilia and systemic symptoms (DReSS)/drug-induced hypersensitivity syndrome (DiHS)—Readdressing the DReSS. Biomedicines. 2022;10(5):999. 10.3390/biomedicines10050999
39 Wolkenstein P, Chosidow O, Fléchet ML, Robbiola O, Paul M, Dumé L, et al. Patch testing in severe cutaneous adverse drug reactions, including Stevens–Johnson syndrome and toxic epidermal necrolysis. Contact Dermatitis. 1996;35(4):234–6. 10.1111/j.1600-0536.1996.tb02364.x