
Download

ORIGINAL ARTICLE
Symptom and quality of life assessment during season undergoing pollen immunotherapy: single center study
Hatice Irmak Çelika*, Ragıp Derea, Çağrı Torun Özela, Ahmet Selmanoğlua, Zeynep Şengül Emeksizb, Emine Dibek Mısırlıoğlub
aDepartment of Pediatric Allergy and Immunology, Ankara Bilkent City Hospital, Ankara, Turkey
bDepartment of Pediatric Allergy and Immunology, Health Sciences University, Ankara Bilkent City Hospital, Ankara, Turkey
This article was presented as a poster at “31st National Congress of Allergy and Clinical Immunology” held in Antalya, Turkey, from 26–30 November, 2025
Abstract
Background: Allergic rhinitis (AR) is an IgE-mediated inflammatory condition of the nasal mucosa. Allergen immunotherapy (AIT) is the only treatment that can modify disease progression and provide long-term symptom control. This study evaluated symptom burden and health-related quality of life (HRQoL) during the pollen season in pediatric patients treated with subcutaneous pollen immunotherapy (SCIT).
Material and Methods: This prospective, cross-sectional study included children aged 6–18 years who received ≥12 months of AIT between 2014 and 2022. All had isolated pollen allergy and were treated with SCIT. Symptom control was assessed using the Total Nasal Symptom Score (TNSS) and Visual Analog Scale (VAS), while HRQoL was measured using PRQLQ or RQLQ depending on age. Patients were grouped by treatment duration: <36 months and ≥36 months.
Results: Forty-seven patients completed questionnaires at least two pollen seasons after their final SCIT dose. Compared with the <36-month group, patients treated for ≥36 months showed significantly lower nasal and ocular symptoms (P < 0.001). Mean TNSS scores were lower (5.42 vs. 9.57, P = 0.018), and more patients had mild symptoms (60.6% vs. 21.4%, P = 0.003). Good symptom control (VAS < 2) was also more frequent (36.4% vs. 14.3%, P = 0.022). HRQoL scores (PRQLQ/RQLQ) were significantly better in the ≥36-month group, particularly in social and school functioning.
Conclusion: SCIT duration ≥36 months is associated with improved symptom control and HRQoL during the pollen season, supporting guideline recommendations of at least 3 years of AIT in pediatric AR.
Key words: allergic rhinitis, quality of life, subcutaneous pollen immunotherapy, Total Nasal Symptom Score, Visual Analog Scale
*Corresponding author: Hatice Irmak Çelik, Department of Pediatric Allergy and Immunology, Ankara Bilkent City Hospital, Universiteler 1604. Cad. No: 9, 06800, Ankara, Turkey. Email address: [email protected]
Received 20 October 2025; Accepted 5 March 2026; Available online 1 July 2026
Copyright: Çelik HI, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Key Messages
-
Subcutaneous pollen immunotherapy administered for ≥36 months provides significantly better symptom control and quality of life in pediatric allergic rhinitis.
-
Our findings reinforce guideline recommendations advocating at least 3 years of continuous AIT for sustained clinical benefit.
Introduction
Allergic rhinitis (AR) is an inflammatory disorder of the nasal mucosa triggered by an immunoglobulin E (IgE)-mediated hypersensitivity reaction in sensitized individuals. Upon allergen exposure, a Th2-driven immune response promotes IgE production, and subsequent mast cell degranulation initiates inflammation.1 AR is highly prevalent, affecting approximately 2–25% of children and 1–40% of adults worldwide. Its hallmark symptoms include nasal discharge, sneezing, nasal congestion, and nasal pruritus; ocular manifestations such as itching, redness, and tearing are also common.2 AR may be a risk factor for the development of asthma and may also predispose to rhinitis-associated comorbidities (e.g., allergic conjunctivitis, otitis media, adenoid hypertrophy),3 highlighting the need for long-term disease control strategies.4
Current AR management incorporates allergen avoidance, pharmacotherapy, allergen immunotherapy (AIT), and patient education. For patients with persistent symptoms who do not respond adequately to medication, AIT remains the only etiologic treatment available.4. AIT modulates the immune response by enhancing regulatory T-cell activity, suppressing IgE production, promoting protective IgG4 antibody production, and reducing mast cell sensitivity, thereby alleviating symptoms and improving quality of life.1 AIT can be administered as sublingual immunotherapy (SLIT) or subcutaneous immunotherapy (SCIT). International guidelines, including those from the European Academy of Allergy and Clinical Immunology (EAACI) and U.S. practice parameters, recommend a minimum of 3 years of AIT to achieve long-term clinical efficacy.1,5,6
Although AR is not life-threatening, it significantly impairs school performance, psychological well-being, and overall quality of life, representing a substantial socioeconomic burden on patients and society.7 In this study, we sought to evaluate the clinical features and health-related quality of life (HRQoL) of pediatric patients during the pollen season after completing SCIT, with particular focus on the relationship between treatment duration and clinical benefit.
Methods
Study design
This prospective, cross-sectional study was conducted at the Department of Pediatric Allergy and Immunology at a City Hospital. Eligible participants were children aged 6–18 years who had received ≥12 months of AIT at the Research and Training Hospital between 2014 and 2022. All patients had isolated pollen atopy and were receiving subcutaneous pollen immunotherapy (SCIT). All patients received SCIT following a conventional build-up protocol with weekly dose escalation, followed by monthly maintenance injections.
Children outside the specified age range, those unwilling to participate, or those who submitted incomplete questionnaires were excluded. Written informed consent was obtained from all participants and/or their legal guardians in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the institutional ethics committee (Approval No: TABED 2-24-86).
Symptom severity and HRQoL were evaluated during the pollen season occurring at least two seasons after the final SCIT dose. Data were collected in accordance with institutional ethical guidelines using online questionnaires and hospital electronic medical records. All participants completed a validated assessment form that incorporated the following clinical instruments: Total Nasal Symptom Score (TNSS), Visual Analog Scale (VAS), Pediatric Rhinoconjunctivitis Quality of Life Questionnaire (PRQLQ), and the adult Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ).
Data collection tools
The study questionnaire incorporated the following validated instruments:
-
Total Nasal Symptom Score (TNSS) – Daily Symptom Score: TNSS evaluates nasal symptoms (congestion, rhinorrhea, nasal itching, sneezing) and ocular symptoms (itching/redness, tearing), each scored on a 4-point scale from 0 (no symptoms) to 3 (severe, intolerable symptoms). Scores across categories are summed to yield a total score ranging from 0 to 18, categorized as mild (0–6), moderate (7–12), or severe (13–18) symptom burden.8
-
Visual Analog Scale (VAS): Symptom severity for nasal congestion, rhinorrhea, nasal itching, and sneezing was self-reported by patients on a 10-cm Likert-type scale (0 = no symptoms, 10 = worst possible symptoms). Participants marked the point that best represented their overall discomfort during the preceding week, ranging from “not bothersome at all” to “extremely bothersome.” Symptom control was classified as uncontrolled (VAS >5), partially controlled (VAS 2–5), or well controlled (VAS <2).9
-
Pediatric Rhinoconjunctivitis Quality of Life Questionnaire (PRQLQ): The PRQLQ, adapted from the Pediatric Quality of Life Inventory (PedsQL™ 4.0), 10 assesses HRQoL in children aged 6–18 years. It consists of four domains—physical functioning (8 items), emotional functioning (5 items), social functioning (5 items), and school functioning (5 items)—with a total of 23 items. Items are scored on a 5-point Likert scale and reverse-coded to a 0–100 scale, where higher scores indicate better HRQoL. For analysis, lower raw scores reflect a better quality of life. PRQLQ has been validated in Turkish populations,11 and although no standard cut-off exists, scores below the median were classified as “lower HRQoL” in this study.
-
Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ): For participants aged 18–23 years, HRQoL was assessed using the RQLQ, which evaluates seven domains: activities, sleep, practical problems, nasal symptoms, eye symptoms, non-nasal/ocular symptoms, and emotional impact. The 28 items are scored from 0 (“not troubled at all”) to 6 (“extremely troubled”), with lower scores indicating better quality of life. The RQLQ has also been validated in Turkish populations,12 and as with the PRQLQ, scores below the median were considered indicative of lower HRQoL.
Clinical data collection
Skin prick testing for pollen allergens—including Secale, rye grass (Lolium), Phleum pratense, Avena sativa (oat grass), wheat, Bermuda grass, Plantago, Cynodon dactylon, Kentucky bluegrass, Festuca pratensis, velvet grass, and orchard grass—was performed using commercial kits (Lofarma®, Milan, Italy). Histamine hydrochloride served as the positive control and 0.9% sodium chloride as the negative control. Results were assessed 15–20 minutes after application, and a wheal diameter ≥3 mm larger than the negative control was considered positive.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). The Kolmogorov–Smirnov test was used to assess the distribution of continuous variables. Normally distributed variables were expressed as mean ± standard deviation (SD), while non-normally distributed data were presented as median (25th–75th percentile). Categorical variables were expressed as counts and percentages.
Between-group comparisons were performed using the independent samples t-test for normally distributed continuous variables and the Mann–Whitney U test for non-normally distributed variables. Within-group comparisons of paired categorical variables (pre- vs. post-treatment) were analyzed using McNemar’s test. Between-group comparisons of categorical variables were conducted using Pearson’s chi-square test, with Fisher’s exact test applied when the expected cell count was <5.
TNSS symptom severity categories (mild, moderate, severe) were compared using the chi-square test. VAS scores were similarly categorized as well-controlled (VAS <2), partially controlled (VAS 2–5), or uncontrolled (VAS >5) and compared between groups.
PRQLQ and RQLQ scores—both total and domain-specific—were compared using either the independent-samples t-test or the Mann–Whitney U test, depending on the data distribution. A p-value of <0.05 was considered statistically significant. Findings were presented in tables and figures where appropriate.
Results
A total of 99 pediatric patients who had received SCIT were screened. Of these, 43 could not be contacted due to outdated contact information, 7 declined participation, and 2 had received SCIT for <12 months; these patients were excluded. The final study cohort comprised 47 patients, of whom 53.2% (25/47) were male. The mean age at symptom onset was 10.4 ± 2.0 years, and the mean age at diagnosis was 11.0 ± 1.3 years. The mean duration of SCIT was 45.3 ± 11.9 months (range: 21–61 months).
Patients were stratified according to SCIT duration: ≥36 months (n=33) and <36 months (n=14). Demographic characteristics and laboratory findings at diagnosis and during follow-up, stratified by treatment duration, are summarized in Table 1.
Table 1 Demographic characteristics and laboratory findings by SCIT duration.
| SCIT <36 mo (n = 14) | SCIT ≥36 mo (n = 33) | Total (n = 47) | P value | |
|---|---|---|---|---|
| Demographics | ||||
| Male sex, n (%) | 8 (57.1%) | 17 (51.5%) | 25 (53.2%) | 0.724 |
| Mean age at symptom onset, y (±SD) | 11.6 ± 3.3 | 9.9 ± 2.8 | 10.4 ± 2.0 | 0.093 |
| Mean age at diagnosis, y (±SD) | 12.6 ± 3.1 | 11.8 ± 2.6 | 11.0 ± 1.3 | 0.375 |
| Baseline laboratory values | ||||
| Total IgE, median (IQR), IU/mL | 386 (141-725) | 255 (145-410) | 297 (145-493) | 0.370 |
| Eosinophil count, median (IQR), cells/μL | 375 (280-575) | 250 (140-550) | 315 (200-550) | 0.108 |
| Follow-up laboratory values | ||||
| Total IgE, median (IQR), IU/mL | 296 (85-552) | 245 (131-305) | 280 (96-325) | 0.553 |
| Eosinophil count, median (IQR), cells/μL | 350 (200-460) | 210 (130-330) | 240 (130-350) | 0.109 |
1Independent samples t-test; 2Mann-Whitney U test.
SCIT: subcutaneous immunotherapy; mo: months; n: number; y: years; SD: standard deviation; IgE: immunoglobulin E; IQR: interquartile range.
When comparing pre- and post-treatment symptoms, patients in the <36-month group demonstrated significant reductions in sneezing, ocular itching, and ocular redness after SCIT (P = 0.025, P = 0.025, and P = 0.046, respectively), while other symptom changes were not statistically significant. In the ≥36-month SCIT group, all assessed nasal and ocular symptoms showed significant reductions following treatment compared with pre-treatment values (P < 0.05 for all comparisons; Figure 1).
Figure 1 Changes in nasal and ocular symptoms before and after SCIT in patients treated for <36 months and ≥36 months. Percentages represent the proportion of patients reporting each symptom.
According to the TNSS results obtained at the end of treatment, the mean symptom score for all patients was 6.66 ± 4.59. Patients in the <36-month SCIT group had significantly higher mean TNSS scores compared with those in the ≥36-month group (9.57 ± 5.52 vs. 5.42 ± 3.55, P = 0.018). When categorized by symptom severity, a significantly higher proportion of patients in the ≥36-month group fell into the mild symptom category compared with the <36-month group (60.6% vs. 21.4%, P = 0.003). Conversely, severe symptoms were markedly more frequent in the <36-month group (35.7% vs. 3.0%). Detailed comparisons are presented in Table 2.
Table 2 Comparison of TNSS results between SCIT duration groups.
| TNSS Category | SCIT <36 mo (n = 14) | SCIT ≥36 mo (n = 33) | Total (n = 47) | P value |
|---|---|---|---|---|
| Mild (0–6) | 21.4% (3/14) | 60.6% (20/33) | 48.9% (23/47) | |
| Moderate (7–12) | 42.9% (6/14) | 36.4% (12/33) | 38.3% (18/47) | 0.003* |
| Severe (13–18) | 35.7% (5/14) | 3.0% (1/33) | 12.8% (6/47) | |
| Mean TNSS (out of 18) | 9.57 ± 5.52 | 5.42 ± 3.55 | 6.66 ± 4.59 | 0.018** |
*Pearson’s chi-square test; **Independent samples t-test.
TNSS: total nasal symptom score; SCIT: subcutaneous immunotherapy; mo: months; n: number.
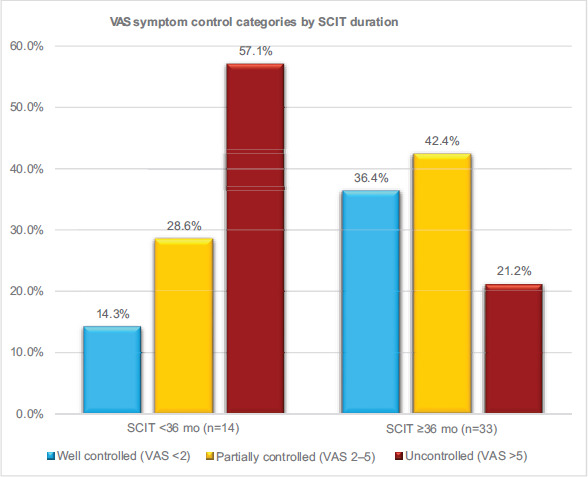
Symptom control levels, as assessed by the VAS, differed significantly according to SCIT duration. In the ≥36-month group, the proportion of well-controlled patients (VAS <2) was significantly higher, while the proportion of uncontrolled patients (VAS >5) was significantly lower compared with the <36-month group (P = 0.022; Figure 2).
Figure 2 Distribution of symptom control levels based on VAS categories according to SCIT duration.
A total of 14 patients aged 12–18 years completed the PRQLQ. Of these, 6 (42.9%) were in the <36-month SCIT group and 8 (57.1%) were in the ≥36-month group. Comparison of PRQLQ domain and total scores between the two groups revealed that patients with ≥36 months of SCIT had significantly better quality of life, particularly in the domains of social functioning, school functioning, and overall PRQLQ scores (P < 0.05 for each; Table 3).
Table 3 PRQLQ domain and total scores by SCIT duration and PRQLQ scores reversed to percentages for HRQoL interpretation.
| Domain, Mean ± SD | SCIT <36 mo (n=6) | SCIT ≥36 mo (n=8) | Total (n=14) | P-value |
|---|---|---|---|---|
| Physical functioning | 2.3 ± 2.1 | 1.1 ± 1.5 | 1.6 ± 1.8 | 0.222 |
| Emotional functioning | 2.8 ± 1.5 | 1.3 ± 1.4 | 1.9 ± 1.6 | 0.062 |
| Social functioning | 4.7 ± 3.1 | 0 ± 0 | 2.0 ± 3.1 | <0.001* |
| School functioning | 10 ± 4.9 | 4.5 ± 3.8 | 6.9 ± 5.0 | 0.035* |
| Total prqlq score | 19.8 ± 9.8 | 6.9 ± 6.2 | 12.4 ± 10.1 | 0.010* |
| Domain, quality of life% | ||||
| Physical functioning | 92.81% | 96.56% | 95.00% | 0.222 |
| Emotional functioning | 86.00% | 93.50% | 90.50% | 0.062 |
| Social functioning | 76.50% | 100.00% | 90.00% | <0.001* |
| School functioning | 50.00% | 77.50% | 65.50% | 0.035* |
| Total prqlq score | 78.48% | 92.50% | 86.52% | 0.010* |
*Student’s t-test. Lower scores and higher percentanges indicate better quality of life.
PRQLQ, pediatric rhinoconjunctivitis quality of life questionnaire; HRQoL, health-related quality of life; SCIT, subcutaneous immunotherapy; mo, months; n, number; SD, standard deviation.
A total of 33 patients aged 18–23 years completed the RQLQ. The mean total RQLQ score was significantly lower in the ≥36-month SCIT group compared with the <36-month group (20.12 ± 21.45 vs. 43.86 ± 31.51, p=0.025), indicating better quality of life in the longer treatment group. Domain-specific results are summarized in Table 4.
Table 4 RQLQ domain and total scores by SCIT duration.
| RQLQ domain, mean ± SD | SCIT <36 mo (n = 7) | SCIT ≥36 mo (n = 26) | Total (n = 33) | P value |
|---|---|---|---|---|
| Activities | 2.00 ± 1.77 | 1.24 ± 1.42 | 1.44 ± 1.52 | 0.263 |
| Sleep | 1.76 ± 1.60 | 0.88 ± 1.05 | 1.12 ± 1.25 | 0.111 |
| Practical problems | 2.57 ± 2.31 | 1.86 ± 1.54 | 2.05 ± 1.76 | 0.372 |
| Nasal symptoms | 2.25 ± 1.43 | 1.82 ± 1.35 | 1.94 ± 1.36 | 0.485 |
| Eye symptoms | 1.39 ± 1.34 | 0.58 ± 0.76 | 0.80 ± 0.99 | 0.061 |
| Non-nasal/ocular symptoms | 0.76 ± 0.68 | 0.38 ± 0.45 | 0.48 ± 0.54 | 0.111 |
| Emotional impact | 1.25 ± 1.21 | 0.55 ± 0.81 | 0.74 ± 0.96 | 0.101 |
| Total RQLQ score | 43.86 ± 31.51 | 20.12 ± 21.45 | 25.15 ± 25.36 | 0.025* |
*Student’s t-test. Lower scores indicate better quality of life.
RQLQ, rhinoconjunctivitis quality of life questionnaire; SCIT, subcutaneous immunotherapy; mo, months; n, number; SD, standard deviation.
Discussion
AR is a common pediatric condition, and its detrimental impact on QoL has been well-documented in previous studies.13 Although pharmacotherapy is the first-line approach for controlling symptoms in most patients, AIT remains the only etiologic treatment capable of modifying the course of the disease and providing sustained clinical benefits.1,14 AIT has gained increasing use in AR management because of its proven efficacy in reducing nasal and ocular symptoms and improving QoL.15
In the present study, we compared the effects of different treatment durations of SCIT on symptom control and QoL in pediatric patients. Our findings demonstrate that children who received ≥36 months of SCIT achieved significantly better outcomes in both symptom control and QoL compared with those treated for shorter durations. These results provide direct clinical support for the EAACI and other international guideline recommendations advocating a minimum of three years of continuous AIT.16
Our results are consistent with those reported by Agenäs et al.,17 who conducted a prospective study of 158 pediatric patients over a three-year follow-up. They observed significant reductions in TNSS scores and improvements in QoL scores by the third year of SCIT.17 Similarly, subgroup analyses from the REACT study by Contoli et al. demonstrated that patients who continued uninterrupted AIT over nine years experienced greater improvements in AR symptoms compared with those lost to follow-up.18 Field and Blaiss19 also highlighted that SCIT administered for at least three years results in sustained long-term symptom control.
Bożek et al. evaluated the efficacy of allergen-specific immunotherapy in 78 patients (43 female, 35 male; aged 18–76 years) with AR, comparing SCIT with placebo after 24 months of treatment. They found that TNSS scores decreased significantly in the SCIT group compared with placebo, indicating substantial improvement in AR, symptoms.20
In our study, VAS assessments yielded comparable findings in favor of longer treatment duration. The proportion of well-controlled patients (VAS < 2) was significantly higher in the ≥36-month group than in the <36-month group, whereas the proportion of patients with uncontrolled symptoms was higher in the short-duration group. These results suggest that treatment duration influences not only immunological response but also patient-reported satisfaction and daily functional capacity. This aligns with the systematic review by Field and Blaiss,19 which emphasized the positive impact of SCIT on clinical scores and patient-perceived symptom reduction, as assessed by VAS, in individuals with AR.
Similarly, in a pediatric cohort study, Song et al.21 compared 193 children receiving SCIT with those treated with pharmacotherapy alone. Over a 3-year follow-up, both groups demonstrated significant VAS score improvement; however, the SCIT group achieved a greater magnitude of improvement than the pharmacotherapy-only group.
AR has been reported to negatively affect patients’ physical, social, and emotional functioning, thereby impairing overall QoL.13 In our study, QoL was assessed according to treatment duration using the PRQLQ and RQLQ scales. Results from both instruments demonstrated significantly higher QoL in patients who received SCIT for ≥36 months. Among patients aged 12–18 years, assessed with the PRQLQ, statistically significant differences were observed in the school and social functioning subdomains. In patients aged ≥18 years, assessed with the RQLQ, mean total scores were significantly lower, indicating better QoL. Similar findings have been reported in the literature. Vieira et al. demonstrated that better control of allergic rhinitis was associated with improved academic productivity and reduced educational impairment in children and young people, whereas poor rhinitis control was linked to greater loss of school performance and educational activities.22 Likewise, Song et al. reported that SCIT produced significantly greater QoL improvements than pharmacotherapy alone in pediatric AR patients.21
In adult patients assessed with the RQLQ, lower total scores similarly reflected better QoL. Bożek et al. also demonstrated that AIT significantly improved QoL, as measured by the RQLQ, compared with placebo.20
A major strength of our study is the comprehensive evaluation of pediatric SCIT recipients not only in terms of symptom control but also QoL, using validated clinical scales and age-appropriate QoL questionnaires to ensure data reliability. Nevertheless, the limited sample size constrains the generalizability of our findings and the ability to draw causal inferences. A major limitation of our study was the lack of baseline TNSS, VAS data prior to initiation of immunotherapy, which precluded within-patient longitudinal comparison. In addition, because baseline PRQLQ scores were not available, we were unable to quantify individual QoL changes from pretreatment to follow-up, and our conclusions are limited to cross-sectional comparisons between treatment-duration groups. Furthermore, the number of studies in the literature that simultaneously evaluate symptom scores and QoL according to SCIT duration in pediatric pollen allergy patients remains very limited. Due to the small number of participants in the PRQLQ subgroup, the statistical power was limited; therefore, the results should be interpreted with caution. It should also be noted that all patients receiving <36 months of SCIT experienced treatment interruptions due to the COVID-19 pandemic, which affected both patient follow-up visits and availability of SCIT extracts (vials). As a result, some patients were unable to complete the planned 3-year course, which we believe was a key factor contributing to higher symptom scores and lower QoL in this group. During the COVID-19 pandemic period, treatment interruptions were observed more frequently among patients in the <36-month group. These interruptions may have reduced cumulative exposure to immunotherapy and thereby contributed to less favorable outcomes.
In conclusion, our findings demonstrate that administering pollen SCIT for more than 36 months in pediatric AR patients provides clear advantages in reducing clinical symptoms and improving QoL. These data confirm the clinical relevance of the minimum treatment duration recommended by international guidelines and reinforce the importance of completing a continuous SCIT course of at least three years.
Ethics Approval
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Ankara Bilkent City Hospital Ethic Committee for clinical studies, approval number: TABED 2-24-86. Written informed consent was obtained from all participants prior to their inclusion in the study.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authors’ Consent for Publication
All authors confirm that they have read and approved the final version of the manuscript. The authors declare that the manuscript represents original work, has not been published previously, and is not under consideration for publication elsewhere.
Acknowledgements
We sincerely thank all patients and their families for their participation and cooperation. We also acknowledge the clinical staff of the Pediatric Allergy and Immunology Departments at City Hospital and Research and Training Hospital for their valuable support during data collection.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Author Contributions
H.I.Ç. conceived the study, coordinated the project, contributed to data collection, analysis, and drafting manuscript and is the corresponding author; R.D. contributed to data collection; Ç.T.Ö. contributed to data collection; A.S. contributed to the literature review and preparation of the manuscript; Z.Ş.E. supervised the study, provided critical feedback, and approved the final version of the manuscript; E.D.M. supervised the study, provided critical feedback, and approved the final version of the manuscript.
Conflicts of Interests
The authors declare that they have no competing interests.
Funding
This study received no funding from any institutions or government.
REFERENCES
1 Wise SK, Damask C, Roland LT, et al. International consensus statement on allergy and rhinology: Allergic rhinitis–2023. Int Forum Allergy Rhinol. 2023;13(4):293–59. 10.1002/alr.23090
2 Klimek L, Bachert C, Pfaar O, et al. ARIA guideline 2019: treatment of allergic rhinitis in the German health system. Allergo J Int. 2019;28(7):255–76. 10.1007/s40629-019-00110-9
3 Brożek JL, Bousquet J, Agache I, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines—2016 revision. J Allergy Clin Immunol. 2017;140(4):950–58. 10.1016/j.jaci.2017.03.050
4 Tosca MA, Trincianti C, Naso M, Nosratian V, Ciprandi G. Treatment of allergic rhinitis in clinical practice. Curr Pediatr Rev. 2024;20(3):271–77. 10.2174/1573396320666230912103108
5 Roberts G, Pfaar O, Akdis C, et al. EAACI guidelines on allergen immunotherapy: allergic rhinoconjunctivitis. Allergy. 2018;73(4):765–98. 10.1111/all.13317
6 Dykewicz MS, Wallace DV, Amrol DJ, et al. Rhinitis 2020: a practice parameter update. J Allergy Clin Immunol. 2020;146(4):721–67. 10.1016/j.jaci.2020.07.007
7 Sultész M, Horváth A, Molnár D, et al. Prevalence of allergic rhinitis, related comorbidities and risk factors in schoolchildren. Allergy Asthma Clin Immunol. 2020;16(1):98. 10.1016/j.jaci.2020.07.007
8 Pfaar O, Demoly P, Gerth van Wijk R, et al. Recommendations for the standardization of clinical outcomes used in allergen immunotherapy trials for allergic rhinoconjunctivitis: an EAACI Position Paper. Allergy. 2014;69(7):854–867. 10.1111/all.12383
9 Klimek L, Bergmann KC, Biedermann T, et al. Visual analogue scales (VAS): Measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care. Allergo J Int. 2017;26(1):16–24. 10.1007/s40629-016-0006-7
10 Varni JW, Seid M, Rode CA. The PedsQL™: measurement model for the pediatric quality of life inventory. Medical Care. 1999;37(2):126–39. 10.1097/00005650-199902000-00003
11 Memik NC, Agaoglu B, Coskun A, Uneri OS, Karakaya I. The validity and reliability of the Turkish Pediatric Quality of Life Inventory for children 13-18 years old. Turk Psikiyatri Dergisi. 2007;18(4):353.
12 Yuksel H, Yilmaz O, Alkan S, Değirmenci PB, Kirmaz C. Validity and reliability of Turkish version of rhinitis and mini-rhinitis quality of life questionnaires. Allergologia et immunopathologia. 2009;37(6):293–97. 10.1016/j.aller.2009.04.006
13 Alblewi SMS, Alenazi LM, Alshahrani RS, et al. Prevalence of allergic rhinitis and its impact on quality of life among pediatric patients in Tabuk, Saudi Arabia. Oman Med J. 2024;39(6):e696. 10.5001/omj.2024.118
14 Wang C, Bao Y, Chen J, et al. Chinese guideline on allergen immunotherapy for allergic rhinitis: the 2022 update. Allergy Asthma Immunol Res. 2022;14(6):604. 10.4168/aair.2022.14.6.604
15 Bao Y, Chen J, Cheng L, et al. Chinese Guideline on allergen immunotherapy for allergic rhinitis. J Thorac Dis. 2017;9(11):4607–4650. 10.21037/jtd.2017.10.112
16 Roberts G, Pfaar O, Akdis CA, et al. EAACI Guidelines on Allergen Immunotherapy: Allergic rhinoconjunctivitis. Allergy. 2018;73(4):765–798. 10.1111/all.13317
17 Agenäs H, Brorsson AL, Kull I, Lindholm-Olinder A. Treatment with pollen allergen immunotherapy improves health-related quality of life in children and adolescents: a three-year follow-up-study. Allergy Asthma Clin Immunol. 2023;19(1):4. 10.1186/s13223-023-00756-9
18 Contoli M, Porsbjerg C, Buchs S, Larsen JR, Freemantle N, Fritzsching B. Real-world, long-term effectiveness of allergy immunotherapy in allergic rhinitis: subgroup analyses of the REACT study. J Allergy Clin Immunol. 2023;152(2):445–452. e444. 10.1016/j.jaci.2023.02.024
19 Field K, Blaiss MS. Sublingual versus subcutaneous immunotherapy for allergic rhinitis: what are the important therapeutic and real-world considerations? Curr Allergy Asthma Rep. 2020;20(9):45. 10.1007/s11882-020-00934-4
20 Bożek A, Kołodziejczyk K, Jarząb J. Efficacy and safety of birch pollen immunotherapy for local allergic rhinitis. Ann Allergy Asthma Immunol. 2018;120(1):53–58. 10.1016/j.anai.2017.10.009
21 Song Y, Long J, Wang T, Xie J, Wang M, Tan G. Long-term efficacy of standardised specific subcutaneous immunotherapy in children with persistent allergic rhinitis due to multiple allergens including house dust mites. J Laryngol Otol. 2018;132(3):230–35. 10.1017/S0022215117002547
22 Vieira RJ, Pham-Thi N, Anto JM, et al. Academic Productivity of Young People With Allergic Rhinitis: A MASK-air Study. J Allergy Clin Immunol Pract. 2022;10(11):3008–3017.e4. 10.1016/j.jaip.2022.08.015