
Download
ORIGINAL ARTICLE
Pediatric drug allergy: a retrospective analysis of clinical features, laboratory parameters, and systemic inflammation indices
Filiz Demir Şahin*, Ozan Kapçay, Mehmet Kılıç
Department of Pediatric Immunology and Allergy, Faculty of Medicine, Fırat University, Elâzığ, Turkey
Abstract
Background: This study aimed to investigate the potential utility of hematological parameters and systemic inflammatory indices as predictive biomarkers in pediatric patients with drug hypersensitivity reactions (DHRs).
Methods: We performed a retrospective review of medical records of children presenting to the Pediatric Allergy and Immunology Clinic at Fırat University Hospital, Turkey, between January 2019 and July 2025 with suspected DHRs. Demographic characteristics, clinical manifestations, reaction phenotypes, complete blood counts, and total immunoglobulin E (IgE) levels were analyzed. Inflammatory indices, such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), eosinophil-to-lymphocyte ratio (ELR), and systemic immune–inflammation index (SII), were calculated subsequently.
Results: Among the 45 children included, drug allergy was confirmed in 14 (31.1%) children. Total IgE levels did not differ significantly between groups (P = 0.712). Monocyte counts were significantly higher in the patient group (P = 0.039), whereas eosinophil counts were elevated in the control group (P = 0.026). Lymphocyte (P = 0.002) and basophil counts (P = 0.002) were significantly lower in the patient cohort. No significant differences were observed in neutrophil or platelet counts. Regarding inflammatory indices, NLR (P = 0.007), PLR (P = 0.006), and SII (P = 0.007) were significantly increased in the patient group, whereas ELR did not differ significantly (P = 0.073).
Conclusion: In this small, single-center cohort (n = 45; confirmed DHR, n = 14), higher NLR, PLR, and SII were observed among children with confirmed DHRs. These preliminary findings suggest that readily available hematological indices may aid hypothesis generation and tentative risk stratification; however, they should be interpreted cautiously and require confirmation in larger prospective studies.
Key words: drug hypersensitivity reactions, inflammatory biomarkers, pediatric drug allergy
*Corresponding author: Filiz Demir Şahin, MD, Department of Pediatric Immunology and Allergy, Faculty of Medicine, Fırat University, Elazığ, Turkey. Email address: [email protected]
Received 9 September 2025; Accepted 15 September 2025; Available online 1 July 2026
Copyright: Şahin FD, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Drug hypersensitivity reactions (DHRs) represent a significant health concern in childhood, encompassing a wide clinical spectrum ranging from mild cutaneous eruptions to life-threatening anaphylaxis. The prevalence of DHRs in the pediatric population is reported to range between 2% and 10%; however, relying solely on clinical history frequently leads to overdiagnosis and unnecessary drug restrictions. This situation consequently narrows therapeutic options, increases healthcare costs, and prolongs treatment duration.1,2 Objective diagnostic approaches, such as skin testing and drug provocation testing (DPT), are therefore essential for confirming the diagnosis. Accurate identification of drug reactions is critical not only for avoiding unwarranted drug avoidance but also for determining safe alternative therapies and preventing potentially severe reactions.
In children, the most common causative agents of drug allergies include antibiotics—particularly β-lactams (penicillins and cephalosporins)—as well as macrolides and nonsteroidal anti-inflammatory drugs (NSAIDs).3,4 According to the Gell and Coombs classification, DHRs are categorized into four main types: Type I (immunoglobulin E [IgE]-mediated), Type II (cytotoxic), Type III (immune complex-mediated), and Type IV (T-cell-mediated delayed-type reactions).5 Antibiotic-induced reactions most frequently involve Type I or Type IV mechanisms; however, recent studies have demonstrated that non-IgE, neutrophil-mediated inflammatory pathways may also play a role in certain cases.6
Maculopapular exanthems are typically associated with the Type IVb DHR, characterized by an eosinophil-dominant T-cell response.7 These benign cutaneous reactions are often infection-related, rather than true IgE-mediated allergies. Therefore, in children with a history of benign rashes, direct amoxicillin provocation without prior skin testing can be performed safely.8 For instance, during Epstein–Barr virus infection, the incidence of rash after amoxicillin exposure ranges between 30% and 100%, and these reactions are frequently mislabeled as drug allergies.8
Similarly, reactions to sulfonamides, macrolides, fluoroquinolones, and NSAIDs usually manifest as delayed-onset cutaneous eruptions with a benign course, while anaphylactic reactions are exceedingly rare.8 Clinically, DHRs are classified as immediate (<6 h) or non-immediate (>6 h) according to the time of onset. Immediate reactions are mostly IgE-mediated, although non-IgE mechanisms—such as mast cell activation through MRGPRX2—are also described.8 Among non-immediate reactions, maculopapular exanthema represents the most frequent benign phenotype, whereas severe forms, such as Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS), Acute Generalized Exanthematous Pustulosis (AGEP), and Stevens–Johnson syndrome–toxic epidermal necrolysis (SJS/TEN) are also identified. These syndromes are associated with distinct T-cell subtypes; for example, DRESS is characterized by a Th2/eosinophilic response, whereas AGEP involves an IL-8-driven neutrophilic pathway.8
The European Academy of Allergy and Clinical Immunology (EAACI) and the European Network for Drug Allergy (ENDA) emphasize that relying exclusively on patient history may lead to unnecessary drug restrictions and highlight the drug provocation test as the gold standard for confirming tolerance to suspected medications.8 The interaction between drugs and the immune system may occur through mechanisms, such as the hapten/prohapten concept, pseudo allergy, or the pharmacologic interaction with immune receptors (p-i concept), which can overlap and trigger distinct cellular responses.9
Non-immediate DHRs are predominantly T-cell-mediated and typically appear from several hours to days after drug exposure. Maculopapular exanthema is the most common manifestation within this group.9 However, studies investigating the immunological and inflammatory biomarkers associated with drug allergies in pediatric populations are limited.
This study aimed to compare children with confirmed drug allergy to those in whom drug allergy was excluded, in terms of clinical characteristics, laboratory parameters, and inflammatory indices in order to identify potential diagnostic biomarkers.
Methods
In this retrospective study, the medical records of patients who presented to the Pediatric Allergy and Immunology Clinic at Fırat University Hospital, Turkey, between January 2019 and July 2025 with a preliminary diagnosis of drug allergy, were reviewed.
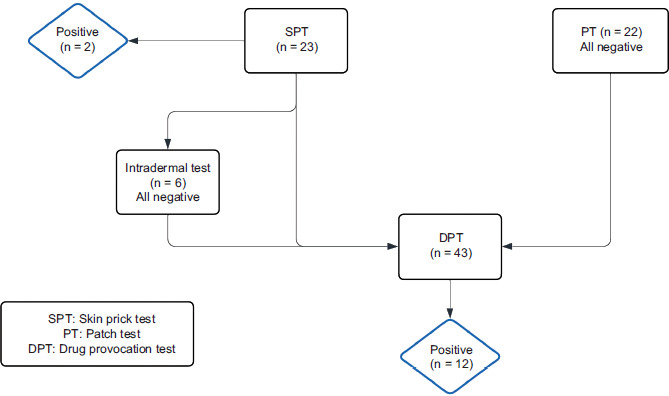
The patient group consisted of children in whom the diagnosis of drug allergy was confirmed based on clinical history, findings of physical examination, and diagnostic testing. The patient group (n = 14) included children with either a positive skin prick test (n = 2) or a positive drug provocation test (n = 12). The control group included age-matched children in whom a drug allergy diagnosis was excluded; these patients had presented to the clinic with suspected drug reactions but had negative results on diagnostic tests. The control group (n = 31) consisted of children in whom DHR was excluded based on negative results from all diagnostic procedures performed, including DPT.
Drug provocation testing is currently considered the gold standard for ruling out drug allergy and is often performed directly in patients with a benign clinical history.8
Inclusion criteria
-
Age between 0 and 18 years
-
Presentation to the clinic with suspected drug reactions
-
Availability of complete medical records, including demographic data, clinical findings, laboratory results, and fully documented diagnostic tests.
Exclusion criteria
-
History of chronic immunodeficiency, malignancy, or hematologic disorders.
-
Ongoing treatment for active infection or inflammatory disease at the time of presentation.
-
Cases with incomplete laboratory data.
The following data were extracted from electronic medical records:
-
Demographic characteristics (age, gender, et al.).
-
Suspected drug and drug class.
-
Type and timing of the reaction.
-
Comorbid conditions (e.g., allergic rhinitis, atopic dermatitis, and asthma).
-
Diagnostic tests performed (skin prick test, intradermal test, patch test, drug provocation test).
-
Management strategies (observation, antihistamines, and epinephrine).
-
Route of drug administration (oral, intravenous, and subcutaneous).
Laboratory parameters such as complete blood counts (CBC) and total IgE levels were collected at the time of presentation. Blood samples were not collected during acute hypersensitivity reaction. All samples for hematological parameters were collected at the initial outpatient evaluation, approximately 4–6 weeks after complete resolution of allergic reaction. At the time of sampling, none of the patients had an active infection, ongoing inflammatory condition, or receiving any medication. CBC results provided neutrophil, lymphocyte, monocyte, eosinophil, basophil, and platelet counts. The following inflammatory indices were calculated subsequently:
-
Neutrophil-to-lymphocyte ratio (NLR) = Neutrophil count/lymphocyte count
-
Platelet-to-lymphocyte ratio (PLR) = Platelet count/lymphocyte count
-
Eosinophil-to-lymphocyte ratio) = Eosinophil count/lymphocyte count
-
Systemic immune-inflammation index (SII) = (Neutrophil × platelet)/lymphocyte
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA).
-
Categorical variables were expressed as frequencies and proportions; differences between groups were evaluated using the Chi-squared test or Fisher’s exact test, as appropriate.
-
The normality of continuous variables was assessed using the Shapiro–Wilk test. Non-normally distributed data were presented as medians (minimum–maximum), and group comparisons were conducted using the Mann–Whitney U test.
-
P < 0.05 was considered statistically significant.
Results
In the patient group, 85.7% were males and 14.3% were females, whereas in the control group, 45.2% were males and 54.8% were females; this gender distribution differed significantly between the groups (P = 0.021). No significant difference was observed in age distribution between the groups (patient group: median 5.5 years [range 1.25–13]; control group: median 7 years [range: 0.83–17]; P = 0.307).
The most frequently reported symptom in the patient group was maculopapular rashes, observed in eight cases (57.1%). Urticaria, anaphylaxis, and angioedema were reported in two patients each (14.3%), yielding a cumulative prevalence of 42.9% for these reactions. In the control group, maculopapular rashes were observed in 14 patients (45.2%), followed by urticaria in 13 patients (41.9%) and angioedema in 4 patients (12.9%); no patient with anaphylaxis was recorded.
The majority of patients in both patient group (85.7%) and control group (83.9%) had no comorbidities. Allergic rhinitis was present in 7.1% patients of the patient group and 9.7% patients of the control group. Atopic dermatitis was observed only in the patient group (7.1%), while asthma was reported exclusively in the control group (6.5%).
Analysis of reaction types revealed that 42.9% of the patients exhibited type I drug reactions, whereas 57.1% demonstrated type IV drug reactions (n = 14). Regarding management of the 14 patients who developed drug reactions, 57.1% were managed with observation alone, 14.3% received antihistamines, 14.3% were treated with epinephrine, and 14.3% received a combination of corticosteroids and antihistamines.
The median reaction duration in the patient group was 5.5 h (range: 0.17–168 h), while in the control group the median duration was 4 h (range: 0.17–12 h). Analysis of comorbidities in the patient group revealed that the majority of patients (85.7%, n = 12) had no additional medical condition. Allergic rhinitis and atopic dermatitis were observed in one patient each (7.1%, n = 1). The most frequently implicated drug in allergic reactions was amoxicillin–clavulanic acid (Table 1). Maculopapular rashes were the predominant clinical manifestation in the patient group (Table 2).
Table 1 Distribution of allergenic drugs according to patient number.
| Allergenic drug | Patients, n (%) |
|---|---|
| Amoxicillin-clavulanate | 7 (50.0) |
| Clarithromycin | 1 (7.1) |
| Cefixime | 1 (7.1) |
| Ibuprofen | 1 (7.1) |
| Cetirizine | 1 (7.1) |
| Azithromycin | 1 (7.1) |
| Cefuroxime | 1 (7.1) |
| Cephalexin | 1 (7.1) |
| Total | 14 (100) |
Table 2 Distribution of reaction types according to diagnostic certainty.
| Reaction type | Patients, n (%) | Controls, n (%) |
|---|---|---|
| Maculopapular rash | 8 (57.1) | 14 (45.2) |
| Urticaria | 2 (14.3) | 13 (41.9) |
| Anaphylaxis | 2 (14.3) | 0 (0.0) |
| Angioedema | 2 (14.3) | 4 (12.9) |
For patients presenting with anaphylaxis, angioedema, or urticaria, the skin prick test was performed initially; in patients with negative results, intradermal testing was conducted for parenterally administered drugs, whereas DPT was applied directly for other medications. In patients with maculopapular exanthema, patch testing was performed, and those with negative results underwent DPT subsequently. The outcomes of the skin tests and drug provocation tests employed for the diagnosis of drug allergy are summarized in Figure 1.
Figure 1 Drug allergy diagnostic workflow and test results.
Laboratory parameters
The median total IgE level was 21.5 IU/mL (range: 17.5–244 IU/mL) in the patient group and 30.9 IU/mL (range: 3.78–3160 IU/mL) in the control group, with no statistically significant difference observed (P = 0.712; Table 3). Neutrophil counts were higher in the patient group (4935/µL [range: 2180–7300]), although this difference was not statistically significant (P = 0.079). Monocyte counts were significantly elevated in the patient group, compared to controls (905/µL [100–1010] vs. 680/µL [100–1470]; P = 0.039). Eosinophil counts were higher in the control group, and this difference was statistically significant (200/µL [10–810] vs. 40/µL [10–470]; P = 0.026). In the control group, children with higher eosinophil counts more frequently had comorbid atopic conditions, such as allergic rhinitis and asthma (P = 0.007). No significant difference was observed in platelet counts between both groups (P = 0.228). Lymphocyte counts were markedly lower in the patient group (1735/µL [1090–8650] vs. 3050/µL [1090–9700]; P = 0.002); similarly, basophil counts were significantly reduced in the patient group (10/µL [10–40] vs. 30/µL [10–240]; P = 0.002).
Table 3 Comparison of laboratory and clinical parameters between patients with confirmed drug allergy and controls without drug allergy.
| Parameter | Patient group median (Min–Max) | Control group median (Min–Max) | P value |
|---|---|---|---|
| Age (years) | 5.5 (1.25–13) | 7 (0.83–17) | 0.307 |
| Reaction duration (h) | 5.5 (0.17–168) | 4 (0.17–12) | 0.522 |
| Total IgE (IU/mL) | 21.5 (17.5–244) | 30.9 (3.78–3160) | 0.712 |
| Neutrophils (µL) | 4935 (2180–7300) | 3790 (1700–7850) | 0.079 |
| Monocytes (µL) | 905 (100–1010) | 680 (100–1470) | 0.039* |
| Eosinophils (µL) | 40 (10–470) | 200 (10–810) | 0.026* |
| Platelets (µL) | 286,000 (264,000–535,000) | 334,000 (265,000–524,000) | 0.228 |
| Lymphocytes (µL) | 1735 (1090–8650) | 3050 (1090–9700) | 0.002** |
| Basophils (µL) | 10 (10–40) | 30 (10–240) | 0.002** |
| Neutrophil/lymphocyte (NLR) | 3.03 (0.27–5.01) | 1.10 (0.20–5.01) | 0.007** |
| Platelet/lymphocyte (PLR) | 201.44 (50.84–262.39) | 102.34 (43.66–262.39) | 0.006** |
| Eosinophil/lymphocyte (ELR) | 0.021 (0.0049–0.0726) | 0.059 (0.00176–0.2727) | 0.073 |
| Neutrophil × platelet/lymphocyte (SII) | 1,102,765 (142,254–1,432,623) | 423,354 (75,083–1,432,623) | 0.007** |
Note: *P < 0.05, **P < 0.01.
Inflammatory indices
The NLR was significantly higher in the patient group (3.03 [0.27–5.01] vs. 1.10 [0.20–5.01]; P = 0.007). The PLR was also elevated in the patient group (201.44 [50.84–262.39] vs. 102.34 [43.66–262.39]; P = 0.006). Although the ELR was higher in the control group, the difference was not statistically significant (P = 0.073). The SII was significantly higher in the patient group, compared to controls (1,102,765 [142,254–1,432,623] vs. 423,354 [75,083–1,432,623]; P = 0.007).
Discussion
In our study, a predominance of male children was observed with confirmed DHRs. This finding aligns with several reports suggesting that males could represent a potential risk factor for the development of DHRs. Duque et al. reported an increased risk of DHRs in boys aged >13 years.10 However, the literature presents inconsistent results regarding gender distribution. Brandão et al. found that the proportion of female patients was higher in both pediatric and adult populations, although no significant difference was observed in the frequency of confirmed DHRs.11 Similarly, Yaytokgil and Vezir demonstrated an equal gender distribution among Turkish children.12 A relatively small sample size in our study warrants cautious interpretation of the observed related findings.
Evaluation of the distribution of suspected drugs demonstrated that amoxicillin-clavulanate was the most frequent causative agent. This finding was consistent in the existing literature, which indicates that β-lactam antibiotics represent the most common cause of drug allergy in the pediatric population.13 In our study, the prevalence of concomitant allergic diseases was 14.3% (2/14), with allergic rhinitis and atopic dermatitis being the most frequently observed conditions. This proportion was notably lower than that reported in a previous study involving 168 children with confirmed drug hypersensitivity, in which concomitant allergic diseases were observed in 44.6% of patients.14 Among children with confirmed DHRs in our cohort, maculopapular eruptions were the most commonly observed cutaneous manifestation (57.1%), followed by urticaria, anaphylaxis, and angioedema (14.3% each). These results are consistent with previous reports indicating that maculopapular eruptions (20–80%) and urticaria/angioedema (20–30%) are the most frequent cutaneous manifestations of DHRs in children.15
In our study, no patient exhibited elevated total IgE levels. Absence of a significant difference in total IgE values aligns with previous reports indicating that total IgE has limited diagnostic value in drug allergies.5 In eight out of 14 patients, the reaction duration was ≥5 h. Delayed-type DHRs develop through heterogeneous mechanisms mediated by different T-cell subsets. Type IVa (monocyte/macrophage), Type IVb (Th2/eosinophil), and Type IVd (neutrophil) pathways are associated with distinct clinical phenotypes.8 Although maculopapular exanthems are typically explained by a Type IVb (Th2/eosinophil-dominant) mechanism, the observed low eosinophil and elevated monocyte counts in our study suggests that multiple immune pathways may be simultaneously activated, rather than a single mechanism being predominant. This finding is consistent with the current guidelines emphasizing the heterogeneous immunopathogenesis of delayed-type reactions.8,9 Similarly, increased monocyte levels may indicate activation of the Type IVa pathway, in which macrophage activation mediated by interferon gamma (IFN-γ) and tumor necrosis factor-α (TNF-α) contributes to the pathogenesis of these reactions.7 The limited number of studies investigating monocyte-mediated mechanisms in drug hypersensitivity enhances the originality of our findings.
Another notable result of our study is that eosinophil and basophil counts were significantly lower in children with confirmed drug allergy, compared to the control group. This supports the notion that DHRs do not always develop through classical IgE-mediated mechanisms but may also involve non-IgE-mediated, monocyte-dominant inflammatory processes. The relatively higher eosinophil levels observed in the control group suggest that false-positive cases based solely on clinical history may be more closely associated with an underlying atopic predisposition. This interpretation is further supported by the observation that children of the control group with higher eosinophil counts more often had comorbid atopic conditions, suggesting that the elevated eosinophil levels may reflect underlying atopic predisposition, rather than drug-related immunologic activation.
In our study, the patient group exhibited significantly elevated NLR, PLR, and SII, a noteworthy observation. These hematological indices serve as indicators of systemic inflammatory burden and are increasingly investigated in the diagnosis and prognosis of chronic inflammatory and allergic diseases. However, studies evaluating these parameters in pediatric drug allergies are limited. Our findings suggest that these indices may serve as potential biomarkers for the diagnosis and risk stratification of DHRs. Moreover, their accessibility and low cost represent a practical advantage for clinical application.
The strengths of our study include the evaluation of all cases using objective methods (skin tests and/or drug provocation tests), allowing for the distinction between true drug allergies and misattributed reactions. Limitations of the study include the relatively small sample size, single-center and retrospective design, and the assessment of inflammatory parameters based solely on single measurements at the time of presentation. In addition, the marked gender imbalance—characterized by a substantially higher proportion of males in the confirmed DHR group—represents a potential confounding factor and should be taken into account when interpreting the findings. Prospective studies that capture the dynamic changes of inflammatory responses over time could provide a more comprehensive understanding of the predictive value of these biomarkers. Additionally, viral reactivation—particularly human herpesvirus 6 (HHV-6) and Epstein–Barr virus (EBV) in cases of DRESS—has been reported as a potential co-trigger in certain DHRs,7,16 and this possible mechanism must be explored in future investigations.
Conclusion
Our study demonstrates that DHRs in children cannot be fully explained by classical IgE-mediated mechanisms alone, and that monocyte-mediated innate immune responses could play a significant role. Hematological indices, such as NLR, PLR, and SII, represent readily accessible biomarkers that may contribute to the diagnostic process. These findings warrant validation in larger cohorts through prospective multicenter studies.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Author Contributions
All authors contributed equally to this article.
Conflict of Interest
The authors declared no potential conflict of interest with respect to research, authorship, and/or publication of this article.
Funding
None.
REFERENCES
1 Atanaskovic-Markovic M, Gaeta F, Medjo B, Gavrovic-Jankulovic M, Cirkovic Velickovic T, Tmusic V, et al. Non-immediate hypersensitivity reactions to beta-lactam antibiotics in children—Our 10-year experience in allergy work-up. Pediatr Allergy Immunol. 2016;27(5):533–8. 10.1111/pai.12565
2 Gomes E, Brockow K, Kuyucu S, Saretta F, Mori F, Blanca-Lopez N, et al. Drug hypersensitivity in children: Report from the pediatric task force of the EAACI Drug Allergy Interest Group. Allergy. 2016;71(2):149–61. 10.1111/all.12774
3 Piccorossi A, Liccioli G, Barni S, Sarti L, Giovannini M, Verrotti A, et al. Epidemiology and drug allergy results in children investigated in allergy unit of a tertiary-care pediatric hospital setting. Allergol Immunopathol (Madr). 2020;46(1):5. 10.1186/s13052-019-0753-4
4 Milosevic K, Malinic M, Plavec D, Lekovic Z, Lekovic A, Cobeljic M, et al. Diagnosing single and multiple drug hypersensitivity in children: A tertiary care center retrospective study. Children (Basel). 2022;9(12):1954. 10.3390/children9121954
5 Pichler WJ. Delayed drug hypersensitivity reactions. Ann Intern Med. 2003;139(8):683–693. 10.7326/0003-4819-139-8-200310210-00012
6 Roberto B, Fabio C, Francesca M, Francesca S, Lucia L, Fabrizio F, et al. Management of the child with allergy to non-antibiotic drugs. Allergy. 2019;90(Suppl 3):5. 10.23750/abm.v90i3-S.8149
7 Thomson P, Hammond S, Naisbitt DJ. Pathology of drug hypersensitivity reactions and mechanisms of immune tolerance. Curr Allergy Clin Immunol. 2022;52(12):1379–90. 10.1111/cea.14235
8 Khan DA, Banerji A, Blumenthal KG, Phillips EJ, Solensky R, White AA, et al. Drug allergy: A 2022 practice parameter update. J Allergy Clin Immunol. 2022;150(6):1333–93. 10.1016/j.jaci.2022.08.028
9 Zhang X, Hu F, Hana M, Wang X, Wang Q, Zhou K, et al. An updated review of the diagnostic methods in drug hypersensitivity reactions. Front Allergy. 2025;4:100045. 10.1016/j.allmed.2025.100045
10 Duque JSR, Cheuk DK, Chong PC, Ip P, Wong WH, Lee PP, et al. Risk factors for drug allergies in Chinese children. Allergy Asthma Proc. 2020;38(4):271–8. 10.12932/AP-191018-0417
11 Brandão LS, Nunes FA, Bastos PGA, Guerzet P, Lacerda AE, Piza CF, et al. Drug hypersensitivity reactions: Are there differences between children and adults? Allergy. 2019;143(2):AB160. 10.1016/j.jaci.2018.12.486
12 Yaytokgil ŞB, Vezir E. Characteristics of drug hypersensitivity reactions in children: A retrospective analysis in an allergy outpatient clinic. Turk J Child Health Dis. 2024;18(4):247–52. 10.12956/tchd.1462063
13 Bergmann M, Caubet JC. Specific aspects of drug hypersensitivity in children. Curr Pharm Des. 2016;22(45):6832–51. 10.2174/1381612822666160926105533
14 Yaytokgil ŞB, Demir KI, Topal ÖY, Metbulut AP, Çelik İK, Toyran M, et al. Evaluation of accompanying allergic disease in children with proven drug allergies. Turk J Med Sci. 2024;54(1):316–23. 10.55730/1300-0144.5793
15 Lezmi G, Alrowaishdi F, Bados-Albiero A, Scheinmann P, de Blic J, Ponvert CJ, et al. Non-immediate-reading skin tests and prolonged challenges in non-immediate hypersensitivity to beta-lactams in children. Pediatr Allergy Immunol. 2018;29(1):84–9. 10.1111/pai.12826
16 Shiohara T, Kano Y. A complex interaction between drug allergy and viral infection. Curr Opin Rheumatol Immunol. 2007;33(1):124–33. 10.1007/s12016-007-8010-9