
Download
RESEARCH ARTICLE
Demographic characteristics and allergen sensitization profiles in patients with allergic rhinitis in Shenzhen, China
Chengzhi Huang, Zhiyuan Tang*
Department of Otorhinolaryngology – Head and Neck Surgery, Shenzhen University General Hospital, Shenzhen, China
Abstract
Background: Allergic rhinitis (AR) is increasingly prevalent in China, yet allergen sensitization data in coastal subtropical cities such as Shenzhen remain scarce.
Objective: To investigate allergen distribution and demographic characteristics among AR patients in Shenzhen, China.
Methods: A retrospective analysis was conducted on 3351 AR patients from January to December 2022. Serum-specific immunoglobulin E (sIgE) levels were measured; values ≥0.35 kU/L were considered positive and graded into six levels. Allergen patterns were compared by gender, age (<14 vs. ≥14 years), and sIgE level.
Results: Clinic visits peaked in August. The most prevalent allergens were Blomia tropicalis (Bt), Dermatophagoides pteronyssinus (Dp), and Dermatophagoides farinae (Df). Other important indoor allergens included cockroach, dog dander, and cat dander. Leading outdoor allergens were Ambrosia artemisiifolia (ragweed), Chenopodium album/Amaranthus retroflexus, and Platanus/Fraxinus. Male patients showed higher sensitization to Dp and Df (P < 0.05). The sensitization proportions for leading allergens (Bt, Dp, and Df) declined with increasing age: compared with adolescents and adults (≥14 years), pediatric patients (<14 years) had significantly higher sensitization to indoor allergens, whereas the adolescent/adult group showed significantly higher sensitization to pollens and molds (P < 0.05). Dp and Df responses peaked at class 3, Bt and cat dander at class 2, and cockroach/dog dander/pollens/molds at class 1, with significant differences in sIgE levels among allergens (P < 0.05).
Conclusion: Dust mites, especially Bt, are the primary source of allergens affecting AR patients in Shenzhen. Sensitization patterns differ by age, gender, and sIgE levels, highlighting the importance of region-specific allergen surveillance and personalized AR management.
Key words: age-related patterns, Blomia tropicalis, indoor and outdoor allergens, regional surveillance, specific IgE levels
*Corresponding author: Zhiyuan Tang, Department of Otorhinolaryngology – Head and Neck Surgery, Shenzhen University General Hospital, 1098 Xueyuan Road, Shenzhen, Guangdong 518055, China. Email address: [email protected]
Received 19 August 2025; Accepted 22 October 2025; Available online 1 March 2026
Copyright: Huang C and Tang Z
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Allergic rhinitis (AR) is a common chronic inflammatory disorder of nasal mucosa, driven by immunoglobulin E (IgE)-mediated hypersensitivity to environmental allergens.1 It is characterized by nasal congestion, sneezing, rhinorrhea, and nasal itching, and can substantially impair quality of life and reduce work productivity. In recent years, the global prevalence of AR has continued to rise, largely attributed to rapid urbanization, environmental pollution, and lifestyle changes.2,3 In China, epidemiological data indicate a 6.5% increase in AR prevalence in recent years, with particularly high proportions reported in densely populated and highly industrialized urban areas.4
Shenzhen, a rapidly growing coastal metropolis in southern China, has a warm and humid subtropical climate. Combined with high population density and frequent human mobility, these conditions create a distinctive allergen exposure environment. A previous study showed that sensitization patterns in subtropical regions differ markedly from those in temperate climates, such as Europe, with higher sensitization to house dust mites, pronounced age-related variations, and only limited overlap in prevalent allergens across regions.5 While allergen sensitization has been investigated in several inland regions of China,6,7 data from Shenzhen remain scarce, despite its unique geographic and demographic characteristics. To address this gap, the present study aimed to characterize the demographic features and allergen sensitization profiles of AR patients in Shenzhen. By analyzing serum-specific IgE (sIgE) levels, this study seeks to provide evidence-based insights to support improved prevention, diagnosis, and individualized management of AR in this region.
Methods
Study population
This retrospective study included AR patients who reported at the Department of Otorhinolaryngology – Head and Neck Surgery, Shenzhen University General Hospital, between January 2022 and December 2022. Inclusion criteria were as follows: (1) presence of typical AR symptoms, such as sneezing, nasal congestion, rhinorrhea, and nasal itching; (2) diagnosis confirmed by clinical history and physician evaluation; (3) availability of sIgE test results; and (4) permanent residents of Shenzhen, China. Exclusion criteria included: (1) comorbid chronic rhinosinusitis or nasal polyps; (2) autoimmune or systemic diseases that may affect immune responses; and (3) incomplete clinical or laboratory data.
Allergen-specific IgE testing
Peripheral venous blood samples were collected from all patients and analyzed using the ImmunoCAP system (Phadia AB, Uppsala, Sweden). A total of 19 common allergens were tested, including dust mites, animal dander, pollens, and molds. A serum sIgE level ≥0.35 kU/mL was considered positive. Sensitization levels were classified into six classes based on sIgE concentration: class 1: 0.35–0.69 kU/mL, class 2: 0.70–3.49 kU/mL, class 3: 3.50–17.49 kU/mL, class 4: 17.50–49.99 kU/mL, class 5: 50.00–99.99 kU/mL, class 6: ≥100 kU/mL.8
Grouping and comparative analysis
Patients were stratified by gender (male vs. female), age (<14 years as pediatric group vs. ≥14 years as adolescent/adult group), and sIgE positivity level. The distribution of allergen sensitization was analyzed across these subgroups to explore demographic variations.
Statistical analysis
All statistical analyses were performed using GraphPad Prism version 8.0.2 (GraphPad Software, San Diego, CA, USA). Categorical data were expressed as percentages. Group comparisons were conducted using the Chi-square test; P < 0.05 was considered statistically significant.
Results
General characteristics
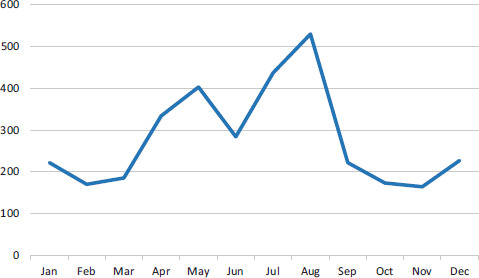
A total of 3351 patients diagnosed with AR were included, comprising 1964 males (58.61%) and 1387 females (41.39%), with a male-to-female ratio of 1.42:1. Among them, 1731 patients (51.66%) were aged <14 years, while 1620 patients (48.34%) were adolescents/adults. Of the 3351 patients diagnosed with AR, the number of clinic visits peaked in August (530 cases) and was lowest in November (164 cases) (Figure 1).
Figure 1 Annual trend in the number of allergen-positive cases (n).
Overall allergen sensitization profile
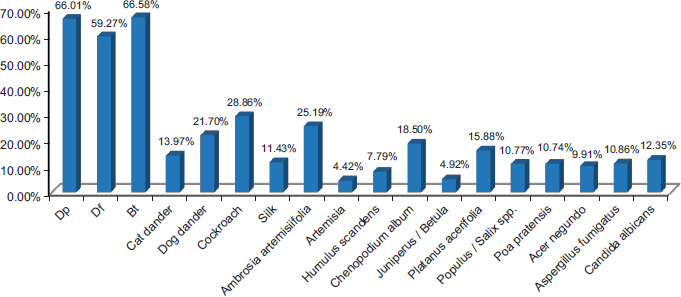
Among all patients, 2503 (74.69%) tested positive for at least one allergen-specific IgE. The most prevalent allergens were Blomia tropicalis (Bt) (66.58%), Dermatophagoides pteronyssinus (Dp) (66.01%), and Dermatophagoides farinae (Df) (59.27%). Other important indoor allergens included cockroach (28.86%), dog dander (21.70%), and cat dander (13.97%). The leading outdoor allergens were Ambrosia artemisiifolia (25.19%), Chenopodium album/Amaranthus retroflexus (18.50%), and Platanus acerifolia/Fraxinus (15.88%) (Figure 2).
Figure 2 Positivity proportions of individual allergens. Df: Dermatophagoides farinae; Bt: Blomia tropicalis; Dp: Dermatophagoides pteronyssinus.
Gender-based differences in allergen sensitization
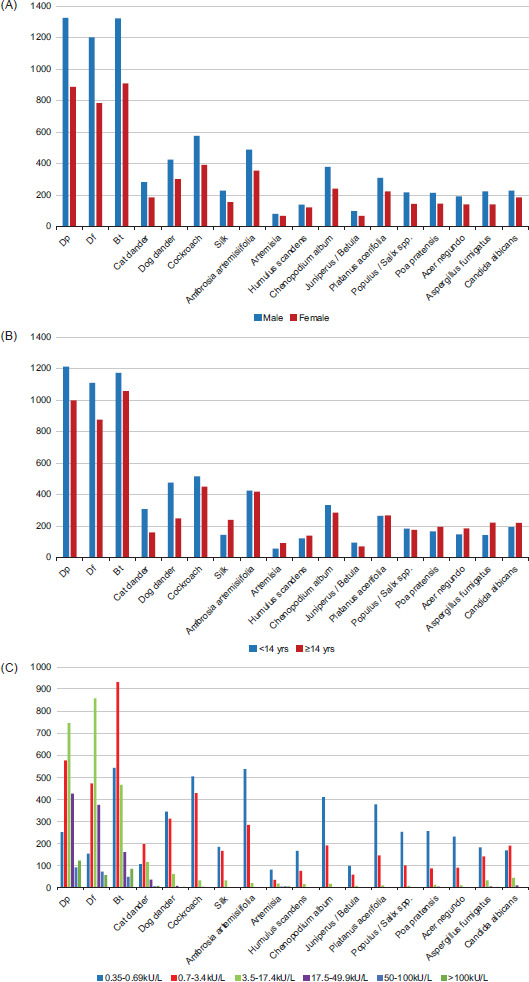
In males, the top three allergens were Df (67.46%), Bt (67.31%), and Dp (61.20%). In females, Bt ranked first (65.54%), followed by Df (63.95%) and Dp (56.52%) (Figure 3A). Male patients had significantly higher sensitization proportions to Dp (χ2 = 4.472, P < 0.05) and Df (χ2 = 7.365, P < 0.05) than females. No significant gender differences were observed for other allergens (Table 1).
Figure 3 (A) Distribution of allergen sensitization by gender (n). (B) Distribution of allergen sensitization by age (n). (C) Distribution of allergen sensitization by quantitative sIgE class (n). Df: Dermatophagoides farinae; Bt: Blomia tropicalis; Dp: Dermatophagoides pteronyssinus.
Table 1 Analysis of allergen distribution by gender.
| Group | Male (n [%]) | Female (n [%]) | χ2 | P |
|---|---|---|---|---|
| Dermatophagoides pteronyssinus | 1325 (59.90) | 887 (40.10) | 4.472 | 0.034 |
| Dermatophagoides farina | 1202 (60.52) | 784 (39.48) | 7.365 | 0.007 |
| Blomia tropicalis | 1322 (59.26) | 909 (40.74) | 1.072 | 0.301 |
| Cat dander | 283 (60.47) | 185 (39.53) | 0.690 | 0.406 |
| Dog dander | 425 (58.46) | 302 (41.54) | 0.003 | 0.960 |
| Cockroach | 576 (59.57) | 391 (40.43) | 0.458 | 0.498 |
| Silk | 227 (59.27) | 156 (40.73) | 0.050 | 0.823 |
| Ambrosia artemisiifolia | 489 (57.94) | 355 (42.06) | 0.174 | 0.677 |
| Artemisia | 80 (54.05) | 68 (45.95) | 1.135 | 0.287 |
| Humulus scandens | 139 (53.26) | 122 (46.74) | 3.108 | 0.078 |
| Chenopodium album/Amaranthus retroflexus | 379 (61.13) | 241 (38.87) | 1.866 | 0.172 |
| Juniperus/Betula | 98 (59.39) | 67 (40.61) | 0.017 | 0.833 |
| Platanus acerifolia/Fraxinus | 309 (59.08) | 223 (40.92) | 0.072 | 0.898 |
| Populus/salix spp. | 217 (60.11) | 144 (39.89) | 0.310 | 0.578 |
| Poapratensis and related grasses | 214 (59.44) | 146 (40.56) | 0.081 | 0.777 |
| Acer negundo and related maples | 192 (57.83) | 140 (42.17) | 0.060 | 0.807 |
| Aspergillus fumigatus | 223 (61.26) | 141 (38.74) | 1.066 | 0.302 |
| Candida albicans and related species | 229 (55.31) | 185 (44.69) | 1.962 | 0.161 |
Age-based differences in allergen sensitization
In the pediatric group (aged <14 years), Df was the most prevalent allergen (70.08%), followed by Bt (67.76%) and Dp (64.12%). In the adolescent/adult group (aged ≥14 years), Bt (65.31%) ranked first, followed by Dp (61.67%) and Df (54.07%) (Figure 3B). Notably, the sensitization proportions of leading allergens (Bt, Dp, and Df) declined with increasing age. Specifically, pediatric patients exhibited significantly higher sensitization to indoor allergens, including Dp (χ2 = 25.996, P < 0.001), Df (χ2 = 34.601, P < 0.001), cat dander (χ2 = 42.993, P < 0.001), and dog dander (χ2 = 71.698, P < 0.001). In contrast, adolescent/adult patients demonstrated higher sensitization to outdoor allergens, including pollens, such as silk (χ2 = 34.861, P < 0.001), Artemisia (χ2 = 10.166, P < 0.05), Poapratensis (χ2 = 5.218, P < 0.05), and Acer negundo (χ2 = 7.711, P < 0.05) as well as molds such as Aspergillus fumigatus (χ2 = 25.583, P < 0.001) and Candida albicans (χ2 = 4.573, P < 0.05) (Table 2).
Table 2 Analysis of allergen distribution by age.
| Group | <14 yr (n [%]) | ≥14 yr (n [%]) | χ2 | P |
|---|---|---|---|---|
| Dermatophagoides pteronyssinus | 1213 (54.84) | 999 (45.16) | 25.996 | <0.001 |
| Dermatophagoides farina | 1110 (56.40) | 876 (43.60) | 34.601 | <0.001 |
| Blomia tropicalis | 1173 (52.58) | 1058 (47.42) | 2.159 | 0.142 |
| Cat dander | 308 (65.81) | 160 (34.19) | 42.993 | <0.001 |
| Dog dander | 477 (65.61) | 250 (34.39) | 71.698 | <0.001 |
| Cockroach | 516 (53.36) | 451 (46.64) | 1.125 | 0.289 |
| Silk | 143 (37.34) | 240 (62.66) | 34.861 | <0.001 |
| Ambrosia artemisiifolia | 425 (50.36) | 419 (49.64) | 0.696 | 0.404 |
| Artemisia | 57 (38.51) | 91 (61.49) | 10.166 | 0.001 |
| Humulus scandens | 122 (46.74) | 139 (53.26) | 2.527 | 0.112 |
| Chenopodium album/Amaranthus retroflexus | 334 (53.87) | 286 (46.13) | 1.387 | 0.239 |
| Juniperus/Betula | 95 (57.58) | 70 (42.42) | 2.192 | 0.139 |
| Platanus acerifolia/Fraxinus | 265 (49.81) | 267 (50.19) | 0.776 | 0.378 |
| Populus/Salix spp. | 184 (50.97) | 177 (49.03) | 0.049 | 0.825 |
| Poapratensis and related grasses | 165 (45.83) | 195 (54.17) | 5.218 | 0.022 |
| Acer negundo and related maples | 147 (44.28) | 185 (55.72) | 7.711 | 0.005 |
| Aspergillus fumigatus | 142 (39.01) | 222 (60.99) | 25.583 | <0.001 |
| Candida albicans and related species | 193 (46.62) | 221 (53.38) | 4.573 | 0.032 |
Distribution of sIgE levels among allergen types
For Dp and Df, most patients exhibited class 3 sIgE levels (3.50–17.49 kU/mL). For Bt and cat dander, sensitization peaked at class 2 (0.70–3.49 kU/mL). For dog dander and cockroach, sensitization was mainly at class 1 (0.35–0.69 kU/mL). Sensitization to pollens and molds was predominantly at class 1 (0.35–0.69 kU/mL), indicating low-level responses (Figure 3C). The distribution of sIgE classes differed significantly among allergen types (χ2 = 5487, P < 0.05) (Table 3).
Table 3 Analysis of allergen distribution by quantitative sIgE class.
| Group | Class 1 (n [%]) | Class 2 (n [%]) | Class 3 (n [%]) | Class 4 (n [%]) | Class 5 (n [%]) | Class 6 (n [%]) | χ2 | P |
|---|---|---|---|---|---|---|---|---|
| Dermatophagoidespteronyssinus | 251 (11.35) | 576 (26.04) | 745 (33.68) | 426 (19.26) | 92 (4.16) | 122 (5.52) | 5487 | <0.001 |
| Dermatophagoides farina | 154 (7.75) | 472 (23.77) | 857 (43.15) | 375 (18.88) | 72 (3.63) | 56 (2.82) | ||
| Blomia tropicalis | 542 (24.29) | 931 (41.73) | 465 (20.84) | 160 (7.17) | 49 (2.20) | 84 (3.77) | ||
| Cat dander | 106 (22.65) | 197 (42.09) | 115 (24.57) | 36 (7.69) | 6 (1.28) | 8 (1.71) | ||
| Dog dander | 344 (47.32) | 312 (42.92) | 61 (8.39) | 7 (0.96) | 0 (0) | 3 (0.41) | ||
| Cockroach | 504 (52.12) | 428 (44.26) | 32 (3.31) | 3 (0.31) | 0 (0) | 0 (0) | ||
| Silk | 184 (48.04) | 166 (43.34) | 32 (8.36) | 1 (0.26) | 0 (0) | 0 (0) | ||
| Ambrosia artemisiifolia | 537 (63.63) | 284 (33.65) | 20 (2.37) | 1 (0.12) | 2 (0.24) | 0 (0) | ||
| Artemisia | 81 (54.73) | 35 (23.65) | 18 (12.16) | 4 (2.70) | 5 (3.38) | 5 (3.38) | ||
| Humulus scandens | 167 (63.98) | 75 (28.74) | 15 (5.75) | 2 (0.77) | 0 (0) | 2 (0.77) | ||
| Chenopodium album/ | ||||||||
| Amaranthus retroflexus | 410 (66.13) | 191 (30.81) | 16 (2.58) | 2 (0.32) | 1 (0.16) | 0 (0) | ||
| Juniperus/Betula | 98 (59.39) | 59 (35.76) | 8 (4.85) | 0 (0) | 0 (0) | 0 (0) | ||
| Platanus acerifolia/Fraxinus | 377 (70.86) | 146 (27.44) | 9 (1.69) | 0 (0) | 0 (0) | 0 (0) | ||
| Populus/Salix spp. | 253 (70.08) | 100 (27.70) | 7 (1.94) | 1 (0.28) | 0 (0) | 0 (0) | ||
| Poapratensis and related grasses | 256 (71.11) | 87 (24.17) | 12 (3.33) | 4 (1.11) | 0 (0) | 1 (0.28) | ||
| Acer negundo and related maples | 230 (69.28) | 90 (27.11) | 10 (3.01) | 2 (0.60) | 0 (0) | 0 (0) | ||
| Aspergillus fumigatus | 182 (50.00) | 141 (38.74) | 32 (8.79) | 6 (1.65) | 0 (0) | 3 (0.82) | ||
| Candida albicans and related species | 168 (40.58) | 190 (45.89) | 44 (10.63) | 9 (2.17) | 2 (0.48) | 1 (0.24) |
Discussion
This study presents a comprehensive overview of the demographic characteristics and allergen sensitization profiles in patients with AR in Shenzhen, China. The results demonstrate that house dust mites—particularly Bt, Dp, and Df—are the predominant sensitizing allergens. This pattern aligns with the subtropical coastal climate of Shenzhen, characterized by warmth and high humidity, which provides optimal conditions for mite proliferation. These findings highlight the central role of dust mites in the pathogenesis of AR in this region and underscore the importance of targeted allergen surveillance and prevention strategies.
The prominence of Bt sensitization in this study is particularly noteworthy, as this allergen has been less frequently reported in northern China but appears to play a major role in subtropical regions, such as Guangdong. Historically, Df was reported as the leading allergen in Shenzhen between 2004 and 2015, followed by Dp, consistent with patterns observed across southern China.9–11 Our findings, however, suggest a potential shift in the allergen spectrum, with Bt emerging as a dominant sensitizer. This trend may reflect advances in allergen detection techniques as well as environmental influences, including Shenzhen’s subtropical monsoon climate and the broader impact of global warming, which may favor Bt proliferation. In addition, although previous work from Guangzhou indicated rising sensitization to animal-derived allergens in association with urbanization and increased pet ownership,12 our study found cockroach sensitization to be more prevalent than pet allergen sensitization in Shenzhen. This likely reflects the city’s warm and humid environment, which is highly conducive to cockroach survival. Together, these results underscore the importance of region-specific allergen surveillance, which is essential for guiding effective prevention measures and tailoring allergen-specific immunotherapy.
Previous studies have suggested that allergen sensitization patterns may differ between male and female patients with AR, potentially due to gender-related differences in immune regulation and the modulatory effects of sex hormones on disease-associated gene expression.13,14 In line with this, our study found that male patients exhibited higher sensitization proportions to Dp and Df, indicating possible gender-related disparities in allergen exposure or immune responsiveness. These differences may be partly mediated by hormonal influences, as estrogen and progesterone enhance humoral and Th2-driven immune responses, whereas testosterone generally exerts immunosuppressive effects.15 Additionally, genetic and epigenetic factors, including X-linked immune regulatory genes, may contribute to gender-specific variations,16 and occupational or behavioral factors could further modulate allergen exposure.17 Further research is warranted to elucidate the biological mechanisms underlying these gender-based differences and their clinical implications.
In our study, the sensitization proportions of leading allergens declined with increasing age. Pediatric patients showed significantly higher sensitization to indoor allergens, including mites and animal dander, whereas adolescents and adults were more strongly sensitized to outdoor allergens, such as pollens and molds. These patterns align with longitudinal studies reporting an age-related decrease in allergen sensitization and serum sIgE levels,18,19 probably attributable to immunosenescence, including thymic involution, reduced naïve T- and B-cell output, and lower IgE production.20 In children, Th2-biased responses, reduced regulatory T-cell activity, and elevated IgE, combined with prolonged indoor exposure, predispose them to indoor allergens. In contrast, adolescents and adults show diminished reactivity to indoor allergens because of immunosenescence, while broader environmental exposure drives higher pollen and mold sensitization. Overall, these findings highlight the roles of immune maturation, senescence, and environmental factors in shaping allergen sensitization and support age-specific prevention and immunotherapy strategies.
With respect to sIgE distribution, most patients sensitized to Dp and Df exhibited moderate IgE concentrations (class 3), whereas Bt and cat dander peaked at class 2, and plant-derived allergens were largely associated with low-level sensitization. These distinctions may reflect differences in allergenic potency, environmental exposure, and host immune responsiveness. Recognizing such patterns is clinically relevant, as they provide insights into the likelihood of symptomatic disease and can guide the selection and prioritization of allergens in immunotherapy protocols.
Despite its strengths, this study has several limitations. First, as a single-center retrospective analysis, the potential for selection bias cannot be excluded, and temporal trends in sensitization could not be assessed. Second, clinical correlations—such as symptom severity, validated scoring systems (e.g., VAS, TNSS), or treatment outcomes—were not incorporated, restricting the ability to determine the clinical significance of sensitization. Future prospective, multicenter studies with integrated clinical data are warranted to validate and extend these findings.
Conclusion
Dust mites—particularly Bt—represent the predominant allergens among AR patients in Shenzhen, with cockroach sensitization exceeds that of pet dander. Allergen patterns differ by age, gender, and sIgE level: males tend to show higher reactivity to Dp and Df, and the overall sensitization to leading allergens declines with increasing age. Pediatric patients are more affected by indoor allergens, whereas adolescents and adults are more affected by pollens and molds. While most allergens elicit low to moderate sIgE levels, mites generally induce stronger sIgE responses. These findings highlight the importance of region-specific allergen surveillance to refine diagnosis, guide individualized allergen avoidance, and optimize immunotherapy strategies for AR.
Ethical Approval and Consent to Participate
This retrospective study utilized anonymized medical records from Shenzhen University General Hospital. According to the Institutional Review Board/Ethics Committee of Shenzhen University General Hospital, formal ethical approval was not required because the study involved no direct patient contact, interventions, or risk of harm. All data were de-identified prior to analysis, and patient confidentiality was strictly maintained. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Data Availability
The datasets are not publicly available due to institutional and privacy restrictions but can be obtained from the corresponding author upon reasonable request and with approval from Shenzhen University General Hospital.
Authors Contribution
Chengzhi Huang was responsible for data analysis, manuscript drafting, and revising. Zhiyuan Tang designed the study and supervised the work.
Conflict of Interest
The authors reported no conflict of interest in this work.
Funding
This study was funded by Shenzhen Science and Technology Program, No.: JCYJ20200109114244249.
REFERENCES
1 Subspecialty Group of Rhinology, Editorial Board of Chinese Journal of Otorhinolaryngology Head and Neck Surgery, Subspecialty Group of Rhinology, Society of Otorhinolaryngology Head and Neck Surgery, Chinese Medical Association. Chinese guideline for diagnosis and treatment of allergic rhinitis (2022 revision). Chin J Otorhinolaryngol Head Neck Surg. 2022;57(2):106–29.
2 Bousquet J, Anto JM, Bachert C, Baiardini I, Bosnic-Anticevich S, Walter Canonica G, et al. Allergic rhinitis. Nat Rev Dis Primers. 2020;6(1):95. 10.1016/S0025-7125(05)70535-6
3 Asam C, Hofer H, Wolf M, Aglas A, Wallner M. Tree pollen allergens—An update from a molecular perspective. Allergy. 2015;70(10):1201–11. 10.1111/all.12696
4 Wang XD, Zheng M, Lou HF, Wang CS, Zhang Y, Bo MY, et al. An increased prevalence of self-reported allergic rhinitis in major Chinese cities from 2005 to 2011. Allergy. 2016;71(8):1170–80. 10.1111/all.12874
5 Larenas-Linnemann D, Michels A, Dinger H, Shah-Hosseini K, Mösges R, Arias-Cruz A, et al. Allergen sensitization linked to climate and age, not to intermittent-persistent rhinitis in a cross-sectional cohort study in the (sub)tropics. ClinTransl Allergy. 2014 Jun 4;4:20. 10.1186/2045-7022-4-20
6 Luo WT, Wang DD, Zhang T, Zheng PY, Leng DL, Li L, et al. Prevalence patterns of allergen sensitization by region, gender, age, and season among patients with allergic symptoms in Mainland China: A four-year multicenter study. Allergy. 2021;76(2):589–93. 10.1111/all.14597
7 Tao XY, Ng CL, Chen D, Lin ZB, Wu SL, Liang MJ, et al. Clinical characteristics and allergen sensitization patterns of patients with local allergic rhinitis in southern China. Int Arch Allergy Immunol. 2018;175(1–2):107–13. 10.1159/000485896
8 Nikolaizik WH, Weichel M, Blaser K, Crameri R. Intracutaneous tests with recombinant allergens in cystic fibrosis patients with allergic bronchopulmonary aspergillosis and aspergillus allergy. Am J Respir Crit Care Med. 2002 Apr 1;165(7):916–21. 10.1164/ajrccm.165.7.2109008
9 Kai YM, Shi LP, Zhang Y. The allergen analysis and nursing of abnormal rhinitis. Chin J Prim Medpharm. 2006;13(2):272–3.
10 Li Y, Chu SD, Zhang J. Analysis of allergen distribution and risk factors in patients with allergic rhinitis. China Modern Doctor. 2022;60(8):54–7.
11 Chen M, Lu MP, Cheng L. Characteristic analysis of allergens in 423 allergic rhinitis patients in Jiangsu and Anhui provinces. Chin J Otorhinolaryngol Integ Med. 2021;29(3):188–94,-99.
12 Wang WH, Huang XK, Chen ZG, Zheng R, Chen YL, Zhang GH, et al. Prevalence and trends of sensitisation to aeroallergens in patients with allergic rhinitis in Guangzhou, China: A 10-year retrospective study. BMJ Open. 2016;6e:011085. 10.1136/bmjopen-2016-011085
13 Hong SN, Won JY, Nam EC, Kim TS, Ryu YJ, Kwon JW, et al. Clinical manifestations of allergic rhinitis by age and gender: A 12 year single-center study. Ann Otorhinolaryngol. 2020;129(9):910–17. 10.1177/0003489420921197
14 De Amici M, Ciprandi G. The age impact on serum total and allergen-specific IgE. Allergy Asthma Immunol Res. 2013 May;5(3):170–4. 10.4168/aair.2013.5.3.170
15 Taneja V. Sex hormones determine immune response. Front Immunol. 2018 Aug 27;9:1931. 10.3389/fimmu.2018.01931
16 Feng Z, Liao M, Zhang L. Sex differences in disease: Sex chromosome and immunity. J Transl Med. 2024 Dec 27;22(1):1150. 10.1186/s12967-024-05990-2
17 Murrison LB, Brandt EB, Myers JB, Hershey GKK. Environmental exposures and mechanisms in allergy and asthma development. J Clin Invest. 2019 Apr 1;129(4):1504–15. 10.1172/JCI124612
18 De Martinis M, Sirufo MM, Suppa M, Silvestre DD, Ginaldi L. Sex and gender aspects for patient stratification in allergy prevention and treatment. Int J Mol Sci. 2020;21(4):1535. 10.3390/ijms21041535
19 Grabenhenrich LB, Keil T, Reich A, Gough H, Beschorner J, Hoffmann U, et al. Prediction and prevention of allergic rhinitis: A birth cohort study of 20 years. J Allergy Clin Immunol. 2015;136(4):932–40 e12. 10.1016/j.jaci.2015.03.040
20 Lynch HE, Goldberg GL, Chidgey A, Van den Brink MR, Boyd R, Sempowski GD. Thymic involution and immune reconstitution. Trends Immunol. 2009 Jul;30(7):366–73. 10.1016/j.it.2009.04.003