
Download
RESEARCH ARTICLE
Baseline serum double-mite (D1+D2) sIgE/tIgE ratio as a predictor of early-phase response to dual-mite subcutaneous immunotherapy in allergic rhinitis
Chengzhi Huang, Zhiyuan Tang*
Department of Otorhinolaryngology – Head and Neck Surgery, Shenzhen University General Hospital, Shenzhen, China
Abstract
Background: Subcutaneous immunotherapy (SCIT) for allergic rhinitis (AR) requires long-term treatment, and its phased efficacy often influences patient adherence. Identifying early biomarkers, such as serum-specific IgE to total IgE (sIgE/tIgE) ratio, may support individualized management.
Objective: To determine the predictive value of baseline double-mite (D1+D2) sIgE/tIgE ratio for phased dual-mite SCIT response in AR patients.
Methods: We prospectively enrolled 194 AR patients sensitized to Dermatophagoides pteronyssinus (D1) and Dermatophagoides farinae (D2) who received dual-mite SCIT between September 2022 and January 2023. Baseline serum tIgE and sIgE (D1+D2) were measured, and the combined sIgE/tIgE ratio was calculated. Treatment response was evaluated by reduction in visual analogue scale (VAS) scores at months 6 and 12, with the efficacy distribution compared between the two time points using the Chi-square test. Univariable and multivariable logistic regression identified predictors of achieving at least an effective response, and receiver operating characteristic (ROC) analysis was applied for sIgE/tIgE ratio when indicated.
Results: SCIT efficacy improved over time, with a significant shift in response distribution between 6 and 12 months (χ2 = 10.084, P = 0.006). At 6 months, multivariable analysis showed that both higher baseline VAS score (OR = 0.954, 95% CI: 0.929–0.980, P < 0.001) and higher sIgE/tIgE ratio (OR = 0.985, 95% CI: 0.972–0.999, P = 0.036) were independently associated with lower likelihood of achieving at least effective response. ROC analysis indicated a cutoff sIgE/tIgE ratio of 26.62% for predicting poor short-term response. At month 12, only baseline VAS score remained a significant predictor (OR = 1.038, 95% CI: 1.005–1.072, P = 0.025).
Conclusion: SCIT efficacy progressively improves over the first year. A higher baseline sIgE (D1+D2)/tIgE ratio (>26.62%) predicts poorer short-term response, highlighting the value of objective biomarkers for early response assessment and individualized management.
Key words: allergen immunotherapy, predictive biomarker, specific IgE, total IgE, treatment outcome
*Corresponding author: Zhiyuan Tang, Department of Otorhinolaryngology – Head and Neck Surgery, Shenzhen University General Hospital, 1098 Xueyuan Road, Shenzhen, Guangdong 518055, China. Email address: [email protected]
Received 19 August 2025; Accepted 27 October 2025; Available online 1 March 2026
Copyright: Huang C and Tang Z
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Allergic rhinitis (AR) is a common chronic inflammatory disorder of the nasal mucosa caused by IgE-mediated hypersensitivity to environmental allergens.1 It affects an estimated 10–40% of the global population and imposes a substantial burden on quality of life, healthcare systems, and work productivity.2 Among inhalant allergens, Dermatophagoides pteronyssinus (D1) and Dermatophagoides farinae (D2) are leading triggers, particularly in East Asia.3
Allergen immunotherapy remains the only disease-modifying treatment for AR. By administering increasing doses of allergen extracts, SCIT induces long-term immune tolerance and is shown to reduce symptoms, medication use, and the risk of disease progression.4,5 However, the prolonged treatment duration and variable phased responses often compromise patient adherence, underscoring the need for reliable predictors—particularly objective biomarkers—to guide pre-treatment counseling and individualized management.
The serum-specific IgE to total IgE (sIgE/tIgE) ratio is proposed as a marker of allergic burden and immunologic responsiveness.6 While previous study has suggested the potential of the sIgE/tIgE ratio in predicting allergen immunotherapy outcomes in asthma,7 its predictive value in AR, particularly in differentiating short- and long-term responses to SCIT, remains unclear. Therefore, this study aimed to evaluate whether the baseline sIgE (D1+D2)/tIgE ratio can predict phased dual-mite SCIT response, with the goal of facilitating early responder identification and optimizing long-term management.
Methods
Study design and participants
This retrospective study included 194 AR patients who received SCIT at the Department of Otorhinolaryngology – Head and Neck Surgery, Shenzhen University General Hospital between September 2022 and January 2023. All participants underwent standardized health education regarding dust mite avoidance and environmental control, with consistently high adherence and no treatment interruptions. Inclusion criteria were: (1) age ≥6 years; (2) AR diagnosed according to the ARIA guidelines;8 (3) dual sensitization to D1 and D2 with sIgE ≥ 0.35 kU/L; and (4) completion of at least 12 months of dual-mite SCIT. Exclusion criteria included incomplete clinical records, irregular follow-up, or comorbidities, such as autoimmune diseases.
Immunotherapy protocol
Patients received standardized SCIT using house dust mite allergen extracts (Allergopharma, Germany) administered via subcutaneous injection. The allergen vaccines were supplied in three concentration vials (bottle No. 1: 50 therapeutic units [TU]/mL; bottle No. 2: 500 TU/mL; and bottle No. 3: 5000 TU/mL).
The treatment regimen comprised two phases: a dose-escalation phase and a maintenance phase. During the dose-escalation phase, injections were administered weekly with the following schedule: weeks 1–4: 0.1 mL, 0.2 mL, 0.4 mL, and 0.8 mL (50 TU/mL); weeks 5–8: 0.1 mL, 0.2 mL, 0.4 mL, and 0.8 mL (500 TU/mL); and weeks 9–14: 0.1 mL, 0.2 mL, 0.4 mL, 0.8 mL, and 1.0 mL (5000 TU/mL). The maintenance phase involved monthly injections of 1.0 mL (5000 TU/mL) from week 14 up to week 152. Dose or interval adjustments were allowed based on clinical response or adverse events.
Emergency medications and equipment for anaphylaxis management were prepared prior to each injection. Patients were observed for 30 min post-injection to monitor adverse reactions, including urticaria or bronchospasm. Clinicians managed adverse events as appropriate. Symptom evaluation and treatment efficacy were assessed every 6 months. The recommended duration of SCIT was 3 years.
IgE measurement and ratio calculation
Baseline serum tIgE, D1-sIgE, and D2-sIgE were measured using the ImmunoCAP system (Thermo Fisher Scientific, Uppsala, Sweden). The sIgE (D1+D2)/tIgE ratio was calculated as follows: sIgE (D1+D2)/tIgE ratio = (D1 — sIgE + D2 — sIgE) ÷ tIgE × 100%.
Efficacy assessment
Efficacy was evaluated at 6 and 12 months based on the percentage reduction in total VAS scores compared with baseline. Each patient rated four nasal symptoms—nasal obstruction, rhinorrhea, sneezing, and nasal itching—and medication use on a 10-cm VAS, where 0 indicated “no symptoms or no medication” and 10 indicated “worst possible symptoms or maximum medication use.” The total VAS score was calculated as the sum of these five items, representing the overall nasal symptom burden and medication requirement. Treatment response was classified as ineffective (<30% reduction from baseline), effective (30–50% reduction), or markedly effective (≥50% reduction). All assessments were patient-reported and completed in person during scheduled clinic visits (baseline, month 6, and month 12) under supervision of an otolaryngologist.
Statistical analysis
All statistical analyses were conducted using SPSS version 27.0.1 (IBM Corp., Armonk, NY, USA). Response distributions between month 6 and month 12 were compared using the Chi-square test. Univariable and multivariable logistic regression analyses were performed to identify independent predictors of SCIT response, defined as a ≥30% reduction in total VAS score at 6 and 12 months. Independent variables included baseline sIgE (D1+D2)/tIgE ratio, age, gender, comorbid allergic diseases, baseline total VAS score (disease severity), baseline tIgE, and baseline sIgE levels. Variables with P < 0.1 in univariable analyses were entered into the multivariable model. Subgroup analyses further evaluated the stability of associations for variables that were independently significant in the multivariable analysis across different strata of age, gender, and comorbid allergic diseases. Sensitivity analyses were performed as needed to assess the robustness of the multivariable findings. For baseline sIgE (D1+D2)/tIgE ratio that showed statistically significant associations with treatment response in multivariable regression, receiver operating characteristic (ROC) curve analysis was conducted to evaluate predictive performance and to determine the optimal cutoff value using the Youden index. All statistical tests were two-tailed, and P < 0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 194 patients with dual mite-sensitized AR who completed at least 12 months of SCIT were included in the analysis. Baseline characteristics—age, gender, comorbid allergic diseases, VAS score, tIgE, sIgE, and sIgE (D1+D2)/tIgE ratio—are summarized in Table 1. Data are presented for the overall cohort as well as for subgroups stratified by treatment response at months 6 and 12. Continuous variables are expressed as mean ± standard deviation (SD), and categorical variables as counts.
Table 1 Baseline demographic and clinical characteristics of patients.
| Variables | Total (n = 194) |
6 M: Ineffective (n = 69) |
6 M: Effective (n = 43) |
6 M: Markedly effective (n = 82) |
12 M: Ineffective (n = 44) |
12 M: Effective (n = 39) |
12 M: Markedly effective (n = 111) |
|---|---|---|---|---|---|---|---|
| Age (years), mean ± SD |
12.65±10.00 | 13.38±11.26 | 11.26±7.62 | 12.78±10.02 | 10.43±7.61 | 13.21±10.51 | 13.34±10.59 |
| Gender (male/female) |
132/62 | 46/23 | 27/16 | 59/23 | 28/16 | 26/13 | 78/33 |
| AR alone/with comorbid allergies | 131/63 | 44/25 | 28/15 | 59/23 | 31/13 | 23/16 | 77/34 |
| VAS scores | 14.17±12.06 | 18.42±11.55 | 22.21±13.94 | 6.38±4.74 | 16.71±10.20 | 22.90±13.81 | 20.78±12.24 |
| tIgE (kU/L), mean±SD |
171.75±179.46 | 575.81±635.30 | 646.15±525.71 | 711.70±784.59 | 748.15±739.10 | 667.40±855.55 | 602.95±584.82 |
| sIgE (kU/L), mean±SD |
171.75±179.46 | 187.46±261.82 | 155.40±88.90 | 167.09±121.33 | 223.41±310.68 | 160.22±116.44 | 115.32±112.72 |
| sIgE (D1+D2)/tIgE ratio, mean±SD | 34.49±26.89 | 40.61±37.81 | 28.97±12.41 | 32.24±19.75 | 37.22±36.89 | 35.52±33.95 | 33.05±18.25 |
Note: AR: allergic rhinitis; IgE: immunoglobulin E; sIgE: serum-specific IgE; tIgE: total IgE; VAS: visual analogue scale.
Efficacy changes from month 6 to month 12
All 194 patients completed at least 12 months of SCIT. Among those classified as effective at month 6, 88.4% maintained or improved their response by month 12, with 53.5% progressing to markedly effective. Of patients with markedly effective response at month 6, 85.4% sustained their response, while only 7.3% regressed to be ineffective. Overall, the response distribution significantly differed between month 6 and month 12 (χ2 = 10.084, P = 0.006), indicating improved treatment outcomes over time (Table 2).
Table 2 Distribution of treatment efficacy at different time points (n).
| Treatment duration | Ineffective | Effective | Markedly effective | χ2 | P |
|---|---|---|---|---|---|
| Month 6 | 69 | 43 | 82 | 10.084 | 0.006 |
| Month 12 | 44 | 39 | 111 |
Baseline sIgE/tIgE ratio and efficacy at month 6
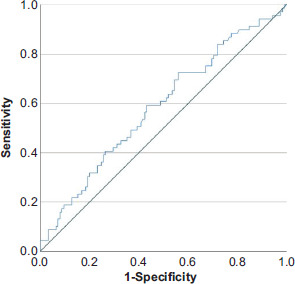
At month 6, the mean baseline sIgE (D1+D2)/tIgE ratios were 40.61% in the ineffective group, 28.97% in the effective group, and 32.24% in the markedly effective group. In univariable logistic regression analysis, both baseline VAS score (P < 0.001) and baseline sIgE (D1+D2)/tIgE ratio (P = 0.037) were identified as potential predictors. These two variables (VAS and sIgE/tIgE) were subsequently entered into the multivariable logistic regression model. The analysis showed higher baseline VAS score (OR = 0.954, 95% CI: 0.929–0.980, P < 0.001) and higher baseline sIgE (D1+D2)/tIgE ratio (OR = 0.985, 95% CI: 0.972–0.999, P = 0.036) remained independent predictors of a lower likelihood of achieving at least an effective response at month 6 (Table 3). Subgroup analyses revealed neither significant interactions between baseline sIgE (D1+D2)/tIgE ratio and age, gender, or comorbid allergic diseases, nor between baseline VAS score and these factors, indicating that the predictive effects of both variables were consistent across subgroups. The ROC curve analysis further assessed the discriminative performance of baseline sIgE (D1+D2)/tIgE ratio for predicting uneffective response. The area under the curve (AUC) was 0.585 (95% CI: 0.501–0.669, P = 0.050), indicating fair predictive ability. The optimal cutoff, determined by the Youden index was 26.62%, yielding a sensitivity of 72.5% and specificity of 56.0% (Figure 1).
Table 3 Logistic regression analysis of factors associated with 6-month response.
| Variables | Univariate OR (95% CI) | P | Multivariate adjusted OR (95% CI) | P |
|---|---|---|---|---|
| Age (years) | 0.989 | 0.456 | ||
| Gender (male vs. female) | 1.103 | 0.760 | ||
| Comorbid allergic diseases (yes vs. no) | 1.301 | 0.407 | ||
| Baseline VAS | 0.955 | <0.001 | 0.954 | <0.001 |
| tIgE (kU/L) | 1.000 | 0.273 | ||
| sIgE (D1+D2) (kU/L) | 0.999 | 0.385 | ||
| sIgE (D1+D2)/tIgE ratio (%) | 0.986 | 0.037 | 0.985 | 0.036 |
Note: IgE: immunoglobulin E; sIgE: serum-specific IgE; tIgE: total IgE.
Figure 1 Receiver operating characteristic (ROC) curve of the baseline sIgE (D1+D2)/tIgE ratio for predicting SCIT efficacy at month 6. The area under the curve (AUC) was 0.585 (95% CI: 0.501–0.669, P = 0.050), and the optimal cutoff value was 26.62%, with a sensitivity of 72.5% and specificity of 56.0%.
Baseline sIgE/tIgE ratio and efficacy at month 12
At month 12, the mean baseline sIgE (D1+D2)/tIgE ratios were 37.22% in the ineffective group, 35.52% in the effective group, and 33.05% in the markedly effective group. In univariable logistic regression analysis, baseline VAS score (P = 0.030) and baseline sIgE (P = 0.083) were identified as potential predictors, whereas baseline sIgE/tIgE ratio was not significantly associated with treatment efficacy (P = 0.450). These two variables (VAS and sIgE) were subsequently entered into the multivariable logistic regression model. The analysis showed that a higher baseline VAS score was independently associated with a greater likelihood of achieving at least an effective response at month 12 (OR = 1.038, 95% CI: 1.005–1.072, P = 0.025), whereas baseline sIgE was not statistically significant (Table 4). Subgroup analyses revealed no significant interactions between baseline VAS score and age, gender, or comorbid allergic diseases, suggesting that the predictive effect of VAS was consistent across these strata.
Table 4 Logistic regression analysis of factors associated with 12-month response.
| Variables | Univariate OR (95% CI) | P | Multivariate adjusted OR (95% CI) | P |
|---|---|---|---|---|
| Age (years) | 1.039 | 0.104 | ||
| Gender (male vs. female) | 1.292 | 0.477 | ||
| Comorbid allergic diseases (yes vs. no) | 0.839 | 0.637 | ||
| Baseline VAS | 1.037 | 0.030 | 1.038 | 0.025 |
| tIgE (kU/L) | 1.000 | 0.278 | ||
| sIgE (kU/L) | 0.998 | 0.083 | 0.998 | 0.079 |
| sIgE (D1+D2)/tIgE ratio (%) | 0.996 | 0.450 |
Note: IgE: immunoglobulin E; sIgE: serum-specific IgE; tIgE: total IgE; VAS: visual analogue scale.
Discussion
Subcutaneous immunotherapy is an established treatment for AR providing long-term symptom control through modulation of the immune response.9 Despite its proven efficacy, clinical responses to SCIT vary across treatment phases, highlighting the need for objective biomarkers that can predict early treatment outcomes and guide individualized management. The serum sIgE/tIgE ratio is proposed as a marker of allergen-specific sensitization and Th2-biased immune activity,10 but its role in predicting early-phase clinical responses to SCIT remains incompletely characterized.
In our study, more than half of the patients who did not achieve at least effective response at month 6 subsequently demonstrated clinical improvement by month 12, including a subset who reached markedly effective outcomes. This delayed response aligns with the immunologic trajectory of SCIT, where tolerance develops progressively through increased allergen-specific IgG4 production and expansion of regulatory T cells.11 Previous studies have shown that significant immunologic and symptomatic changes may not be evident until after 1 year of therapy,12,13 indicating that early non-response may reflect slower immune adaptation, rather than true treatment failure. Moreover, patients who responded at month 6 generally maintained their efficacy at month 12, highlighting the cumulative and sustained benefits of prolonged SCIT, consistent with long-term studies reporting improved symptom control, reduced medication use, and disease-modifying effects beyond 3 years of treatment.14,15 Collectively, these findings underscore that early clinical evaluation may underestimate the full therapeutic potential of SCIT and emphasize the importance of adequate treatment duration when assessing efficacy.
The sIgE/tIgE ratio may provide additional insight into phased treatment dynamics. In our cohort, patients with higher baseline VAS (a subjective measure) and higher baseline sIgE (D1+D2)/tIgE ratios (an objective immunologic indicator) were more likely to exhibit suboptimal short-term responses to dual-mite SCIT. The ROC analysis further demonstrated that a baseline sIgE (D1+D2)/tIgE ratio exceeding 26.62% predicted poorer short-term responsiveness. However, this association diminished by month 12, when higher baseline VAS scores were instead correlated with greater clinical improvement. These findings may also help reconcile discrepancies in previous studies reporting higher sIgE/tIgE ratios (e.g., >16.2%) as predictors of favorable long-term outcomes,16,17 as those analyses typically evaluated the overall efficacy without distinguishing early- from late-phase responses. Mechanistically, a high sIgE/tIgE ratio indicates strong allergen-specific IgE dominance relative to total IgE, reflecting heightened sensitization and Th2 polarization at baseline.18 Such patients may initially present with a more reactive effector environment, requiring longer allergen exposure to achieve immune deviation and tolerance.19 As desensitization progresses, the influence of allergen-specific IgE becomes functionally less relevant,20 consistent with the observed convergence of clinical outcomes by month 12. Therefore, the sIgE/tIgE ratio may serve as a dynamic biomarker of immunologic transition and could be useful for interpreting early-phase responses. Clinically, patients with high ratios may benefit from individualized counseling and sustained therapy, as early suboptimal improvement does not necessarily indicate treatment failure.
This study has several limitations. First, its retrospective single-center design may have introduced selection bias and limits the generalizability of the findings. Second, only patients monosensitized to dust mites were included; therefore, the results may not be extrapolated to individuals with polysensitization or different allergen profiles. Finally, although the baseline sIgE (D1+D2)/tIgE ratio threshold identified in this cohort (>26.62%) was associated with short-term outcomes, its predictive performance was limited (AUC = 0.585, 95% CI: 0.501–0.669, P = 0.050), with sensitivity and specificity of only 72.5% and 56.0%, respectively, and external validation in larger, multicenter, and prospective studies is warranted before it can be implemented in clinical practice.
Conclusion
In summary, SCIT demonstrates progressively improved efficacy over the first year of treatment. A higher baseline sIgE (D1+D2)/tIgE ratio, particularly >26.62%, was associated with poorer short-term response, highlighting its potential as an objective biomarker for early-phase outcome prediction and patient stratification. Importantly, extended therapy led to clinical improvement even in patients with elevated baseline ratios, underscoring the importance of adequate treatment duration, individualized pre-treatment counseling, and careful follow-up.
Statement of Ethics
This retrospective study used anonymized medical records from Shenzhen University General Hospital. According to the Institutional Review Board/Ethics Committee of Shenzhen University General Hospital, ethics approval was not required as no direct patient contact or risk was involved. All data were de-identified and analyzed anonymously. The study complied with the Declaration of Helsinki ethical standards.
Mandatory Disclosure on Use of Artificial Intelligence
The authors declare that no AI-assisted tools were used in the preparation of this manuscript. All references have been manually verified for accuracy and relevance.
Data Availability
The datasets are not publicly available due to institutional and privacy restrictions but can be obtained from the corresponding author upon reasonable request and with approval from Shenzhen University General Hospital.
Authors Contribution
Chengzhi Huang was responsible for data analysis, manuscript drafting, and revising. Zhiyuan Tang designed the study and supervised the work.
Conflict of Interest
The authors reported no conflict of interest in this work.
Funding
This study was funded by Shenzhen Science and Technology Program No.: JCYJ20200109114244249.
REFERENCES
1 Pawankar R. Allergic diseases and asthma: A global public health concern and a call to action. World Allergy Organ J. 2014 May 19;7(1):12. 10.1186/1939-4551-7-12
2 Li Q, Zhang X, Feng Q, Zhou H, Ma C, Lin C, et al. Common allergens and immune responses associated with allergic rhinitis in China. J Asthma Allergy. 2023 Aug 17;16:851–61. 10.2147/JAA.S420328
3 Jeong KY, Park JW. Allergens of regional importance in Korea. Front Allergy. 2021 Mar 5;2:652275. 10.3389/falgy.2021.652275
4 Sousa L, Martín-Sierra C, Pereira C, Loureiro G, Tavares B, Pedreiro S, et al. Subcutaneous immunotherapy induces alterations in monocytes and dendritic cells homeostasis in allergic rhinitis patients. Allergy Asthma Clin Immunol. 2018 Nov 15;14:45. 10.1186/s13223-018-0271-8
5 Sohn MH. Efficacy and safety of subcutaneous allergen immunotherapy for allergic rhinitis. Allergy Asthma Immunol Res. 2018 Jan;10(1):1–3. 10.4168/aair.2018.10.1.1
6 Chang ML, Cui C, Liu YH, Pei LC, Shao B. Analysis of total immunoglobulin E and specific immunoglobulin E of 3,721 patients with allergic disease. Biomed Rep. 2015 Jul;3(4):573–7. 10.3892/br.2015.455
7 Yao H, Wang L, Zhou X, Jia X, Xiang Q, Zhang W. Predicting the therapeutic efficacy of AIT for asthma using clinical characteristics, serum allergen detection metrics, and machine learning techniques. Comp Biol Med. 2023 Nov;166:107544. 10.1016/j.compbiomed.2023.107544
8 Brożek JL, Bousquet J, Agache I, Agarwal A, Bachert C, Bosnic-Anticevich S, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. 2017 Oct;140(4):950–8.
9 Hao Q, Chen Z, Yin Y, Cao Y, Deng J. Efficacy of subcutaneous specific immunotherapy for allergic rhinitis combined with asthma: a retrospective analysis. Am J Transl Res. 2024 Oct 15;16(10):5933–42. 10.62347/JOAN8017
10 López JF, Bel Imam M, Satitsuksanoa P, Lems S, Yang M, Hwang YK, et al. Mechanisms and biomarkers of successful allergen-specific immunotherapy. Asia Pac Allergy. 2022 Oct 31;12(4):e45. 10.5415/apallergy.2022.12.e45
11 Weinfeld D, Westin U, Hellkvist L, Mellqvist UH, Jacobsson I, Cardell LO. A preseason booster prolongs the increase of allergen specific IgG4 levels, after basic allergen intralymphatic immunotherapy, against grass pollen seasonal allergy. Allergy Asthma Clin Immunol. 2020 Apr 28;16:31. 10.1186/s13223-020-00427-z
12 Penagos M, Eifan AO, Durham SR, Scadding GW. Duration of allergen immunotherapy for long-term efficacy in allergic rhinoconjunctivitis. Curr Treat Options Allergy. 2018;5(3):275–90. 10.1007/s40521-018-0176-2
13 Yeğit OO, Demir S, Ünal D, Olgaç M, Terzioğlu K, Eyice Karabacak D, et al. Adherence to subcutaneous immunotherapy with aeroallergens in real-life practice during the COVID-19 pandemic. Allergy. 2022 Jan;77(1):197–206. 10.1111/all.14876
14 Ren L, Wang C, Xi L, Gao Y, Zhang Y, Zhang L. Long-term efficacy of HDM-SCIT in pediatric and adult patients with allergic rhinitis. Allergy Asthma Clin Immunol. 2023 Mar 11;19(1):20. 10.1186/s13223-023-00781-8
15 Fritzsching B, Contoli M, Porsbjerg C, Buchs S, Larsen JR, Elliott L, et al. Long-term real-world effectiveness of allergy immunotherapy in patients with allergic rhinitis and asthma: Results from the REACT study, a retrospective cohort study. Lancet Reg Health Eur. 2021 Nov 30;13:100275. 10.1016/j.lanepe.2021.100275
16 Wang N, Song J, Sun SR, Zhu KZ, Li JX, Wang ZC, et al. Immune signatures predict response to house dust mite subcutaneous immunotherapy in patients with allergic rhinitis. Allergy. 2024 May;79(5):1230–41. 10.1111/all.16068
17 Di Lorenzo G, Mansueto P, Pacor ML, Rizzo M, Castello F, Martinelli N, et al. Evaluation of serum s-IgE/total IgE ratio in predicting clinical response to allergen-specific immunotherapy. J Allergy Clin Immunol. 2009 May;123(5):1103–10, 1110.e1–4. 10.1016/j.jaci.2009.02.012
18 Pascal M, Moreno C, Dávila I, Tabar AI, Bartra J, Labrador M, et al. Integration of in vitro allergy test results and ratio analysis for the diagnosis and treatment of allergic patients (INTEGRA). Clin Transl Allergy. 2021 Aug;11(7):e12052. 10.1002/clt2.12052
19 León B. Understanding the development of Th2 cell–driven allergic airway disease in early life. Front Allergy. 2023 Jan 10;3:1080153. 10.3389/falgy.2022.1080153
20 Akdis CA, Akdis M. Mechanisms of allergen–specific immunotherapy and immune tolerance to allergens. World Allergy Organ J. 2015 May 14;8(1):17. 10.1186/s40413-015-0063-2