
Download


Case REPORT
Anaphylaxis following a skin test with progesterone: A case report
Elif Nur Keklikoglua*, Can Tuzerb
aDermatology Department, Sultan Abdulhamid Han Training and Research Hospital, Istanbul, Turkey
bAdult Allergy and Immunology Department, Sultan Abdulhamid Han Training and Research Hospital, Istanbul, Türkiye
Abstract
Progestogen hypersensitivity is a broad spectrum of disorders that may present with cutaneous manifestations such as urticaria and eczema-like lesions, as well as systemic symptoms including anaphylaxis. Anaphylaxis due to progestogen hypersensitivity is very rare but should be considered in cases of recurrent anaphylaxis, particularly in young female patients. The timing of symptoms is the leading hint, as endogenous progesterone-induced reactions typically occur during the luteal phase of the menstrual cycle. Exogenous progesterone exposure, such as through oral contraceptives or assisted reproductive technologies (e.g., in vitro fertilization), has also been reported to trigger similar reactions. Therapeutic options include systemic corticosteroids, antihistamine tablets to control symptoms, and antihormone agents aiming the ovulation suppression. In refractory patients who are unresponsive to medical therapy, surgical options such as oophorectomy may be considered. In this report, a case of progesterone-associated anaphylaxis, triggered by an intradermal progesterone test, is presented, and a successful symptom control was achieved through the high-dose omalizumab treatment. As an alternative treatment option, omalizumab can be safely used in cases of progestogen hypersensitivity, especially in young female patients planning pregnancy.
Key words: anaphylaxis, omalizumab, progestogen hypersensitivity, urticaria
*Corresponding author: Elif Nur Keklikoglu, Dermatology Department, Sultan Abdulhamid Han Training and Research Hospital, Istanbul, Turkey. Email address: [email protected]
Received 5 July 2025; Accepted 13 October 2025; Available online 1 January 2026
Copyright: Keklikoglu EN and Tuzer C
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Progestogen hypersensitivity (PH) is a heterogeneous group of disorders characterized by cutaneous manifestations ranging from urticaria, angioedema, and eczematous skin lesions to erythema multiforme and anaphylaxis.1 In cases related to endogenous progesterone, recurrent cyclic cutaneous attacks and/or prolonged symptoms can be observed.2-4 Additionally, some procedures involving the use of exogenous progesterone, such as contraception and in vitro fertilization (IVF), have been reported to cause related symptoms.1 The symptoms triggered by endogenous progesterone typically begin in the twenties, whereas those related to exogenous exposure occur at older ages.5 In the first half of the menstrual cycle, known as the follicular phase, the oocyte matures and is released from the ovary following follicular rupture as a consequence of the estrogen peak. Progesterone secretion begins 24–48 h before ovulation and peaks in the mid-luteal phase.3 Therefore, in most patients sensitive to endogenous progesterone, the symptoms typically appear approximately 3−10 days before menstruation and resolve a few days after menses, following the decline in progesterone levels.1,6
Several diagnostic methods, such as skin prick tests, intradermal tests, and progesterone-specific immunoglobulin E (IgE) measurements, have been demonstrated.7,8 Finally, provocation tests are applied if the preceding methods yield insufficient evidence.9 Oral,9 intramuscular,10 and intravaginal11,12 routes are used. Gonadotropin-releasing hormone (GnRH) analogs, oral contraceptives, and tamoxifen are some radical treatment options. On the other hand, symptom-relieving medications such as antihistamines, systemic steroids, and omalizumab might be other options.6 In refractory cases, bilateral oophorectomy can be considered.13 All treatment modalities should be decided upon a conversation with the patient. Herein, we present the first case of anaphylaxis following an intradermal test procedure with progesterone and its response to an upgraded dose of omalizumab (450 mg per month).
Case Report
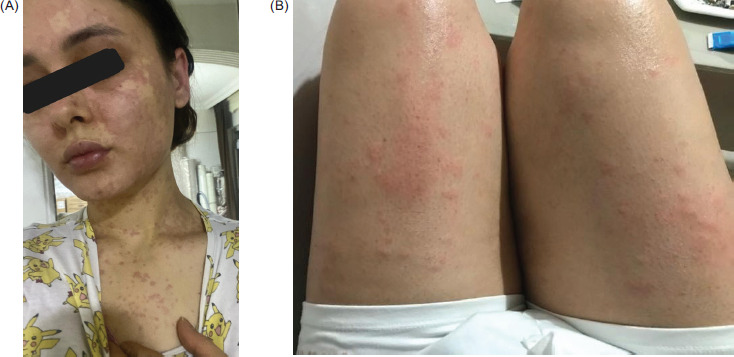
A 26-year-old female patient was referred to the Allergy and Immunology outpatient clinics because of recurrent generalized urticarial and angioedema attacks during the past 3 years. Over the last 4 months before admission, anaphylactic episodes characterized by severe bronchospasms following urticaria started to occur (Figures 1A and 1B). She had no other allergic or nonallergic comorbidities. No consistent history was present for any drug or food hypersensitivity reaction. No abnormalities were observed in the biochemical parameters or complete blood counts. Upon detailed questioning, it was learned that anaphylactic episodes occur approximately 1 week before the onset of menstruation, which corresponds to the mid-luteal phase.
Figure 1 Recurrent urticaria and angioedema attacks in the patient.
Serum progesterone level in the symptomatic phase (one week before menses) was detected as 15.9 μg/L. However, it was 1.07 μg/L in the asymptomatic period. A skin prick test and intradermal tests with progesterone were planned due to the possibility of PH. Skin prick test result (with 1/10 dilution of 50 mg/mL progesterone ampule) was negative. Additionally, intradermal tests were performed with dilutions of 1/1000, 1/100, and 1/10. At the 1/10 diluted concentration, it yielded a positive result (with widespread erythema and a 6 mm papule at the injection site) (Figure 2). The skin tests were also performed on five healthy controls for comparison, which were negative (Figure 3). We used 0.9% saline for the dilution.14 Twenty minutes after intradermal testing, the patient developed nausea, bronchospasm, respiratory distress, and syncope. Her blood pressure was 60–40 mmHg, and her pulse O2 saturation was 88%. Immediately, 0.5 mg epinephrine intramuscularly, 1 mg/kg methylprednisolone intravenously, and 45.5 mg pheniramine maleate were administered. The patient was stabilized and subsequently observed for 24 h. The serum tryptase level measured 20 min after the anaphylactic episode was 3.57 μg/L (0–11,4 μg/L), and the basal level (measured 24 h later) was 1.2 μg/L. A mutational analysis of the c-KIT gene was carried out, and no mutation was detected. Additionally, to exclude the possibility of estrogen-related dermatitis, both laboratory and skin tests were performed. Following a skin prick test with 1/10 dilution, intradermal skin testing with estradiol valerate, diluted with saline at concentrations of 1/1000, 1/100, and 1/10, yielded negative results (Figure 4). The serum estrogen level measured during the symptomatic period was 109 ng/L, which was not higher compared to the level of 125 ng/L taken during the asymptomatic period. Considering the onset time of anaphylactic episodes, a positive skin test result with progesterone and the recurrence of anaphylaxis following the skin test, the patient was diagnosed with progesterone-related anaphylaxis. Before the treatment, the 7-day-Urticaria activity score (UAS-7) was calculated as 37, and the Dermatological Life Quality Index (DLQI) score was calculated as 24. Owing to the lack of response to four doses of antihistamine therapy daily, 300 mg of omalizumab was initiated monthly at the beginning of the luteal phase. After 3 months, urticarial symptoms were alleviated, but dyspnea and angioedema attacks were not. UAS-7 and DLQI scores were improved to 21 and 19, respectively. However, it was not an adequate response, and the patient refused to take an antihormone therapy because of an infertility risk. Therefore, the omalizumab dose was increased, and at the 450 mg dose, we reached a full clinical response (no clinical symptoms and additional treatment for at least 6 months) when the injections were applied a few days before the mid-luteal phase. Following 6 months, the UAS-7 score was calculated as 0 and the DLQI score was 4. Therefore, we planned a lifelong treatment with high-dose omalizumab.
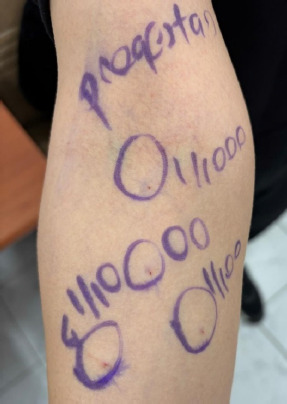
Figure 2 Intradermal tests with progesterone and 0.9% saline. Negative results were observed at 1/1000 and 1/100 dilutions, while a positive response was observed at 1/10 dilution.
Figure 3 Intradermal tests with progesterone yielded negative results in healthy controls.
Figure 4 Intradermal tests with estradiol valerate at 1/1000, 1/100, and 1/10 dilutions using saline resulted negative.
Discussion
The most distinguishing feature in this case was the recurrence of anaphylaxis after the skin test procedure. Besides being the first in this respect, the anaphylactic episodes were interestingly resolved after a high-dose anti-IgE treatment.
PH is also called “autoimmune progesterone dermatitis.” Indeed, the word “autoimmune” is a misnomer, and autoimmunity has not been demonstrated in its pathogenesis. Progesterone is thought to induce mast cell degranulation via an IgE-mediated mechanism. It is speculated that this condition relates to the cross-reactivity between the synthetic progesterone products in hormone therapies and endogenous progesterone.15 However, a significant proportion of cases occur in the absence of exogenous progesterone exposure. Estrogen, which is dominant in reproductive-aged women, stimulates T helper 2 (Th2) cells, inducing cytokine release and inhibiting B-cell apoptosis. These mechanisms create a Th2-dominant environment, which may lead to progesterone sensitivity and the production of progesterone-specific IgEs.1 The higher frequency of chronic spontaneous urticaria in women than in men might be due to sex hormone-related hypersensitivities. Cases of delayed-type (type IV) hypersensitivity associated with T-cell activity have also been reported.1,16,17 Patch testing or late reading of intradermal tests with progesterone can guide us in these cases.5,18
Owing to the variability of clinical symptoms and lack of standardized diagnostic criteria, PH may often be unrecognized. Some authors have proposed three diagnostic criteria: the presence of clinical manifestations compatible with PH, symptom onset in correlation with the menstrual cycle, and symptom resolution with ovulation inhibition.1 A low sensitivity for skin tests is shown in pH; a study reported that only 55% of patients had a positive skin test, and some patients with a positive skin test did not have a clinical history suggestive of type I hypersensitivity.19 Progesterone challenge by oral, intravaginal, or intramuscular can be performed in cases when the diagnosis is uncertain.9-12 In this patient, we did not skip to the challenge test since the patient experienced an anaphylaxis during the intradermal testing process, besides having a positive skin test result consistent with clinical history.
When planning a treatment, several factors, such as age, fertility desire, and symptom severity, should be considered. Tamoxifen therapy, an antiestrogen treatment modality that suppresses ovulation, has adverse effects on the menstrual cycle and bone metabolism. GnRH analogs also suppress estrogen, which leads to amenorrhea, hot flashes, a loss of libido, urogenital atrophy, and decreased bone mineralization.1 Thalidomide is rarely used because of its undesirable and toxic side effects.2 Bilateral oophorectomy can be considered in patients who are unwilling to become pregnant and unresponsive to other treatments, but it may lead to early menopause and premature osteoporosis. Although some cases have been treated with oral contraceptives, there is a possibility of disease exacerbation due to their progesterone content.20
An oral, intramuscular or intravaginal desensitization with progesterone can be performed. In cases requiring high-dose progesterone for IVF, rapid intramuscular desensitization protocols have been shown.21 These protocols should be performed in centers that are well equipped to manage anaphylaxis. Moreover, after a desensitization, an oral contraceptive or intravaginal progesterone is needed to maintain a stable progesterone level and prevent a resensitization.3
Omalizumab is a safe treatment option for young patients, especially those planning pregnancy. A review of seven randomized, placebo-controlled trials on chronic spontaneous urticaria found no significant difference in adverse events between omalizumab and placebo groups.22 A real-life study conducted in pregnant women showed that no adverse effects, pregnancy complications or congenital anomalies in infants were observed whilst omalizumab therapy.23 Omalizumab was efficacious even in refractory cases. A patient showed a good response to omalizumab therapy even after bilateral oophorectomy had failed to resolve symptoms.6 In another report, omalizumab was commenced for a progesterone-induced anaphylaxis in a 12-year-old girl, not without affecting her sexual development with antihormone therapies.24 Omalizumab can also be used as an adjuvant therapy before a risky desensitization to progesterone.25,26 In this patient, if high-dose omalizumab treatment had resulted in an inadequate clinical response, a rapid desensitization protocol following premedication with omalizumab would have been planned.
If the goal is symptom control, nonhormonal medical treatments, including antihistamines, systemic steroids and omalizumab, are preferred. Because the patient was young and currently planning a pregnancy, omalizumab therapy was initiated. In fertile women who do not respond to nonhormonal medical treatments, a desensitization may be considered. Although desensitization regimens have been studied in a few cases, successful outcomes have been shown.27 Healthy pregnancies and live births have been reported in patients desensitized to progesterone as well as those treated with omalizumab.5
Conclusion
Progestogen hypersensitivity (pH) should be considered in women with recurrent cutaneous symptoms and/or anaphylactic episodes during the mid-luteal phase. In the present case, a desensitization to progesterone might be so challenging, and the patient was reluctant. Regarding the existing literature, high-dose omalizumab therapy was the most appropriate treatment option for this patient. As in the present case, treatment modalities should be individualized, considering the patient’s clinical presentation and desire for fertility.
Author Contributions
All authors contributed equally to this article.
Conflicts of Interest
The authors had no relevant financial interests to disclose.
Funding
None.
REFERENCES
1 Chiarella SE, Buchheit KM, Foer D. Progestogen hypersensitivity. J Allergy Clin Immunol Pract. 2023;11(12):3606–3613 e2. 10.1016/j.jaip.2023.07.050
2 Snyde JL, Krishnaswamy G. Autoimmune progesterone dermatitis and its manifestation as anaphylaxis: A case report and literature review. Ann Allergy Asthma Immunol. 2003;90(5):469–77; quiz 477, 571. 10.1016/S1081-1206(10)61838-8
3 Buchheit KM, Bernstein JA. Progestogen hypersensitivity: Heterogeneous manifestations with a common trigger. J Allergy Clin Immunol Pract. 2017;5(3):566–74. 10.1016/j.jaip.2017.01.019
4 Aghazadeh N, Chattha AJ, Hartz MF, Davis DMR. Autoimmune progesterone dermatitis in the adolescent population. Pediatr Dermatol. 2021;38(2):380–4. 10.1111/pde.14423
5 Xu G, Yuson R, Rafferty M, Thai TL, Limaye S. Progestogen hypersensitivity: Successful use of progesterone desensitisation and omalizumab to facilitate in vitro fertilisation. Intern Med J. 2024;54(10):1749–52. 10.1111/imj.16517
6 Varghese A, Paul T, Kim H, Van Uum S, Vadas P, Azzola A. Effect of omalizumab for autoimmune progesterone dermatitis refractory to bilateral oophorectomy: A case report. Allergy Asthma Clin Immunol. 2021;17(1):58. 10.1186/s13223-021-00561-2
7 Dhaliwal G, Batra J, Ankireddypalli AR, Gorle S, Kanugula AK, Kaur J. Progesterone hypersensitivity induced by exogenous progesterone exposure. Cureus. 2023;15(9):e44776. 10.7759/cureus.44776
8 Ghosh D, Bernstein JA. Development of a progesterone-specific IgE assay for diagnosing patients with suspected progestogen hypersensitivity. Ann Allergy Asthma Immunol. 2019;122(6):616–22. 10.1016/j.anai.2019.03.032
9 Ljubojevic Hadzavdic S, Kulišić SM, Grgec DL, Poljanac A, Ilić B. Autoimmune progesterone dermatitis diagnosed by lymphocyte transformation test and progesterone provocation test. Acta Dermatovenerol Croat. 2018;26(3):276–7.
10 Oskay T, Kutluay L, Kaptanoğlu A, Karabacak O. Autoimmune progesterone dermatitis. Eur J Dermatol. 2002;12(6):589–91.
11 Le K, Wood G. A case of autoimmune progesterone dermatitis diagnosed by progesterone pessary. Australas J Dermatol. 2011;52(2):139–41. 10.1111/j.1440-0960.2011.00753.x
12 Nemeth H, Kovács E, Gödény S, Simics E, Pfliegler G. Autoimmune progesterone dermatitis diagnosed by intravaginal progesterone provocation in a hysterectomised woman. Gynecol Endocrinol. 2009;25(6):410–2. 10.1080/09513590902770164
13 Medeiros S, Rodrigues-Alves R, Costa M, Afonso A, Rodrigues A, Cardoso J. Autoimmune progesterone dermatitis: Treatment with oophorectomy. Clin Exp Dermatol. 2010;35(3):e12–3. 10.1111/j.1365-2230.2009.03217.x
14 Aksoy FÇ, Evans SE, Karaduman A. Otoimmün progesteron dermatiti: Olgu sunumu ve literatürün g özden geçirilmesi. Arch Turk Dermatol Venerol Turkderm. 2009;43(3):122–5.
15 Kasperska-Zajac A, Brzoza Z, Rogala B. Sex hormones and urticaria. J Dermatol Sci. 2008;52(2):79–86. 10.1016/j.jdermsci.2008.04.002
16 Li RC, Buchheit KM, Bernstein JA. Progestogen hypersensitivity. Curr Allergy Asthma Rep. 2018;18(1):1. 10.1007/s11882-018-0758-x
17 Foer D, Buchheit KM. Progestogen hypersensitivity: An evidence-based approach to diagnosis and management in clinical practice. Immunol Allergy Clin North Am. 2017;37(4):773–84. 10.1016/j.iac.2017.07.006
18 Stranahan D, Rausch D, Deng A, Gaspari A. The role of intradermal skin testing and patch testing in the diagnosis of autoimmune progesterone dermatitis. Dermatitis. 2006;17(1):39–42. 10.2310/6620.2006.05045
19 Foer D, Tran LK, Wickner P, Castells M, Marquis KA, Buchheit KM. Challenges in skin testing for progestogen hypersensitivity. Ann Allergy Asthma Immunol. 2021;126(1):100–2. 10.1016/j.anai.2020.09.002
20 Toms-Whittle LM, John LH, Griffiths DJ, Buckley DA. Autoimmune progesterone dermatitis: A diagnosis easily missed. Clin Exp Dermatol. 2011;36(4):378–80. 10.1111/j.1365-2230.2010.03979.x
21 Foer D, Buchheit KM, Gargiulo AR, Lynch DM, Castells M, Wickner PG. Progestogen hypersensitivity in 24 cases: Diagnosis, management, and proposed renaming and classification. J Allergy Clin Immunol Pract. 2016;4(4):723–9. 10.1016/j.jaip.2016.03.003
22 Pongdee T, Li JT. Omalizumab safety concerns. J Allergy Clin Immunol. 2025;155(1):31–5. 10.1016/j.jaci.2024.11.005
23 Patruno C, Guarneri F, Nettis E, Bonzano L, Filippi F, Ribero S, et al. Safety of omalizumab in chronic urticaria during pregnancy: A real-life study. Clin Exp Dermatol. 2024;49(4):344–7. 10.1093/ced/llad386
24 Heffler E, Fichera S, Nicolosi G, Crimi N. Anaphylaxis due to progesterone hypersensitivity successfully treated with omalizumab. J Allergy Clin Immunol Pract. 2017;5(3):852–4. 10.1016/j.jaip.2017.01.003
25 Gadoury-Levesque V, Bernstein J. A case of refractory recurrent cyclical angioedema and urticaria successfully treated with multiple steps therapy. Annals Allergy Asthma Immunol. 2018;121(5):S85. 10.1016/j.anai.2018.09.276
26 Lavery WJ, Bernstein JA. Cyclical hypersensitivity, anaphylaxis, and related hormonal reaction. Ann Allergy Asthma Immunol. 2019;122(2):140–7. 10.1016/j.anai.2018.11.016
27 Prieto-Garcia A, Sloane DE, Gargiulo AR, Feldweg AM, Castells M. Autoimmune progesterone dermatitis: Clinical presentation and management with progesterone desensitization for successful in vitro fertilization. Fertil Steril. 2011;95(3):1121 e9–13. 10.1016/j.fertnstert.2010.10.038