
Download
ORIGINAL ARTICLE
Diagnostic outcomes and temporal changes in skin tests and specific immunoglobulin E levels following Hymenoptera sting reactions: single-center analysis of 194 patients
Leyla Çevirme, Güzin Özden*, Susamber Dik, Merve Erkoç, Hakan Basır, Reyhan Sevil Cansunar
Division of Immunology and Allergy Diseases, Adana City Training and Research Hospital, Yüreğir, Adana, Turkey
Abstract
Hymenoptera stings are a common occurrence worldwide, with a significant proportion of the general population experiencing at least one sting during their lifetime. The order Hymenoptera includes several species, such as honey bees, hornets, bumblebees, and yellow jackets, that cause hypersensitivity reactions. The most common form of hypersensitivity is systemic sting reaction mediated by specific immunoglobulin E (sIgE) to venom components. The prevalence of systemic sting reaction in the general population is estimated to be approximately 3%, while gross local reactions are reported in 2.4–26.4% of individuals, with higher proportions in beekeepers. Identification of the offender insect is crucial for proper diagnosis and treatment, but many patients are unable to correctly distinguish the responsible venom. Standard diagnostic tools, such as intradermal testing and Hymenoptera venom sIgE tests, play an important role in determining venom sensitivity. However, cross-reactivity between different venoms makes accurate identification difficult. In this study, we aim to analyze the clinical history of patients with Hymenoptera venom hypersensitivity and evaluate the diagnostic approach. Understanding these factors is important to improve diagnostic accuracy and optimize patient management. Further research is needed to improve diagnostic tools and develop personalized treatment strategies to reduce the risk of severe allergic reactions in susceptible individuals. Our study suggests that diagnostic tests should be performed rapidly in reactions that develop after an Apis sting, especially due to the significant decrease in Apis sIgE levels.
Key words: Apis-specific IgE, Hymenoptera, IDT, systemic sting reacion, venom skin test, vespula
*Corresponding author: Güzin Özden, MD, Division of Immunology and Allergy, Adana City Training and Research Hospital, Yüreğir, Adana 01370, Turkey. Email address: [email protected]
Received 28 May 2025; Accepted 21 August 2025; Available online 1 January 2026
Copyright: Çevirme L, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
The Hymenoptera order encompasses more than 100,000 known species of insects worldwide, and insect sting are very common in these species.1 Hymenoptera venom allergy is a potentially life-threatening allergic reaction that occurs after a venom sting. Up to 3% of the general population may develop systemic sting reaction (SSR) after a venom sting during their lifetime2 The order Hymenoptera consists of the family Apidae, consisting of the species Apis mellifera (honey bees) and Bombus (wasps), while the family Vespidae consists of subfamilies Vespinae (three genera: Vespa [hornets], Dolicho-Vespula [wasps], Vespula [wasps or yellow jackets]), and Polistinae (one genus: Polistes, the wasps).3 The most common form of hypersensitivity to Hymenoptera stings is SSR. The reaction is mediated by specific immunoglobulin E (sIgE) to components of the Hymenoptera venom. Clinical manifestations include generalized skin reactions (flushing, urticaria, and angioedema) and mild-to-moderate respiratory, cardiovascular, or gastrointestinal manifestations. Occasionally, severe manifestations, such as severe airway obstruction, anaphylactic shock (often with loss of consciousness), and respiratory/circulatory arrest, may occur.2 Another clinical finding is the large local reaction (LLR). This is defined as a swelling of >10 cm in diameter that lastS for more than 24 h.3 Approximately 80% of LLRs have a swelling diameter of 10–20 cm, and others have a swelling diameter of >20 cm. LLRs heal in approximately 7 days (range 1–21 days).4 Bee venom studies have shown that approximately 3% of the general population in the United States5 and Europe6 have SSR from Hymenoptera stings. The frequency of LLRs has been reported to range from 2.4% to 26.4% but is as high as 38% in beekeepers; both clinical presentations depend on the population studied and the methodology used.2,6 Better diagnostic tests are needed because most patients cannot distinguish the type of venom causing SSR.7 İntradermal tests (IDT) and Hymenoptera venom (HV) sIgE indications to the perpetrator insect depend largely on the patient’s history. In our study, we aimed to discuss the clinical history, diagnostic approach, and compatibility/incompatibility of cross-reactions between different types of venoms.
Materials and Methods
Study design and data collection
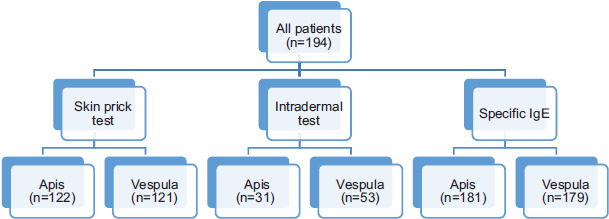
The case history of 194 patients who applied to the allergy and immunology outpatient clinic of Adana City Hospital, Adana, Türkiye, between January 01, 2018 and May 01, 2024 were reviewed retrospectively. Age, gender, place of residence, atopy, comorbidities, medications used, and whether they were beekeepers or not were recorded. In addition, the type of bee that stung them was noted based on the patient’s history. Clinical manifestations of the patient after bee sting, emergency room visits, and treatments they received were also noted. Skin prick tests (SPTs) and IDT performed on the patients and HV sIgE values were recorded. HV sIgE positivity was determined by ThermoFisher Scientific ImmunoCAP. The classification in this method is as follows: class 0: <0,35 kilo units per liter (kU/L) (no allergy), class 1: 0.35–0.7 kU/L (low positive allergy), class 2: 0.70–3.5 kU/L (positive allergy), class 3: 3.50–17.5 kU/L (strong positive allergy), class 4: 17.5–50 kU/L (high positive allergy), class 5: 50–100 kU/L (very high positive allergy), and class 6: ≥100 kU/L (extremely positive allergy). According to this classification, values ≥ 0.35 kU/L are positive and <0.35 kU/L are negative.8 SPTs were performed with Apis and Vespula venoms, positive and negative controls. Histamine 10,000 mL was used as a positive control and 0.09% sodium isotonic was used as a negative control. For SPT >3 mm from the negative control was accepted as a positive test result. IDT was performed with 0.02–0.05-mL injection, which created a 2–3-mm blep/induration on the skin. Patients with induration larger than the injected diameter were accepted as positive. IDT is more sensitive than SPTs. SPT with venom concentrations of 10 µg/mL, 100 µg/mL.9 IDTs are usually performed with concentrations of 0.1 µg/mL and 1.0 µg/mL in children and with concentrations of 0.001 µg/mL and 0.01 µg/mL in adults.8 If there is no reaction with SPT, IDT is performed with doses of 0.001 µg/mL in children and 0.01 µg/mL in adults. Skin tests are performed at least 4–6 weeks after the Hymenoptera sting to exclude false negatives. Diagnostic tests included in the study are shown in Figure 1.
Figure 1 Diagnostic tests included in the study.
The study was planned and conducted in accordance with the principles of the Declaration of Helsinki. Approval was obtained from the Adana City Hospital Ethics Committee on May 30, 2024 (Meeting No.: 1, Decision No.: 7). The Ethics Committee of Adana City Hospital waived the need for patient approval and/or informed consent because of the study’s retrospective nature.
Statistical analysis
Statistical analyses were performed using the Jamovi software (The Jamovi Project, version 2.3, 2022). Descriptive statistics were presented as mean ± standard deviation (SD) for continuous variables, and as frequencies and percentages for categorical variables.
Comparisons between categorical variables (e.g., reaction type, diagnostic test positivity according to bee species, and reaction categories) were performed using the Chi-square test or Fisher’s exact test when expected cell counts were <5. Continuous variables were compared using the independent samples t-test for normally distributed data or the Mann–Whitney U test for non-normally distributed data.
The effect of time interval between allergic reaction and admission to the clinic (≤6 months vs. ≥6 months) for skin test and venom sIgE positivity was evaluated using Chi-square or Fisher’s exact test for categorical outcomes and independent samples t-test or Mann–Whitney U test for continuous variables; P <0.05 was considered statistically significant.
Results
The mean age of 194 patients included in the study at the time of inclusion was 42.18±14.14 years, and 52% of the patients were males. In all, 72% (n = 88) of the patients lived in urban areas, and the rate of beekeeping was 12% (n = 17). Demographic and clinical characteristics of the patients are given in Table 1. The rate of anaphylaxis in patients was 73.7% (n = 143) and the rate of emergency room admission was 95.7% (n = 141). Adrenaline was administered to 61.6% (n = 61) of the patients. Reaction characteristics and treatments received are included in Table 2. While 97.4% (n = 139) of the patients experiencing anaphylaxis were admitted to the emergency department, adrenaline was administered to 71.1% (n = 101) patients.
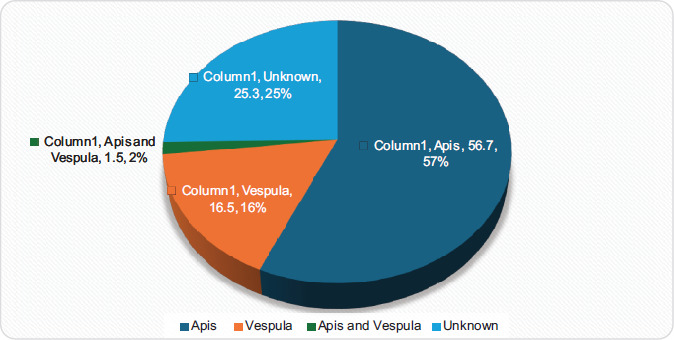
The most common suspected bee species observed in patient histories is Apis, and the others are listed in Figure 2.
Table 1 Demographic and clinical characteristics of patients.
| Age, years mean±SD (n =194) | 42.18±14.14 |
| Gender n (%) | 194 (100) |
| Male/Female | 101 (52.1%)/93 (47.9%) |
| Place of residence (n =122) n (%) | |
| Rural | 34 (27.9%) |
| Urban | 88 (72.1%) |
| Family history of venom allergy (n = 89) n (%) | 10 (11.2%) |
| Beekeeping (n = 141) n (%) | 17 (12.1%) |
| Atopy (n = 172) n (%) | 83 (48.3%) |
| Comorbid disease (n = 190) n (%) | |
| Diabetes mellitus | 17 (8.9%) |
| Hypertension | 16 (8.4%) |
| Atherosclerotic heart disease | 2 (1.1) |
| Medication (n = 190) n (%) | |
| ACEi | 4 (2.1%) |
| Beta blocker | 6 (3.2%) |
SD: standard deviation; ACEi: angiotensin-converting enzyme inhibitör.
Table 2 Reaction characteristics and treatments received.
| Reaction type (n = 194) n (%) | |
| Large local reaction | 9 (4.6%) |
| Generalized urticaria | 42 (21.6%) |
| Anaphylaxis | 143 (73.7%) |
| Urgent administration (n = 141) n (%) | 135 (95.7%) |
| Treatments received (n = 99) n (%) | |
| Antihistamine | 2 (2.0%) |
| Antihistamines and steroids | 34 (34.3%) |
| Antihistamine, steroids, and adrenaline | 61 (61.6%) |
| None | 2 (2.0%) |
Figure 2 Suspicious bee species.
While 85.5% (n = 94) of the patients who described reactions to Apis were diagnosed with SPT and/or Apis sIgE, 78.1% (n = 25) of the patients who described reactions to vespula were diagnosed with SPT and/or vespula sIgE. There were three patients with a history of both Apis and Vespula; one of them had only Apis, one had vespula, and the other had both Apis and Vespula sensitivity. In all, 56% (n = 110) of the stings were from honey bees and 16% (n = 32) from wasps. Among patients who could not identify bee species, 61.2% (n = 30) had Apis sensitivity and 51% (n = 25) had Vespula sensitivity. SPT and sIgE positivity according to bee species in the history are shown in Table 3. Reaction to the bee venom reported in the history was confirmed by skin tests (SPT with or without IDT) and/or sIgE in 82.6% (n = 95) of anaphylaxis cases, 81.5% (n = 22) of generalized urticaria cases, and 100% (n = 3) of extensive local reactions. Skin tests and sIgE positivity according to reaction types are shown in Table 4. The time that patients with an allergic recation to HV took to apply to the clinic differed. The tests were performed in the first week of the patient’s first visit to clinic. The patients were grouped as those who applied in ≤6 months and those who applied in ≥6 months. In these two groups, skin tests and sIgE results were examined for both Apis and Vespula types. In case of patients who applied after 6 months, a statistically significant decrease was found only in the Apis sIgE arm. There was also a decrease in Vespula sIgE, but it was not statistically significant. In both bee groups, skin test negativity was higher in patients who applied after 6 months, but it was not statistically significant.
Table 3 Reaction type, SPT, IDT, and specific IgE positivity according to bee species in the history.
| Apis (n = 110) | Vespula (n = 32) | Both (n = 3) | Unknown (n = 49) | |
|---|---|---|---|---|
| Reaction type, n/n (%) | ||||
| Large local reaction | 2/110 (1.8%) | 1/32 (3.1%) | 0/3 (0.0%) | 6/49 (12.2%) |
| Generalized urticaria | 22/110 (20.0%) | 5/32 (15.6%) | 0/3 (0.0%) | 15/49 (30.6%) |
| Anaphylaxis | 86/110 (78.2%) | 26/32 (81.3%) | 3/3 (100.0%) | 28/49 (57.1%) |
| Apis positivity, n/n (%) | ||||
| SPT | 50/68 (73.5%) | 8/22 (36.4%) | 1/2 (50.0%) | 11/30 (36.7%) |
| IDT | 2/13 (15.4%) | 3/9 (33.3%) | 0/1 (0.0%) | 0/8 (0.0%) |
| Specific IgE | 79/103 (76.7%) | 14/29 (48.3%) | 1/3 (33.3%) | 24/46 (52.2%) |
| ST and/or specific IgE | 94/110 (85.5%) | 22/32 (68.8%) | 2/3 (66.7%) | 30/49 (61.2%) |
| Vespula positivity, n/n (%) | ||||
| SPT | 11/67 (16.4%) | 9/22 (40.9%) | 0/2 (0.0%) | 5/30 (16.7%) |
| IDT | 0/29 (0.0%) | 0/12 (0.0%) | 0/1 (0.0%) | 1/11 (9.1%) |
| Specific IgE | 41/102 (40.2%) | 20/29 (69.0%) | 2/3 (66.7%) | 24/45 (53.3%) |
| ST and/or specific IgE | 45/110 (40.9%) | 25/32 (78.1%) | 2/3 (66.7%) | 25/49 (51.0%) |
Ig: immunoglobulin; SPT: skin prick test; IDT: ıntradermal test; ST: skin test.
Table 4 SPT, IDT, and specific IgE positivity according to reaction types.
| Large local reaction (n = 9) | Generalized urticarial (n = 42) | Anaphylaxis (n = 143) | |
|---|---|---|---|
| Apis positivity | |||
| SPT | 3/6 (50.0%) | 17/36 (47.2%) | 50/80 (62.5%) |
| IDT | 1/2 (50.0%) | 0/7 (0.0%) | 4/22 (18.2%) |
| Specific IgE | 3/8 (37.5%) | 22/37 (59.5%) | 93/136 (68.4%) |
| ST and/or specific IgE | 6/9 (66.7%) | 31/42 (73.8%) | 111/143 (77.6%) |
| Vespula positivity | |||
| SPT | 0/6 (0.0%) | 8/35 (22.9%) | 17/80 (21.3%) |
| IDT | 0/4 (0.0%) | 1/11 (9.1%) | 0/38 (0.0%) |
| Specific IgE | 4/8 (50.0%) | 21/37 (56.8%) | 62/134 (46.3%) |
| ST and/or specific IgE | 4/9 (44.4%) | 23/42 (54.8%) | 70/143 (49.0%) |
| Verification of bee in the story | 3/3 (100.0%) | 22/27 (81.5%) | 95/115 (82.6%) |
Ig: ımmunoglobulin; SPT: skin prick test; IDT: ıntradermal test; ST: skin test.
Discussion
In this study, we present patients with a history of venom allergy, including 194 patients, in more than half of whom the suspected species was Apis. Three-quarters of the reactions were anaphylaxis, and almost all of the patients went to the emergency room.
The goal of diagnosing venom allergy is to classify the severity of SSR and assess individual patient’s risk of anaphylaxis. If venom immunotherapy is indicated based on the history of SSR from an insect sting, IgE-mediated HV sensitization must be demonstrated. In addition, the perpetrator insect must be identified based on history and test results. HV sIgE can be detected in serum in ~40% of the total population. Only a fraction of these cases have evidence of true pathogenic, that is allergic, reactions.10–13
Factors that increase exposure to bee stings include beekeeping, families of beekeepers, and intensive outdoor activities (two variables). In our study, only 17 patients were beekeepers. The number of male patients was predominant, which may be attributed to male jobs that require more outdoor activities. In all, 11% of the patients had a family history of bee venom stings. The demographic characteristics in our study were consistent with the literature.13,14 Although those living in rural areas are at a risk of stings, the majority of our patients (72%) lived in urban areas. This could be explained by the fact that urbanities more potentially contacted us.
Better diagnostic tests are needed because most patients are not able to distinguish the venom causing SSR.7 IDT and HV sIgE are the best available tests. One study found significant discrepancies between skin tests and sIgE in both patient and control groups. Again, this study found that HV sIgE was a test with higher sensitivity but lower specificity. It was found that using HV sIgE as the initial diagnostic test would result in fewer IDTs. However, as is known, combining both tests would help to detect missed or double-positive cases. It was of concern that a group of patients had a history of SSR despite having a negative skin test.15
In our study, 85.5% of the patients who described reactions to Apis were diagnosed with skin tests and/or Apis sIgE, and 78.1% of the patients who described reactions to Vespula were diagnosed with skin tests and/or vespula sIgE. There were three patients with a history of both Apis and Vespula; one had only Apis, one had Vespula, and the other had both Apis and Vespula sensitization. One-fourth of the patients could not determine the bee species, and 61.2% of these patients had Apis sensitivity and 51% had Vespula sensitivity. Owing to hospital conditions, transportation, individual patient’s problems, and the COVID-19 pandemic, we could not perform skin tests and sIgE levels on all patients at the same time. However, it was observed that our diagnosis rate with both tests was still quite high. There may be incompatibilities between sIgE and IDT, but they are thought to be complementary tests. sIgE is recommended as the initial test and IDT as a complementary test.15 During follow-up, only skin tests for HV were performed, which were negative, and with this approach all possible sensitivities were determined. Similarly, we tested the sIgE levels in 76.7% of the patients with a history of Apis stings and 69% of those with a history of Vespula stings.
Some studies have shown that patients with a history of Hymenoptera stings with negative skin tests may experience SSR again upon subsequent exposure to Hymenoptera venom.9 In addition, the limited diagnostic accuracy of IDT is indicated by the fact that skin test results may be positive despite the absence of a sting history. Despite this, skin test is still considered the most reliable testing method. It is generally recommended over in vitro testing for initial evaluation.5
Although the study done by Golden et al.5 recommended performing a skin test first, the proportion of HV sIgE tests in our study was quite high. In another study.16 HV sIgE tests was recommended as the first diagnostic testing method. In our study, 122 patients underwent SPT with Apis and 121 patients underwent SPT with Vespula. In addition, the number of patients who underwent IDT with Apis was 31 and with Vespula 53. In all, 181 patients underwent Apis sIgE and 179 patients underwent Vespula sIgE. We used both skin tests and HV sIgE level as diagnostic tests. Our sIgE tests were found to be compatible with the clinical presentations of the patients.
There is a weak correlation between the venom concentration that has a positive result in IDT or HV sIgE levels and severity of the reaction.5 In patients with a history of anaphylaxis, the rate of detecting positivity in skin tests and/or HV sIgE for Apis was found to be higher. In contrast, in the group with a history of Vespula stings, the positivity rate of the tests was higher in those with a history of LLRs. However, the number of patients in each clinical group was not equal or balanced. We can only state that there was a clinical correlation consistent with the literature in the group with anaphylaxis resulting from Apis stings.
In patients without anaphylaxis, allergy testing is not indicated and is generally not recommended. In patients with multiple insect bite poisoning history, allergy testing is not recommended because it may not yield clear results and may cause confusion if it is not clinically significant. Exceptions may be made at the discretion of the clinician if it is necessary to identify bee or Vespid venom in addition to a history of anaphylaxis.2 Of our patients, 143 had anaphylaxis. Of these anaphylactic patients, 111 (77%) had positive Apis skin test and/or sIgE and 70 (49%) had positive Vespula skin test and/or sIgE. Of the 115 patients presenting with anaphylaxis, 95 had positive skin test and/or sIgE consistent with the history.
In our study, atopy was detected at a proportion of 48%. This was confirmed using clinical findings, total IgE levels, inhalation SPT, and Phadiatop test. Although atopy cannot be determined by considering total IgE elevation alone, it has been shown that patients with high total IgE levels are clinically more susceptible to Hymenoptera stings.17 Considering the significant atopy proportion detected in our study, we can reach a similar conclusion.
In patients experiencing systemic reactions because of Hymenoptera stings, dual positivity between Vespula and Apis Mellifera is common.18 The cross-reactive component responsible for this dual sensitization is hyaluronidase.1,19 Current diagnostic tests may be insufficient to differentiate between asymptomatic sensitization and clinically significant allergy. Therefore, it may be necessary to evaluate cross-reactive carbohydrate determinants (CCDs).3 The detection of skin test and sIgE positivity for a bee species other than the one found in the patient’s history suggests a possible cross-reactivity. In our patients who had allergic reactions to Apis stings, skin test and/or sIgE were 85% positive for Apis and 40% positive for Vespula, indicating cross-reactivity. However, we could not perform CCD testing because it was difficult to access and was not included in routine tests.
It is recommended to measure HV sIgE levels shortly after the patient’s first sting occurrence, even if it is soon after the incident. If the result is negative, the measurement should be repeated approximately 2–6 weeks after the sting. In this case, a significant change in HV sIgE concentration may help indicate previous allergen exposure and the specific type of venom involved.20,21 If the patient presents after >2 weeks of the sting reaction, it is recommended to perform the tests as soon as possible. This is because HV sIgE levels may decrease rapidly to some extent depending on individual’s atopic status.22,23 In both Apis and Vespula groups, patients who presented after 6 months showed lower positivity rates in skin tests and a decline in sIgE levels. However, the only statistically significant finding was the decrease in Apis sIgE levels. Studies have shown that individual conditions can influence the proportion of decline in HV sIgE levels, which may decrease either rapidly or slowly. In our study, we also observed findings consistent with this, particularly in Apis sIgE level.
Studies have demonstrated that patients stung by wasp species are more likely to experience severe reactions.21 In contrast, our study found that although the number of patients in the Apis and Vespula groups was similar, the proportion of anaphylaxis was higher in those stung by Apis. Among patients with anaphylaxis, the positivity proportion for Apis was 77%, compared to 49% for Vespula.
Patients whose first sting reaction is severe anaphylaxis need more aggressive treatment. This is because such reactions may indicate a higher risk of more severe outcomes in subsequent or re-sting events.22 In our study, 95% of the patients visited the emergency department, 61% received adrenaline treatment. This finding highlights the low rate of adrenaline administration among patients presenting to healthcare facilities. Additionally, 42 patients who visited the emergency department were excluded from these proportions because they could not recall the treatment they had received, and their medical records were inaccessible.
In Turkey, the lifetime incidence of sting exposure has been estimated as 94.5%, the systemic reaction proportion as 7.5%, and the serious systemic reaction proportion as 2.2%. In Turkey, Hymenoptera stings, reported most frequently, are caused by the honey bee (Apis mellifera) and the Vespid (Vespula vulgaris).23 Patients should undergo a diagnostic evaluation to determine the species of the perpetrator insect, plan treatment, and educate patients about avoidance measures. Detailed and careful questioning can usually establish the diagnosis of a Hymenoptera sting reaction. However, to identify the responsible species, sensitivity should be confirmed by a skin test reaction to the venom or detection of venom sIgE antibodies, as recall bias may occur.21
The results of our study were consistent with the data of our country. In our study, the most frequent sting reaction results were with Apis and Vespula, and Hymenoptera types were confirmed with skin tests and/or sIgE. We performed a considerable amount of diagnostic tests. We detected a history of anaphylaxis at a proportion of 73% and this was much higher than the results of our country. The possible reason for this could be the seasonal rural living culture and more intensive gardening work in the region.
The first limitation of our study was that there was missing information in histories because ours was a retrospective study. The second limitation was that twe could not perform skin testing and sIgE on all patients. The third limitation was that we could not distinguish cross-reactions because we did not perform CCD.
Conclusions
It was observed that the most common perpetrator species of bee sting were Apis and Vespula, and Hymenoptera types were confirmed by skin tests and/or sIgE. Adding skin tests to the evaluation along with sIgE for the perpetrator bee increased the proportion of diagnosis. According to the history files in our study, skin tests performed after 6 months were negative, with decreased levels of HV sIgE. Performance of these diagnostic procedures is as important as the methods used. Determining the HV that caused allergic reaction is very important for a successful treatment.
Informed Consent Statement
This study is retrospective. No additional tests were requested from the patients for the study. No procedures were performed on the patients without their consent.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Author’s Contribution
Leyla Çevirme and Güzin Özden contributed to the design and concept of the study. Leyla Çevirme and Susamber Dik carried out data collection. Leyla Çevirme and Merve Erkoç performed statistical analyses and data interpretation. Leyla Çevirme, Reyhan Sevil Cansunar, and Güzin Özden drafted the manuscript. Leyla Çevirme, Hakan Basır, Güzin Özden, and Merve Erkoç checked the final manuscript and revised it critically. All authors read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declared no conflict of interest.
Funding
This research received no external funding.
REFERENCES
1 Sturm GJ, et al. EAACI guidelines on allergen immunotherapy: Hymenoptera venom allergy. Allergy. 2018, April;73(4):744–64. 10.1111/all.13262
2 Ruëff F. et al. Diagnosis and treatment of Hymenoptera venom allergy: S2k Guideline of the German Society of Allergology and Clinical Immunology (DGAKI) in collaboration with the Arbeitsgemeinschaft für Berufs-und Umweltdermatologie e.V. (ABD), the Medical Association of German Allergologists (AeDA), the German Society of Dermatology (DDG), the German Society of Oto-Rhino-Laryngology, Head and Neck Surgery (DGHNOKC), the German Society of Pediatrics and Adolescent Medicine (DGKJ), the Society for Pediatric Allergy and Environmental Medicine (GPA), German Respiratory Society (DGP), and the Austrian Society for Allergy and Immunology (ÖGAI). Allergol Select. 2023; 7:154–90. 10.5414/ALX02430E.
3 Arif F, Williams M. Hymenoptera stings [Internet]. İn StatPearls. Treasure Island, FL: StatPearls Publishing, 2025. Available from: http://www.ncbi.nlm.nih.gov/books/NBK518972/ Accessed: Aug 19, 2025.
4 Tripolt P, Arzt-Gradwohl L, Čerpes U, Laipold K, Binder B, Sturm GJ. Large local reactions and systemic reactions to insect stings: Similarities and differences. PLoS ONE. 2020, April;15(4):e0231747. 10.1371/journal.pone.0231747
5 Golden DBK. et al. Stinging insect hypersensitivity: A practice parameter update 2016. Ann Allergy Asthma Immunol. 2017, January;118(1):28–54. 10.1016/j.anai.2016.10.031
6 Bilò BM and Bonifazi F. Epidemiology of insect-venom anaphylaxis, Curr Opinion Allergy Clin Immunol. 2008, August;8(4):330–37. 10.1097/ACI.0b013e32830638c5
7 Baker TW, Forester JP, Johnson ML, Stolfi A, Stahl MC. The HIT study: Hymenoptera ıdentification test—How accurate are people at identifying stinging insects? Ann Allergy Asthma Immunol. 2014;113(3):267–70. 10.1016/j.anai.2014.05.029
8 Park KH, Lee J, Sim DW, Lee SC. Comparison of Singleplex specific IgE detection ımmunoassays: ImmunoCAP Phadia 250 and Immulite 2000 3g allergy. Ann Lab Med. 2018;38(1):23–31. 10.3343/alm.2018.38.1.23
9 Wang Q, Watson NL, Beakes DE Schwartz DJ. Hymenoptera venom skin testing: Adopting an accelerated test protocol. Ann Allergy Asthma Immunol. 2023;131(2):224–30. 10.1016/j.anai.2023.04.004
10 Blank S et al. Prevalence of Hymenoptera venom allergy and sensitization in the population-representative German KORA cohort. Allergo J Int. 2019;28(6):183–91. 10.1007/s40629-018-0089-4
11 Schäfer T. Epidemiologie der Insektengiftallergie. Allergo J. 2009;18(5):353–358. 10.1007/BF03362108
12 Schäfer T, Przybilla B. IgE antibodies to Hymenoptera venoms in the serum are common in the general population and are related to indications of atopy. Allergy. 1996;51(6):372–7. PMid: 8837658
13 Sturm GJ et al. Sensitization to Hymenoptera venoms is common, but systemic sting reactions are rare. J Allergy Clin Immunol. 2014;133(6):1635–43.e1. 10.1016/j.jaci.2013.10.046
14 Schäfer T, Przybilla B. IgE antibodies to Hymenoptera venoms in the serum are common in the general population and are related to indications of atopy [Internet]. Allergy. 1996;51(6):372–7. PMid: 8837658. Available from: https://www.unboundmedicine.com/medline/citation/8837658/IgE_antibodies_to_Hymenoptera_venoms_in_the_serum_are_common_in_the_general_population_and_are_related_to_indications_of_atopy_ Accessed: Aug. 19, 2025.
15 Park HJ, Brooks DI, Chavarria CS, Wu RL, Mikita CP, Beakes DE. Combining discordant serum IgE and skin testing ımproves diagnostic and therapeutic accuracy for Hymenoptera venom hypersensitivity ımmunotherapy. J Allergy Clin Immunol Pract. 2022;10(3):837–43.e3. 10.1016/j.jaip.2021.08.037
16 Jappe U, Raulf-Heimsoth M, Hoffmann M, Burow G, Hübsch-Müller C, Enk A. In vitro Hymenoptera venom allergy diagnosis: Improved by screening for cross-reactive carbohydrate determinants and reciprocal inhibition. Allergy. 2006;61(10): 1220–9. 10.1111/j.1398-9995.2006.01232.x
17 Sturm GJ, Schuster C, Kranzelbinder B, Wiednig M, Groselj-Strele A, Aberer W. Asymptomatic sensitization to Hymenoptera venom ıs related to total ımmunoglobulin E levels. Int Arch Allergy Immunol. 2009;148(3):261–4. 10.1159/000161586
18 Müller U, Roth A, Yman L, Patrizzi R. Use of RAST technique in wasp sting hypersensitivity: Cross-reactions between various ınsect antigens are specially considered. Allergy. 1978;33(4):197–202. 10.1111/j.1398-9995.1978.tb01534.x.
19 Tischler S, Trautmann A, Goebeler M, Stoevesandt J. Bee/Vespula venom-specific IgE ratio greater than 5:1 ındicates culprit ınsect in double-sensitized patients. J Allergy Clin Immunol Pract. 2025;13(1):79–88.e4. 10.1016/j.jaip.2024.10.029
20 Sturm GJ, Böhm E, Trummer M, Weiglhofer I, Heinemann A, Aberer W. The CD63 basophil activation test in Hymenoptera venom allergy: a prospective study. Allergy. 2004;59(10):1110–1117. 10.1111/j.1398-9995.2004.00400.x
21 Moffitt JE, et al. Stinging insect hypersensitivity: A practice parameter update. J Allergy Clin Immunol. 2004;114(4):869–86. 10.1016/j.jaci.2004.07.046
22 Boburka SM. Reducing the sting: Diagnosis and management of Hymenoptera venom allergy. JAAPA. 2021;34(8):28–32. 10.1097/01.JAA.0000758196.47706.91
23 Kalyoncu AF, Demir AU, Özcan Ü, Özkuyumcu C, Şahin AA, Bariş YI. Bee and wasp venom allergy in Turkey.Ann Allergy Asthma Immunol. 1997;78(4):408–12. 10.1016/S1081-1206(10)63203-6