
Download


REVIEW
Efficacy of hypertonic saline nasal irrigation in allergic rhinitis: A systematic review and meta-analysis
Nishtha Singha*, Sheetu Singhb, Arvind Kumar Sharmac, Udaiveer Singha, Vaibhav Bhatnagard, Virendra Singhb
aDepartment of Respiratory Medicine, Asthma Bhawan, Jaipur, India
bDepartment of Pulmonary Medicine, Rajasthan Hospital, Jaipur, India
cDepartment of Community Medicine, Geetanjali Institute of Medical Sciences Jaipur, India
dDepartment of Computer Applications, Manipal University Jaipur, India
Abstract
Saline nasal irrigation provides symptom relief in allergic rhinitis (AR), but the optimal saline concentration remains uncertain. The comparative efficacy of 3% hypertonic saline nasal irrigation (HSNI) versus 0.9% isotonic saline is still debated. We conducted a meta-analysis to evaluate nasal symptom scores from studies comparing HSNI with control (isotonic saline or no saline) in patients with AR. Systematic search of PubMed, Scopus, and Cochrane Central was performed for randomized controlled trials (RCTs) comparing 3% HSNI with control from inception to May 8, 2024. Primary outcomes were total nasal symptom scores and antihistamine use. We pooled mean differences and odds ratios (OR) with 95% confidence intervals (CI) using a random effects model and assessed heterogeneity with I2. Nine RCTs involving 645 patients met the inclusion criteria. Follow-up ranged from 4 weeks to 2 months. The mean age was 35.49 years in adults and 9.3 years in children. HSNI significantly reduced nasal symptom scores compared with control in adults (MD = −2.09; 95% CI: −3.86 to −0.33; P = 0.02; I2 = 97%) and children (MD = −0.97; 95% CI: −1.51 to −0.44; P = 0.0004; I2 = 42%). Antihistamine use was also lower with HSNI than control (OR = 0.39; 95% CI: 0.21–0.70; P = 0.002; I2 = 14%), but no significant difference was found between HSNI and isotonic saline alone (OR = 0.69; 95% CI: 0.41–1.16; P = 0.16; I2 = 0%). HSNI appears effective in reducing symptoms and medication use in allergic rhinitis across age groups.
Key words: nasal wash, allergic rhinitis, saline irrigation, hypertonic versus isotonic saline
*Corresponding author: Nishtha Singh, Asthma Bhawan, Jaipur, Rajasthan, India. Email address: [email protected]
Received 7 May 2025; Accepted 25 June 2025; Available online 1 September 2025
Copyright: Singh N, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Allergic rhinitis (AR) is an atopic disease that forms part of a broader spectrum of allergic conditions. It is an immunoglobulin-E-mediated allergic inflammatory response driven by type 2 helper (Th2) cells.1 AR is a systemic allergic response that frequently coexists with asthma and other allergic conditions.2 The cardinal symptoms of AR include nasal blockage, nasal discharge, nasal pruritus, and sneezing.3 AR and other allergic diseases affect 10–30% of the global population.4 In India, data from the Global Asthma Network (GAN) study conducted between August 2017 and February 2018 show that the prevalence of AR among 6–7-year olds is 7.7% (7.4–8.1%), 13–14-year olds is 23.5% (23.0–24.1%), and adults is 9.8% (9.55–9.96%).5 According to the International Study for Asthma and Allergies in Childhood phase 3 (ISAAC-3) conducted between 2001 and 2003, the prevalence of AR was 11.3% (7.3%, 26.7%) in the 6–7 years age group and 24.4% (4.1%, 45.7%) in 13–14 year age group.5 Prevalence rates have significantly decreased over time, according to time trends in AR from ISAAC-1, ISAAC-3, and GAN (P <.05).5 The physician-based diagnosis of AR was around 15% with a high patient symptom-based diagnosis.6 Although AR predominantly affects children, it also impacts adults, contributing to significant morbidity, productivity loss, and healthcare costs. AR peaks between the second and the fourth decades of life and then gradually decreases.
Management of AR involves allergen avoidance, though this often requires substantial lifestyle modifications. Intranasal corticosteroids (INCS) are the first-line treatment to alleviate nasal symptoms. However, long-term use of INCS is associated with adverse effects, including nasal irritation, epistaxis, and dryness, which frequently lead to intolerance and treatment discontinuation.7 Additionally, prolonged oral or injectable steroid use is not recommended due to systemic side effects.8
Isotonic saline nasal irrigation (ISNI) is often suggested as a supplementary treatment for AR, as it helps remove allergens and mucus from the nasal lining, thereby alleviating local inflammation and reducing the severity of symptoms in AR patients. Rinsing the nasal passages provides symptom relief and enhances overall nasal cleanliness. Saline irrigation enhances mucociliary clearance, facilitating the removal of allergens and inflammatory agents from the nasal passages. This therapy employs different concentrations of nasal saline, but no formulation has been proven superior.8 Numerous studies have highlighted the clinical advantages of ISNI, resulting in its inclusion as a complementary treatment in the 2018 AR guidelines.8 Research has shown notable improvements in symptom scores and quality of life metrics with regular saline irrigation in both adults and children suffering from allergic rhinitis.9 Both isotonic and hypertonic solutions have been effective in enhancing mucociliary clearance times. Hypertonic solutions are believed to have additional anti-inflammatory effects on the nasal lining.10 Interestingly, a previous study indicated that hypertonic saline solutions might be more effective than isotonic ones for symptom relief in certain cases, but lacks recent data.10 Given the absence of recent meta-analyses on the effectiveness of hypertonic saline nasal irrigation (HSNI) in adults with AR, and the outdated nature of previous meta-analyses, such as one from 2012,
we decided to undertake this meta-analysis.9,11,12 Consequently, we performed a systematic review and updated meta-analysis to assess the efficacy of HSNI as a treatment approach for adults and children with AR.
Materials and Methods
Eligibility criteria
Inclusion in this meta-analysis was restricted to studies that met all the following eligibility criteria: (1) randomized trials; (2) comparing HSNI with control (isotonic nasal saline wash or no nasal irrigation); (3) enrolled patients who had allergic rhinitis regardless of age, gender, and ethnicity; and (4) reporting of any one of the clinical outcomes of interest.
We excluded studies with (1) no control group; (2) patients with acute, chronic, or postoperative rhinitis; (3) comparison between saline and other medicines for allergic rhinitis; (4) overlapping study populations; (5) non-English studies; and (6) animal studies.
Search strategy and data extraction
We systematically searched PubMed, Scopus, and Cochrane Central Register of Controlled Trials from inception to May 2024 with the following search terms: “allergic rhinitis,” “nasal irrigation,” “saline solution,” “saline rinse,” “brine irrigation,” “intranasal normal saline,” “nasal saline,” and “nasal lavages.”
The references from all included studies, previous systematic reviews, and meta-analyses were also searched manually for any additional studies. Two authors (N.S. and U.S.) independently extracted the data following a predefined search criterion and conducted the quality assessment. The prospective meta-analysis protocol was registered on PROSPERO on July 31, 2024, under the protocol CRD42024570873.
Endpoints and subgroup analysis
The main outcome included was total nasal symptom scores. This score is measured based on the following symptoms: nasal discharge, nasal obstruction, nasal itching, and sneezing. The secondary outcome included the rate of use of antihistamines by the patients. We performed a subgroup analysis comparing HSNI with ISNI and HSNI with no nasal irrigation.
Quality assessment
We evaluated the risk of bias in randomized studies using the Cochrane Risk of Bias assessment tool version 2, in which studies are scored as high, low, or unclear risk of bias in five domains: selection, performance, detection, attrition, and reporting biases.13 Two independent authors completed the risk of bias assessment (N.S. and V.S.). Disagreements were resolved through a consensus after discussing the reasons for the discrepancy. Publication bias was investigated by funnel plot analysis of point estimates according to study weights.
Statistical analysis
This systematic review and meta-analysis were performed and reported following the Cochrane Collaboration Handbook for Systematic Review of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement guidelines.14,15
Continuous outcomes were compared. Odds ratios with 95% CIs were used to compare treatment effects for categorical endpoints.
We assessed heterogeneity with I2 statistics and the Cochrane Q test, P < 0.10, and I2 > 25%, were considered significant for heterogeneity. We used the DerSimonian and Laird random effects model.
We also performed a sensitivity analysis using the leave-one-out method: removing each study from the outcome assessment. We used Review Manager 5.4 (Cochrane Center, The Cochrane Collaboration, Denmark) for all statistical analysis.
Results
Study selection and characteristics
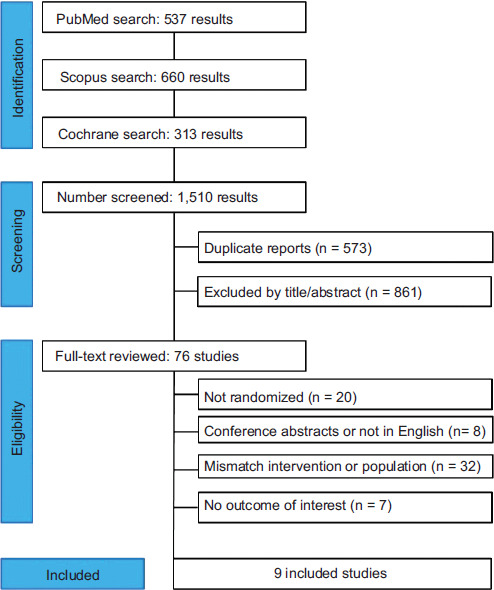
As detailed in Figure 1, the initial search yielded 1510 results. After removing duplicates and ineligible studies, 76 remained which were fully reviewed based on the inclusion criteria. Of these, nine randomized studies were included, comprising 645 patients (Figure 1) with a mean age of 35.49 years in adults and 9.3 years in children.16–24 A total of 287 patients (44.5%) received HSNI, 298 patients (46.2%) received ISNI, and 60 patients (9.3%) received no saline irrigation. There was considerable variability between studies regarding follow-up periods and definitions of total nasal symptom scores. Study characteristics are summarized in Table 1.
Table 1 Baseline characteristics of the studies included in the meta-analysis.
| Study | HSNI concentration | Control | Volume & daily frequency | Follow-up (weeks) | Male, % HSNI/ISNI | Age, y HSNI/ISNI mean or range |
Participants | Country | Adult/children study | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Sansila et al. (2020) | 1.8% | ISNI (0.9%) | 80 mL BD | 4 | 25.29/34.88 | 38.37/35.61 (mean) |
78 | Thailand | Adult | 1.Questionnaire for allergic rhinoconjunctivitis (Rcq-36)2.Nasal symptom score3.Adverse events |
| Singh et al. (2017) | 2.2% | ISNI (0.9%) | 2 sprays TDS | 8 | 53.3/50 | 35.5/32.5 (mean) |
60 | India | Adult | 1.Nasal symptom score |
| Di Berardino et al. (2017) | 1.8% | No irrigation | 0.13 mL TDS | 4 | 53.8/81.8 | 25 ± 5.3/ 27 ± 6.8 (mean) |
40 | Italy | Adult | 1.Nasal symptom score2.Mucociliary clearance3.Use of antihistamines |
| Garavello et al. (2010) | 3% | No irrigation | 10 mL TDS | 6 | NA | 23.9 ± 5.4/ 24.4 ± 5.8 (mean) |
45 | Italy | Adult | 1.Nasal symptom score2.Use of antihistamines3.Rhinomanometry |
| Rattanamaneewong et al. (2021) | 3% | ISNI (0.9%) | 5 mL BD | 4 | 54.8/63.3 | 9.7 ± 2.6/ 8.8 ± 1.9 (mean) |
61 | Thailand | Children | 1.Nasal symptom score 2.Questionnaire for allergic rhinoconjunctivitis (Rcq-36)3.Nasal cytology changes |
| Malizia et al. (2017) | 3% | ISNI (0.9%) | 5 mL BD | 3 | 25/11 (M/F) |
8.9 ± 2.26/ 10.16 ± 2.39 (mean) |
30 | Italy | Children | 1.Nasal symptom score2.Life quality questionnaires: NCC,PRQLQ, PSQI3.Antihistamine use |
| Marchisio et al. (2012) | 2.7% | ISNI (0.9%) or No irrigation | 20 mL BD | 4 | 137/83 (M/F) | 5–9 years (range) |
220 | Italy | Children | 1.Nasal symptom score2.Rhinoscopy3.Middle ear infection4.Antihistamine use |
| Satdhabudha and Poachanukoon (2012) | 1.25% | ISNI (0.9%) | 240 mL BD | 4 | 60/61 (M/F) | 6–15 years (range) |
81 | Thailand | Children | 1.Nasal symptom score2.Questionnaire for allergic rhinoconjunctivitis (Rcq-36)3.Saccharine clearance time |
| Garavello et al. (2003) | 3% | No irrigation | 2.5 mL TDS | 6 | 8/12 (M/F) | 6–12 years (range) |
20 | Italy | Children | 1.Nasal symptom score2.Antihistamine use |
F, female; HSNI: Hypertonic nasal saline irrigation; ISNI: Isotonic nasal saline irrigation; M, male; NA, not available; Rcq-36: Questionnaire for Thai allergic rhinoconjunctivitis patients
Figure 1 PRISMA flow diagram of study screening and selection.
Pooled analysis of all studies
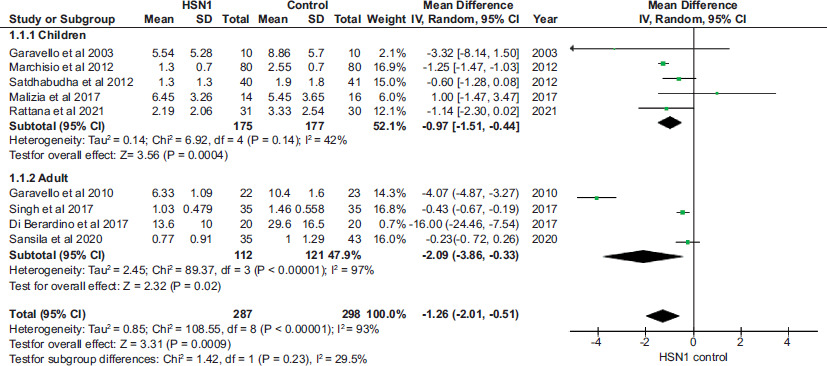
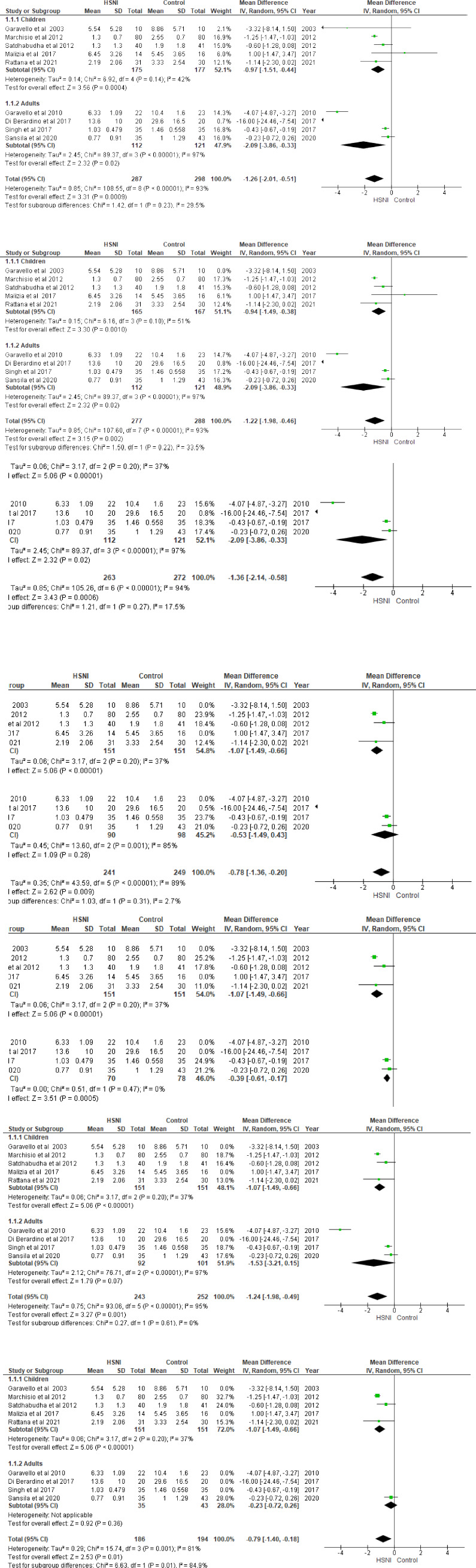
Compared with control (isotonic nasal saline wash or no nasal irrigation), among adults receiving HSNI, among the four studies16–19 there was a significant reduction in total nasal symptom scores (MD −2.09; 95% CI −3.86 to −0.33; P = 0.02; I2 = 97%; Figure 2). When standardized mean difference (SMD) was used, the difference remained statistically significant (SMD −1.21; 95% CI −2.15 to −0.27; P = 0.01; I2 = 90%).
Figure 2 Forest plot of the improvement of nasal symptoms scores in the HSNI and control groups: Overall meta-analysis. The incidence of total symptom scores was significantly lower in HSNI group compared to ISNI and no saline group in children (P = 0.0004) and adults (P = 0.02). CI: Confidence interval; HSNI; Hypertonic saline nasal irrigation; ISNI: Isotonic saline nasal irrigation; Control: Isotonic + No saline irrigation.
In children, among the five studies analyzed,20–24 HSNI was associated with a statistically significant reduction in total nasal symptom scores compared with control (MD −0.97; 95% CI −1.51 to −0.44; P = 0.0004; I2 = 42%; Figure 2). However, using SMD, we found no difference between groups (SMD −0.61; 95% CI −1.38 to −0.15; P = 0.11; I2 = 90%).
Compared with control, HSNI also demonstrated a trend toward reduced antihistamine consumption in three studies20,21,23 (OR 0.39; 95% CI 0.21–0.70; P = 0.002; I2 = 14%; Figure 3).
Figure 3 Forest plot comparing rates of rescue antihistamine use in HSNI with ISNI and no saline groups: Overall meta-analysis. CI: Confidence interval; HSNI: Hypertonic saline nasal irrigation; ISNI: Isotonic saline nasal irrigation; Control: Isotonic + No saline irrigation.
Subanalysis in selected populations
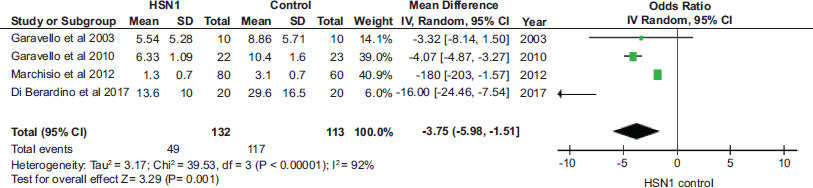
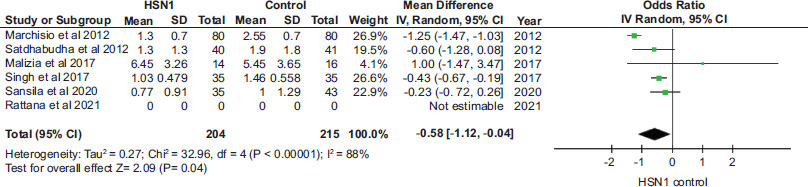
Subgroup analysis revealed a reduction in nasal symptom score for HSNI when compared with no irrigation only (MD −3.75; 95% CI −5.98 to −1.51; P = 0.001; I2 = 92%; Figure 4) and with ISNI only (MD −0.58; 95% CI −1.12 to −0.04; P = 0.04; I2 = 88%; Figure 5). We found no difference in antihistamine consumption between the HSNI group and the ISNI only group (OR 0.69; 95% CI 0.41 to 1.16; P = 0.16; I2 = 0%; Figure 6).
Figure 4 Forest plot of subgroup analysis comparing HSNI and no saline groups. CI: Confidence interval; HSNI: Hypertonic saline nasal irrigation; Control: No saline irrigation.
Figure 5 Forest plot of subgroup analysis comparing nasal symptom score in HSNI and ISNI groups. CI: Confidence interval; HSNI: Hypertonic saline nasal irrigation; ISNI or control: Isotonic saline nasal irrigation.
Figure 6 Forest plot of subgroup analysis of rates of rescue antihistamine use in HSNI and ISNI groups. CI: Confidence interval; HSNI: Hypertonic saline nasal irrigation; ISNI or control: Isotonic saline nasal irrigation.
Quality assessment
Given the high heterogeneity, a leave-one-out sensitivity analysis was performed by systematically removing each study to assess the stability of the results. The exclusion of individual studies caused the total mean difference to shift from −1.26 to −0.70, meaning the estimated effect weakens as high heterogeneity studies are removed.
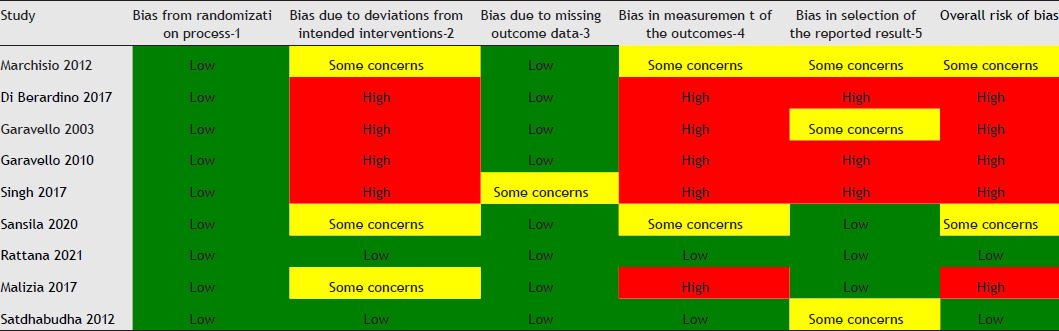
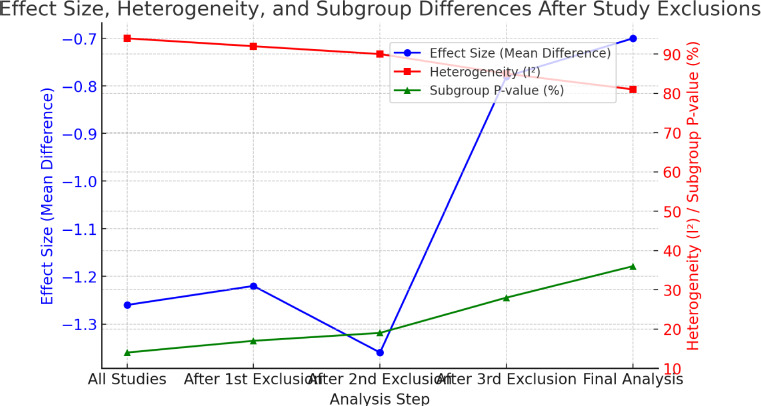
Quality assessment was conducted using the Risk of Bias 2 (RoB 2) tool. Five studies were deemed to have a high risk of bias, as outlined in Table S1. We performed a sensitivity analysis removing them as depicted in Figure S1. Figure S2 shows a graph illustrating the changes in effect size (mean difference), heterogeneity (I2), and subgroup differences (P) as studies were excluded. Excluding certain studies for sensitivity analysis led to a noticeable reduction in heterogeneity, with I2 decreasing from 94 to 81%, primarily by removing high-variability adult studies. The overall effect size weakened, shifting a mean difference from −1.26 to −0.70, and CI became narrower, reflecting increased precision. Subgroup differences between adults and children remained statistically nonsignificant throughout (P > 0.1), but the distinction further diminished after exclusions, with the adult subgroup effect approaching nonsignificance (P = 0.36). These changes suggest that excluded studies contributed to both higher heterogeneity and stronger apparent subgroup differences. Funnel plot analysis indicated a symmetrical distribution of studies, suggesting minimal publication bias (Figure S3).
Discussion
This systematic review and meta-analysis assessed the efficacy of HSNI in managing AR, drawing on data from nine studies involving 645 participants. The pooled findings indicated that HSNI significantly improved nasal symptom scores in both adults and children compared to ISNI and no irrigation. While these results are statistically compelling, their clinical interpretation warrants careful consideration.
The symptomatic improvements align with HSNI’s proposed mechanism of action, mechanical clearance of allergens, mucus, and inflammatory cytokines (IL-4, IL-5, IL-9, IL-13, and TNF-α) from the nasal mucosa.25–28 This process likely contributes to reduced local inflammation and enhanced mucociliary function,29–31 both of which are critical for symptom relief in AR.32–34 However, the reported absolute mean differences, –2.09 in adults and –0.97 in children, require cautious interpretation, particularly in light of inconsistent reporting of the minimal clinically important difference (MCID) across studies.
Although there was a trend toward reduced antihistamine use, HSNI did not significantly outperform ISNI in this regard. This raises relevant clinical concerns about its ability to decrease medication reliance, particularly pertinent in pediatric patients and those pursuing steroid-sparing strategies. The lack of significant reduction in pharmacologic use suggests that while HSNI enhances symptom control, its utility in minimizing medication burden remains unproven.
Subgroup analyses confirmed consistent symptomatic benefits across age groups and comparators (ISNI and no irrigation). However, considerable variability in saline concentrations (1.25–3.00%), irrigation techniques, and treatment durations across studies limits the generalizability of the results and precludes definitive recommendations regarding optimal formulation. For instance, Marchisio et al.23 and Malizia et al.21 found superior outcomes in children, whereas Satdhabudha and Poachanukoon20 reported no additional benefit of buffered HSNI over ISNI.29 These discrepancies emphasize the importance of viewing HSNI as a heterogeneous intervention influenced by delivery parameters and formulation differences.
Among adult populations, Sansila et al.16 and Singh et al.17 reported greater symptom relief with HSNI than with ISNI, while Garavello et al.18,27 found significant benefits in pregnant women. Additionally, Di Berardino et al.19 observed enhanced mucociliary clearance during pollen seasons, an important implication for seasonal AR management.
These results align with the ARIA guidelines, which recommend nasal saline irrigation as an effective adjunctive therapy in both seasonal and perennial AR, especially in children and individuals seeking to minimize corticosteroid use.35 Moreover, the GINA guidelines underscore the necessity of controlling comorbid AR to achieve optimal asthma outcomes.36 In this context, HSNI may offer additional benefit by mitigating upper airway inflammation, potentially contributing to better asthma control.
Current AR management primarily relies on INCS, with add-on options such as antihistamines, decongestants, cromolyn, or leukotriene receptor antagonists for patients with persistent symptoms.37 However, long-term antihistamine use can result in side effects such as drowsiness and dizziness, while prolonged INCS use raises concerns regarding growth suppression in children and elevated intraocular pressure.38 Given these safety considerations, nonpharmacological strategies such as nasal irrigation are garnering attention as viable alternatives. HSNI, with its demonstrated efficacy and low side effect profile, emerges as a promising option for patients seeking symptom relief without the risks associated with long-term medication.
From a practical standpoint, HSNI is inexpensive, safe, and easily accessible, making it especially valuable in low-resource settings or for individuals who cannot tolerate pharmacologic therapies. Nevertheless, in view of its comparable impact on antihistamine usage relative to ISNI, a universal preference for HSNI cannot be currently endorsed.
Future research should aim to address these gaps by investigating whether HSNI contributes to reduced medication dependence, improves patient-reported outcomes, or modifies disease progression. Standardized comparative protocols evaluating different saline concentrations and incorporating quality-of-life metrics are essential to refine the clinical role of HSNI in AR management.
In conclusion, while current evidence supports HSNI as a safe and effective adjunct with consistent symptomatic benefits, its precise clinical positioning—particularly in comparison to ISNI—requires further elucidation through robust, well-designed studies.
Limitations
This analysis has several limitations. A major concern is the high degree of heterogeneity across studies, especially among adult cohorts (I2 = 97%). This likely stems from differences in saline concentration, irrigation volume and frequency, treatment duration (ranging from 3 to 8 weeks), and the symptom scoring tools employed. Nevertheless, the direction of effect consistently favored HSNI. Subgroup comparisons (HSNI vs ISNI and HSNI vs no irrigation) and leave-one-out sensitivity analyses reduced heterogeneity (from I2 = 94 to 81%) and supported the robustness of the findings.
Another limitation is study quality. Five of the nine studies were assessed as having a high risk of bias, potentially exaggerating effect sizes. Sensitivity analysis excluding these studies reduced the pooled effect size (from –1.26 to –0.70) but preserved the direction of benefit, with narrower confidence intervals suggesting greater precision. This supports the credibility of the observed benefit, albeit with a degree of caution.
Further limitations include the lack of consistent stratification by disease severity, seasonality (seasonal vs perennial), and symptom domains (e.g., nasal symptoms, mucociliary clearance, quality-of-life outcomes). Consequently, the specific effect of HSNI in subgroups could not be adequately assessed. Though qualitative improvements were observed irrespective of severity, this remains a methodological limitation.
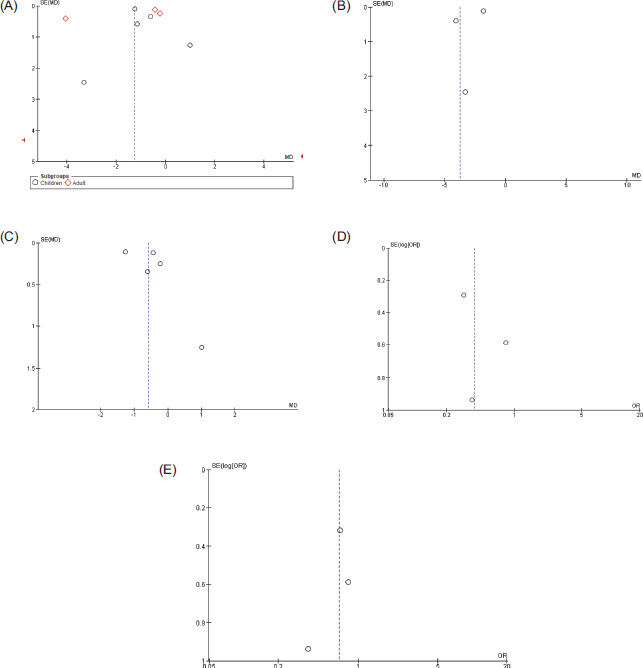
Lastly, the potential for publication bias cannot be entirely ruled out. Although visual inspection of funnel plots suggested minimal bias, the limited number of included studies restricts the reliability of this assessment.
Conclusions
This systematic review and meta-analysis highlight the potential benefits of HSNI in AR management, particularly in reducing nasal symptoms and possibly decreasing antihistamine reliance. Given its favorable safety profile and nonpharmacological nature, HSNI may serve as a valuable adjunctive treatment. However, future large-scale randomized controlled trials are necessary to standardize irrigation protocols, determine optimal saline concentrations, and clarify the role of HSNI alongside conventional pharmacological treatments.
By refining nasal irrigation strategies, clinicians can provide AR patients with a simple, effective, and well-tolerated intervention to improve quality of life.
Acknowledgments
None.
Ethics Approval
This is a systematic review and meta-analysis study. Ethics committee approval was obtained by all nine studies included in the meta-analysis.
Informed Consent
Informed consent was obtained from all individual participants in the 9 studies included in this meta-analysis. All studies involved human participants.
Disclosure
All authors report no relationships that could be construed as a conflict of interest. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Authors’ Contributions
All authors contributed equally to this article.
Conflicts of Interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
No funding was received to assist with the preparation of this manuscript.
REFERENCES
1 Skoner DP. Allergic rhinitis: Definition, epidemiology, pathophysiology, detection, and diagnosis. J Allergy Clin Immunol. 2001;108(1 Suppl):S2–8. 10.1067/mai.2001.115569
2 Genuneit J, Seibold AM, Apfelbacher CJ, Konstantinou GN, Koplin JJ, La Grutta S, et al. Overview of systematic reviews in allergy epidemiology. Allergy. 2017;72(6):849–56. 10.1111/all.13123
3 Kakli HA, Riley TD. Allergic rhinitis. Prim Care. 2016;43(3):465–75. 10.1016/j.pop.2016.04.009
4 Pearce N, Sunyer J, Cheng S, Chinn S, Björkstén B, Burr M, et al. Comparison of asthma prevalence in the ISAAC and the ECRHS. ISAAC Steering Committee and the European Community Respiratory Health Survey. International Study of Asthma and Allergies in Childhood. Eur Respir J. 2000;16(3):420–6. 10.1183/9031936.00.16337700
5 Barne M, Singh S, Mangal DK, Singh M, Awasthi S, Mahesh PA, et al. Global Asthma Network Phase I, India: Results for allergic rhinitis and eczema in 127,309 children and adults. J Allergy Clin Immunol Global. 2022;1(2):51–60. 10.1016/j.jacig.2022.01.004
6 Wheatley LM, Togias A. Clinical practice. Allergic rhinitis. N Engl J Med. 2015;372(5):456–63. 10.1056/NEJMcp1412282
7 Small P, Kim H. Allergic rhinitis. Allergy Asthma Clin Immunol. 2011;7 Suppl 1(Suppl 1):S3. 10.1186/s13223-018-0280-7
8 Wise SK, Lin SY, Toskala E, Orlandi RR, Akdis CA, Alt JA, et al. International Consensus Statement on Allergy and Rhinology: Allergic rhinitis. Int Forum Allergy Rhinol. 2018;8(2):108–352. 10.1002/alr.22073
9 Li CL, Lin HC, Lin CY, Hsu TF. Effectiveness of hypertonic saline nasal irrigation for alleviating allergic rhinitis in children: A systematic review and meta-analysis. J Clin Med. 2019;8(1):64. 10.3390/jcm8010064
10 Cordray S, Miner L, Harjo JB. Comparison of intranasal hypertonic Dead sea saline spray and intranasal aqueous triamcinolone spray in seasonal allergic rhinitis. Ear Nose Throat J. 2005;84(7):426–30.
11 Wang Y, Jin L, Liu S-X, Fan K, Qin M-L, Yu S-Q. Role of nasal saline irrigation in the treatment of allergic rhinitis in children and adults: A systematic analysis. Allergol Immunopathol (Madr). 2020;48(4):360–67. 10.1016/j.aller.2020.01.002
12 Hermelingmeier KE, Weber RK, Hellmich M, Heubach CP, Mösges R. Nasal irrigation as an adjunctive treatment in allergic rhinitis: A systematic review and meta-analysis. Am J Rhinol Allergy. 2012;26(5):e119–25. 10.2500/ajra.2012.26.3787
13 Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. 10.1136/bmj.l4898
14 Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al., editors. Cochrane handbook for systematic reviews of interventions version 6.3. [cited 2022 Feb). Cochrane, 2022. Available from: www.training.cochrane.org/handbook
15 Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372:n71 10.1136/bmj.n71
16 Sansila K, Eiamprapai P, Sawangjit R. Effects of self-prepared hypertonic nasal saline irrigation in allergic rhinitis: A randomized controlled trial. Asian Pac J Allergy Immunol. 2020;38(3):200–7. 10.12932/AP-090618-0331
17 Singh R, Galagali JR, Kumar S, Bahurupi Y, Chandrachood M. Comparative study of intranasal hypertonic seawater saline versus intranasal normal saline in allergic rhinitis. Int J Otorhinolaryngol Head Neck Surg. 2017;3(1):104–7. 10.18203/issn.2454-5929.ijohns20164810
18 Garavello W, Somigliana E, Acaia B, Gaini L, Pignataro L, Gaini RM. Nasal lavage in pregnant women with seasonal allergic rhinitis: A randomized study. Int Arch Allergy Immunol. 2010;151(2):137–41. 10.1159/000236003
19 Di Berardino F, Zanetti D, D’Amato G. Nasal rinsing with an atomized spray improves mucociliary clearance and clinical symptoms during peak grass pollen season. Am J Rhinol Allergy. 2017;31(1):40–3. 10.2500/ajra.2016.30.4383
20 Satdhabudha A, Poachanukoon O. Efficacy of buffered hypertonic saline nasal irrigation in children with symptomatic allergic rhinitis: A randomized double-blind study. Int J Pediatr Otorhinolaryngol. 2012;76(4):583–8. 10.1016/j.ijporl.2012.01.022
21 Malizia V, Fasola S, Ferrante G, Cilluffo G, Montalbano L, Landi M, et al. Efficacy of buffered hypertonic saline nasal irrigation for nasal symptoms in children with seasonal allergic rhinitis: A randomized controlled trial. Int Arch Allergy Immunol. 2017;174(2):97–103. 10.1159/000481093
22 Rattanamaneewong K, Chinratanapisit S, Piromrat K, Thambamrung N. Efficacy of hypertonic saline irrigation for nasal symptoms in children with perennial allergic rhinitis: A randomized double-blind study. J Med Assoc Thai. 2021;104:1570–7.
23 Marchisio P, Varricchio A, Baggi E, Bianchini S, Capasso ME, Torretta S, et al. Hypertonic saline is more effective than normal saline in seasonal allergic rhinitis in children. Int J Immunopathol Pharmacol. 2012;25(3):721–30. 10.1186/1824-7288-40-47
24 Garavello W, Romagnoli M, Sordo L, Gaini RM, Di Berardino C, Angrisano A. Hypersaline nasal irrigation in children with symptomatic seasonal allergic rhinitis: A randomized study. Pediatr Allergy Immunol. 2003;14(2):140–3. 10.1034/j.1399-3038.2003.00021.x
25 König K, Klemens C, Eder K, San Nicoló M, Becker S, Kramer MF, et al. Cytokine profiles in nasal fluid of patients with seasonal or persistent allergic rhinitis. Allergy Asthma Clin Immunol. 2015;11:26. 10.1186/s13223-015-0093-x
26 Small P, Keith PK, Kim H. Allergic rhinitis. Allergy Asthma Clin Immunol. 2018;14(Suppl 2):51. 10.1186/s13223-018-0280-7
27 Pawankar R, Hayashi M, Yamanishi S, Igarashi, T. The paradigm of cytokine networks in allergic airway inflammation. Curr Opin Allergy Clin Immunol. 2015;15:41–8. 10.1097/ACI.0000000000000129
28 Scadding, G. Cytokine profiles in allergic rhinitis. Curr Allergy Asthma Rep. 2014;14:435. 10.1007/s11882-014-0435-7
29 Barham HP, Harvey RJ. Nasal saline irrigation: Therapeutic or homeopathic. Braz J Otorhinolaryngol. 2015;81:457–58. 10.1016/j.bjorl.2015.07.002
30 Bonnomet A, Luczka E, Coraux C, de Gabory L. Non-diluted seawater enhances nasal ciliary beat frequency and wound repair speed compared to diluted seawater and normal saline. Int Forum Allergy Rhinol. 2016;6:1062–68. 10.1002/alr.21782
31 Georgitis JW. Nasal hyperthermia and simple irrigation for perennial rhinitis. Changes in inflammatory mediators. Chest. 1994;106:1487–92. 10.1378/chest.106.5.1487
32 Chen J-R, Jin L, Li X-Y. The effectiveness of nasal saline irrigation (seawater) in treatment of allergic rhinitis in children. Int J Pediatr Otorhinolaryngol. 2014;78:1115–18. 10.1016/j.ijporl.2014.04.026
33 Gallant JN, Basem JI, Turner JH, Shannon CN, Virgin FW. Nasal saline irrigation in pediatric rhinosinusitis: A systematic review. Int J Pediatr Otorhinolaryngol. 2018;108:155–62. 10.1016/j.ijporl.2018.03.001
34 Rabago D, Zgierska A. Saline nasal irrigation for upper respiratory conditions. Am Fam Physician. 2009;80(10):1117–19.
35 Klimek L, Bachert C, Pfaar O, Becker S, Bieber T, Brehler R, et al. ARIA guideline 2019: Treatment of allergic rhinitis in the German health system. Allergol Select. 2019;3(1):22–50. 10.5414/ALX02120E
36 Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2025. [cited 2025 May]. Available from: www.ginasthma.org
37 Ridolo E, Barone A, Nicoletta F, Paoletti G, Heffler E, Malvezzi L, et al. Intranasal corticosteroid and antihistamine combinations in the treatment of allergic rhinitis: The role of the novel formulation olopatadine/mometasone furoate. Expert Rev Clin Immunol. 2023;19(6):575–84. 10.1080/1744666X.2023.2200165
38 Fein MN, Fischer DA, O’Keefe AW, Sussman GL. CSACI position statement: Newer generation H1-antihistamines are safer than first-generation H1-antihistamines and should be the first-line antihistamines for the treatment of allergic rhinitis and urticaria. Allergy Asthma Clin Immunol. 2019;15(1):61. 10.1186/s13223-019-0375-9
Supplementary
Table S1 Critical appraisal of individual studies according to the Cochrane Collaboration’s tool for assessing risk of bias in randomized trials.
Figure S1 Sensitivity analysis to assess the effects of excluding studies on heterogeneity and subgroup differences
Figure S2 The graph illustrating the changes in effect size (mean difference), heterogeneity (I2), and subgroup differences (p-values) as studies were excluded.
Figure S3 Funnel plot for nasal symptom improvement in all studies (A), in subgroups comparing HSNI with no saline (B), in subgroups comparing HSNI with ISNI(C), rates of rescue antihistamine use comparing HSNI with ISNI and no saline (D) and rates of rescue antihistamine use comparing HSNI with ISNI(E) showed no definitive evidence of publication bias. Sensitivity analysis excluding each study found no change in significance of results.