
Download
ORIGINAL ARTICLE
Health literacy in patients with inborn errors of immunity
Makbule Seda Bayrak Durmaz, Göksal Keskin, Seda Altıner*
Division of Immunology and Allergy, Department of Internal Medicine, Ankara University School of Medicine, Ankara, Turkey
Abstract
Background and Objectives: Health literacy (HL) is essential for managing chronic conditions such as inborn errors of immunity (IEI). Limited HL may lead to poor clinical outcomes and inefficient healthcare use; however, HL among IEI patients remains underexplored. The aim of this study was to evaluate HL levels in adult IEI patients using the Turkish Health Literacy Scale (TSOY-32) and to identify associated sociodemographic factors.
Materials and Methods: This cross-sectional study included 27 adult IEI patients receiving regular immunoglobulin therapy at an allergy and immunology clinic. Participants completed the TSOY-32 via face-to-face interviews. The scale assessed HL across two dimensions—Treatment and Services (TS) and Disease Prevention/Health Promotion (DP/HP)—and four information processing stages. Sociodemographic data were also collected.
Results: According to the TSOY-32 general index, 44.4% of patients had inadequate or problematic HL. Significant associations were observed between HL levels (particularly in the DP/HP dimension) and age, gender, education, and marital status. Younger adults (18–34 years) showed higher HL than those aged 35 and older and married participants had lower HL than singles. Although HL improved with education, no significant link was found between educational level and overall HL. Economic status had a positive but nonsignificant relationship with HL.
Conclusion: A significant proportion of IEI patients had limited HL, which may negatively impact treatment adherence. Tailored educational interventions that take into account patients’ HL levels (e.g., simplified visual materials, brief in-clinic education, digital tools) could help enhance self-management. Larger studies are warranted to clarify the determinants of HL and improve care in this population.
Key words: health literacy, inborn errors of immunity, sociodemographic factors, treatment adherence, Turkish Health Literacy Scale (TSOY-32)
*Corresponding author: Seda Altiner, MD, Assistant Professor at Division of Allergy and Clinical Immunology, Department of Internal Medicine, Ankara University, School of Medicine, Ankara, Turkey. Email address: [email protected]
Received 5 May 2025; Accepted 26 June 2025; Available online 1 September 2025
Copyright: Durmaz MSB, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Health literacy (HL), as defined by the National Institutes of Health, is the ability of individuals to obtain, process, and understand essential health information and services needed to make informed decisions.1 This skill plays a crucial role in enabling individuals to maintain their health, access appropriate treatments, and navigate the healthcare system effectively.
Numerous studies have demonstrated that limited HL is strongly linked to poorer health outcomes, higher rates of hospital admissions, inadequate use of preventive healthcare services, insufficient knowledge about medical conditions, and increased healthcare costs.2,3 Alarmingly, the prevalence of limited HL has been reported to reach as high as 36%.4 The 1992 National Adult Literacy Survey, which assessed literacy skills in English among more than 26,000 adults in the United States, revealed that nearly half of American adults possess low or limited literacy skills, highlighting the widespread nature of this issue.5 A large-scale systematic review encompassing data from 85 studies further underscores the prevalence of limited HL in the United States and its consistent associations with education, ethnicity, and age.2 Although HL is correlated to some extent with educational level, studies show that a significant number of patients may not follow this pattern. Patients with higher education but low HL are particularly at risk, as physicians may rely on their educational background and overestimate their understanding.6
Previously referred to as “primary immunodeficiency diseases,” inborn errors of immunity (IEI) comprise a heterogeneous group of congenital disorders affecting components of the innate and/or adaptive immune systems. These conditions are characterized by immune dysregulation leading to increased susceptibility to infections, autoinflammation, lymphoproliferation, autoimmunity, atopy, and malignancies.7 The International Union of Immunological Societies (IUIS) classifies IEIs into 10 phenotypic categories.8 IEIs affect approximately 1 in 1000–5000 individuals worldwide.9 Early diagnosis and timely intervention are critical in preventing complications. Moreover, adults and elderly patients with IEI frequently present with multiple comorbidities involving various organ systems. In this context, improving HL in this population is of significant importance, as it can positively impact patient management, similar to its role in many other chronic diseases.
In this study, our aim was to evaluate HL levels among patients with IEI managed in our allergy and immunology clinic using the Turkish Health Literacy Scale (TSOY-32), a validated and reliable questionnaire in Turkish.10 Identifying deficiencies in HL may help improve the management of IEI patients and reduce associated morbidity and mortality.
Material and Methods
Study design and participants
This study was designed as a descriptive, cross-sectional study. Patients diagnosed with IEI according to the diagnostic criteria of the European Society for Immunodeficiencies (ESID), who were actively followed up in our adult allergy and immunology outpatient clinic and receiving regular immunoglobulin replacement therapy (IGRT), were included in the study.11 Survey data were collected after obtaining approval from the local ethics committee (Approval Number: İ08-590-23). Only patients who provided written informed consent were included. Data collection was conducted during either routine outpatient clinic visits or infusion units. Exclusion criteria were: being under 18 years of age, not providing written informed consent, and not receiving regular IGRT.
Data collection
Many scales have been developed using different methods to measure HL.2 The TSOY-32, developed by Okyay et al. in 2016 based on the European Health Literacy Survey study, was published by the Turkish Ministry of Health as a validated and reliable instrument in Turkish.10,12
Data were collected through a two-part survey administered to participants. The first section gathered sociodemographic information, including age, gender, education level, and socioeconomic status. The second section consisted of the TSOY-32, which assesses HL.
The TSOY-32 evaluates HL across two main dimensions—treatment and services (TS), and disease prevention/health promotion (DP/HP)—and four key processes—accessing, understanding, evaluating, and applying health information. The scale includes 32 items, each rated on a 5-point Likert scale ranging from 1 (very easy) to 4 (very difficult) and 5 (I don’t know). Responses are scored from 1 (very difficult) to 4 (very easy), and the total score is standardized to a range of 0–50 using the formula: Index = (Arithmetic Mean − 1) × (50/3)
Scores are classified into four categories:
-
0–25 points: Inadequate HL: Individuals in this group have serious problems finding, understanding, evaluating, and applying health-related information.
-
>25–33 points: Problematic/Limited HL: Although individuals in this group have some basic skills in HL, they may have difficulty understanding and applying complex information.
-
>33–42 points: Adequate HL: Individuals in this group generally have a good level of finding, understanding, and applying health-related information.
-
>42–50 points: Excellent HL: This represents individuals with the highest level of competence in accessing, understanding, and applying health information.
The TSOY-32 scale results were calculated separately as general index, two-dimensional (TS and DP/HP) indexes, and four subcategories (access to information [AI], understanding of information [UI], evaluating information [EI], using/applying information [UAI]) indexes with the specified formula. Each index score was classified into one of the four previously defined HL categories.
Statistical analysis
All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) software version 22.0. Descriptive statistics were presented as frequency (percentage), mean ± SD, or median (minimum-maximum). The χ2 and Exact tests were used to compare the proportions in different categorical groups. Continuous variables were investigated with visual and analytical methods to determine the normal distribution and analyzed with the Student’s t-test. A p-value of < 0.05 was considered statistically significant.
Results
Sociodemographic characteristics
Twenty-seven IEI patients agreed to participate in the study, of which 11 (40.7%) were females and 16 (59.3%) males. The mean age was 41.78 ± 14.13 years. In terms of age distribution, one patient was aged 18–24 years, 11 were aged 25–34, 13 were aged 35–64, and two were aged 65 or older. Fifteen participants (55.6%) were married. Regarding education, 18.5% (n = 5) were primary and middle school graduates, 48.1% (n = 13) were high school graduates, and 33.3% (n = 9) held a university degree or higher. Seventeen patients (63%) were employed and 11 (40.7%) reported sufficient income to cover their expenses. The sociodemographic characteristics of the patients are shown in Table 1.
Table 1 Sociodemographic characteristics of the patients.
| n (%) | |
|---|---|
| Gender Male Female |
16 (59.3) 11 (40.7) |
| Age Groups, Years 18–24 25–34 35–64 ≥65 |
1 (3.7) 11 (40.7) 13 (48.1) 2 (7.4) |
| Occupation Worker Self-employed Civil servant Retired Unemployed |
6 (22.2) 5 (18.5) 3 (11.1) 3 (11.1) 10 (37.0) |
| Marital Status Married Single |
15 (55.6) 12 (44.4) |
| Educational Status Primary and middle school High school University degree or higher |
5 (18.5) 13 (48.1) 9 (33.3) |
| Income and Expense Situation Income less than expense Income and expense equal Income more than expense |
9 (33.3) 11 (40.7) 7 (25.9) |
The TSOY-32 survey results
Based on the general index of the TSOY-32 survey, participants’ HL levels were classified as: 18.5% had inadequate HL, 25.9% had problematic/limited HL, 29.6% had adequate HL, and 25.9% had excellent HL. When the two-dimensional indices were examined, the participants were mostly classified as problematic/limited HL (n = 9, 33.3%) in the TS index, whereas the participants were mostly classified as adequate HL and excellent HL (n = 8, 29.6%; n = 8, 29.6%, respectively) in the DP/HP index. Detailed results for the general index, two-dimensional indices, and the four HL subcategories are presented in Table 2.
Table 2 Frequency distribution of HL categories in matrix components.
| Dimension | Health Literacy Category, n (%) | |||
|---|---|---|---|---|
| Inadequate | Problematic | Adequate | Excellent | |
| General | 5 (18.5) | 7 (25.9) | 8 (29.6) | 7 (25.9) |
| Treatment and services Access to information Understanding information Evaluating information Using/applying information |
4 (14.8) 6 (22.2) 4 (14.8) 8 (29.6) 5 (18.5) |
9 (33.3) 3 (11.1) 6 (22.2) 6 (22.2) 2 (7.4) |
8 (29.6) 11 (40.7) 11 (40.7) 7 (25.9) 13 (48.1) |
6 (22.2) 7 (25.9) 6 (22.2) 6 (22.2) 7 (25.9) |
| Disease prevention/Health promotion Access to information Understanding information Evaluating information Using/applying information |
6 (22.2) 9 (33.3) 6 (22.2) 8 (29.6) 5 (18.5) |
5 (18.5) 2 (7.4) 3 (11.1) 3 (11.1) 8 (29.6) |
8 (29.6) 7 (25.9) 10 (37.0) 11 (40.7) 7 (25.9) |
8 (29.6) 9 (33.3) 8 (29.6) 5 (18.5) 7 (25.9) |
| Access to health-related information | 5 (18.5) | 8 (29.6) | 6 (22.2) | 8 (29.6) |
| Understanding health-related information | 4 (14.8) | 6 (22.2) | 9 (33.3) | 8 (29.6) |
| Evaluating health-related information | 8 (29.6) | 6 (22.2) | 7 (25.9) | 6 (22.2) |
| Using/applying health-related information | 5 (18.5) | 6 (22.2) | 11 (40.7) | 5 (18.5) |
The impact of sociodemographic data on the TSOY-32 survey—General index
According to the general index of the TSOY-32 survey, the relationships between sociodemographic variables and HL levels are detailed in Table 3. The analysis revealed no statistically significant associations between gender, age groups, educational level, income level, marital status, and employment status with HL levels (p = 0.153, p = 0.252, p = 0.827, p = 0.055, and p = 0.679, respectively).
Table 3 The impact of sociodemographic data on the TSOY-32 survey.
| Health Literacy Category General Index, n (%) | |||||
|---|---|---|---|---|---|
| Inadequate | Problematic | Adequate | Excellent | p-value | |
| Gender Male Female |
4 (25) 1 (9.1) |
3 (18.8) 4 (36.4) |
3 (18.8) 5 (45.5) |
6 (37.5) 1 (9.1) |
0.153 |
| Age Groups, Years 18–34 ≥ 35 |
1 (8.3) 4 (26.7) |
2 (16.7) 5 (33.3) |
4 (33.3) 4 (26.7) |
5 (41.7) 2 (25.9) |
0.252 |
| Educational Status Primary + middle school High school University degree or higher |
0 (0) 3 (23.1) 2 (22.2) |
2 (40) 2 (15.4) 3 (33.3) |
2 (40) 4 (30.8) 3 (22.2) |
1 (20) 4 (30.8) 2 (22.2) |
0.827 |
| Income and expense situation Income less than expense Income and expense equal Income more than expense |
2 (22.2) 3 (27.3) 0 (0) |
2 (22.2) 3 (27.3) 2 (28.6) |
3 (33.3) 3 (27.3) 2 (28.6) |
2 (22.2) 2 (18.2) 3 (42.9) |
0.805 |
| Marital Status Married Single |
2 (20) 2 (16.7) |
6 (40) 1 (8.3) |
5 (33.3) 3 (25) |
1 (16.7) 6 (50) |
0.055 |
| Occupation Employed Unemployed |
4 (23.5) 1 (10) |
4 (23.5) 3 (30) |
4 (23.5) 4 (40) |
5 (29.4) 2 (20) |
0.679 |
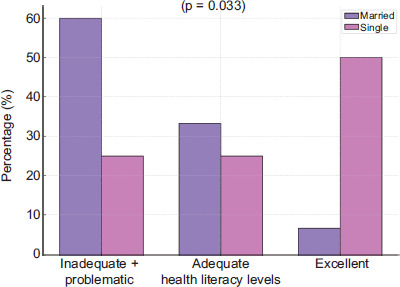
In the analysis of HL across gender, a higher proportion of male participants demonstrated excellent HL compared to females (37.5% vs. 9.1%), whereas females were more likely to be in the adequate HL category (45.5% vs. 18.8%); however, this difference was not statistically significant (p = 0.153). Similarly, when participants were grouped by age, those aged 18–34 showed a higher proportion of excellent HL than those aged 35 and above (41.7% vs. 13.3%); again, this difference did not reach statistical significance (p = 0.252). A linear-by-linear trend toward better HL in younger individuals was observed, but did not meet the threshold for statistical significance (p = 0.051). Regarding marital status, analyzing the distribution by combining the inadequate HL and problematic HL groups revealed a statistically significant difference (p = 0.033). Married individuals were more likely to have “inadequate or problematic HL” (60%) compared to single individuals (25%), whereas single individuals had a higher proportion of excellent HL (50%) compared to married individuals (6.7%) (Figure 1).
Figure 1 Distribution of HL levels by marital status.
For income levels, individuals with income exceeding expenses had a higher proportion of excellent HL (42.9%) compared to other groups, while those with income below expenses exhibited higher proportions in the inadequate and problematic HL categories (22.2%). Employment status revealed that nonworking participants had a higher proportion of adequate HL (40%), while working participants had a higher proportion of excellent HL (29.4%). However, none of these distributions—except for marital status—were statistically significant.
The impact of sociodemographic data on the TSOY-32 survey—Two-dimensional index
The relationship between sociodemographic variables and HL categories within the TS and DP/HP dimensions of the TSOY-32 survey was analyzed. Within the TS dimension, no statistically significant associations were observed between HL categories and gender, age groups, marital status, income level, or employment status (p = 0.080, p = 0.340, p = 0.196, p = 0.130, and p = 0.679, respectively).
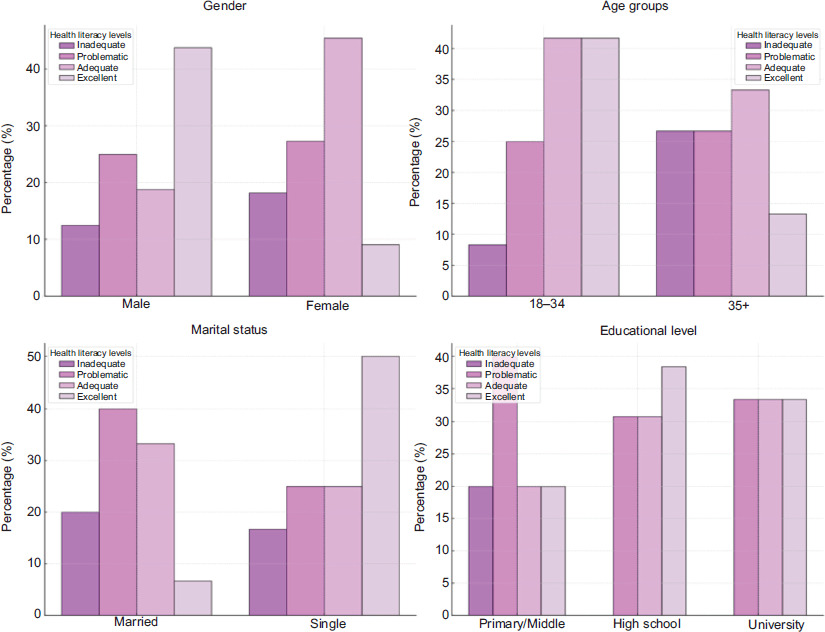
In contrast, the DP/HP dimension revealed statistically significant associations between HL categories and gender (p = 0.031), age groups (p = 0.042), marital status (p = 0.033), and educational level (p = 0.024) (Figure 2). Male participants demonstrated a higher proportion of excellent HL (43.8%) compared to females (9.1%), while females showed a higher proportion in the adequate HL category (45.5% vs. 18.8%). Among age groups, 41.7% of individuals aged 18–34 were in the excellent HL category, whereas only 13.3% of those aged 35 and above fell into this category. Accordingly, 26.7% of individuals aged 35 and above were in the inadequate HL category compared to 8.3% in the 18–34 age group. Regarding marital status, 40% of married participants were in the adequate HL category, while 6.7% were in the excellent HL category. Furthermore, 50% of single participants were in the excellent HL category. For educational levels, 20% of primary and middle school graduates were in the inadequate HL category, 30.8% of high school graduates were in the adequate HL category, and 33.3% of university graduates were in the excellent HL category. Additionally, no statistically significant associations were found between HL and income levels (p = 0.352) or employment status (p = 0.196) within the DP/HP dimension. However, 42.9% of individuals with income exceeding expenses fell into the excellent HL category, while 27.3% of those with income equal to expenses were in the inadequate HL category. Nonworking participants had a higher proportion in the adequate HL category (40%), whereas working participants had a higher proportion in the excellent HL category (29.4%). These differences, however, were not statistically significant.
Figure 2 Relationships between HL categories and gender, age groups, marital status, and education level in the disease prevention and health promotion dimension (p = 0.031, p = 0.042, p = 0.033, p = 0.024, respectively).
The impact of sociodemographic data on the TSOY-32 survey—Subcategories index
The analysis of HL subcategories and their associations with sociodemographic variables across the TS and DP/HP dimensions revealed noteworthy findings (Table 4). Among the general subcategories, a statistically significant relationship was found between understanding health-related information (UHRI) and gender and marital status (p = 0.013 and p = 0.049, respectively). A significant relationship was also observed between using/applying health-related information (UAHRI) and gender (p = 0.023). In contrast, no statistically significant relationship was found with any sociodemographic variable for accessing health-related information (AHRI) and evaluating health-related information (EHRI). In terms of dimensions, a statistically significant relationship was found between sociodemographic variables and subcategories within the TS dimension only between the age categorical subgroups and TS-EHRI (p = 0.026). Within the DP/HP dimension, statistically significant associations with sociodemographic variables were observed in the DP/HP-EHRI, DP/HP-UHRI, and DP/HP-UAHRI categories (Table 4).
Table 4 The impact of sociodemographic data on the TSOY-32/subcategories index.
| Using/applying health-related information, n (%) | |||||
|---|---|---|---|---|---|
| Gender Male Female |
3 (18.8) 2 (18.2) |
5 (31.3) 1 (9.1) |
3 (18.8) 8 (72.7) |
5 (31.3) 0 (0) |
0.023 |
| Understanding health-related information, n (%) | |||||
| Gender Male Female |
4 (25) 0 (0) |
3 (18.8) 3 (27.3) |
2 (12.5) 7 (63.6) |
7 (43.8) 1 (9.1) |
0.013 |
| Marital Status Married Single |
2 (13.3) 2 (16.7) |
6 (40) 0 (0) |
5 (33.3) 4 (33.3) |
2 (13.3) 6 (50) |
0.049 |
| Treatment and Services Evaluating health-related information, n (%) | |||||
| Age Groups, Years 18–34 ≥35 |
0 (0) 8 (53.3) |
4 (33.3) 2 (13.3) |
4 (33.3) 3 (20) |
4 (33.3) 2 (13.3) |
0.026 |
| Disease prevention/health promotion Evaluating health-related information, n (%) | |||||
| Marital Status Married Single |
6 (40) 2 (16.7) |
2 (13.3) 1 (8.3) |
7 (46.7) 4 (33.3) |
0 (0) 5 (41.7) |
0.048 |
| Age Groups, Years 18–34 ≥35 |
2 (16.7) 6 (40) |
1 (8.3) 2 (13.3) |
4 (33.3) 7 (46.7) |
5 (41.7) 0 (0) |
0.048 |
| Gender Male Female |
6 (37.5) 2 (18.2) |
0 (0) 3 (27.3) |
5 (31.3) 6 (54.5) |
5 (31.3) 0 (0) |
0.023 |
| Disease prevention/health promotion Using/applying health-related information, n (%) | |||||
| Gender Male Female |
6 (37.5) 3 (27.3) |
0 (0) 2 (18.2) |
2 (12.5) 5 (45.5) |
8 (50) 1 (9.1) |
0.028 |
| Marital Status Married Single |
7 (46.7) 2 (16.7) |
0 (0) 2 (16.7) |
6 (40) 1 (8.3) |
2 (13.3) 7 (58.3) |
0.012 |
| Disease prevention/health promotion Understanding health-related information, n (%) | |||||
| Gender Male Female |
5 (31.3) 1 (9.1) |
1 (6.3) 2 (18.2) |
3 (18.8) 7 (63.6) |
7 (43.8) 1 (9.1) |
0.037 |
Discussion
This study is of particular importance as it represents, to our knowledge, one of the first investigations specifically assessing HL in adults diagnosed with IEI. Using the validated TSOY-32, we aimed to provide insights into HL levels within this patient group. Our findings revealed that nearly half of the participants exhibited inadequate or problematic HL levels. Notably, the disease DP/HP dimension and its subcategories were significantly associated with sociodemographic variables such as gender, age group, marital status, and educational level. These results underscore the need to better understand the determinants of HL in this population.
Limited HL is a globally recognized concern. For example, in a study conducted in Turkey evaluating HL among patients presenting to the green triage area of a tertiary hospital emergency department, it was reported that 57.9% of patients had inadequate or problematic HL levels.13 Additionally, another Turkish study assessing HL among students receiving education in health-related fields demonstrated that 44.4% of the participants had inadequate or problematic HL despite their health-focused education.14 Furthermore, various studies conducted in the United States have also reported that nearly half of the participants possess limited HL levels.5 Our findings are consistent with previous national and international studies reporting low levels of HL. In particular, among individuals with chronic and complex conditions like IEI, inadequate HL may negatively impact treatment adherence, self-management, and long-term health outcomes. These results highlight the need for effective and targeted interventions to improve HL in this vulnerable patient group.
To support this need, only a limited number of studies have examined the dynamics of HL in the context of immunodeficiency. One such study, conducted in Germany, evaluated 209 patients with common variable immunodeficiency (CVID) and identified four subgroups based on perceived physical and mental health status. It reported significant differences in patient-reported outcomes such as HL and functional capacity across these subgroups.15 Notably, these HL-related differences were not found to be associated with clinical course or laboratory parameters. Furthermore, the same research group developed a training program to enhance HL, focusing on communication with physicians and health-related communication in the workplace. Patient feedback indicated high acceptability and perceived relevance of the intervention.16 These findings suggest that structured HL interventions are feasible and may address unmet needs in this population. However, these studies did not focus primarily on the relationship between HL and core sociodemographic variables. Our study, although based on a smaller sample, directly measured HL using a validated tool for general HL and statistically examined its associations with age, gender, education, and marital status. This perspective may help clarify how HL varies according to individual factors, contributing to the development of tailored and effective educational strategies.
Additional evidence from other chronic immune-mediated diseases further highlights the relevance of HL to both clinical and behavioral outcomes. For instance, in Chinese patients with rheumatoid arthritis, HL was inversely associated with disease activity markers such as erythrocyte sedimentation rate and joint involvement, while positively associated with self-efficacy and medication adherence.17 Similarly, a study involving African American women with systemic lupus erythematosus reported worse clinical outcomes among those with limited HL, suggesting that inadequate HL may exacerbate disease burden and increase vulnerability in specific patient subgroups.18 These findings highlight that HL can be addressed as a modifiable factor in chronic disease management.
In addition, studies in other chronic conditions, such as cancer, have confirmed a positive correlation between HL and treatment adherence.19–21 For instance, in patients receiving oral chemotherapy, higher HL was linked to better adherence and improved clinical outcomes.21 In our study, most IEI patients demonstrated “problematic” HL in the TS dimension while showing relatively higher proficiency in DP/HP. These patterns underscore the need for personalized educational interventions that reflect individual HL profiles and promote active engagement in care processes.
In the dimension of DP/HP, significant associations were found between HL and sociodemographic factors such as gender, age, marital status, and education level, suggesting that this dimension is considerably influenced by individuals’ sociodemographic characteristics; however, the absence of significant relationships between sociodemographic variables and the TS dimension suggests that this dimension is less influenced by these variables. Our findings indicated that, regarding DP/HP, males predominantly exhibited an “excellent” level of HL, whereas females more frequently demonstrated an “adequate” level. However, no significant gender differences were identified in the TS dimension. These results are both consistent with and contradictory to various studies in the literature.14,22–24 Such discrepancies might be attributable to differences in individuals’ sociodemographic characteristics, social roles, and gender-based expectations. The higher proficiency observed among females in the EHRI subcategory warrants further investigation to understand underlying factors.
Our study found higher HL among individuals with higher income, although this relationship was not statistically significant. This observation aligns with prior research and might be explained by the higher socioeconomic status providing more resources, improved access to health information, and greater opportunities for preventive health behaviors.25 Larger scale studies are warranted to further investigate this potential association. Additionally, our findings revealed that adults aged 18–34 exhibited higher HL levels compared to those aged 35 and older, consistent with previous studies indicating superior information-seeking skills and technology use among younger adults.14 The lower HL observed among older adults underscores the need for age-specific educational programs and supportive interventions, particularly targeting patients with IEI. Regarding education level, our study observed that HL increased with higher education levels; however, this difference was not statistically significant. While this finding aligns with studies reporting improved HL with increasing educational attainment, existing literature also suggests that the positive relationship between education level and HL may not always be direct or consistent.6,14,26,27 Hence, educational interventions should be inclusively designed to address individuals across all education levels.
To our knowledge, this is among the first studies to assess general HL in individuals with IEI. The 32-item TSOY-32, a validated and reliable instrument for the general Turkish population, had previously been applied in both the general population and various chronic disease groups.10,13,14,28 Although not specifically developed or validated for IEI populations, it provides a structured means to evaluate general HL, which was the primary focus of our study. Our findings offer preliminary insight into HL profiles in this group and suggest that older adults, married individuals, and those with lower educational attainment may be particularly at risk. This underscores the need for targeted educational interventions tailored to these subgroups. Moreover, the two-dimensional, four subprocess structure of the TSOY-32 enabled a detailed characterization of patients’ HL patterns. Future studies could consider developing or validating disease-specific HL tools to complement these findings and enhance context-specific assessment.
However, several limitations should be acknowledged. This study was conducted in a single tertiary care center with a relatively small sample size that may limit generalizability. Although our institution serves as a national referral center for adult IEI patients, participation was affected by personal constraints (e.g., lack of time or interest), and some patients were not accessible due to intermittent follow-up through referral-based care models. To maintain sample homogeneity, patients not receiving regular IGRT were excluded. Nevertheless, approximately three-quarters of patients who routinely received IGRT at our center agreed to participate.
Despite its limitations, this study provides valuable preliminary data on HL in adults with IEI and highlights the importance of personalized educational approaches. Based on our clinical experience, practical interventions may include simplified, visually supported materials for patients with limited HL; brief individualized sessions integrated into routine outpatient care; short video-based modules; and reinforcement of key messages by trained nursing staff. These strategies can enhance communication, foster engagement, and support effective disease management.
In conclusion, our findings indicate that a substantial proportion of IEI patients have inadequate or problematic HL, which may negatively affect treatment adherence and clinical outcomes. Tailoring education to individual HL levels and promoting active patient involvement in care may help mitigate these challenges. Regular monthly IGRT visits offer direct contact with healthcare providers, presenting a key opportunity to deliver such interventions. Future multicenter studies with larger samples are needed to identify factors affecting HL in IEI populations and to assess the impact of targeted educational strategies.
Author Contributions
All authors contributed equally to this article.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
None.
REFERENCES
1 Ratzan SC, Parker RM. Introduction. In: Selden CR, Zorn M, Ratzan SC, Parker RM (eds.), National Library of Medicine Current Bibliographies in Medicine: Health Literacy. NLM Pub. no. CBM 2000–1. Bethesda, MD: National Institutes of Health, U.S. Department of Health and Human Services; 2000.
2 Paasche-Orlow MK, Parker RM, Gazmararian JA, Nielsen-Bohlman LT, Rudd RR. The prevalence of limited health literacy. J Gen Intern Med. 2005;20(2):175–84. 10.1111/j.1525-1497.2005.40245.x
3 Andrus MR, Roth MT. Health literacy: A review. Pharmacotherapy. 2002;22(3):282–302. 10.1592/phco.22.5.282.33191
4 Katz P, Dall’Era M, Trupin L, Rush S, Murphy LB, Lanata C, et al. The impact of limited health literacy on patient-reported outcomes in systemic lupus erythematosus. Arthritis Care Res. 2017. 10.1002/acr.24361
5 Kirsch I, Jungeblut A, Jenkins L, Kolstad A. Adult literacy in America: A first look at the findings of the National Adult Literacy Survey. Washington, DC: National Center for Education Statistics, U.S. Department of Education; 1993.
6 Glassman SD, Carreon LY, Brown ME, Jones JS, Edward J, Li J, et al. The impact of health literacy on health status and resource utilization in lumbar degenerative disease. Spine J. 2019;19(4):711–6. 10.1016/j.spinee.2018.10.012
7 Pieniawska-Śmiech K, Pasternak G, Lewandowicz-Uszyńska A, Jutel M. Diagnostic Challenges in Patients with Inborn Errors of Immunity with Different Manifestations of Immune Dysregulation. J Clin Med. 2022 Jul 20;11(14):4220. 10.3390/jcm11144220
8 Tangye SG, Al-Herz W, Bousfiha A, Cunningham-Rundles C, Franco JL, Holland SM, et al. Human inborn errors of immunity: 2022 update on the classification from the International Union of Immunological Societies Expert Committee. J Clin Immunol. 2022;42(7):1473–1507. 10.1007/s10875-022-01289-3
9 Baloh CH, Chong H. Inborn errors of immunity. Prim Care. 2023;50(2):253–68. 10.1016/j.pop.2022.12.001
10 Okyay P, Abacıgil F. Türkiye sağlık okuryazarlığı ölçekleri güvenilirlik ve geçerlilik çalışması. Avrupa sağlık okuryazarlığı ölçeği Türkçe uyarlaması (ASOY-TR). Mayıs. 2016:24–41.
11 Seidel MG, Kindle G, Gathmann B, Quinti I, Buckland M, van Montfrans J, et al. The European Society for Immunodeficiencies (ESID) Registry working definitions for the clinical diagnosis of inborn errors of immunity. J Allergy Clin Immunol Pract. 2019;7(6):1763–70. 10.1016/j.jaip.2019.02.004
12 HLS-EU Consortium. Comparative report of health literacy in eight EU member states. The European Health Literacy Survey HLS-EU; 2012. Available from: http://www.health-literacy.eu
13 Özdemir S, Algın A, Akça HŞ, Eroğlu SE. Health literacy in the emergency department: A cross-sectional descriptive study. Eurasian J Emerg Med. 2020;19(2):94–7.
14 Yılmaz Güven D, Bulut H, Öztürk S. Sağlık bilimleri fakültesi öğrencilerinin sağlık okuryazarlığı düzeylerinin incelenmesi. J Hist Cult Art Res. 2018;7(2):400–9. 10.7596/taksad.v7i2.1511
15 Bayrhuber M, Tinsel I, Goldacker S, Kindle G, Warnatz K, Farin E, et al. Perceived health of patients with common variable immunodeficiency–A cluster analysis. Clin Exp Immunol. 2019;196(1):76–85. 10.1111/cei.13252. Epub 2019 Jan 13. PMid: 30637715; PMCID: PMC6422638.
16 Bayrhuber M, Tinsel I, Goldacker S, Farin E, Warnatz K, Nieters A. Entwicklung einer schulung zur förderung der gesundheitskompetenz von patienten mit variablem immundefekt (CVID) [Development of an intervention to enhance health literacy of patients with common variable immunodeficiency (CVID)]. Gesundheitswesen. 2021;83(3):195–7. 10.1055/a-1005-7235. Epub 2019 Oct 15. PMid: 31614384.
17 Liu T, Meng W, Wang W, Sun G, Chen X, Lu Y, et al. A cross-sectional study of predictive factors of health literacy among rheumatoid arthritis patients in China. Front Psychol. 2024;15:1390442. 10.3389/fpsyg.2024.1390442. PMid: 38993349; PMCID: PMC11236717.
18 Maheswaranathan M, Boan AD, Ramakrishnan V, Johnson H, Rose J, Dismuke-Greer CL, et al. Association of limited health literacy with clinical and patient-reported outcomes in individuals with systemic lupus erythematosus. ACR Open Rheumatol. 2024;6(11):780–9. 10.1002/acr2.11719. Epub 2024 Aug 18; PMCID: PMC11557983. PMid: 39155276;.
19 Saqlain M, Riaz A, Malik MN, Khan S, Ahmed A, Kamran S, et al. Medication adherence and its association with health literacy and performance in activities of daily livings among elderly hypertensive patients in Islamabad, Pakistan. Medicina. 2019;55(5):163. 10.3390/medicina55050163
20 Ngoh LN. Health literacy: A barrier to pharmacist-patient communication and medication adherence. J Am Pharm Assoc. 2009;49(5):e132–46. 10.1331/JAPhA.2009.07075
21 Gönderen Çakmak HS, Uncu D. Relationship between health literacy and medication adherence of Turkish cancer patients receiving oral chemotherapy. Asia Pac J Oncol Nurs. 2020;7(4):365–9. 10.4103/apjon.apjon_30_20
22 Almaleh R, Helmy Y, Farhat E, Hasan H, Abdelhafez A. Assessment of health literacy among outpatient clinics attendees at Ain Shams University Hospitals, Egypt: A cross-sectional study. Public Health. 2017;151:137–45. 10.1016/j.puhe.2017.06.024
23 Duong TV, Chang PW, Yang SH, Chen MC, Chao WT, Chen T, et al. A new comprehensive short-form health literacy survey tool for patients in general. Korean Soc Nurs Sci. 2017;11(1):30–5. 10.1016/j.anr.2017.02.001
24 Javadzade SH, Sharifirad G, Radjati F, Mostafavi F, Reisi M, Hasanzade A. Relationship between health literacy, health status, and healthy behaviors among older adults in Isfahan, Iran. J Educ Health Promot. 2012;1:31. 10.4103/2277-9531.100160
25 Ozdemir H, Alper Z, Uncu Y, Bilgel N. Health literacy among adults: A study from Turkey. Health Educ Res. 2010;25(3):464–77. 10.1093/her/cyp068
26 Bakker CJ, Koffel JB, Theis-Mahon NR. Measuring the health literacy of the Upper Midwest. J Med Libr Assoc. 2017;105(1):34–43. 10.5195/jmla.2017.105
27 Newsome C, Mallawaarachchi I, Conklin J, Ray G. Health literacy of student pharmacists. Curr Pharm Teach Learn. 2018;10(3):340–3. 10.1016/j.cptl.2017.11.005
28 Karataş G, Yava A, Tosun N, Koyuncu A. Hipertansiyon hastalarında öz etkililik ve sağlık okuryazarlığının değerlendirilmesi: Güneydoğu Anadolu örneği. Turk J Cardiovasc Nurs. 2024;15(37):79–86.