
Download
ORIGINAL ARTICLE
Living at risk: Exploring the psychological effects of childhood food allergy on mothers
Elif Küçüka*, Fatih Çiçekb
aDepartment of Psychiatry, Yuksek Ihtisas University, Ankara, Turkey
bDepartment of Pediatrics, İstinye University, İstanbul, Turkey
Abstract
Objectives: Food allergy (FA) is a growing public health concern, imposing significant psychosocial burdens on families and necessitating strict allergen avoidance. The unpredictability of severe reactions is associated with increased anxiety, dietary restrictions, and reduced quality of life.
Methods: We conducted a cross-sectional study including 77 mothers of children (0–12 years) with FA and 71 mothers of healthy children. Participants completed the Spielberger State-Trait Anxiety Inventory (STAI), Zarit Caregiver Burden Scale (ZCBS), and European Health Impact Scale (EUROHIS-QOL). Statistical analyses compared anxiety, caregiver burden, and quality of life between groups and explored sociodemographic factors.
Results: Mothers in the FA group had significantly higher state anxiety (STAI-S) (P < 0.001) and ZCBS scores (P < 0.001) compared to controls. However, trait anxiety (STAI-T) did not differ significantly between groups (P = 0.508). Additionally, mothers of children with FA reported lower EUROHIS-QOL scores (P = 0.009). Low maternal educational levels (P = 0.005) and middle-range income levels ($500–1000/month, P = 0.027) were significantly associated with higher anxiety and caregiver burden. Cow’s milk protein allergy (CMPA) specifically increased trait anxiety (P = 0.035) and reduced mothers’ quality of life (P = 0.003). No significant associations were found between anxiety or caregiver burden and anaphylaxis or other allergenic triggers.
Conclusion: Food allergy significantly elevates maternal anxiety and caregiving burden, and reduces quality of life, especially in CMPA cases. Sociodemographic factors exacerbate these effects, highlighting the need for comprehensive, multidimensional interventions. Psychological support and broader public awareness initiatives may help alleviate adverse outcomes and improve caregiver well-being.
Key words: anxiety, burden of care, food allergy, mother, quality of life
*Corresponding author: Elif Küçük, Department of Psychiatry, Yüksek Ihtisas University, Ankara, Turkey. Email address: [email protected]
Recevied 27 March 2025; Accepted 29 June 2025; Available online 1 September 2025
Copyright: Küçük E and Çiçek F
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introductıon
Food allergy (FA) is an important public health concern, with increasing prevalence reported in recent years.1–3 FA affects approximately 10% of infants and 4–5% of older children.4 Management primarily involves avoiding exposure to allergens and implementing a treatment plan in case of accidental exposure.5 In some cases, exposure to food allergens can be life-threatening. While FA-related anaphylaxis is rare, the estimated incidence of fatal food anaphylaxis is 1.81 per million people per year.6
The unpredictability of severe allergic reactions significantly impacts families, resulting in heightened anxiety, dietary restrictions, and decreased quality of life.7 The constant necessity to avoid allergenic foods can limit social activities, leading to social isolation.8 Routine daily activities, such as meal preparation, school attendance, or dining out, can impose substantial psychosocial burdens.9 Research has highlighted that families of children with FA experience a reduction in their quality of life.8–10 Children with FA and their families have reported experiencing anxiety and depressive symptoms due to these changes.11,12 Caregivers of children with a history of anaphylaxis also tend to adopt a more protective and cautious attitude.13 These findings highlight that FAs impact not only physical health but also psychological well-being. Therefore, understanding the psychosocial burden this situation places on families is of great importance.
Social support has been identified as a protective factor against psychiatric symptoms and disorders among families of children with FA.14 However, research on quality of life, caregiver burden, and psychological effects among these families, especially in our country, remains limited. This lack of data hampers the development of comprehensive support systems.
In this study, we aim to assess the quality of life, caregiver burden, and anxiety levels among mothers of children with FA, examine the influence of demographic factors, and compare these outcomes to those of mothers with healthy children.
Methods
Study design and participants
This cross-sectional study included mothers of children aged 0–12 years diagnosed with FA attending the Pediatric Allergy and Immunology Clinic at Kartal Dr. Lutfi Kirdar City Hospital from June 1, 2023, to September 1, 2023. The control group comprised mothers of children aged 0–12 years visiting the Pediatric Health and Disease Clinic for routine checkups without active complaints (e.g., vaccinations, monthly assessments, nutritional education, growth, and development monitoring). Exclusion criteria included metabolic diseases, immune deficiencies, chronic heart diseases, endocrine, renal, pulmonary, gastrointestinal, hepatic, central nervous system diseases, malignancies, or other chronic illnesses in children or family members. Mothers with active psychiatric conditions, those receiving psychiatric medications, or those unwilling to participate were also excluded. Written informed consent was obtained from all participants after detailed explanations. Participants completed a demographic questionnaire, Spielberger State-Trait Anxiety Inventory (STAI), Zarit Caregiver Burden Scale (ZCBS), and European Health Impact Scale (EUROHIS-QOL).
Ethical approval was granted by the Ethics Committee of Kartal Dr. Lutfi Kirdar City Hospital (Approval No: 2023/514/250/29, Date: May 29, 2023), and the study was conducted per the Declaration of Helsinki. A sample size of at least 140 participants (70 per group) was determined using G*Power 3.1, considering an alpha error of 0.05, power of 0.9, and effect size of 0.5.
Food allergy
Food Allergy diagnosis was made by pediatric allergy specialists based on clinical history, positive skin prick test results, and/or specific IgE testing. Food challenge tests were performed when clinically indicated.15
Spielberger State-Trait Anxiety Inventory
Developed by Spielberger et al.,16 the Turkish validity of the scale was established by Öner.17 The scale consists of two subscales, each containing 20 items that assess state and trait anxiety. The State Anxiety Inventory (STAI-S) measures how an individual feels at a particular moment under specific conditions, while the Trait Anxiety Inventory (STAI-T) reflects how an individual generally feels. Scores on the scale range from 20 to 80, with higher scores on each subscale indicating higher levels of anxiety.
Zarit Caregiver Burden Scale
Developed by Zarit et al. and validated in Turkish by Özlü et al., the Zarit Caregiver Burden Scale (ZCBS) consists of 19 items rated from 1 to 5, with scores ranging from 19 to 95.18,19 Higher scores indicate increased distress and caregiver burden.
European Health Impact Scale-8 (EUROHIS-QOL)
EUROHIS-QOL is an 8-item scale adapted from the World Health Organization Quality of Life Scale. This scale covers various topics, including quality of life, health status, energy level, independence in daily activities, self-esteem, social relationships, economic situation, and living environment. The scale scores each item from 0 (not at all) to 5 (completely).20 Eser et al. conducted the Turkish validity and reliability study of the scale in 2010. There are various methods to calculate the scale scoring, including taking the average of responses, summing the scores, or converting the total score to a scale of 100.21 Higher scores represent a better quality of life.
Statistical analysis
The data were analyzed using IBM SPSS Statistics Standard Concurrent User V 29 (IBM Corp., Armonk, New York, USA). Descriptive statistics were presented as the number of units (n), percentage (%), mean ± standard deviation, median, interquartile range, minimum, and maximum values. We assessed the normal distribution of numerical variables using the Shapiro–Wilk normality test. The homogeneity of variances among groups was analyzed using Levene’s test. If the data had a normal distribution, we performed independent sample t-tests for comparisons between two groups of numerical variables; otherwise, we used the Mann–Whitney U test. We conducted one-way analysis of variance for comparisons among three groups of numerical variables, based on the normal distribution of the data. For comparisons of categorical variables among groups, Pearson’s chi-square analysis was employed. If the results of the chi-square analysis were significant, we conducted subgroup analyses using the Bonferroni-corrected two-proportion Z test. Based on the normality of the data, we used Pearson or Spearman correlation coefficients to compare numerical variables with each other. P-value < 0.05 was considered statistically significant.
Results
This cross-sectional study included 77 mothers of children aged 0–12 years diagnosed with FA and 71 mothers of healthy children. As shown in Table 1, the average age of mothers did not significantly differ between the FA group and the control group (P = 0.213). Likewise, there was no significant difference in the median age of children, which was 18.0 months (IQR: 22.5) in the FA group and 24.0 months (IQR: 27.0) in the control group (P = 0.128). Gender distribution between groups also showed no significant difference, with 44.2% (n = 34) females in the FA group and 59.2% (n = 42) females in the control group (P = 0.068). The groups did not differ significantly in terms of maternal education levels (P = 0.124) or employment status (P = 0.074). The median duration of food allergy diagnosis was 12 months (IQR: 13.5), and 13.0% (n = 10) of mothers reported having another child with FA (Table 1).
Table 1 Comparison of sociodemographic characteristics between food allergy and control groups.
| Groups | |||
|---|---|---|---|
| Food allergy (n = 77) | Control (n = 71) | P | |
| Mother’s age (year) | 31.8 ± 5.1 | 30.9 ± 4.3 | 0.213‡ |
| Child’s age (month) | 18.0 (22.5) | 24.0 (27.0) | 0.128† |
| Gender, n (%) | |||
| Girl | 34 (44.2) | 42 (59.2) | 0.068& |
| Boy | 43 (55.8) | 29 (40.8) | |
| Mother’s education level, n (%) | |||
| Primary and Secondary school | 9 (11.7) | 16 (22.5) | 0.124& |
| High school and above | 68 (83.3) | 55 (77.5) | |
| Employment status, n (%) | |||
| Employed | 15 (19.5) | 24 (33.8) | 0.074& |
| Unemployed | 62 (80.5) | 47 (66.2) | |
| Family income, n (%) | 0.001& | ||
| <500 $ | 17 (22.1)a | 24 (33.8)a | |
| 500-1000 $ | 31 (40.3)a | 9 (12.7)b | |
| >1000 $ | 29 (37.6)a | 38 (53.5)a | |
| Duration of food allergy (months) | 12 (13.5) | ||
| Food allergy in another child, n (%) | 10 (13.0) | ||
n: Unit (patient); number %: Column per cent, numerical data are given as mean ± standard deviation, median (minimum–maximum) or median (interquartile range) values; ‡: Independent samples t test; †: Mann–Whitney U test, &: Pearson chi-square test. P < 0.05 is statistically significant.
a,bindicate differences between groups in each row. There is no statistical difference between groups with the same superscripts.
The most frequently reported allergenic foods were eggs (72.7%, n = 56) and cow’s milk (66.2%, n = 51), followed by hazelnuts (16.9%, n = 13) and peanuts (15.6%, n = 12). Other allergens, including sesame, wheat, fruit, and fish, were reported less frequently. The most commonly observed clinical symptoms among children with FA were redness (88.3%, n = 68), restlessness (84.4%, n = 65), and itching (81.8%, n = 63). Additional symptoms observed were rashes (49.4%, n = 38), diarrhea (27.3%, n = 21), stomach ache (18.2%, n = 14), vomiting (10.4%, n = 8), respiratory distress or wheezing indicative of anaphylaxis (6.5%, n = 5), and constipation (5.2%, n = 4) (Table 2).
Table 2 Foods causing allergic reactions and observed symptoms.
| Allergic foods | n | % |
|---|---|---|
| Egg | 56 | 72.7 |
| Cow’s milk | 51 | 66.2 |
| Hazelnut | 13 | 16.9 |
| Peanut | 12 | 15.6 |
| Sesame | 3 | 3.9 |
| Wheat | 1 | 1.3 |
| Fruit | 1 | 1.3 |
| Fish | 1 | 1.3 |
| Others | 8 | 10.4 |
| Symptoms | ||
| Redness | 68 | 88.3 |
| Restlessness | 65 | 84.4 |
| Itching | 63 | 81.8 |
| Rashes | 38 | 49.4 |
| Diarrhea | 21 | 27.3 |
| Stomach ache | 14 | 18.2 |
| Vomiting | 8 | 10.4 |
| Shortness of breath - Wheezing | 5 | 6.5 |
| Constipation | 4 | 5.2 |
n: Unit (participant) number; %: Column per cent.
As presented in Table 3, mothers in the FA group had significantly higher scores on the STAI-S (P < 0.001) and ZCBS (P < 0.001) compared to mothers of healthy children. There was no significant difference in STAI-T scores between groups (P = 0.508). Mothers in the FA group also reported significantly lower EUROHIS-QOL scores (P = 0.009). Analysis by sociodemographic characteristics revealed that mothers with primary or secondary education had significantly higher STAI-T scores compared to those with higher education levels (P = 0.005). Caregiver burden was significantly higher in mothers earning $500–1000 per month (46.4 ± 12.3) compared to those earning less than $500 (40.4 ± 9.0) or more than $1000 (42.7 ± 9.1) per month (P = 0.027). Furthermore, mothers with another child who had FA showed significantly higher ZCBS scores (P = 0.024). No other significant associations were found between anxiety, caregiver burden, or quality of life scores and maternal age, child age, child gender, number of siblings, employment status, or duration of food allergy diagnosis.
Table 3 Comparison of scale scores by groups and sociodemographic characteristics.
| STAI-S | STAI-T | ZCBS | EUROHIS-QOL | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| rho | Mean± SD | P | rho | Mean ± SD | P | rho | Mean ± SD | P | rho | Mean ± SD | P* | |
| Groups | ||||||||||||
| Food allergy | 42.2 ± 10.7 | <0.001‡ | 43.5 ± 8.7 | 0.508* | 46.1 ± 11.9 | <0.001* | 27.0 ± 5.4 | 0.009* | ||||
| Control | 34.9 ± 8.3 | 42.6 ± 8.3 | 39.8 ± 6.6 | 29.1 ± 4.3 | ||||||||
| Mother’s age | 0.083¥ | 0.315 | 0.056¥ | 0.497 | 0,037¥ | 0.651 | -0,003¥ | 0.968 | ||||
| Child’s age | -0.154 | 0.062 | -0.007 | 0.928 | -0.035 | 0.674 | -0.063 | 0.447 | ||||
| Child’s age,(yr) | ||||||||||||
| <3 | 39.6 ± 10.7 | 0.066* | 42.9 ± 8.7 | 0.710* | 39.2 ± 8.8 | 0.339* | 28.2 ± 5.0 | 0.389* | ||||
| >3 | 36.1 ± 8.5 | 43.5 ± 8.1 | 42.4 ± 10.2 | 27.4 ± 5.0 | ||||||||
| Gender | ||||||||||||
| Girl | 37.4 ± 10.4 | 0.104* | 42.4 ± 8.4 | 0.338* | 42.0 ± 10.2 | 0.203* | 28.1 ± 5.1 | 0.832* | ||||
| Boy | 40.2 ± 10.0 | 43.8 ± 8.6 | 44.2 ± 10.2 | 27.9 ± 4.9 | ||||||||
| Number of siblings | -0.019 | 0.823 | 0.106 | 0.200 | -0.074 | 0.374 | -0.057 | 0.493 | ||||
| Mother’s education level | ||||||||||||
| Primary and secondary | 39.2 ± 10.5 | 0.825* | 47.4 ± 10.0 | 0.005* | 42.1 ± 8.6 | 0.607* | 27.2 ± 5.1 | 0.369* | ||||
| school | ||||||||||||
| High school and above | 38.7 ± 10.3 | 42.2 ± 7.9 | 43.3 ± 10.5 | 28.2 ± 5.0 | ||||||||
| Employment status | ||||||||||||
| Employed | 38.9 ± 9.9 | 0.899* | 43.2 ± 7.6 | 0.902* | 44.5 ± 9.1 | 0.341* | 27.9 ± 4.1 | 0.917* | ||||
| Unemployed | 38.7 ± 10.4 | 43.0 ± 8.8 | 42.6 ± 10.6 | 28.0 ± 5.3 | ||||||||
| Family income | ||||||||||||
| <$500 | 38.5 ± 10.6 | 0.302Ф | 44.0 ± 8.8 | 0.271Ф | 40.4 ± 9.0 | 0.027“ | 27.1 ± 5.0 | 0.23Ф | ||||
| $500-1000 | 40.8 ± 11.3 | 44.2 ± 9.1 | 46.4 ± 12.3 | 27.8 ± 5.5 | ||||||||
| >$1000 | 37.7 ± 9.3 | 41.8 ± 7.9 | 42.7 ± 9.1 | 28.7 ± 4.6 | ||||||||
| Duration of food allergy | -0.048 | 0.680 | -0.111 | 0.339 | 0.014 | 0.903 | -0.109 | 0.346 | ||||
| Food allergy in another child | ||||||||||||
| Yes | 44.9 ± 9.9 | 0.403* | 48.1 ± 6.9 | 0.073* | 54.0 ± 11.2 | 0.024* | 26.8 ± 3.4 | 0.901* | ||||
| No | 41.9 ± 10.8 | 42.8 ± 8.8 | 44.9 ± 11.6 | 27.0 ± 5.6 | ||||||||
| Anaphylaxis | ||||||||||||
| Yes | 36.8 ± 8.9 | 0.241 | 37.0 ± 6.8 | 0.083 | 41.8 ± 15.7 | 0.405 | 28.6 ± 6.2 | 0.495 | ||||
| No | 42.6 ± 10.7 | 44.0 ± 8.7 | 46.4 ± 11.7 | 26.9 ± 5.3 | ||||||||
‡: Independent samples t test; rho: Spearman correlation coefficient; ¥: Pearson correlation coefficient; Ф: One-way analysis of variance. P < 0.05 is statistically significant.
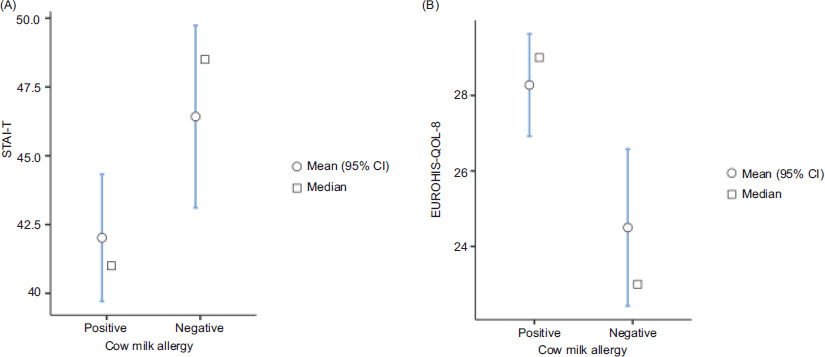
Evaluation based on specific allergenic triggers indicated that only cow’s milk protein allergy (CMPA) was significantly associated with elevated STAI-T scores (P = 0.035) and decreased EUROHIS-QOL scores (P = 0.003). Egg allergy was not significantly associated with differences in any of the assessed scales (STAI-T, P = 0.472; STAI-S, P = 0.615; ZCBS, P = 0.991; EUROHIS-QOL, P = 0.671) (Figure 1) (Table 4).
Figure 1 Comparison of STAI-T and EUROHIS-QOL scores in mothers of children with CMPA and other food allergies.
Table 4 Comparison of scales based on food allergy triggers.
| Group | N | Mean | P | ||
|---|---|---|---|---|---|
| Cow’s milk protein allergy | STAI-T | Yes | 51 | 42.0 ± 8.4 | 0.035 |
| No | 26 | 46.4 ± 8.6 | |||
| STAI-S | Yes | 12 | 44.2 ± 8.6 | 0.502 | |
| No | 65 | 41.9 ± 11 | |||
| ZCBS | Yes | 51 | 45.5 ± 12.0 | 0.521 | |
| No | 26 | 47.3 ± 11.8 | |||
| EUROHIS-QOL | Yes | 51 | 28.3 ± 5.0 | 0.003 | |
| No | 26 | 24.5 ± 5.4 | |||
| Egg Allergy |
STAI-T | Yes | 56 | 43.9 ± 7.9 | 0.472 |
| No | 21 | 42.3 ± 10.6 | |||
| STAI-S | Yes | 56 | 42.6 ± 10.4 | 0.615 | |
| No | 21 | 41.2 ± 11.7 | |||
| ZCBS | Yes | 56 | 46.1 ± 11.7 | 0.991 | |
| No | 21 | 46.1 ± 12.7 | |||
| EUROHIS-QOL | Yes | 56 | 27.2 ± 4.8 | 0.671 | |
| No | 21 | 26.6 ± 6.7 |
P < 0.05 is statistically significant.
As presented in Table 5, significant positive correlations were found between STAI-S and STAI-T scores (r = 0.572, P < 0.001). Similarly, ZCBS scores showed significant positive correlations with both STAI-S (r = 0.416, P < 0.001) and STAI-T (r = 0.574, P < 0.001) scores. Conversely, significant negative correlations were observed between EUROHIS-QOL scores and STAI-S (r = −0.306, P = 0.007), STAI-T (r = −0.518, P < 0.001), and ZCBS (r = −0.501, P < 0.001) scores, highlighting that increased anxiety and caregiver burden were associated with reduced quality of life.
Table 5 Relationships between scale scores.
| STAI-S | STAI-T | ZCBS | ||||
|---|---|---|---|---|---|---|
| r | P | r | P | r | P | |
| STAI-T | 0.572 | <0.001 | ||||
| ZCBS | 0.416 | <0.001 | 0.574 | <0.001 | ||
| EUROHIS-QOL | -0.306 | 0.007 | -0.518 | <.001 | -0.501 | <0.001 |
r: Pearson correlation coefficient.
Discussion
It is crucial to understand and address the potential psychosocial effects of FA on families to optimize FA management strategies and provide targeted support for parents. Numerous studies in the literature have separately evaluated caregiver burden, depression, and anxiety in families with food-allergic children.8,22–24 Living with constant concerns about potential allergic reactions and the necessity for rigorous allergen avoidance significantly impacts the daily routines of both children with FA and their families.25 In the present study, we evaluated the quality of life, caregiver burden, and anxiety levels among mothers of children diagnosed with FA and compared these outcomes with mothers of healthy children.
Previous studies have emphasized that the greatest psychological impact of FA in children is on mothers.26 Accordingly, this study specifically targeted mothers to explore the psychosocial consequences of FA on families. Consistent with existing literature, we employed the STAI to assess parental anxiety related to their child’s FA.27,28 The STAI effectively distinguishes between state anxiety—reflecting transient feelings of anxiety experienced during specific situations—and trait anxiety, indicative of a person’s enduring predisposition to perceive situations as stressful.28 State anxiety, therefore, captures maternal anxiety at the moment of FA assessment, while trait anxiety reflects more generalized anxiety tendencies. Goodwin et al. previously reported no significant differences in anxiety or depression between families of children with FA and those without.29 However, in alignment with the majority of published studies, our findings revealed significantly higher anxiety levels among mothers of children with FA compared to controls.22,27,28 Kılıç et al. similarly reported increased anxiety, depression, and caregiver burden in mothers of FA-affected children.8 Our results demonstrated significantly elevated state anxiety among mothers in the FA group; however, trait anxiety did not differ significantly from controls. This contrasts with Soller et al., who reported a correlation between elevated state anxiety and heightened FA-related anxiety among parents.30 Possible explanations for this discrepancy may include differences in sample characteristics, such as the severity of allergic reactions experienced, parental educational levels, socioeconomic status, and availability of social support systems. Methodological differences, including variations in the timing of assessments or the specific instruments used to measure FA-related anxiety, may also have contributed to these contrasting results. Further research addressing these factors could help clarify the nuanced relationship between situational anxiety responses and general anxiety predisposition among parents managing food allergies. Similar to prior research, our data did not identify associations between maternal anxiety levels and child age, gender, number of children, or previous anaphylaxis history.28 Nevertheless, mothers with only primary education exhibited significantly higher STAI-T scores compared to those with higher educational attainment. Charana et al.,31 in a study conducted in Greece, also found higher STAI-T anxiety among parents with either low or high education levels compared to intermediate education levels. This suggests that individuals with lower educational attainment might face greater challenges in disease understanding and management, consequently experiencing increased anxiety.
Consistent with the previous literature, our findings indicate that mothers of children with FA experience a significantly greater caregiver burden compared to mothers of healthy children.5,8,12,32 Our results also align with studies demonstrating that this caregiver burden is closely associated with elevated anxiety levels among caregivers managing FA.33,34 Howe et al. reported that multiple factors—including multiple food allergies, the age at initial allergic reaction, socioeconomic status, atopic dermatitis, and the risk of anaphylaxis—can markedly influence caregiver quality of life. Their findings particularly highlighted that allergies to milk or eggs notably increased the caregiving burden.35 Parents described the experience as caring for a child “living at risk.”36 Similarly, our study found that low family income and having another child diagnosed with FA were significant factors contributing to increased caregiver burden. Unlike other studies, however, our findings did not demonstrate an increased caregiver burden associated with anaphylaxis, which we attribute to the relatively small number of anaphylactic cases in our sample. While previous studies frequently employed the Food Allergy Quality of Life–Parental Burden Questionnaire to evaluate parental quality of life and caregiver burden, we utilized the ZCBS in this study due to the absence of a validated Turkish version of the former instrument.10,34
Previous research has consistently highlighted that caregivers of children with chronic illnesses exhibit more psychiatric symptoms and experience a lower overall quality of life.37–39 In line with these findings, our study also demonstrated reduced quality of life among families caring for children with FA.40,41 Parents of children with FA commonly reported experiencing constant vigilance and an overwhelming need to monitor their child’s daily activities closely. These concerns were frequently attributed to inadequate awareness about FA in educational settings and insufficient support from healthcare providers.42 The necessity to strictly avoid allergenic foods can significantly restrict social participation, dietary habits, and lead to social isolation for both the affected child and their family, further diminishing their quality of life.8 Mandell et al. also emphasized that dietary restrictions due to FA have profound implications for the entire family, including siblings, who often also modify their behavior to prevent exposure to allergens.43 Interventions such as ensuring widespread availability of epinephrine auto-injectors in schools, enhancing food labeling clarity to better support parental understanding, and establishing parent-to-parent support groups have the potential to significantly enhance the quality of life for families impacted by FA.10 Additionally, it is essential for healthcare professionals to recognize the psychological burden that FA places on families and to refer patients and caregivers for appropriate psychological or psychiatric support when necessary.
In our patient group, CMPA and egg allergy were identified as the most common allergy triggers. Our findings demonstrated that CMPA significantly affected both trait anxiety and quality of life among caregivers. Abrams et al. similarly reported that avoiding cow’s milk often results in substantial social restrictions, placing children with CMPA at a higher risk of psychosocial difficulties compared to those with other food allergies.44 In our country, cow’s milk and dairy products play a prominent role in traditional dietary patterns. Previous research highlights that the impact of food allergies can vary significantly between cultures, influenced by dietary practices, cultural norms, and the prevalence of specific allergenic foods.34,45 For instance, Jung et al. studied 190 Korean families and observed reduced quality of life among parents of children allergic to soy or cow’s milk, emphasizing the central role of soy in Asian diets.34 Similarly, Warren et al. indicated that avoidance of commonly consumed foods such as cow’s milk and eggs poses greater daily challenges for families in Western societies, further decreasing parental quality of life.10
Our study has several limitations, including its single-center design and relatively small sample size, which may limit the generalizability of the findings. Additionally, only mothers were included, based on previous research suggesting that mothers tend to experience greater psychosocial impacts.26 Despite these limitations, the use of multiple validated scales adapted for the Turkish population enhances the robustness and reliability of our results.
Conclusion
In conclusion, our study demonstrates that mothers of children with food allergies experience significantly higher anxiety levels, greater caregiver burden, and diminished quality of life. Specifically, mothers of children with CMPA exhibited particularly elevated anxiety levels, further exacerbating their quality-of-life impairment. These findings highlight the importance of addressing the psychiatric support needs of mothers managing childhood food allergies, alongside enhancing societal awareness of the challenges associated with food allergies. Comprehensive interventions encompassing medical, social, and psychological support, as well as structured educational programs and supportive community-based activities, are recommended to substantially improve the overall quality of life for these caregivers.
Ethics Approval and Consent to Participate
The study was approved by the Dr. Lütfi Kırdar City Hospital Ethics Committee, Approval number 2023/514/250/29, dated May 29, 2023, and informed consent has been obtained from all participants.
Consent for Publication
Participants were enrolled with informed consent, and the study was conducted per the Declaration of Helsinki.
Availability of Data and Materials
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Competing Interests
The authors declare no competing interests.
Clinical Trial Number
Clinical trial number: not applicable.
Authors’ Contributions
All authors contributed equally to this article.
Conflicts of Interest
The authors declare no potential conflicts of interest to research, authorship and/or publication of this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
1 Prescott S, Allen KJ. Food allergy: Riding the second wave of the allergy epidemic. Pediatr Allergy Immunol. 2011;22(2):155–60. 10.1111/j.1399-3038.2011.01145.x
2 Sicherer SH, Sampson HA. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J Allergy Clin Immunol. 2018;141(1):41–58. 10.1016/j.jaci.2017.11.003
3 Spolidoro GCI, Amera YT, Ali MM, Nyassi S, Lisik D, Ioannidou A, et al. Frequency of food allergy in Europe: An updated systematic review and meta-analysis. Allergy. 2023;78(2):351–68. 10.1111/all.15560
4 Sampath V, Abrams EM, Adlou B, Akdis C, Akdis M, Brough HA, et al. Food allergy across the globe. J Allergy Clin Immunol. 2021;148(6):1347–64. 10.1016/j.jaci.2021.10.018
5 Allen CW, Bidarkar MS, vanNunen SA, Campbell DE. Factors impacting parental burden in food-allergic children. J Paediatr Child Health. 2015;51(7):696–8. 10.1111/jpc.12794
6 Umasunthar T, Leonardi-Bee J, Hodes M, Turner PJ, Gore C, Habibi P, et al. Incidence of fatal food anaphylaxis in people with food allergy: A systematic review and meta-analysis. Clin Exp Allergy. 2013;43(12):1333–41. 10.1111/cea.12211
7 Turner PJ, Arasi S, Ballmer-Weber B, Conrado AB, Deschildre A, Gerdts J, et al. Risk factors for severe reactions in food allergy: Rapid evidence review with meta-analysis. Allergy. 2022;77(9):2634–52. 10.1111/all.15318
8 Kılıç N, Kaya Ş, Taşçı G, Özsoy F, Kılıç M. Quality of life in children with food allergies, psychiatric symptoms, and caregiving burden of their mothers. Allergol Immunopathol (Madr). 2023;51(5):48–56. 10.15586/aei.v51i5.860
9 Cummings AJ, Knibb RC, King RM, Lucas JS. The psychosocial impact of food allergy and food hypersensitivity in children, adolescents and their families: A review. Allergy. 2010;65(8):933–45. 10.1111/j.1398-9995.2010.02342.x
10 Warren CM, Gupta RS, Sohn MW, Oh EH, Lal N, Garfield CF, et al. Differences in empowerment and quality of life among parents of children with food allergy. Ann Allergy Asthma Immunol. 2015;114(2):117–25. 10.1016/j.anai.2014.10.025
11 Protudjer JLP, Golding M, Salisbury MR, Abrams EM, Roos LE. High anxiety and health-related quality of life in families with children with food allergy during coronavirus disease 2019. Ann Allergy Asthma Immunol. 2021;126(1):83–88.e1. 10.1016/j.anai.2020.09.010
12 Yücel E, Yılmazbaş NP, Erbilgin S, Terzi Ö, Özçeker D. Evaluation of anxiety and caregiver burden in the mothers of 0–2-year-old children with food allergy. Nam Kem Med J. 2022;10(1):8–14. 0.4274/nkmj.galenos.2021.63935
13 Herbert LJ, Dahlquist LM. Perceived history of anaphylaxis and parental overprotection, autonomy, anxiety, and depression in food allergic young adults. J Clin Psychol Med Settings. 2008;15(4):261–9. 10.1007/s10880-008-9130-y
14 Lao-araya M, Trakultivakorn M. Prevalence of food allergy among preschool children in northern Thailand. Pediatr Int. 2012;54(2):238–43. 10.1111/j.1442-200X.2011.03544.x
15 Muraro A, Werfel T, Hoffmann-Sommergruber K, Roberts G, Beyer K, Bindslev-Jensen C, et al. EAACI food allergy and anaphylaxis guidelines: Diagnosis and management of food allergy. Allergy. 2014;69(8):1008–25. 10.1111/all.12429
16 Spielberger CD, Gorsuch RL, Lushene RE. Manual for State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press; 1970
17 Öner NP. State and trait anxiety in Turkish patients and normals. Ser Clin C Psychology: Stress & Anxiety. 1983;2:107–19.
18 Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: Correlates of feelings of burden. Gerontologist. 1980;20(6):649–55. 10.1093/geront/20.6.649
19 Ozlu A, Yıldız M, Aker T. A reliability and validity study on the Zarit caregiver burden scale. Arch Neuropsychiatr. 2009;46:38–42.
20 Schmidt S, Mühlan H, Power M. The EUROHIS-QOL 8-item index: Psychometric results of a cross-cultural field study. Eur J Public Health. 2006;16(4):420–8. 10.1093/eurpub/cki155
21 Eser E, Lağarlı T, Baydur H, Akkurt V, Akkuş H, Arslan E, et al. EUROHIS (WHOQOL-8.Tr) Türkçe sürümünün Türk toplumundaki psikometrik özellikleri. Turk J Public Health. 2010;8(3):136–52.
22 Lau GY, Patel N, Umasunthar T, Gore C, Warner JO, Hanna H, et al. Anxiety and stress in mothers of food-allergic children. Pediatr Allergy Immunol. 2014;25(3):236–42. 10.1111/pai.12233
23 Roberts K, Meiser-Stedman R, Brightwell A, Young J. Parental anxiety and posttraumatic stress symptoms in pediatric food allergy. J Pediatr Psychol. 2021;46(6):688–97. 10.1093/jpepsy/jsab012
24 Kan A, Ture M, Yilmaz K, Emre E, Baş G. Maternal anxiety, stress, and depression: The role of food allergy. Asthma Allergy Immunol.2022;20:1–6. 10.21911/aai.675
25 Ostblom E, Egmar AC, Gardulf A, Lilja G, Wickman M. The impact of food hypersensitivity reported in 9-year-old children by their parents on health-related quality of life. Allergy. 2008;63(2):211–8. 10.1111/j.1398-9995.2007.01559.x
26 King RM, Knibb RC, Hourihane JO. Impact of peanut allergy on quality of life, stress and anxiety in the family. Allergy. 2009;64(3):461–8. 10.1111/j.1398-9995.2008.01843.x
27 Zijlstra WT, Flinterman AE, Soeters L, Knulst AC, Sinnema G, L’Hoir MP, et al. Parental anxiety before and after food challenges in children with suspected peanut and hazelnut allergy. Pediatr Allergy Immunol. 2010;21(2 Pt 2):e439–e445. 10.1111/j.1399-3038.2009.00929.x
28 Beken B, Celik V, Gokmirza Ozdemir P, Sut N, Gorker I, Yazıcıoğlu M. Maternal anxiety and internet-based food elimination in suspected food allergy. Pediatr Allergy Immunol. 2019;30(7):752–9. 10.1111/pai.13100
29 Goodwin RD, Rodgin S, Goldman R, Rodriguez J, deVos G, Serebrisky D, et al. Food allergy and anxiety and depression among ethnic minority children and their caregivers. J Pediatr. 2017;187:258–264.e1. 10.1016/j.jpeds.2017.04.055
30 Soller L, To S, Hsu E, Chan ES. Current tools measuring anxiety in parents of food-allergic children are inadequate. Pediatr Allergy Immunol. 2020;31(6):678–85. 10.1111/pai.13260
31 Charana A, Tripsianis G, Matziou V, Vaos G, Iatrou C, Chloropoulou P. Preoperative anxiety in Greek children and their parents when presenting for routine surgery. Anesthesiol Res Pract. 2018;2018:5135203. 10.1155/2018/5135203
32 Hoehn JL, Dahlquist LM, Hahn AL, Bollinger ME. Parents of children with food allergy: Gender differences in perceived impact and perceived food allergy severity. J Pediatr Psychol. 2017;42(2):186–97. 10.1093/jpepsy/jsw059
33 Birdi G, Cooke R, Knibb R. Quality of life, stress, and mental health in parents of children with parentally diagnosed food allergy compared to medically diagnosed and healthy controls. J Allergy (Cairo). 2016;2016:1497375. 10.1155/2016/1497375
34 Jung M, Kang U, Kim S, Yoo HW, Kim HY, Kim M, et al. Psychological distress and perceived burden in parents of Korean children with IgE-mediated food allergy. J Korean Med Sci. 2023;38(27):e208. 10.3346/jkms.2023.38.e208
35 Howe L, Franxman T, Teich E, Greenhawt M. What affects quality of life among caregivers of food-allergic children? Ann Allergy Asthma Immunol. 2014;113(1):69–74.e2. 10.1016/j.anai.2014.04.016
36 Gillespie CA, Woodgate RL, Chalmers KI, Watson WTA. “Living with risk”: Mothering a child with food-induced anaphylaxis. J Pediatr Nurs. 2007;22(1):30–42. 10.1016/j.pedn.2006.05.007
37 Faden SY, Merdad N, Faden YA. Parents of children with neurodevelopmental disorders: A mixed methods approach to understanding quality of life, stress, and perceived social support. Cureus. 2023;15(4):e37356. 10.7759/cureus.37356
38 Brown SC, Whelan K, Frampton C, Wall CL, Gearry RB, Day AS. Food-related quality of life in children and adolescents with Crohn’s disease. Inflamm Bowel Dis. 2022;28(12):1838–43. 10.1093/ibd/izac010
39 Ražnatović Ðurović M, Janković J, Ćirković A, Timotijević ZS, Rašić J, Vitković L, et al. Impact of atopic dermatitis on the quality of life of children and their families. Ital J Dermatol Venerol. 2021;156(1):29–35. 10.23736/S2784-8671.19.06447-2
40 Westwell-Roper C, To S, Andjelic G, Lu C, Lin B, Soller L, et al. Food-allergy-specific anxiety and distress in parents of children with food allergy: A systematic review. Pediatr Allergy Immunol. 2022;33(1):e13695. 10.1111/pai.13695
41 Knibb RC, Jones CJ, Herbert LJ, Screti C. Psychological support needs for children with food allergy and their families: A systematic review. Pediatr Allergy Immunol. 2024;35(3):e14108. 10.1111/pai.14108
42 Lagercrantz B, Persson Å, Kull I. “Healthcare seems to vary a lot”: A focus group study among parents of children with severe allergy. J Asthma. 2017;54(7):672–8. 10.1080/02770903.2016.1258079
43 Mandell D, Curtis R, Gold M, Hardie S. Anaphylaxis: How do you live with it? Health Soc Work. 2005;30(4):325–35. 10.1093/hsw/30.4.325
44 Abrams EM, Kim H, Gerdts J, Protudjer JLP. Milk allergy most burdensome in multi-food allergic children. Pediatr Allergy Immunol. 2020;31(7):827–34. 10.1111/pai.13274
45 Arik Yilmaz E, Cavkaytar O, Buyuktiryaki B, Soyer O, Sahiner UM, Sekerel BE, et al. Factors affecting food allergy-related quality of life from parents’ perception in Turkish children. Allergy Asthma Immunol Res. 2018;10(4):379–86. 10.4168/aair.2018.10.4.379