
Download
ORIGINAL ARTICLE
Gender and age differences in the risk of allergic reactions following the Pfizer-BioNTech COVID-19 and AstraZeneca vaccine using skin prick test and intradermal test among patients with high risk for hypersensitivity
Leonora Svarçaa, Sonja Bojadzievab, Premtim Rashitic*, Albiona Rashiti-Bytyçid,e, Diar Kabashic
aDepartment of Allergology and Clinical Immunology, University Clinical Center of Kosovo, Prishtina, Republic of Kosovo
bDepartment of Gastroentero Hepathology, University Pediatric Clinic, Faculty of Medicine, Ss. Cyril and Methodius University, Skopje, Republic of North Macedonia
cFaculty of Medicine, University of Prishtina, University Clinical Center of Kosovo, Prishtina, Republic of Kosovo
dNational Institute of Public Health, Prishtina, Republic of Kosovo
eAlma Mater Europaea Campus College Rezonanca, Pejton, Prishtine, Kosovo
Abstract
Objective: The aim of this study was to assess the association between allergic reactions after COVID-19 vaccination and the history of high-risk allergy, individual predisposing factors such as age and gender, and COVID-19 vaccine type.
Materials and methods: This retrospective cohort study included 234 adult patients (18 years old and above) who underwent a COVID-19 vaccine allergy test up until February 2023 in a Clinic of Allergy and Clinical Immunology in the University Clinical Center of Kosovo. All patients suspected of allergy underwent skin testing: SPT (skin prick test) and IDT (intradermal test) using either an mRNA (ribonucleic messenger acid) vaccine (BNT162b2, Pfizer-BioNTech) and/or an adenoviral vector vaccine (AZD1222, AstraZeneca). Subsequent immunization was administered under careful medical observation.
Results: Among the 234 patients with a high-risk allergy profile, several potential risk factors were identified, including a history of multiple allergies, previous anaphylaxis, and/or drug allergies. In our cohort, food allergies were reported by 20 patients (8.5%) and multiple drug allergies were reported by 118 patients (50.4%). Due to the retrospective nature of the study, we cannot establish causality. Therefore, older age and receipt of the Pfizer-BioNTech vaccine were found to be associated with increased allergic reactions after COVID-19 vaccination, while male gender was associated with decreased risk. Although previous allergic manifestations were common among those with reactions, they were not significantly associated with increased risk after adjustment for confounders. The absence of a control group consisting of vaccinated individuals without a high-risk allergy history limits the generalizability of our findings.
Conclusions: Immediate allergic reactions to COVID-19 vaccines are rare but can be severe and reoccur. Findings suggest that gender and age-specific factors may influence the response to the vaccine. Nevertheless, COVID-19 vaccines remain a critical tool in preventing severe disease and controlling the ongoing pandemic.
Key words: age, gender, COVID-19 vaccine, SPT, IDT
*Corresponding author: Premtim Rashiti, Faculty of Medicine, University of Prishtina, University Clinical Center of Kosovo, Prishtina, Republic of Kosovo. Email address: [email protected]
Received 27 March 2025; Accepted 11 June 2025; Available online 1 September 2025
Copyright: Svarça L, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
The onset of the COVID-19 pandemic has led to widespread health, economic, and societal impacts globally. According to the WHO (World Health Organization), COVID-19, the cause of the coronavirus pandemic, is caused by various mutated strains of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2).1 This novel virus first appeared in December 2019 in China and later spread worldwide. Globally, there are over 777 million confirmed cases of COVID-19, including over 7.1 million deaths.2 According to official statistics, from the start of the pandemic Kosovo has registered approximately 274,000 COVID-19 cases and 3200 deaths.
Despite numerous protective measures, the profound impacts of COVID-19 continue to affect human lives, economic stability, and various other societal aspects. To date, vaccination remains the main tool to prevent morbidity and mortality and to control the pandemic by reducing transmission and protecting human lives. Vaccine development progresses through multiple stages, starting with animal-based preclinical tests to evaluate safety and efficacy. It then moves to human clinical trials,3,4 initially involving a limited number of volunteers and progressively expanding to include more participants to enhance the reliability of safety and efficacy data.3 COVID-19 vaccines were introduced on July 22, 2020, and to date, more than 13.64 billion doses have been administered globally. This indicates that approximately 67% of the global population has completed the primary vaccination series of the COVID-19 vaccine while 32% has received at least one booster.2 In Kosovo, as of May 21, 2022, approximately 46% of the total population had received a complete primary series of the COVID-19 vaccine.2 The Pfizer/BioNTech and Astra Zeneca vaccines became one of the leading tools in the battle against the pandemic.4 Both types of vaccines have been associated with COVID-19 vaccine reactions and adverse events, including some local reactions such as redness, swelling, and pain at the injection site and some systemic reactions such as fever, fatigue, headache, chills, vomiting, diarrhea, and new or worsening muscle/joint pain.5 Additionally, while uncommon, COVID-19 vaccines can cause severe side effects such as anaphylaxis, blood clots, myocarditis, pericarditis, along with auditory changes like hearing loss and tinnitus; however, the incidence of anaphylaxis remains low, affecting only a small fraction of vaccinated individuals.6
Hence, ensuring the safety of COVID-19 vaccines is crucial, prioritizing the outweighing of benefits over risks. Through diligent monitoring and management of rare adverse events, healthcare professionals maintain the vaccines’ efficacy and safety, safeguarding both individuals and public. However, severe or rare adverse events may not be identified in phase 3 trials due to limited sample size, inclusion criteria, and participants’ characteristics, which may differ from the population receiving the immunization.7 Throughout clinical trials, individuals who previously had allergic reactions to vaccine components or other vaccines were not included. Similarly, those with allergies experienced typical skin reactions post-vaccination, including reactions at the injection site, urticaria, morbilliform, and erythromelalgia reactions as well as herpes zoster, chilblains, and sensations of burning feet. Additionally, although rare, some recipients have shown severe allergic reactions like anaphylaxis,8 leading to more severe symptoms, including respiratory difficulties, facial and throat swelling, and lowered blood pressure.9 In these cases, immediate medical attention is necessary to prevent further complications. Raising awareness about the potential risks and symptoms of severe allergic reactions to COVID-19 vaccines is crucial. Prompt identification and appropriate management of these reactions are key to reducing complications and enhancing the safety of vaccine recipients. Notably, more than 90% of anaphylactic cases following vaccination have occurred in females, with 81% having reported previous allergies. Furthermore, our study did not include specific testing for polyethylene glycol (PEG), which is suggested as a potential allergen in COVID-19 vaccines. This is a limitation, as we cannot confirm whether observed allergic reactions were indeed PEG-related. Due to growing concerns over vaccine-induced allergic reactions, both medical professionals and researchers have been compelled to issue updated safety guidelines for administering these vaccines to individuals with known allergies. Despite these recommendations, uncertainty remains, and healthcare providers should educate their patients about potential allergic reactions and ensure seeking immediate medical attention if symptoms arise.10
In the Republic of Kosovo, vaccination against COVID-19 began on March 2021 based on the State Plan for vaccination against COVID-19, drawn up by the Committee for immunization against COVID-19 within the Ministry of Health. As in other countries in the region, vaccine supply was initially limited; therefore, vaccination was prioritized for high-risk populations, including health workers, residents in nursing homes and all social workers, and people aged over 80 years as well as people with chronic diseases (people on dialysis, with diabetes, cardiovascular disease).11 The second phase included the following prioritization: people aged 65–79 years, other persons with chronic diseases, and teachers and security forces involved in the management of COVID-19. The third phase included vaccination of approximately 50% of the general population, including in the age group of 40–64 years, the remaining population with significant health conditions, and public sector workers.12
The aim of this study was to assess the association between the history of high-risk allergy and the risk of allergic reactions after COVID-19 vaccination. The findings of this study could support the national strategic readiness and response plan of the Republic of Kosovo. Finally, this study aimed to predict the post-vaccination side effects based on individual predisposing factors such as age, gender, and COVID-19 vaccine type.
Materials and Methods
This retrospective cohort study included 234 adult patients (aged 18 years and above) who underwent COVID-19 vaccine allergy testing up to February 2023 at the Clinic of Allergy and Clinical Immunology, University Clinical Center of Kosovo. The vaccine allergy tests were done by trained allergologists. The recruitment of patients was done through referral from other health facilities. All relevant health facilities were informed to refer patients with a history of COVID-19 vaccine allergy or those considered high-risk for allergic reactions. The participants were divided into two groups: patients with a history of hypersensitivity to the first COVID-19 vaccine dose and patients with a high risk of allergic reaction, including atopic, allergy, or anaphylaxis history. Those with a prior diagnosis of uncontrolled asthma, acute urticaria, or angioedema were excluded if they were receiving antihistamines or corticosteroids or had mastocytosis.
This study collected anamnesis data of the patients who fulfilled the inclusion criteria. Furthermore, all patients suspected of allergy underwent skin testing: SPT (skin prick test) and IDT (intradermal test) with COVID-19 vaccine (mRNA [ribonucleic messenger acid] and adenovector viral vaccines). The standardized workup consisted of skin tests with two anti-SARS-CoV-mRNA vaccine and adeno viral vector vaccine. SPTs with histamine and NaCl (sodium chloride) 0.9% were used as positive and negative controls. If skin tests were negative, SPT (1:1) and IDR at dilutions of 1:100 and 1:10 were performed after 48 hours. If skin tests returned positive, a complementary workup was done, including mRNA and adenoviral vector vaccine (SPT 1:1, IDR 1:100 and 1:10). IDR with NaCl 0.9% was used as a negative control. Skin tests were performed on the anterior face of the forearm. SPT was performed with allergy lancets (Staller point, STALLERGENES GmbH, Kamp-Lintfort, Germany) and IDR was performed with tuberculin syringes for the vaccines (1 mL syringes with 25G or 27G needles). The volume injected for IDR was adjusted to reach an initial wheal of 3–5 mm. The skin test was considered positive in the case of a papule of 3 mm or more in comparison to the steady-state with erythema at 20 minutes. The test was considered inconclusive if a papule measuring less than 3 mm was observed or if there was no erythema in the negative control test (NaCl 0.9%). It is important to acknowledge that the SPT and IDT are not fully validated for COVID-19 vaccines. The sensitivity and specificity of these methods for detecting vaccine allergies remain under investigation. Data were collected using a survey questionnaire administered to the health professionals that included a part with demographic data and data on the patient; allergies (air, food, drug allergy, vaccines, and ingredients of vaccine); and data on clinic manifestation (local, systemic, anaphylaxis) and comorbidities.
This study was performed in accordance with the Declaration of Helsinki and with the approval of the University Clinical Center of Kosovo institutional review board.
Statistical analysis
Statistical analysis was performed using SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA). Frequencies and percentages were measured for categorical data and quantitative variables were analyzed using measures of central tendency (mean, median, minimum, and maximum values) and measures of dispersion (standard deviation). Pearson’s chi-squared test (χ2) or Fisher’s exact test was used to assess associations between categorical variables. Risk factors were quantified using relative risks (RRs) and 95% confidence intervals (CIs). A two-sided analysis with a significance level of p < 0.05 was used to determine statistical significance.
Results
Patient characteristics
During the study period, 234 patients with a history of allergic reactions were evaluated at the Clinic of Allergy and Clinical Immunology, University Clinical Center of Kosovo. Most patients were female (69.66%), with a mean age of 43.07 ± 15.5 years. A strong majority had a medical history of prior allergies (99.57%) while 73.50% had some kind of allergic manifestation. Specifically, local allergic manifestations were observed in 35.89% of patients (Table 1).
Table 1 Demographic characteristics and allergy history.
| Characteristics | Participants n (%) (N = 234) |
|---|---|
| Age | 43.07 ±15.5 |
| Sex: female | 163 (69.66%) |
| Prior allergic reaction, total | 233 (99.57%) |
| Air | 34 (14.53%) |
| Food | 20 (8.55%) |
| Medicines | 118 (50.43%) |
| Hymenoptera | 23 (9.83%) |
| Previous vaccines | 22 (9.82% |
| Ingredients in vaccine | 4 (1.71%) |
| Other allergies | 22 (9.40%) |
| Allergic manifestations, total | 172 (73.50%) |
| Local | 84 (35.89%) |
| Systemic | 61 (26.06%) |
| Anaphylaxis | 27 (11.58%) |
| Associated diseases of the patient | |
| Cardiovascular | 51 (21.78%) |
| Hypertension | 30 (12.82%) |
| Hypotension | 1 (0.48%) |
| Other CVD | 20 (8.55%) |
| Diabetes | 8 (3.42%) |
The main reasons for referral included concern for potential allergy (n = 233), a suspected allergic reaction to a non-COVID-19 vaccine (n = 22), and a suspected allergic reaction to the first dose of a COVID-19 vaccine. Patients testing negative were recommended to receive a vaccine based on established guideline criteria.
Association of demographic characteristics and risk of allergic reaction
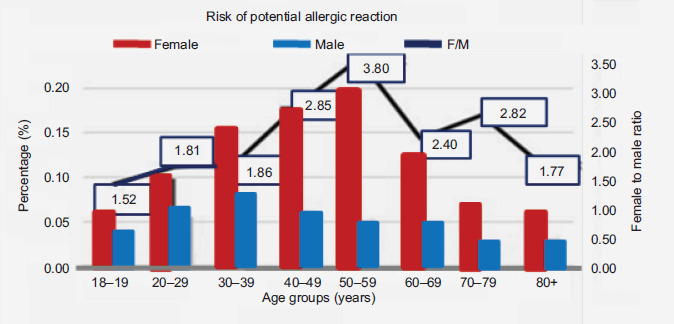
An analysis of patient medical histories before the initial vaccination with any of the COVID-19 vaccines included in this study indicated that females across all age groups exhibited a higher likelihood of experiencing allergic events. Notably, the RRs for adverse allergic reactions in females compared to males escalated from 1.52 in the youngest demographic to 3.80 among those aged 50–59 years, before decreasing to 1.77 in individuals aged 80–89 years. Despite these variations, the most significant disparities in RRs were predominantly seen in the age bracket of 30–69 years.
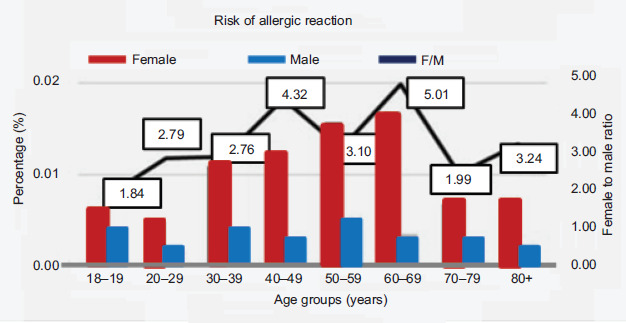
The female-to-male RRs for adverse events were higher following administration of the first vaccine dose (Figures 1 and 2). For instance, in terms of adverse events, the most pronounced gender disparity was observed in the 50–59-year age group, where the female-to-male RR peaked at 5.01. In the context of allergic reactions specifically, the RR for females versus males was highest at 4.32 in the 40–49-year age bracket and dropped to 1.84 among those aged 18–19 years. Overall, the influence of age was marked, with the lowest gender-specific RRs occurring at the youngest and oldest ends of the age spectrum.
Figure 1 Female-to-male ratio of the percentage reporting potential risk of allergic reaction prior to administrating the first dose of the COVID-19 vaccine.
Figure 2 Female-to-male ratio of the percentage reporting adverse events after the first dose of the COVID-19 vaccine.
High-risk allergy history was associated with an increased risk of allergic reactions (RR = 2.48; 95% CI: 1.95–3.28). Adjustment of other potential confounders did not change the association significantly (aRR = 2.87; 95% CI: 1.98–3.06). In the adjusted analyses, the presence of reported history of high-risk allergy was associated with an increased risk of diagnosed allergic reaction in the study after the administration of the Astra Zeneca Covid-19 vaccine (aRR = 3.93; 95% CI: 2.45–6.78) and Pfizer-BioNTech (aRR = 4.36; 95% CI: 2.63–7.58), although risks were consistently higher after the Pfizer-BioNTech vaccine.
Further analyses indicated that older age (RR = 1.00; 95% CI: 0.98–1.00), a history of previous allergic reactions, and receipt of the Pfizer-BioNTech vaccine (compared to AstraZeneca) (RR = 1.49; 95% CI: 1.37–1.70) were associated with an increased risk of allergic reactions after COVID-19 vaccination, while being male versus female was associated with a decreased risk of allergic reactions after (RR = 0.69; 95% CI: 0.61–0.73) (Table 2).
Table 2 Predictors of allergic risk following administration of the first dose of COVID-19 vaccine.
| Parameters | Unadjusted RR (95% CI) | p value | Adjusted RR (95% CI) | p value |
|---|---|---|---|---|
| Sex (male vs. female) | 0.69 (0.61,0.73) | <0.001 | 0.69 (0.61,0.73) | <0.001 |
| Age (years) | 1.00 (0.98,1.00) | 0.021 | 1.00 (0.98,1.00) | 0.01 |
| Astra versus Pfizer-BioNTech | 1.49 (1.38,1.70) | <0.001 | 1.49 (1.37,1.70) | <0.001 |
| Previous allergic reactions | 0.77 (0.71, 0.83) | <0.001 | 0.99 (0.87, 1.12) | 0.834 |
Discussion
Safety concerns—particularly those related to severe allergic reactions—represent a significant barrier to the implementation of large-scale vaccination programs. To date, the safety data from clinical trials of the COVID-19 vaccine have largely lacked gender-specific analysis; instead, adverse events have been broadly compared between those receiving the vaccine and those in the placebo group. To our knowledge, this is one of the rare studies to report on demographic differences in the allergic risk associated with COVID-19 vaccine for highly allergic patients.
In our cohort, 234 patients defined as being at high risk for an allergic reaction were referred to receive immunization under medical observation. In this group, the mean age was 43 years and comprised 69.6% women. The absence of a control group of vaccinated individuals without a high-risk allergy history limits the generalizability of our findings.
The outcomes of this research align with established patterns observed in allergic diseases, where incidences are notably higher in females compared to males, particularly with respect to drug allergies.13,14 Within the group of highly sensitive adults studied, several risk factors were identified, including a history of multiple allergies and anaphylactic incidents as well as drug sensitivities. Specifically, in our sample, food allergies were noted in 20 participants (8.5%), while a significant 118 individuals (50.4%) reported multiple drug allergies. This contrasts sharply with the broader adult population where food allergies affect less than 5%, and severe or multiple drug allergies are even rarer, affecting less than 1%.15,16 Moreover, further analyses indicated that older age and receipt of Pfizer-BioNTech vaccine were associated with an increased risk of allergic reactions after COVID-19 vaccination, while being male versus female was associated with decreased risk.
Published research following the global rollout of the COVID-19 vaccination program has documented a higher incidence of adverse events among females.17,18 For instance, an analysis within the European Economic Area of 30 thromboembolic incidents post-vaccination with the AstraZeneca ChAdOx1-S vaccine revealed that 63% occurred in women. The types of thrombotic events identified included deep vein thrombosis, hepatic vein thrombosis, mesenteric vein thrombosis, portal vein thrombosis, and carotid artery thrombosis.19 As mentioned earlier, an exception in gender associated risk of allergic reactions is myocarditis following vaccination with the mRNA vaccines, which occurs predominantly in young males at rates of about 1 out of every 6 occurrences within a set of 10,000.20 However, this study was not designed to capture data on other rare adverse events, such as myocarditis. Furthermore, in the surveillance system for adverse effects following immunization in Australia, females accounted for 55% of reports overall and 80% of adults.21 A subsequent study assessing fever and rash post-MMR (measles, mumps, and rubella) vaccination in infants indicated that female infants displayed a higher likelihood of allergic reactions even when adjusting for underlying health conditions.19 Furthermore, a gender-focused analysis of adverse events following immunization in Canada (2012–2015) showed a female-to-male reporting rate ratio (RRR) of 1.9, with the highest RR (6.3) observed among adults aged 18–64 years. Additionally, this study highlighted that the most severe gender-specific RRs involved conditions such as oculorespiratory syndrome, anesthesia-related paresthesia, and anaphylaxis.22 Likewise, a study in Spain confirmed the findings with more reports in females registered in the computerized reporting registry of adverse events.23 Systematic review of seasonal influenza vaccine data that analyzed immunogenicity, efficacy, effectiveness, and safety showed that after stratification by sex, the higher rates of adverse events were that of following immunization in females.24
According to a CDC (Centers for Disease Control and Prevention) report, 49% of the reported severe allergic reactions were ultimately classified as non-anaphylactic allergic responses, indicating that the true incidence of post-vaccination allergic reactions may therefore be lower than that reported in this study.25 Given the scale of the worldwide mass vaccination efforts and the volume of citizens who were vaccinated in a short time frame, a complete review of all reported allergy symptoms is still not feasible. Further prospective research is essential to better understand the risk factors associated with verified allergic reactions following COVID-19 vaccination. Additionally, self-reported symptoms of allergies can offer vital insights for researchers and medical experts. Recent publications in this field have shown that most individuals, even those who experienced immediate and potential allergic responses after the initial vaccine dose, were able to safely receive a second dose.26 This study also noted that only a small number of participants failed to complete their vaccination schedule, suggesting that reactions to the first dose might not necessarily be allergic in nature or could be triggered by non-IgE (immunoglobulin E) mediated mechanisms.27
Conclusion
In conclusion, the consistently higher rates of adverse events observed among females across all age groups following COVID-19 vaccination highlight the potential influence of gender-specific factors on vaccine response. Given these observations, further research is needed before any vaccine dosage adjustments based on gender could be recommended. Present findings indicate the need for cautious interpretation. Nevertheless, this vaccine plays a crucial role in preventing a deadly disease and remains a key instrument in managing the COVID-19 pandemic. Thus, immunizing the general population—while addressing safety and allergy-related concerns among individuals with a history of allergic reactions—remains a critical public health objective.
Author Contributions
All authors contributed equally to this article.
Conflicts of Interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
None.
REFERENCES
1 WHO. WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. 2023 [cited 2023 Apr 29]. Available from: https://covid19.who.int/
2 WHO. COVID-19 vaccination, World data [Internet]. 2024. Available from: https://data.who.int/dashboards/covid19/vaccines?n=o
3 Deb B, Shah H, Goel S. Current global vaccine and drug efforts against COVID-19: Pros and cons of bypassing animal trials. J Biosci. 2020;45(1):82. 10.1007/s12038-020-00053-2
4 Shavit R, Maoz-Segal R, Iancovici-Kidon M, Offengenden I, Haj Yahia S, Machnes Maayan D, et al. Prevalence of allergic reactions after Pfizer-BioNTech COVID-19 vaccination among adults with high allergy risk. JAMA Netw Open. 2021;4(8):e2122255. 10.1001/jamanetworkopen.2021.22255
5 McNeil MM, DeStefano F. Vaccine-associated hypersensitivity. J Allergy Clin Immunol. 2018;141(2):463–72. 10.1016/j.jaci.2017.12.971
6 Thanh Le T, Andreadakis Z, Kumar A, Gómez Román R, Tollefsen S, Saville M, et al. The COVID-19 vaccine development landscape. Nat Rev Drug Discov. 2020;19(5):305–6. 10.1038/d41573-020-00073-5
7 Yaamika H, Muralidas D, Elumalai K. Review of adverse events associated with COVID-19 vaccines, highlighting their frequencies and reported cases. J Taibah Univ Med Sci. 2023;18(6):1646–61. 10.1016/j.jtumed.2023.08.004
8 Li YE, Wang S, Reiter RJ, Ren J. Clinical cardiovascular emergencies and the cellular basis of COVID-19 vaccination: From dream to reality? Int J Infect Dis. 2022;124:1–10. 10.1016/j.ijid.2022.08.026
9 Rosenblatt AE, Stein SL. Cutaneous reactions to vaccinations. Clin Dermatol. 2015;33(3):327–32. 10.1016/j.clindermatol.2014.12.009
10 Fiorillo G, Pancetti S, Cortese A, Toso F, Manara S, Costanzo A, et al. Leukocytoclastic vasculitis (cutaneous small-vessel vasculitis) after COVID-19 vaccination. J Autoimmun. 2022;127:102783. 10.1016/j.jaut.2021.102783
11 Watson OJ, Barnsley G, Toor J, Hogan AB, Winskill P, Ghani AC. Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect Dis. 2022;22(9):1293–302. 10.1016/S1473-3099(22)00320-6
12 Rashiti-Bytyçi A, White Johansson E, Kaçaniku-Gunga P, Danis K, Schoeps A, Dörre A, et al. Estimation of COVID-19 vaccine effectiveness against infections and severe outcomes using routine surveillance data in Kosovo, July–September 2021. Jakupi A, editor. PLoS One. 2024;19(7):e0305629. 10.1371/journal.pone.0305629
13 Chen W, Mempel M, Schober W, Behrendt H, Ring J. Gender difference, sex hormones, and immediate type hypersensitivity reactions. Allergy. 2008;63(11):1418–27. 10.1111/j.1398-9995.2008.01880.x
14 Leynaert B, Sunyer J, Garcia-Esteban R, Svanes C, Jarvis D, Cerveri I, et al. Gender differences in prevalence, diagnosis and incidence of allergic and non-allergic asthma: A population-based cohort. Thorax. 2012;67(7):625–31. 10.1136/thoraxjnl-2011-201249
15 Gupta RS, Warren CM, Smith BM, Jiang J, Blumenstock JA, Davis MM, et al. Prevalence and severity of food allergies among US adults. JAMA Netw Open. 20194;2(1):e185630. 10.1001/jamanetworkopen.2018.5630
16 Dhopeshwarkar N, Sheikh A, Doan R, Topaz M, Bates DW, Blumenthal KG, et al. Drug-induced anaphylaxis documented in electronic health records. J Allergy Clin Immunol Pract. 2019;7(1):103–11. 10.1016/j.jaip.2018.06.010
17 Blumenthal KG, Robinson LB, Camargo CA, Shenoy ES, Banerji A, Landman AB, et al. Acute allergic reactions to mRNA COVID-19 vaccines. JAMA. 2021;325(15):1562–5. 10.1001/jama.2021.3976
18 Esposito D, Titievsky L, Beachler DC, Hawes JCL, Isturiz R, Scott DA, et al. Incidence of outcomes relevant to vaccine safety monitoring in a US commercially-insured population. Vaccine. 201818;36(52):8084–93. 10.1016/j.vaccine.2018.10.052
19 Green MS, Peer V, Magid A, Hagani N, Anis E, Nitzan D. Gender differences in adverse events following the Pfizer-BioNTech COVID-19 vaccine. Vaccines. 2022;10(2):233. 10.3390/vaccines10020233
20 Bozkurt B, Kamat I, Hotez PJ. Myocarditis with COVID-19 mRNA vaccines. Circulation. 2021;144(6):471–84. 10.1161/CIRCULATIONAHA.121.056135
21 Clothier HJ, Lawrie J, Lewis G, Russell M, Crawford NW, Buttery JP. SAEFVIC: Surveillance of adverse events following immunisation (AEFI) in Victoria, Australia, 2018. Commun Dis Intell. 2020;15:44. 10.33321/cdi.2020.44.46
22 Harris T, Nair J, Fediurek J, Deeks SL. Assessment of sex-specific differences in adverse events following immunization reporting in Ontario, 2012–15. Vaccine. 2017;35(19):2600–4. 10.1016/j.vaccine.2017.03.035
23 Alguacil-Ramos AM, Muelas-Tirado J, Garrigues-Pelufo TM, Portero-Alonso A, Diez-Domingo J, Pastor-Villalba E, et al. Surveillance for adverse events following immunization (AEFI) for 7 years using a computerised vaccination system. Public Health. 2016;135:66–74. 10.1016/j.puhe.2015.11.010
24 Tadount F, Doyon-Plourde P, Rafferty E, MacDonald S, Sadarangani M, Quach C. Is there a difference in the immune response, efficacy, effectiveness and safety of seasonal influenza vaccine in males and females?–A systematic review. Vaccine. 2020;38(3):444–59. 10.1016/j.vaccine.2019.10.091
25 Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine—United States, December 14–23, 2020. MMWR Morb Mortal Wkly Rep. 2021;70(2):46–51. 10.15585/mmwr.mm7002e1
26 Bunyavanich S, Rifas-Shiman SL, Platts-Mills TAE, Workman L, Sordillo JE, Gillman MW, et al. Peanut allergy prevalence among school-age children in a US cohort not selected for any disease. J Allergy Clin Immunol 2014 Sep;134(3):753–5. 10.1016/j.jaci.2014.05.050
27 Li L, Robinson LB, Patel R, Landman AB, Fu X, Shenoy ES, et al. Association of self-reported high-risk allergy history with allergy symptoms after COVID-19 vaccination. JAMA Netw Open. 2021;4(10):e2131034. 10.1001/jamanetworkopen.2021.31034