
Download
ORIGINAL ARTICLE
Effectiveness of a penicillin allergy delabeling program—real-world data from Croatia
Ivan Marković*, Jelena Barišić, Marina Božan Aksentijević, Ivica Lokner, Vesna Vukičević Lazarević
Special Hospital for Pulmonary Diseases, Zagreb, Croatia
Abstract
Penicillin allergy is the most commonly reported drug allergy, often leading to unnecessary avoidance of beta-lactam antibiotics, increased use of alternative broad-spectrum antibiotics, and higher healthcare costs. However, studies indicate that over 90% of penicillin allergy labels are erroneous. This study presents real-world data from a penicillin allergy delabeling program conducted at the Special Hospital for Pulmonary Diseases in Zagreb, Croatia. A total of 132 adult patients with a reported beta-lactam allergy were evaluated with a stepwise diagnostic protocol, including medical history review, skin tests, specific IgE, and drug provocation tests. Five patients were delabeled directly, while 127 underwent diagnostic testing. Among 121 participants who completed the protocol, penicillin allergy was confirmed in 13 (10.74%) patients, and the label was retained in an additional 3 patients because of high-risk history, resulting in an overall confirmed allergy rate of 13.2%. The negative predictive values for STs were 99.07% and 94.39% for immediate and delayed reactions, respectively, while the NPV of sIgE for immediate reactions was 100%. No severe reactions occurred during the diagnostic process. Hundred and five out of one hundred and thirty two (79.5%) patients were safely delabeled. These findings confirm the safety and effectiveness of PAD programs in outpatient settings and highlight the potential for improving antibiotic stewardship by reducing unnecessary beta-lactam avoidance.
Key words: penicillin allergy, allergy delabeling, drug provocation test, real-world data, specific IgE
*Corresponding author: Ivan Marković, Special Hospital for Pulmonary Diseases, Zagreb, Croatia. Email address: [email protected]
Received 11 March 2025; Accepted 30 June 2025; Available online 1 September 2025
Copyright: Marković I, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Beta-lactam allergy is the most frequently reported drug allergy. It has been estimated that, in developed countries, 5–15% of the population carries a penicillin allergy label.1 Because of concerns about cross-reactivity between penicillins and other beta-lactams, patients are often advised to avoid all beta-lactam antibiotics. However, most labels are acquired in childhood and are incorrect, as studies indicate that true penicillin allergy can be confirmed only in less than 10% of these patients.2,3 The common reasons for mislabeling are misinterpretation of viral rashes, infection-induced urticaria, somatoform reactions, or predictable side effects, for example, gastrointestinal symptoms as an allergy, or a positive family history of beta-lactam allergy.4
The high number of reported allergies to beta-lactams leads to frequent prescriptions of antibiotics of alternative classes, which results in less effective treatment of bacterial infections, promotion of bacterial resistance, more adverse events, more treatment complications, and increased healthcare costs.5–7 In hospitalized patients, carrying penicillin allergy labels is associated with increased length of hospital stay, higher readmission rates, and higher mortality.8 Therefore, penicillin allergy labels present a global public health concern.
Antimicrobial stewardship programs focus on improving patient outcomes by reducing the emergence and spread of multidrug-resistant infections.5 Documented penicillin allergy and consequent increased use of alternative broad-spectrum antibiotics were associated with an increased risk of Clostridium difficile and methicillin-resistant Staphylococcus aureus (MRSA) infections.9 Implementing penicillin allergy delabeling (PAD) into routine clinical practice is a vital tool for improving antibiotic stewardship, decreasing antibiotic resistance, and optimizing patient care.10
In this study, we report real-world data on delabeling adult patients with a history of penicillin allergy in an outpatient allergy clinic. The objective was to assess the rate of patients with reported penicillin allergy who could be delabeled.
Materials and Methods
Participants and clinical setting
In 2022, a PAD program was launched in the Special Hospital for Pulmonary Diseases, Zagreb, Croatia. We conducted a retrospective analysis of patients who were included in the PAD program from June 2022 to December 2024. Eligible patients were adults (aged 18 or older) with a documented beta-lactam antibiotic allergy who were referred to the allergy outpatient clinic by general practitioners. Exclusion criteria included a history of a severe cutaneous adverse reaction or an organ immune-mediated injury (drug-induced liver injury, acute interstitial nephritis, or hemolytic anaemia) triggered by a beta-lactam antibiotic. These adverse events represent contraindications for delabeling.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was thoroughly reviewed and approved by the Special Hospital for Pulmonary Diseases Institutional Review Board. In their assessment, the Board deemed the waiver of informed consent as ethically appropriate, considering the retrospective nature and objectives of the study, which posed minimal risk to participants. In addition, stringent data privacy protection measures were implemented, including data anonymization, secure storage, limited access, and adherence to data protection regulations, ensuring participant confidentiality and integrity throughout the research process.
Diagnostic protocol and data collection
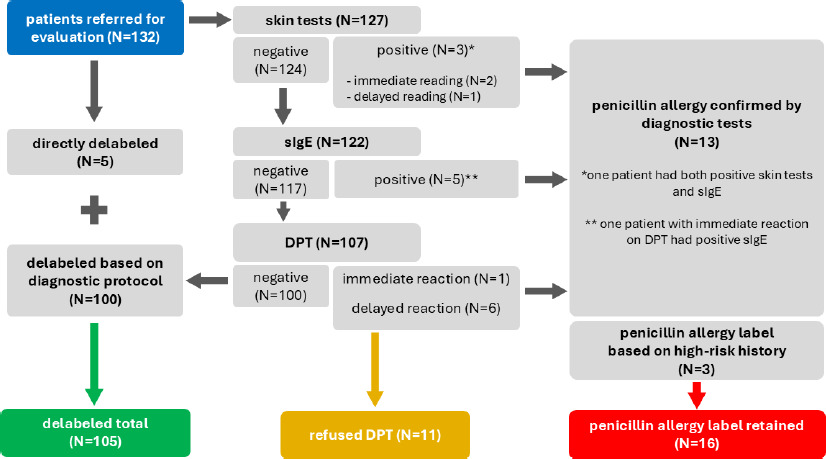
The diagnostic algorithm is shown in Figure 1. Initially, the clinical history and medical records were reviewed by an allergy and clinical immunology specialist for risk stratification. Thereafter, the patients were either delabeled directly or referred for diagnostic evaluation.
Figure 1 Diagnostic protocol and outcomes of the penicillin allergy delabeling program. Flowchart illustrating the diagnostic process for penicillin allergy delabeling, including patient stratification and testing outcomes. Patients were either directly delabeled or underwent diagnostic testing based on clinical history. Skin tests included immediate (20 minutes) and delayed (24–48 hours) readings. Specific IgE (sIgE) to penicillin V and penicillin G was measured in the blood, and drug provocation testing (DPT) was performed in eligible patients. Patients with negative test results were delabeled, while those with positive results or a high-risk history retained their allergy label.
Skin tests (STs) were performed with DAP® Penicillin Test Kit (Diater, Spain), which contains benzylpenicilloyl-octa-L-lysine (BP-OL) and sodium benzylpenilloate, according to the manufacturer’s instructions.11 We also included benzylpenicillin, and amoxicillin and clavulanate (AXC). Negative skin prick tests (SPTs) were followed by intradermal tests (IDTs) with nonirritating concentrations.12 Immediate readings were recorded after 20 minutes, while delayed readings of IDTs were recorded after 24–48 hours in selected patients with a history of a nonimmediate reaction.
Specific IgE (sIgE) to penicillin V (PV) and penicillin G (PG) were determined by ImmunoCAP (Thermo Fisher Scientific/Phadia, Uppsala, Sweden), with a cutoff of 0.35 kIU/L as per the manufacturer’s recommendation.
Drug provocation test (DPT) included oral administration of AXC in a two-step protocol in low-risk patients (25%, followed by 75% of the single dose of 875 mg + 125 mg) or a four-step protocol (1%, followed by 10%, 40%, and 49% of the single dose) in high-risk patients. In case of a history of a nonimmediate reaction, prolonged 3-day DPT was performed by instructing patients to take two additional single doses, once daily, in the following 2 days.
The delabeling was considered successful following negative DPT. Penicillin allergy was confirmed in case of positive STs, sIgE, or DPT. All patients with confirmed penicillin allergy labels were offered further testing to beta-lactams of different classes, such as cephalosporins, with dissimilar side chains.
Data analysis
The study utilized descriptive statistics, specifically aligning with its retrospective design and objectives focused on demographic and clinical insights into allergic reactions to beta-lactam antibiotics. The free MS Excel-based statistical program DAG-STAT13 was used for all calculations.
Results
Out of 132 patients referred for evaluation, none met the exclusion criteria. Demographic data and clinical characteristics of index reactions are shown in Table 1. Five patients were delabeled directly, and others (N=127) underwent diagnostic tests (Figure 1). Overall, 121/132 (91.7%) participants completed the protocol, while others refused the DPT.
Table 1 Basic characteristics of the participants and clinical details of the index reactions.
| N (%) | N (%) | |||
|---|---|---|---|---|
| Patients | Type of IR | |||
| Male | 39 (29.5) | Immediate | 34 (25.8) | |
| Female | 93 (70.5) | Delayed | 25 (18.9) | |
| Total | 132 (100) | Unknown | 73 (55.3) | |
| Mean age | 48 years | Causative drug | ||
| Time since IR | Amoxicillin + clavulanate | 48 (36.4) | ||
| <1 year | 23 (17.4) | Amoxicillin | 9 (6.8) | |
| 1–5 years | 8 (6.1) | Ampicillin | 4 (3) | |
| 5–10 years | 4 (3) | Penicillin G | 25 (18.9) | |
| >10 years | 97 (73.5) | Penicillin V | 4 (3) | |
| Cephalosporin | 5 (3.8) | |||
| Unknown | 37 (28.1) |
IR: index reaction.
The results of the diagnostic test are shown in Table 2. All participants with positive STs (two immediate and one delayed reading) experienced a recent index reaction, ranging from 7 to 12 weeks before testing. Among sIgE-positive patients, three reported the index reaction occurring within 7 months of testing, and two experienced a remote reaction (>10 years).
Table 2 Results of diagnostic tests of patients with a confirmed penicillin allergy diagnosis.
| N | Age (years) | Sex | Type of IR | Time since IR | Drug causing IR | Skin tests | Total IgE (kIU/L) | Specific IgE (kIU/L) | Drug provocation test with AXC | Further evaluation | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PG | PV | ||||||||||
| 1 | 63 | F | Immediate | >10 years | AXC | Neg | 308 | 0.13 | 0.45 | N/D | Tolerated cephalexin |
| 2 | 43 | M | Unknown | >10 years | Unknown | Neg | 442 | 0.05 | 0.52 | Immediate reaction | Tolerated cefuroxime |
| 3 | 34 | M | Immediate | 7 weeks | AXC | Pos (AXC) | 689 | 0.03 | 0.05 | N/D | N/D |
| 4 | 66 | M | Delayed * | 12 weeks | AXC | Pos (BP-OL) | 178 | 3.24 | 3.25 | N/D | Tolerated ceftriaxone |
| 5 | 72 | F | Delayed | >10 years | PG | Neg | 15 | 0 | 0.01 | Delayed reaction (MPE) | N/D |
| 6 | 48 | F | Unknown | >10 years | PV | Neg | 81 | 0.01 | 0.03 | Delayed reaction (FDE) | Tolerated cefuroxime and ceftriaxone |
| 7 | 64 | F | Delayed | >10 years | AMP | Neg | N/D | N/D | N/D | Delayed reaction (MPE) | Tolerated cefuroxime and PV |
| 8 | 43 | F | Unknown | >10 years | Unknown | Neg | 13 | 0 | 0.01 | Delayed reaction (MPE) | Tolerated cefuroxime |
| 9 | 66 | F | Unknown | 16 weeks | AXC | Neg | 134 | 0.12 | 2.15 | N/D | Tolerated cefuroxime and ceftriaxone |
| 10 | 51 | F | Delayed | 9 weeks | AXC | Pos (AXC)** | 1988 | 0.30 | 0.20 | N/D | Tolerated cefuroxime |
| 11 | 23 | F | Unknown | >10 years | AXC | Neg | 71 | 0 | 0.01 | Delayed reaction (MPE) | N/D |
| 12 | 48 | M | Immediate | 28 weeks | AXC | Neg | 357 | 1.55 | 2.04 | N/D | Tolerated ceftriaxone |
| 13 | 71 | F | Delayed | >10 years | Unknown | Neg | 40 | 0 | 0.01 | Delayed reaction (MPE) | N/D |
AMP: ampicillin; AXC: amoxicillin and clavulanate; BP-OL: benzylpenicilloyl-octa-L-lysine; FDE: fixed drug eruption; IR: index reaction; MPE: maculopapular exanthema; N/D: not done; PG: penicillin G; PV: penicillin V; * delayed-onset urticaria; ** delayed reading of intradermal test.
Most DPTs (N=88) were single-dose graded challenges, while the remaining (N=19) were prolonged, as previously described. A single patient developed a mild systemic reaction 45 minutes after the two-step DPT (Table 2). He had negative STs and a positive sIgE to PV (at the time of the challenge, the results were still pending). Another six patients developed a mild nonimmediate reaction following the DPT.
Penicillin allergy was diagnosed in 13/121 (10.74%) participants who completed the protocol. In three more patients with negative STs and sIgE, but with a high-risk history (severe immediate reaction and the presence of additional risk factors including advanced age and cardiovascular comorbidities in two subjects; high suspicion for drug fever in one subject), we decided not to proceed to the DPT with AXC but to retain the penicillin allergy label instead. Overall, the penicillin allergy label was retained in 16/121 (13.2%) patients.
Eleven patients with confirmed labels subsequently tolerated one or more cephalosporin antibiotics with dissimilar side chains, while the other five patients did not opt for further evaluation. Of note, patient 7 (Table 2) tolerated PV in a DPT, which confirmed the diagnosis of a selective aminopenicillin allergy. Patient 3 had a positive skin test with AXC and clavulanate, and a negative skin test with amoxicillin, implying a selective clavulanate allergy, but he refused DPT with amoxicillin or PV.
In summary, delabeling was successful in 105/132 (79.5%) subjects. In a subgroup of patients who underwent DPT (N=107), STs’ negative predictive value (NPV) was 99.07% and 94.39% for immediate and delayed reactions, respectively. The NPV of sIgE for immediate reactions was 100% in our group. No patient developed a systemic reaction to penicillin skin testing. There were no severe immediate or delayed reactions after the DPT.
Discussion
In this study, we retrospectively analyzed the rate of patients with a beta-lactam allergy label who can be safely delabeled, and estimated the rate of true allergy, both immediate and delayed-type, to penicillin antibiotics. With a successful delabeling rate of 79.5%, our study aligns with existing literature suggesting that the majority of penicillin allergy labels are erroneous.1,3–5 This result underscores the significant potential for PAD programs to improve patient outcomes and enhance antibiotic stewardship.
Our PAD program was based on a stepwise diagnostic protocol performed by allergists in an outpatient clinic, which included focused history, STs, sIgE, and DPT. All patients who were not delabeled directly underwent diagnostic tests before proceeding to DPT. In five of these subjects, in vitro tests were not performed because of technical issues.
Clinical decision-making tools have been developed14–16 and validated,14 enabling risk stratification in patients with reported penicillin allergy. Patients with an estimated low risk for severe reactions may be cleared for direct oral challenges, which would save resources and enable access to PAD programs for a higher number of subjects in different clinical settings, while patients at high risk would be referred for a complete allergy evaluation. In a Norwegian PAD program performed in a hospital setting outside an allergy clinic, 49% of the subjects were delabeled through a direct oral challenge without any serious adverse events,17 indicating the feasibility and safety of an algorithm based on risk stratification. In contrast to this study, we aimed to assess the safety of a PAD program led by allergists and estimate the diagnostic performance (NPVs) of sIgE and STs in the Croatian population. Therefore, we performed diagnostic tests according to the protocol in all eligible subjects (excluding those who could be delabeled directly) instead of selecting low-risk patients for direct oral challenge. However, in the future, implementing simple clinical decision-making tools could significantly enhance the PAD program.
In our group, allergy to at least one penicillin antibiotic was confirmed in 13/121 (10.74%) patients who completed the protocol. The penicillin allergy label was retained in three more skin test – and sIgE-negative participants with a high-risk history, so the final rate of confirmed labels was 13.22%. Two of these patients reported a history of severe but remote immediate reaction to penicillin derivatives, and both had cardiovascular comorbidities as risk factors for severe anaphylaxis. The third patient had a convincing history of drug fever related to AXC.
Although STs and sIgE to penicillins have high NPV, their sensitivity is relatively low.18 Moreover, a significant proportion of penicillin-allergic patients lose their sensitivity over time, and both STs and sIgE are less likely to be positive if performed years after the index reaction.19,20 In the study by Rosenfield et al., 12 out of 222 skin test-negative patients reacted to the DPT (5.4% false negative rate).21 Taking this into account, we decided not to expose patients with a high-risk history to AXC in a DPT but to offer allergy testing to cephalosporins with dissimilar side chains instead. Two participants (including the one with suspected drug fever) opted for further workup and tolerated cefuroxime in a DPT. Although maintaining allergy labels solely based on high-risk history, without having performed DPT, may have led to overestimating our cohort’s actual penicillin allergy rate, we still suggest that this cautious individualized approach aligns well with real-world clinical practice.
The diagnosis of penicillin allergy was confirmed by STs or sIgE in six patients and by DPT in seven patients. All reactions after the DPT (one immediate and six delayed) were mild, and there were no serious adverse events. The allergy was classified as immediate-type in six, and as delayed-type in seven patients.
Peculiarly, patient 4 (Table 2) reported a history of a recent hypersensitivity reaction manifesting as urticarial eruption with an onset >24 hours after taking the last dose of AXC. The diagnostic evaluation revealed both positive immediate readings of IDT to major penicillin determinant (BP-OL) and positive sIgE to PV and PG. Delayed-appearing urticaria is a recognized clinical phenotype of nonimmediate hypersensitivity reactions to beta-lactam antibiotics.22 Atanaskovic-Markovic et al. investigated a group of 1026 children who reported nonimmediate reactions to beta-lactam antibiotics.23 Among 19 subjects with a positive DPT, 13 developed urticaria, and 3 had urticaria and angioedema. The median time interval to the onset of symptoms was 13 hours (range 2–48 hours) after the last dose. In this cohort, there were four positive immediate readings of IDTs, which, according to the authors’ explanation, may be because of inaccurate reporting of the timing of reactions by parents. The description of the index reaction in our patient might have been prone to recall bias. The patient may have developed new sensitization during treatment with AXC and failed to notice and report milder symptoms at the onset of the reaction after the last dose. Considering all these factors, the allergic reaction in this patient was classified as immediate-type.
Our results show a low level of agreement between penicillin STs and in vitro tests, as only one out of five patients with a positive sIgE also displayed a positive immediate reading of IDT to the major penicillin determinant. Another patient with a positive immediate reading of IDT to AXC had a likely diagnosis of a selective allergy to clavulanate, as previously explained, and thus sIgE to the components we used (PV and PG) is not expected to be positive. Although in vitro allergy tests to penicillins lack sensitivity and the range of allergens is limited,24 elevated sIgE levels have been related to a history of immediate type reactions, circulatory symptoms, angioedema, and adrenaline treatment.25 Sousa-Pinto et al. assessed the diagnostic accuracy of both in vivo and in vitro penicillin allergy diagnostic tests in a meta-analysis, revealing a summary sensitivity of 30.7% and 19.3%, and a specificity of 96.8% and 97.4% for STs and sIgE, respectively.18
Strikingly, patient 12 (Table 2), who developed anaphylaxis with ST-elevation myocardial infarction (Kounis syndrome) during intravenous infusion of AXC and shortly after intramuscular application of gentamicin, had negative STs, but sIgE to PG and PV were elevated. The reaction occurred 7 months before testing. If in vitro tests had not been included in our diagnostic algorithm, this patient might have been unnecessarily subjected to the high risk associated with a DPT. In a study by Blanca et al., 2 out of 10 patients who had negative STs reacted but developed a reaction during the DPT were found to have had positive sIgE to amoxicilloyl or benzylpenicilloyl. Moreover, positive in vitro tests were found in a significant proportion of patients with negative STs who had experienced two or more immediate reactions to a penicillin antibiotic or had developed systemic reactions after skin testing despite being skin test negative.26 Considering the relatively low sensitivity of diagnostic tests,18 estimating an individual risk based on clinical judgment remains of utmost importance.
This study has some limitations. Firstly, the participants were adults referred by those general practitioners who were aware of the launch of the PAD program in our institution. Therefore, the study may be subject to referral bias, and the results may not be entirely generalizable. Furthermore, we did not perform sIgE to amoxicillin as the test was unavailable at our center during the study period. Including this test in the diagnostic protocol might improve the accuracy of in vitro diagnostics. Particularly, it might aid in discerning patients with a selective aminopenicillin allergy who could yet be treated with PG or PV.
Also, the protocols for DPT differed based on allergists’ judgment and clinical decisions. Not all patients with a history of delayed reactions underwent a prolonged 3-day challenge, so some of the delayed reactions might have been missed. However, our results show that a single dose of AXC was sufficient to cause a type 4 hypersensitivity reaction in at least four out of six patients (Table 2).
In our protocol, AXC was selected for the DPT because of its widespread availability and practicality, as it is the most commonly prescribed beta-lactam antibiotic in Croatia.27 However, it’s important to note that clavulanate by itself can sometimes cause allergic reactions, which may result in false-positive results.
Despite these limitations, we emphasize that this study was intended to estimate the performance of a PAD program in a real-world clinical setting, thereby filling a gap in the existing literature and providing new insights and practical implications for future PAD protocols. Further strengths of the study include a large sample size and the implementation of a comprehensive diagnostic protocol, ensuring more accurate identification of true allergies.
Conclusion
The majority of patients with a label of penicillin allergy can be safely delabeled. Considering the high prevalence of labels, their public health implications, and consequent economic burden, PAD programs should be pursued. Further research is needed to evaluate the performance and concordance between different diagnostic tests and to optimize the delabeling protocols.
Acknowledgements
The authors would like to express their gratitude to the patients who participated in this study and to the medical staff at the Special Hospital for Pulmonary Diseases, Zagreb, for their invaluable support in implementing the penicillin allergy delabeling program.
Authors Contribution
IM conceptualized and designed the study and wrote the original draft. VVL secured funding and supervised the study. All authors contributed to writing and editing the manuscript, interpreted the results, and gave the final approval.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
Funding
The authors received no funding for this article.
REFERENCES
1 Blumenthal KG, Peter JG, Trubiano JA, Phillips EJ. Antibiotic allergy. Lancet. 2019 Jan;393(10167):183–98. 10.1016/S0140-6736(18)32218-9
2 Castells M, Khan DA, Phillips EJ. Penicillin Allergy. Longo DL, editor. N. Engl. J. Med. 2019 Dec 12;381(24):2338–51. 10.1056/NEJMra1807761
3 Iuliano S, Senn L, Moi L, Muller YD, Ribi C, Buss G, et al. Management of beta-lactam antibiotics allergy: a real-life study. Front. Allergy. 2022 Apr 8;3:853587. 10.3389/falgy.2022.853587
4 Brockow K, Wurpts G, Trautmann A. Patients with questionable penicillin (beta-lactam) allergy: Causes and solutions. Allergol Sel. 2022 Jan 1;6(01):33–41. 10.5414/ALX02310E
5 Stone CA, Trubiano J, Coleman DT, Rukasin CRF, Phillips EJ. The challenge of de-labeling penicillin allergy. Allergy. 2020 Feb;75(2):273–88. 10.1111/all.13848
6 Lee R. Penicillin allergy delabeling can decrease antibiotic resistance, reduce costs, and optimize patient outcomes. Fed. Pract. [Internet]. 2020 Oct 10 [cited 2025 Jan 5];(Vol 37 No 10). Available from: https://www.mdedge.com/fedprac/article/229631/hospital-medicine/penicillin-allergy-delabeling-can-decrease-antibiotic
7 Fransson S, Boel JB, Mosbech HF, Garvey LH. Penicillin allergy delabeling has a significant impact on subsequent antibiotic use in primary care. World Allergy Organ. J. 2024 Sep 17(9):100958. 10.1016/j.waojou.2024.100958
8 Macy E and Contreras R. Health care use and serious infection prevalence associated with penicillin “allergy” in hospitalized patients: a cohort study. J. Allergy Clin. Immunol. 2014 Mar 133(3):790–6. 10.1016/j.jaci.2013.09.021
9 Blumenthal KG, Lu N, Zhang Y, Li Y, Walensky RP, Choi HK. Risk of meticillin resistant Staphylococcus aureus and Clostridium difficile in patients with a documented penicillin allergy: population based matched cohort study. BMJ. 2018 Jun 27;k2400. 10.1136/bmj.k2400
10 Doña I, Labella M, Bogas G, Sáenz De Santa María R, Salas M, Ariza A, et al. Antibiotic allergy de-labeling: a pathway against antibiotic resistance. Antibiotics. 2022 Aug 3;11(8):1055. 10.3390/antibiotics11081055
11 smpc_dap_penicilina_en.pdf [Internet]. [cited 2025 Jan 4]. Available from: https://www.diater.com/media/attachments/2023/08/03/smpc_dap_penicilina_en.pdf
12 Brockow K, Garvey LH, Aberer W, Atanaskovic-Markovic M, Barbaud A, Bilo MB, et al. Skin test concentrations for systemically administered drugs—an ENDA / EAACI Drug Allergy Interest Group position paper. Allergy. 2013 Jun;68(6):702–12. 10.1111/all.12142
13 Mackinnon A. A spreadsheet for the calculation of comprehensive statistics for the assessment of diagnostic tests and inter-rater agreement. Comput. Biol. Med. 2000 May 30(3):127–34. 10.1016/S0010-4825(00)00006-8
14 Trubiano JA, Vogrin S, Chua KYL, Bourke J, Yun J, Douglas A, et al. Development and validation of a penicillin allergy clinical decision rule. JAMA Intern. Med. 2020 May 1;180(5):745. 10.1001/jamainternmed.2020.0403
15 Su C, Belmont A, Liao J, Kuster JK, Trubiano JA, Kwah JH. Evaluating the PEN-FAST clinical decision-making tool to enhance penicillin allergy delabeling. JAMA Intern. Med. 2023 Aug 1;183(8):883. 10.1001/jamainternmed.2023.1572
16 Sabato V, Gaeta F, Valluzzi RL, Van Gasse A, Ebo DG, Romano A. Urticaria: the 1-1-1 criterion for optimized risk stratification in β-lactam allergy delabeling. J. Allergy Clin. Immunol. Pract. 2021 Oct 9(10):3697–704. 10.1016/j.jaip.2021.05.037
17 Alnæs MB, Oppegaard O, Kittang BR, Lygre SHL, Langeland AB, Skodvin B, et al. A new pathway for penicillin delabeling in Norway. World Allergy Organ. J. 2023 Nov 16(11):100829. 10.1016/j.waojou.2023.100829
18 Sousa-Pinto B, Tarrio I, Blumenthal KG, Araújo L, Azevedo LF, Delgado L, et al. Accuracy of penicillin allergy diagnostic tests: a systematic review and meta-analysis. J Allergy Clin. Immunol. 2021 Jan 147(1):296–308. 10.1016/j.jaci.2020.04.058
19 Doña I, Guidolin L, Bogas G, Olivieri E, Labella M, Schiappoli M, et al. Resensitization in suspected penicillin allergy. Allergy. 2023 Jan;78(1):214–24. 10.1111/all.15508
20 Solensky R and Khan DA. Evaluation of antibiotic allergy: the role of skin tests and drug challenges. Curr. Allergy Asthma. Rep. 2014 Sep 14(9):459. 10.1007/s11882-014-0459-z
21 Rosenfield L, Kalicinsky C, Warrington R. A retrospective comparison of false negative skin test rates in penicillin allergy, using pencilloyl-poly-lysine and minor determinants or Penicillin G, followed by open challenge. Allergy Asthma Clin. Immunol. 2015 Dec 11(1):34. 10.1186/s13223-015-0098-5
22 Romano A, Atanaskovic-Markovic M, Barbaud A, Bircher AJ, Brockow K, Caubet J, et al. Towards a more precise diagnosis of hypersensitivity to beta-lactams—an EAACI position paper. Allergy. 2020 Jun;75(6):1300–15. 10.1111/all.14122
23 Atanaskovic-Markovic M, Gaeta F, Medjo B, Gavrovic-Jankulovic M, Cirkovic Velickovic T, Tmusic V, et al. Nonimmediate hypersensitivity reactions to beta-lactam antibiotics in children—our 10-year experience in allergy workup. Pediatr. Allergy Immunol. 2016 Aug 27(5):533–8. 10.1111/pai.12565
24 Wurpts G, Aberer W, Dickel H, Brehler R, Jakob T, Kreft B, et al. Guideline on diagnostic procedures for suspected hypersensitivity to beta-lactam antibiotics. Allergol Sel. 2020 Jan 1;4(01):11–43. 10.5414/ALX02104E
25 Lendal V, Fransson S, Mosbech H, Boel JB, Kahlhofen N, Blom LH, et al. Clinical relevance of specific IgE in penicillin allergy investigation. Int. Arch. Allergy Immunol. 2024 Oct 25;1–8. 10.1159/000541243
26 Blanca M, Mayorga C, Torres MJ, Reche M, Moya C, Rodriguez JL, et al. Clinical evaluation of pharmacia CAP systemTM RAST FEIA amoxicilloyl and benzylpenicilloyl in patients with penicillin allergy. Allergy. 2001 Sep;56(9):862–70. 10.1034/j.1398-9995.2001.00995.x
27 Petrac L, Gvozdanovic K, Perkovic V, Petek Zugaj N, Ljubicic N. Antibiotics prescribing pattern and quality of prescribing in Croatian dental practices-5-year national study. Antibiotics. 2024 Apr 9;13(4):34. 10.3390/antibiotics13040345