
Download
ORIGINAL ARTICLE
Feasibility of MASK-air® use in allergic rhinitis patients receiving immunotherapy and the effect on quality of life
Özge Kama Başcia*, Arzu Yorgancioglub, Soner Gunesc, Cengiz Kirmazd
aBalikesir University, Faculty of Medicine, Department of Internal Medicine, Bigadiç Caddesi, Balıkesir, Türkiye
bManisa Celal Bayar University, Faculty of Medicine, Department of Pulmonology, Manisa, Türkiye
cDenizli Pamukkale District Health Directorate, Department of Public Health, Denizli, Türkiye
dManisa Celal Bayar University, Faculty of Medicine, Department of Internal Medicine, Division of Immunology and Allergy, Manisa, Türkiye
Abstract
Background: The aim of MASK-air® application is to enhance awareness of allergic rhinitis (AR) and its complications, thereby reducing the risk of developing asthma.
Objective: The aims of this study were to evaluate the impact of MASK-air® on the quality of life (QoL) and symptomatology of AR patients undergoing allergen immunotherapy (AIT). The study also evaluated patient satisfaction with the application.
Materials and Methods: A prospective cross-sectional study was conducted between August and November 2019 at a tertiary Allergy and Immunology center involving patients receiving AIT. Participants were instructed on accessing and utilizing MASK-air® daily through face-to-face interviews. Concurrently, the Score for Allergic Rhinitis (SFAR) and the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) were administered alongside MASK-air® Visual Analog Scale (VAS) scores. After 6 months, RQLQ scores were reassessed and a satisfaction survey was conducted.
Results: This study comprised 96 patients. Significant correlations were observed among SFAR, RQLQ, and VAS scores. After 6 months of MASK-air® usage, improvements in QoL and symptom reduction were evident. Notably, participants who consistently used MASK-air® demonstrated significant reductions in activity limitations and hay fever scores compared to irregular users (p = 0.05 and p = 0.02, respectively). Additionally, participants under 40 years of age and those with higher education levels exhibited a greater inclination toward online monitoring via the application. Overall, participants found MASK-air® practical, citing various advantages and disadvantages.
Conclusion: MASK-air® serves as a valuable tool for physicians in managing treatment and is associated with validated, reliable scales. Its use was linked to enhanced QoL and symptom reduction among participants, irrespective of treatment duration.
Key words: allergic rhinitis, immunotherapy, MASK-air®, quality of life
*Corresponding author: Özge Kama Başci, Balikesir University, Faculty of Medicine, Department of Internal Medicine, Bigadiç Caddesi, Balıkesir, Türkiye. Email address: [email protected]
Received 9 September 2024; Accepted 5 March 2025; Available online 1 May 2025
Copyright: Özge KB, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Allergic rhinitis (AR) is a prevalent inflammatory condition of the nasal mucosa that significantly impacts patients’ quality of life (QoL) and functional capacity. It develops as a type 1 hypersensitivity reaction of the nasal airway mucous membranes to external allergens.1 The global prevalence of AR ranges from 15% to 20%, whereas in Türkiye it varies between 8.9% and 27.7%, depending on the region.2,3 AR symptoms can be classified as intermittent or persistent, and their severity is categorized as mild, moderate, or severe based on symptom burden and its impact on QoL. Studies have highlighted the substantial economic burden of AR due to diagnostic and treatment costs, reduced work productivity, and impaired sleep quality.4 Symptom scoring tools, such as the Score for Allergic Rhinitis (SFAR), and QoL assessment scales, such as the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ), are widely utilized for diagnosis and treatment evaluation which have been validated in Türkiye.5
Subcutaneous immunotherapy (SCIT) is the only disease-modifying treatment available for AR and is recommended for patients with moderate to severe persistent AR who are intolerant to or unresponsive to standard therapies. SCIT involves the subcutaneous administration of small amounts of allergen extract to induce immune tolerance. Its initiation requires confirmation of immunoglobulin E (IgE)-mediated AR through diagnostic testing, identification of relevant allergen sensitization, appropriate symptom severity and duration, and access to standardized, high-quality allergen extracts.6 Studies indicate that patients undergoing SCIT for ≥ 36 months experience lower relapse rates compared to those receiving shorter treatment durations.7
With the growing integration of digital health solutions, mobile health (mHealth) applications are increasingly employed in clinical practice to enhance patient self-management and remote monitoring.8 The Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines provide structured treatment pathways for managing rhinitis and asthma, incorporating digital tools to optimize patient outcomes.8 The MASK-air® application, developed within the ARIA framework, is a mobile health tool designed for personalized monitoring and management of AR symptoms. It enables patients to track their symptoms, medication use, and environmental triggers, offering real-time data for healthcare providers.9 A preliminary study on the development of a Turkish version of the MASK-air® app was conducted in April 2018, during which information about its functionality was disseminated among healthcare professionals.10
This study investigates the feasibility and effectiveness of the Turkish adaptation of the MASK-air® app in supporting remote SCIT monitoring. Specifically, it evaluates patient satisfaction, AR symptom control, and QoL improvements before and after mobile app use. Additionally, the usability and sustainability of the app are assessed to determine its potential integration into routine clinical practice.
Materials and Methods
Study design
The institutional review board of Celal Bayar University in Manisa (protocol 20.478.486) approved this study. Patients who underwent SCIT for AR in the Allergy and Immunology Outpatient Clinic of Balikesir University Faculty of Medicine between August and November 2019 were included.
Inclusion criteria for the study:
-
Eighteen years of age or older
-
Using a mobile phone compatible with either iOS or Android operating systems
-
Not having additional chronic diseases
-
Being literate or being accompanied by a literate individual to use the application throughout the study
-
Having symptoms of AR classified according to ARIA and diagnosed with moderate to severe AR
-
Having an allergen sensitivity of 3 (+) or higher in the skin prick test
-
Willingness to participate in the study
Exclusion criteria for the study:
-
Not having a smart phone with an operating system capable of regularly using the Mask-air® application
-
Having additional comorbid diseases or additional allergic conditions
-
Discontinuing treatment or follow-up for any reason
-
Having an acute or chronic infection
-
Forced Expiratory Volume (FEV1) below 70% on pulmonary function test (PFT)
Population
Patients diagnosed with AR at the Allergy Polyclinic, Department of Internal Medicine, Manisa Celal Bayar University, were recruited as study participants. Detailed medical histories were taken from all patients, consent forms confirming their willingness to participate were signed, and demographic characteristics were recorded. A comprehensive history was obtained. An examination of the head, neck, and respiratory system was conducted, confirming nasal and ocular symptoms. A chest X-ray and PFT were performed to rule out the presence of asthma. All patients underwent skin prick tests conducted by an allergy immunology specialist physician and a specialist nurse.
All participants were trained by the same resident physician in the outpatient clinic. The application was installed free of charge on the patients’ phones, and they were instructed on how to enter data into MASK-air®. On the same day, each patient completed their initial personal assessment of AR symptoms. The same physician answered patients’ questions during their first use of the application.
MASK-air® collects information on patients’ baseline characteristics, usual rhinitis symptoms, and disease type (intermittent/persistent). In addition, MASK-air® includes a daily monitoring questionnaire that evaluates how symptoms affect users’ daily lives and the types of treatments used. When participants presented for their monthly SCIT dose, the data they had entered over the past month were reviewed via the QR (Quick Response) code in the application. Face-to-face consultations were continued to ensure regular use of the application.
Skin prick test
The skin prick test applied to the patients in this study included 14 types of allergens, including dust mites (Dermatophagoides farinae, Dermatophagoides pteronyssinus), molds (Alternaria, Aspergillus), cat fur, grasses, tree pollen (olive), weeds (wormwood, stick weed, nerve weed), and latex.
Precautions were taken to ensure that patients had not used antihistamine medications for the 10 days prior to the test. A prick lancet was used to ensure standardization. Histamine hydrochloride at a concentration of 10 mg/mL was used for positive control. Reactions were read by the researcher administering the test after 20 minutes. The skin test was evaluated based on the diameter of the induration, and patients demonstrating equal or greater induration in relation to histamine against the allergens were included in the study.
Data collection
Symptom severity was assessed using the Visual Analog Scale (VAS) integrated into the MASK-air® application. The VAS, ranging from 0 (no symptoms) to 10 (most severe symptoms), allowed participants to record the daily severity of their general condition, nasal and ocular symptoms, asthma symptoms, impact on work productivity, and shortness of breath.
Data recorded in the MASK-air® application was accessed during the patients’ monthly SCIT follow-up visits. At each visit, participants scanned a QR code within the app using their smartphones, allowing clinicians to retrieve their symptom data directly. This approach enabled real-time monitoring of treatment progress and symptom fluctuations while minimizing recall bias in symptom reporting.
Symptom assessment
Symptoms were evaluated daily, monthly, and annually using VAS scores. The SFAR scale was applied to assess symptom severity for AR patients. The SFAR scale consists of eight items, where a score of 7 or higher is considered significant. The RQLQ includes 28 questions across seven components where each symptom is assessed on a severity scale of 0 to 6. The seven main headings are sleep, nonallergic complaints, practical issues, nasal complaints, ocular complaints, activities, and emotional status. Patients were asked to respond to each question with 0 for “No disturbance” to 6 for “Extreme disturbance.” Additionally, patients recorded three activities restricted by their illness in daily life.
Follow-up process and satisfaction survey Implementation
Patients were interviewed whenever they came for immunotherapy doses, the number of times the Mask-Air® application was used was recorded, and encouraged to continue using it. Furthermore, a second RQLQ questionnaire was administered 6 months after the initiation of MASK-air® use. A seven-question survey assessing the usability, applicability, advantages and disadvantages of the mobile health application, and the patients’ future follow-up through remote mobile applications was prepared and administered during the controls 6 months later.
Statistical analyses
After checking and numbering the questionnaire forms, they were recorded in IBM SPSS Statistics (Version 21.0; IBM Corp., Armonk, NY) along with other data obtained from the study. The G-power version 3.1.9.6 was used to determine the sample size. Based on the first and subsequent measurements from the source studies, the effect size was determined as 0.56 and 0.77, respectively,11,12 suggesting a minimum of 44 participants based on a 5% margin of error and a power level of 95%. The study was planned to be conducted with a minimum of 44 participants, and a total of 96 participants were studied.
Descriptive data were presented as frequency, percentage, mean, and standard deviation. Univariate analyses for dependent and independent variables were performed using the Shapiro-Wilk test for variables meeting the normality assumptions. Decisions were made based on histogram evaluations when at least two conditions were met. The t-test was used for binary groups, while ANOVA (Analysis of Variance) (post hoc Tukey) was used for three or more groups. For cases not meeting normality assumptions, the Mann-Whitney U test was used for binary groups and the Kruskal-Wallis test was used for three or more groups. The relationships between continuous variables were examined using the Pearson correlation analysis when normality assumptions were met and Spearman correlation analysis otherwise. A Type 1 error value of p < 0.05 was considered significant.
Results
The study included 96 patients (62 females and 34 males) admitted to the University Allergy and Immunology Clinic. The mean age was 33.9 years, 59.4% had intermittent AR, 42.7% were smokers, and 20.8% lived in rural areas. The most common allergens observed in the skin prick test were grass mix (80, 83.3%), herb and cereal mix (80, 83.3%), Plantago lanceolata (58, 60.4%), Galium aparine (cleavers) (64, 66.6%), Artemisia (36, 37.5%), and house dust mites, including Dermatophagoides pteronyssinus (52, 54.1%) and Dermatophagoides farinae (51, 53.1%). Other notable allergens included Aspergillus fumigatus (33, 34.3%), Aspergillus tenuis (22, 22.9%), cat epithelium (23, 23.9%), olive pollen (20, 20.8%), and latex (5, 5.2%). The mean duration of immunotherapy was 21.8 ± 15.28 months. Table 1 summarizes the demographic and clinical information of the patients.
Table 1 Demographic characteristics and allergic rhinitis features of the patients.
| Baselines characteristics | N (%) | Baselines characteristics | N (%) |
|---|---|---|---|
| Age (years) Mean ± SD | 33.9 ± 9.6 | Year of AIT treatment | |
| Age categories | ≤ 12 months | 35 (36.4) | |
| < 29 years | 33 (34.4) | 13–24 months | 23 (23.9) |
| 30-39 years | 38 ( 39.6) | 25–36 months | 17 (17.7) |
| > 40 years | 25 (26.6) | ≥ 37 months | 21 (21.8) |
| Sex | Positive skin prick test | ||
| Female | 62 | D. Farinea | 51 (53.1) |
| Male | 34 | D. Pteronyssinus | 52 (54.1) |
| Educational status | A. Tenius | 22 (22.9) | |
| Illiterate | 1 | A. Fumigatus | 33 (34.3) |
| Literate | 4 | Cat epithelium | 23 (23.9) |
| Primary school | 14 | Olive | 20 (20.8) |
| Middle school | 8 | Grass mix | 80 (83.3) |
| High school | 28 | Herb and cereal mix | 80 (83.3) |
| University | 37 | Artemisia | 36 |
| Smoking | Plantago lanceolata | 58 | |
| Smoker | 41 (42.7) | Galium aperine | 64 |
| Non-smoker | 55 (57.3) | Latex | 5 |
| Living, n | Type of AIT | ||
| Urban | 76 | Grass, weed, and grain (GWG) | 45 |
| Rural | 20 | House dust mite (HDM) | 20 |
| Year of Diagnosis | GWG + HDM | 27 | |
| ≤ 1 year | 25 | Olive | 2 |
| 2–4 years | 51 | Latex | 1 |
| 5 years | 20 | Cat epithelium | 1 |
| AR Classification, n | |||
| Intermittent | 57 | ||
| Persistent | 39 |
The mean SFAR score recorded during the initial interviews was 13.3 ± 1.5, and 64% of the patients had at least one parent or sibling diagnosed with AR, asthma, or eczema. RQLQ symptom scores, total scores, and most frequently restricted activities scores were calculated before MASK-air® (Table 2). The SFAR total scores and VAS in MASK-air® were analyzed and their correlations with the RQLQ symptom scores were assessed, revealing that all RQLQ symptom scores other than those related to restricted activities were significantly associated with the SFAR scores (p < 0.05).
Table 2 RQLQ scores before and after MASK-air®.
| RQLQ symptoms (n = 96) | Before MASK-air®(RQLQ1) Mean ± SD | 6-Month assessment (RQLQ2) Mean ± SD |
|---|---|---|
| Sleep | 3.53 ± 1.08 | 0.98 ± 0.8 |
| Non-hay fever symptoms | 1.83 ± 1.11 | 0.90 ± 0.84 |
| Practical problems | 2.25 ± 1.68 | 0.99 ± 0.74 |
| Nasal symptoms | 2.54 ± 1.57 | 1.33 ± 0.96 |
| Eye symptoms | 1.80 ± 1.43 | 1.06 ± 0.92 |
| Emotions | 2.69 ± 1.33 | 0.95 ± 0.81 |
| Restricted Activities | 3.53 ± 1.08 | 1.89 ± 0.97 |
| RQLQ Total | 65.80 ± 30.48 | 28.18 ± 14.67 |
| Activities (n) | ||
| House cleaning (39) | 4.02 ± 1.34 | 2.63 ± 1.16 |
| Vacuuming (30) | 3.53 ± 1.22 | 2.10 ± 1.77 |
| Picnic (28) | 3.67 ± 1.51 | 2.07 ± 1.86 |
| Walking (22) | 3.40 ± 1.05 | 2.78 ± 1.52 |
| Outdoor activities (19) | 3.57 ± 1.01 | 2.70 ± 1.50 |
| Gardening (18) | 3.66 ± 1.28 | 2.68 ± 1.53 |
| Go shopping (15) | 3.8 ± 1.26 | 2.59 ± 1.46 |
| Regular social life (14) | 3.28 ± 0.99 | 1.47 ± 1.22 |
| Tinkering (12) | 3.08 ± 1.24 | 1.38 ± 1.10 |
| Driving (11) | 3.27 ± 0.64 | 1.37 ± 1.06 |
MASK-air® VAS scores were correlated with all RQLQ symptom scores, except dyspnea and SFAR (Table 3). While this study excluded patients with a clinical asthma diagnosis, the MASK-air® tool generates an asthma-related score based on patient-reported symptoms. These scores do not indicate the actual presence of asthma, but rather reflect symptom patterns captured by the tool. To ensure clarity, we revised the analysis accordingly. Notably, a strong correlation (p < 0.01) was observed between the MASK-air® workability and classroom discomfort scores and the patients’ total RQLQ scores (Table 3). After a 6-month follow-up, the RQLQ was repeated to compare the overall improvement in QoL and functioning after using the app, with a significant increase in QoL observed across all RQLQ functions (p < 0.001) (Table 2).
Table 3 Comparisons between MASK-air® VAS, SFAR scores, and RQLQ1 symptoms results.
| Mask-air®VAS | Mean ± SD | SFAR p < 0.05 | RQLQ1 symptoms | RQLQ p < 0.05 |
|---|---|---|---|---|
| Global allergy symptoms | 54.2 ± 10.4 | 0.000 | Practical problems | 0.000 |
| Eyes | 50.5 ± 12.9 | 0.000 | Eyes symptoms | 0.000 |
| Nose | 55.8 ± 10.8 | 0.000 | Nasal symptoms | 0.000 |
| Asthma | 46.3 ± 9.5 | 0.000 | Non-hay fever symptoms | 0.000 |
| Work | 47.9 ± 9.1 | 0.001 | Restricted activities | 0.000 |
| Sleep | 51.3 ± 11.5 | 0.000 | Sleep | 0.000 |
| Dyspnea | 45.0 ± 9.2 | 0.071 | Non-hay fever symptoms | 0.000 |
| Classroom discomfort | 44.8 ± 8.5 | 0.000 | Restricted activities | 0.002 |
The RQLQ, VAS, and SFAR scores were examined for the patient’s demographics and medical history. A comparison of genders revealed higher emotional symptom levels in the female respondents (p = 0.041), while no significant differences were noted in other functioning areas. Furthermore, QoL and sleep quality were noted to decline significantly in the smokers (p < 0.05), while the sleep quality (p = 0.037), eye scores (p = 0.045), and total RQLQ scores (p = 0.007) of the patients residing in rural areas were higher than those residing in urban areas. While no distinction was identified between occupational categories, the QoL and functioning of the unemployed respondents were significantly better than those who were employed. The patients were categorized into three subgroups based on the duration of their AR diagnosis: 2 years and less, between 2 and 5 years, and 5 years and over. The symptoms that varied between the different groups are outlined in Table 4. There were no discernible differences in the nasal functions of the patients with intermittent and chronic AR. Among those who underwent several allergen immunotherapy (AIT) treatments, the symptom scores were decreased and the general QoL scores were increased (p = 0.023).
Table 4 RQLQ symptom scores according to year of diagnosis of allergic rhinitis.
| Year of diagnosis | Restricted activities Mean ± SD | Practical problems Mean ± SD | Nasal Mean ± SD | Eye Mean ± SD | Emotions Mean ± SD | RQLQ total Mean ± SD |
|---|---|---|---|---|---|---|
| ≤ 1 year n = 25 | 3.90 ± 0.90 | 3.10 ± 1.71 | 4.69 ± 1.91 | 3.53 ± 1.94 | 4.26 ± 1.87 | 28.38 ± 9.71 |
| 2–4 years n = 51 | 3.19 ± 0.98 | 1.81 ± 1.40 | 2.72 ± 1.73 | 1.86 ± 1.68 | 3.30 ± 1.62 | 18.58 ± 8.51 |
| ≥ 5 years n = 20 | 3.91 ± 1.26 | 2.30 ± 1.96 | 3.45 ± 2.47 | 2.38 ± 1.87 | 3.51 ± 1.89 | 22.43 ± 10.99 |
| p | 0.015 | 0.003 | 0.008 | 0.005 | 0.080 | 0.006 |
Patients were categorized into four groups based on the length of their AIT. During the initial interviews, the patient group in the first year of treatment recorded the highest RQLQ scores. After 6 months of follow-up and treatment, a noticeable and statistically significant improvement was observed in the QoL of the therapy group along with a reduction in symptoms. When comparing RQLQ scores based on treatment duration, significant differences were noted in all parameters during the initial measurement. After 6 months, further improvements were observed, particularly in the Practical Problems subscale, where eye symptoms (p = 0.029) and sleep issues (p = 0.036) showed significant reductions (Table 5).
Table 5 Comparison of RQLQ score reductions after MASK-air® use based on treatment duration.
| RQLQ symptoms months of AIT | n | Mean ± SD | p | |
|---|---|---|---|---|
| Non-hay fever | ≤ 12 | 35 | 11.20 ± 7.85 | 0.060 |
| 13–24 | 23 | 8.69 ± 6.15 | ||
| 25–36 | 17 | 7.47 ± 5.56 | ||
| ≥ 37 | 21 | 6.14 ± 7.53 | ||
| Practical problems | ≤ 12 | 35 | 6.14 ± 4.90 | 0.000 |
| 13–24 | 23 | 2.17 ± 2.49 | ||
| 25–36 | 17 | 3.47 ± 3.71 | ||
| ≥ 37 | 21 | 1.80 ± 4.29 | ||
| Nose | ≤ 12 | 35 | 9.11 ± 6.00 | 0.001 |
| 13–24 | 23 | 4.47 ± 3.55 | ||
| 25–36 | 17 | 5.52 ± 5.37 | ||
| ≥ 37 | 21 | 3.61 ± 5.31 | ||
| Eyes | ≤ 12 | 35 | 5.60 ± 4.94 | |
| 13–24 | 23 | 3.95 ± 3.74 | 0.036 | |
| 25–36 | 17 | 3.00 ± 4.34 | ||
| ≥ 37 | 21 | 2.33 ± 3.56 | ||
| RQLQ Total | ≤ 12 | 35 | 48.05 ± 23.74 | |
| 13–24 | 23 | 31.21 ± 21.81 | 0.005 | |
| 25–36 | 17 | 37.82 ± 24.21 | ||
| ≥ 37 | 21 | 27.14 ± 20.41 | ||
*AIT: Allergen Immunotherapy.
Following six months of consistent MASK-air® use, we conducted a survey to evaluate usage frequency, suitability for purpose, and perceived benefits while collecting additional comments. Patients were categorized into five subgroups based on their usage frequency: daily, more than once a week, less than once a week, more than once a month, and less than once a month. During the MASK-air® usage, distribution (n = 96) was as follows: 18% (n = 18) used the app daily, 23% (n = 22) more than once a week, 20% (n = 19) less than once a week, 24% (n = 23) more than once a month, and 14% (n = 14) less than once a month. The binomial test indicated that all proportions were statistically significant (p < 0.001) when tested against an expected proportion of 0.5.
The group that used the app daily had significantly lower activity limitation scores and nasal-ocular symptoms than other groups (p = 0.05, p = 0.02). However, there was no significant difference in the overall QoL among the groups. Participants who reported benefiting from the intervention demonstrated greater improvements in overall QoL (p = 0.026) and eye symptom scores (p = 0.018).
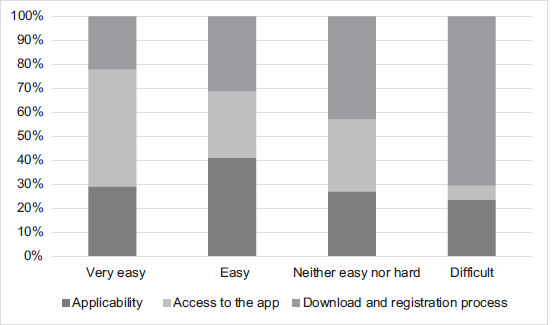
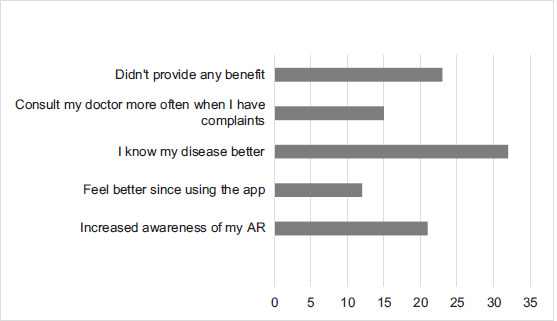
A seven-question survey was designed to assess the MASK-air® application usage process. The majority of patients (51%) reported that they downloaded the program without difficulty and found the registration and usage process straightforward. Additionally, 75% reported benefiting from the application, 33% stated that they gained a better understanding of the disease, 21.9% reported increased disease awareness, 79% experienced no disadvantages while using the program, 24% had difficulty allocating time for regular use, 25% struggled to answer the questions consistently, and six respondents noted that nasal itching was not included among the symptoms in the application.
Survey questions and responses are summarized and presented in detail in Figures 1 and 2. When patients were asked for their thoughts on being followed up in a digital environment to reduce the frequency of hospital admissions in the future, 82% of the respondents gave positive or neutral responses. Among the participants, those aged 40 and older showed a notable decline in interest in distant follow-ups using mobile health apps (p = 0.07). Conversely, a greater preference for digital follow-up was noted as education increased (p = 0.014). Within the various professional groups, civil servants and students had a lower preference for remote monitoring and hospital visits than nonpublic employees and the unemployed (p = 0.005). Finally, no correlation was noted between patient preference for remote digital follow-up and their RQLQ, SFAR, and VAS scores.
Figure 1 Evaluation of Mask-air®.
Figure 2 Advantages of using MASK-air®.
Discussion
This study evaluates the effect of mobile health application use on QoL in AR patients and the correlations between VAS scores recorded on MASK-air®, SFAR, and RQLQ symptom scores. While MASK-air® and its data limitations have been assessed in a limited number of international studies, no study to date has evaluated its limitations, benefits, and disadvantages in Turkey. Additionally, patient satisfaction and perspectives on remote monitoring were among our study’s objectives.
The demographic characteristics of our patient group align with known AR risk factors, including younger age, higher education level, rural residence, and smoking.15 A significant proportion (64%) reported a family history of allergic conditions, consistent with previous studies indicating a higher incidence in individuals with parental allergy history.16 Skin prick testing was used as the primary diagnostic tool, with SFAR as an additional measure. While serum-specific IgE testing is an alternative, its routine use is limited due to high costs.17
Regional climatic and economic differences influence aeroallergen profiles across Turkey.18 In this study, the predominant allergens were pollens (grasses, grains, Galium aperine, Plantago lanceolata, olive pollen), followed by Dermatophagoides pteronyssinus (52%) and Dermatophagoides farinae (51%). House dust mites were particularly prevalent in coastal areas, including Manisa, where Mediterranean flora and olive trees contribute to sensitization. Among patients who underwent AIT, 28% were treated for grass weed and house dust mite allergens.
Impact of smoking on quality of life
Active smokers had higher RQLQ symptom scores and lower QoL than nonsmokers. While one study on 1144 AR patients found no significant impact of smoking on nasal symptoms and RQLQ scores, another reported reduced efficacy of AIT in smokers.16,22 Given that all participants in our study were AIT recipients, smoking may have influenced RQLQ scores by diminishing treatment effectiveness.
Effectiveness of MASK-air® and VAS correlations
MASK-air® is a validated tool for AR management, with its initial phase studies published in 2015.23 In our study, VAS scores significantly correlated with SFAR and RQLQ, reinforcing previous findings that mobile health applications can effectively track disease severity. The 2017 MASK-air® study by the ARIA group showed that many individuals using the application had not been formally diagnosed with AR, did not consistently report their data, or failed to regularly adhere to their prescribed treatments.24 Moreover, it is known that many individuals with AR remain undiagnosed due to not consulting a physician, and among those who do seek medical care, patients with mild/moderate symptoms are more likely to discontinue follow-ups compared to those with severe symptoms.25,26
Therefore, our study was conducted with a homogeneous patient population consisting of individuals with moderate to severe AR who were under AIT and regular follow-up, ensuring the sustainability of MASK-air® use and monthly monitoring while minimizing the influence of frequent treatment changes or untreated cases.
A multicenter study analyzing MASK-air® data from 14,189 participants across 23 countries demonstrated significant correlations between work efficiency (VAS work) and other VAS categories, including nasal and ocular symptoms.27 The European Academy of Allergy and Clinical Immunology (EAACI)-defined Combined Symptom and Medication Score (CSMS) is commonly used to assess treatment effectiveness, but due to inconsistent antihistamine and nasal steroid use among our participants, CSMS was not calculated.
Quality of life improvement and AIT duration
No prior study has investigated the relationship between MASK-air® use and RQLQ. Our findings indicate a significant improvement in QoL following AIT. Studies on AIT-related QoL have shown substantial improvements across different sensitization types and treatment modalities.11,28 A 2017 study applying RQLQ at baseline, 6 months, and 1 year posttreatment in SCIT and SLIT (sublingual immunotherapy) groups found significant enhancements in overall QoL and RQLQ subdomains within the first 6 months.29
In our study, RQLQ and symptom scores were recorded at baseline and 6 months post-AIT. Patients were categorized based on treatment duration, revealing significant symptom reductions and improved QoL across all groups. While all patients demonstrated decreased RQLQ scores at 6 months, differences between those treated for ≤ 1 year and those treated for ≥ 2 years were not statistically significant. Correlation analysis suggested that the gap between pre- and posttreatment RQLQ scores narrowed with shorter treatment durations. Notably, the most significant improvements occurred in patients treated for ≤ 1 year, indicating that symptom relief observed in 65% of patients treated for longer durations may not be solely attributable to AIT.
User experience and compliance with MASK-air®
A unique aspect of this study is the MASK-air® evaluation questionnaire, which has never been documented in prior literature. MASK-air® aims to aid treatment decision-making, facilitate symptom monitoring, and enhance patient engagement in clinical practice.6,8 In our patient survey, users found the application easy to use and relevant to their condition. The most commonly reported benefits were improved symptom recognition and increased disease awareness, aligning with our study’s objectives.
The primary barriers to mobile health research include ethical considerations and patient compliance. In a large-scale study, among 14,000 MASK-air® users, the median usage duration was 4 days for volunteers and 2 days for participants from Türkiye.27 Another study reported an estimated secondary compliance rate of only 5% among users.30 In our study, only 18% of respondents reported daily MASK-air® use, with irregular usage and data gaps preventing accurate VAS score calculations.
When questioned about difficulties using the MASK-air® app, many patients reported challenges in maintaining regular engagement, reflecting findings from earlier mobile health studies.25 The most common complaint was notification inconsistencies, with users stating that notifications disappeared after a week of inactivity. However, this issue seems to reflect a lack of regular app use rather than a technical flaw.
Study limitations
This study has several limitations. First, patient compliance with MASK-air® use was suboptimal, with only 18% of participants reporting daily use. This irregularity led to data gaps, preventing accurate VAS score calculations and limiting the assessment of symptom fluctuations over time.
Second, the study population consisted exclusively of AIT recipients, which may have introduced selection bias. Since patients not receiving AIT were excluded, our findings on QoL improvements cannot be generalized to all AR patients.
Third, treatment adherence and medication use (e.g., antihistamines, nasal steroids) were self-reported and not actively monitored. Consequently, the study could not calculate CSMS, a standard metric for AR management.
Fourth, the study followed a cross-sectional design, which restricts the ability to establish causal relationships between MASK-air® use and QoL improvements. Longitudinal studies with extended follow-up periods could provide more robust insights.
Finally, regional variations in aeroallergen exposure and environmental factors may have influenced patient responses. Although the study included participants from different regions, climatic and socioeconomic factors were not explicitly controlled, which could have affected symptom severity and treatment outcomes.
Conclusion
With the rise of mobile health apps and digital accessibility, these tools are becoming essential for diagnosis and treatment or in self-diagnosis and early initiation of treatment for the undiagnosed. It is noteworthy that younger respondents with higher levels of education, government employees who may struggle to find time for hospital visits during working hours, and students were more positive toward this goal. In conclusion, the idea of disease monitoring through mobile technology was welcomed and the supporting benefits of the MASK-air® application, which is increasingly being used in clinical trials, were recognized. The idea of digital follow-up was of particular interest to participants who were employed and had a high level of education. VAS scores from the program showed a strong correlation with scores generated by the RQLQ and SFAR scales.
Author Contributions
All authors contributed equally to this article.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to research, authorship and/or publication of this article.
Funding
None.
REFERENCES
1 Kozma CM, Sadik MK, Watrous ML. Economic outcomes for the treatment of allergic rhinitis. Pharmacoeconomics 1996;10(1):4–13. 10.2165/00019053-199610010-00002
2 Mims JW. Epidemiology of allergic rhinitis. Int Forum Allergy Rhinol 2014;4(Suppl 2):18–20. 10.1002/alr.21385
3 Kurt E, Metintas S, Basyigit I, Bulut I, Coskun E, Dabak S, et al. Prevalence and risk factors of allergies in Turkey (PARFAIT): Results of a multicentre cross-sectional study in adults. Eur Respir J 2009;33(4):724–33. 10.1183/09031936.00082207
4 Reed SD, Lee TA, McCrory DC. The economic burden of allergic rhinitis: A critical evaluation of the literature. Pharmacoeconomics 2004;22(6):345–61. 10.2165/00019053-200422060-00002
5 Cingi C, Songu M, Ural A, Annesi-Maesano I, Erdogmus N, Bal C, et al. The score for allergic rhinitis study in Turkey. Am J Rhinol Allergy 2011;25(5):333–7. 10.2500/ajra.2011.25.3665
6 Zuberbier T, Bachert C, Bousquet PJ, Passalacqua G, Walter Canonica G, Merk H, et al. GA2 LEN/EAACI pocket guide for allergen-specific immunotherapy for allergic rhinitis and asthma. Allergy 2010;65(12):1525–30. 10.1111/j.1398-9995.2010.02474.x
7 Penagos M, Durham SR. Allergen immunotherapy for long-term tolerance and prevention. J Allergy Clin Immunol 2022;149(3):802–11. 10.1016/j.jaci.2022.01.007
8 Bousquet J, Schünemann HJ, Samolinski B, Demoly P, Baena-Cagnani CE, Bachert C, et al. Allergic rhinitis and its impact on asthma (ARIA): Achievements in 10 years and future needs. J Allergy Clin Immunol 2012;130(5):1049–62. 10.1016/j.jaci.2012.07.053
9 Yorgancıoğlu AA, Kalayci Ö, Cingi C, Gemicioğlu B, Kalyoncu AF, Agache I, et al. ARIA 2016 executive summary: Integrated care pathways for predictive medicine across the life cycle. Tuberk Toraks 2017;65(1):32–40. 10.5578/tt.52766
10 Yorgancıoğlu AA, Gemicioğlu B, Kalaycı Ö, Kalyoncu AF, Cingi C, Murray R, et al. Türkiye’de mask (Mobile Airways Sentinel networK) allerji günlüğü uygulaması: Allerjik rinit ve astımda arıa ile bütünleşmiş mobil teknoloji kullanımı. Tuberk Toraks 2018;66(2):176–81. 10.5578/tt.66913
11 Cuesta-Herranz J, Laguna JJ, Mielgo R, Pérez-Camo I, Callejo AM, Begoña L, et al. Quality of life improvement with allergen immunotherapy treatment in patients with rhinoconjunctivitis in real life conditions. Results of an observational prospective study (ÍCARA). Eur Ann Allergy Clin Immunol 2019;51(5):10.23822/EurAnnACI.1764-1489.104. 10.23822/EurAnnACI.1764-1489.104
12 Morris MS, Lowery A, Theodoropoulos DS, Duquette RD, Morris DL. Quality of life improvement with sublingual immunotherapy: A prospective study of efficacy. J Allergy (Cairao) 2012;2012:1–6. 10.1155/2012/253879
13 Yalcin AD, Öncel S, Akcan A, Eravsar K, Polat HH, Terzioglu E. Antalya’da 16 yaş üstünde allerjik astim, rinit ve konjonktivit prevalansi. Turkiye Klin J Med Sci 2010;30(3):888–94. 10.5336/medsci.2008-9901
14 Fröhlich M, Pinart M, Keller T, Reich A, Cabieses B, Hohmann C, et al. Is there a sex-shift in prevalence of allergic rhinitis and comorbid asthma from childhood to adulthood? A meta-analysis. Clin Transl Allergy 2017;7:44. Published 2017 Dec 5. 10.1186/s13601-017-0176-5
15 Zhang Y, Lan F, Zhang L. Advances and highlights in allergic rhinitis. Allergy 2021;76(11):3383–9. 10.1111/all.15044
16 Bousquet PJ, Cropet C, Klossek JM, Allaf B, Neukirch F, Bousquet J. Effect of smoking on symptoms of allergic rhinitis. Ann Allergy Asthma Immunol 2009;103(3):195–200. 10.1016/S1081-1206(10)60181-0
17 Roberts G, Pfaar O, Akdis CA, Ansotegui IJ, Durham SR, Gerth van Wijk R, et al. EAACI guidelines on allergen immunotherapy: Allergic rhinoconjunctivitis. Allergy 2018;73(4):765–98. 10.1111/all.13317
18 Sakar A, Yorgancioglu A, Dinc G, Yuksel H, Celik P, Dagyildizi L, et al. The prevalence of asthma and allergic symptoms in Manisa, Turkey (a western city from a country bridging Asia and Europe). Asian Pacific J Allergy Immunol 2006;24(1):17–25.
19 Başak O, Başak S, Gültekin B, Tekin N, Söylemez A. The prevalence of allergic rhinitis in adults in Aydin, Turkey. Rhinology 2006;44(4):283–7.
20 Öztürk Ö, Tokmak A, Güçlü E. Skin prick test results of patients with allergic rhinitis in Düzce. Duzce Med J 2005;7(1):11–4.
21 Edıger D, Günaydin FE, Erbay M, Şeker Ü. Trends of sensitization to aeroallergens in patients with allergic rhinitis and asthma in the city of Bursa, south Marmara sea region of Turkey. Turkish J Med Sci 2020;50(2):330–6. Published 2020 Apr 9. 10.3906/sag-1908-139
22 Specjalski K, Łata J, Wasilewska E, Chełmińska M, Jassem E, Niedoszytko M, et al. Smoking history is negatively associated with allergen specific immunotherapy efficacy: A retrospective analysis. Postep Dermatologii i Alergol 2019;36(6):673–6. 10.5114/ada.2018.80654
23 Vieira RJ, Sousa-Pinto B, Cardoso-Fernandes A, Jácome C, Portela D, Amaral R, et al. Control of allergic rhinitis and asthma test: A systematic review of measurement properties and COSMIN analysis. Clin Transl Allergy 2022;12(9):e12194. 10.1002/clt2.12194
24 Brożek JL, Bousquet J, Agache I, Agarwal A, Bachert C, Bosnic-Anticevich S, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines—2016 revision. J Allergy Clin Immunol 2017;140(4):950–8. 10.1016/j.jaci.2017.03.050
25 Bousquet J, Arnavielhe S, Bedbrook A, Bewick M, Laune D, Mathieu-Dupas E, et al. MASK 2017: ARIA digitally-enabled, integrated, person-centred care for rhinitis and asthma multimorbidity using real-world-evidence. Clin Transl Allergy 2018;8:45. Published 2018 Oct 25. 10.1186/s13601-018-0227-6
26 Spinozzi F, Murgia N, Baldacci S, Maio S, Pala AP, Casciari C, et al. Characteristics and predictors of allergic rhinitis undertreatment in primary care. Int J Immunopathol Pharmacol 2016;29(1):129–36. 10.1177/0394632015595779
27 Bédard A, Antó JM, Fonseca JA, Arnavielhe S, Bachert C, Bedbrook A, et al. Correlation between work impairment, scores of rhinitis severity and asthma using the MASK-air® App. Allergy 2020;75(7):1672–88. 10.1111/all.14204
28 Pedregal-Mallo D, Pacheco E, Rodrigo JP, Llorente JL, Alvarez-Marcos C. Impact of immunotherapy on quality of life in patients with house dust mite allergic rhinitis. Allergy. 2020;75(7):1783–5. 10.1111/all.14215
29 Schwanke T, Carragee E, Bremberg M, Reisacher WR. Quality-of-life outcomes in patients who underwent subcutaneous immunotherapy and sublingual immunotherapy in a real-world clinical setting. Am J Rhinol Allergy 2017;31(5):310–6. 10.2500/ajra.2017.31.4465
30 Menditto E, Guerriero F, Orlando V, Crola C, Di Somma C, Illario M, et al. Self-assessment of adherence to medication: A case study in campania region community-dwelling population. J Aging Res 2015;2015:682503. 10.1155/2015/682503