
Download
CASE REPORT
Anaphylaxis due to green beans (Phaseolus vulgaris): a new phenotype?
Estela Menéndez Riveroa*, Manuel Prados Castañoa, Isabel María Domínguez Romeroa, María José Martínez Martínezb, Fernando Pineda De La Losab
aAllergy Department, Hospital Universitario Virgen del Rocío, Seville, Spain
bDepartment of Research and Development, Inmunotek SL, Alcalá de Henares, Madrid, Spain
Abstract
Background: Anaphylaxis is a severe allergic reaction with increasing incidence in Europe. It is often caused by food, insect venom, and drugs. White, red, and green beans (Phaseolus vulgaris) are legumes of the Fabaceae family consumed worldwide. In Spain, beans are the third most consumed legume species after chickpeas and lentils. Allergy to different legumes is very frequent in children and represents the fifth cause of food allergy.
Objective: Demonstrate a new phenotype in patients with green bean anaphylaxis.
Material and Methods: We report a 20-year-old woman who experienced anaphylaxis after consuming cooked green beans and required emergency treatment. There were no associated cofactors such as medications, alcohol, or physical exercise. After the episode, she tolerated well nuts, garlic, chickpeas, peas, and soy. Prick-prick with raw and cooked green bean, ISAC, SDS-PAGE and IgE-Western blot were performed.
Results: The prick+prick test with raw and cooked green beans was positive. The sodium dodecyl sulfate–polyacrylamide gel electrophoresis–immunoglobulin E (SDS-PAGE/IgE)–western blot analysis with white and red beans as well as cooked and raw green beans showed identification of several proteins with a molecular weight of 25–75 kDa in the extract of raw beans. Only one protein with a molecular weight of approximately 10 kDa was recognized in cooked beans.
Conclusion: We present a case of anaphylaxis induced by green beans (Phaseolus vulgaris) because of a 10-kDa protein and tolerance to other legumes, which suggests a new phenotype.
Key words: anaphylaxis, green beans, Phaseolus vulgaris, 10-kDa protein
*Corresponding author: Estela Menéndez-Rivero, Allergy Unit, Hospital Universitario Virgen del Rocío, Avenue Manuel Siurot, S/n, 41013 Seville, Spain. Email address: [email protected]
Received 11 July 2024; Accepted 25 September 2024; Available online 1 January 2025
Copyright: Menéndez-Rivero E, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Anaphylaxis is one of the most life-threatening allergic reactions. In Europe, the number of patients presenting to the emergency departments with this condition has increased; approximately one in 300 persons has experienced anaphylaxis at some time in their lives. Hypersensitivity to food and insect venom is the main cause of anaphylaxis, followed by drugs.1,2
White, red, and green beans (Phaseolus vulgaris), legumes of the Fabaceae family, are consumed globally. In Spain, beans are the third most consumed legume species after chickpeas and lentils. Allergy to different legumes is very frequent in children and represents the fifth cause3 of food allergy3 and manifests itself in different forms, such as angioedema by inhalation,4 local manifestations,5 and anaphylaxis.6 Cross-reactivity between beans is frequent, although not always relevant clinically.3,7
We present a case of anaphylaxis after consumption of cooked green beans (Phaseolus vulgaris) because of a 10-kDa molecular weight protein but tolerance to other legumes.
Case report
Our patient was a 20-year-old woman with a personal history of intermittent mild rhinoconjunctivitis because of sensitization to pollens with good evolution after 4 years of subcutaneous immunotherapy against olive and grass pollen. Years later of the previous diagnosis, she consulted for an episode that occurred a few minutes after consuming green beans cooked with garlic, and presented pruritus of the tongue and pharynx, chest and neck, generalized heat, and edema of the eyelids, lips, and tongue with obnubilation, pharyngeal tightness, and dyspnea. The patient recovered within a few hours after being treated in the emergency department with adrenaline, corticosteroids, and antihistamines.
There were no associated cofactors, such as medications, alcohol, or physical exercise and she had not consumed any other legumes in the hours prior to anaphylaxis. After the episode, she tolerated well all nuts, garlic, chickpeas, soybeans, lettuce, tomato, and other vegetables, but avoided red and green beans. Therefore, we banned red and green beans, both raw and cooked, from her food.
In addition, she was prescribed treatment, such as antihistamines, oral corticosteroid, and adrenaline, in case of inadvertent intake of potentially allergenic food. She was instructed regarding the usage and when to use adrenaline autoinjector. The patient refused to undergo oral challenge tests with other foods. In addition, she showed clinical manifestations only with the performed prick+prick test.
Skin prick tests (SPT) were performed with a battery of commercial aeroallergens (mites, fungi, pollens, and animal epithelium) (Roxall Lab., Bilbao, Spain); they were positive for Olea europaea, grass, and Platanus acerifolia pollens, horse, cat, and dog dander as well as Dermatophagoides pteronyssinus (house dust mites).
The prick+prick test with raw and cooked green beans was positive for 15- and 10-mm wheals, respectively. In addition, pruritic papules appeared on the thorax and upper extremities that disappeared in 2 h with antihistamines.
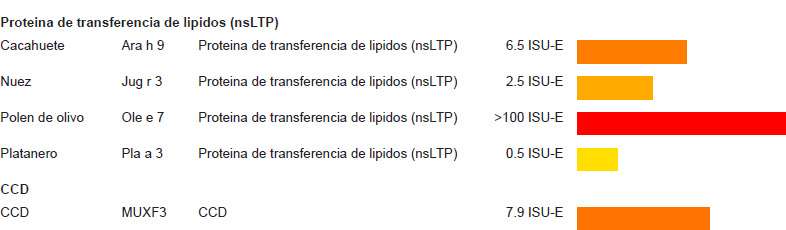
Specific immunoglobulin E (IgE) levels and molecular study were measured, and positive results were obtained for pollens, house dust mites, and horse, cat, and dog epithelium. The patient also tested positive for some lipid transporter proteins (LTPs) and cross-reactive carbohydrate determinants (CCDs) (Figure 1).
Figure 1 Molecular study for allergen-specific IgE (ImmunoCAP ISAC E112i®).
Protein extracts were prepared from white and red beans as well as cooked and raw green beans by grinding them in phosphate-buffered saline solution (PBS, 1/5 w/v) and incubating with magnetic stirring at 2–8°C for 16 h. Protein concentration was measured after centrifuging at 10,000 rpm for 10 min by using the Bio-Rad Protein Assay kit.4
Samples were analyzed by sodium dodecyl sulfate–polyacrylamide gel electrophoresis (SDS-PAGE) to determine protein profile. For western blot analysis, proteins were transferred to a nitrocellulose membrane, incubated overnight with patient serum, and treated with mouse anti-human IgE 1:2000 dilution for 1 h prior to visualization of bands by chemiluminescence.
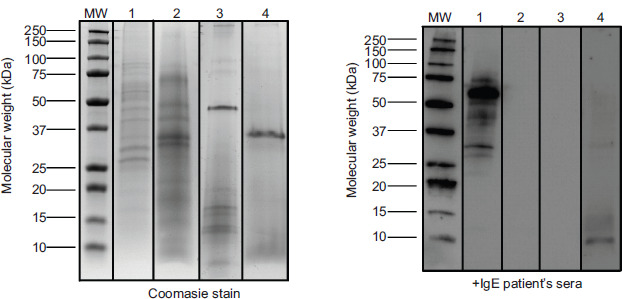
The SDS-PAGE/IgE–western blot analysis showed recognition of several proteins with a molecular weight of 25–75 kDa in the extract of raw beans. However, only one protein with a molecular weight of approximately 10 kDa was recognized in cooked beans. In contrast, there was no recognition by the patient’s IgE to white bean or red bean extracts, demonstrating that the patient was not sensitized (Figure 2).
Figure 2 SDS-PAGE/IgE–western blot analysis. Lane 1: raw green beans; lane 2: white beans; lane 3: red kidney beans; and lane 4: cooked green beans.
Discussion
Some of the bands recognized in our patient’s raw bean extract were described as a cause of allergy in cooked white and red beans (Phaseolus vulgaris),8 but they disappeared with cooking. The band of approximately 10 kDa molecular weight in cooked beans was probably the cause of anaphylaxis and coincided with molecular weight of an LTP as described previously by Pastorello et al.;9 the authors described it as responsible for asthma, gastrointestinal symptoms, and oral allergy syndrome (OAS) with consumption of peach, but no patient had anaphylaxis with green beans. Another difference in our case was that there was tolerance to peach.
The high levels of LTPs appearing with ImmunoCAP ISAC™ E112i®, Phadia, Thermo Fisher Scientific Uppsala, Sweden. and the absence of symptoms with peanuts and nuts indicated sensitization without clinical repercussions or cross-reactivity with pollen LTPs. Tolerance to other LTPs from different foods could be explained by different epitopes among LTPs present in pink fruits, nuts, and green beans as reported in our patient.10
Asero et al.11 described a 35-kDa protein found in cooked beans as a cause of anaphylaxis; however, this was not recognized in our patient in neither raw nor cooked beans.
Cross-reactivity between legumes is debatable. It has been demonstrated in children with white and red beans as well as several other legumes.3,8,9 However, cross-reactivity between legumes is not always relevant clinically.12 In our case, there was tolerance to other legumes, which could be explained because the patient’s 10-kDa protein matched with LTP and not with 7S and 11S globulins, the main protein fractions attributed to co-sensitization between legumes.12 The patient refused to undergo oral challenge tests with other foods. Therefore, we surmised that different phenotypes are present in legume allergy with different proteins involved.
Conclusion
We reported a case of anaphylaxis induced by green beans (Phaseolus vulgaris) because of a 10-kDa molecular weight protein and tolerance to other legumes, which suggested a new phenotype.
Author Contributions
E. Menéndez-Rivero and M. Prados-Castaño conceived of the presented idea. Both M.J. Martínez and F. Pineda de la Losa prepared and verified the extracts; analyzed the samples carring out the analysis contributed to the interpretation of the results. M. Prados-Castaño encouraged E. Menéndez-Rivero to investigate and supervised the findings of this work. All authors discussed the results and contributed to the final manuscript.
Conflict of Interest
The authors declared no potential conflict of interest with respect to research, authorship, and/or publication of this article.
Funding
Not applicable.
REFERENCES
1 Panesar SS, Javad S, de Silva D, Nwaru BI, Hickstein L, Muraro A, et al. The epidemiology of anaphylaxis in Europe: A systematic review. Allergy. 2013;68(11):1353–61. Epub 14 Oct 2013. 10.1111/all.12272
2 Bilò MB, Martini M, Tontini C, Corsi A, Antonicelli L. Anaphylaxis. Eur Ann Allergy Clin Immunol. 2021Jan;53(1): 4–17. Epub 7 Jan 2021. 10.23822/EurAnnACI.1764-1489.158
3 Ibáñez MD, Martínez M, Sánchez JJ, Fernández-Caldas E. Reactividad cruzada de las legumbres. Allergol et Immunopathol. 2003;31(3):151–61. 10.1016/S0301-0546(03)79283-0
4 Martínez Alonso JC, Callejo Melgosa JA, Fuentes Gonzalo MJ, Martín García C. Angioedema induced by inhalation of vapours from cooked white bean in a child. Allergolet Immunopathol (Madr). 2005;33(4):228–30. 10.1042/BST0330228
5 Cabanillas B, Jappe U, Novak N. Allergy to peanut, soybean, and other legumes: Recent advances in allergen characterization, stability to processing and IgE cross-reactivity. Mol Nutr Food Res. 2018;62(1)1-9. 10.1002/mnfr.201700446
6 Rougé P, Culerrier R, Thibau F, Didier A, Barre A. A case of severe anaphylaxis to kidney bean: Phaseolin (vicilin) and PHA (lectin) identified as putative allergens. Allergy. 2011;66:301–2. 10.1111/j.1398-9995.2010.02466.x
7 Pereira MJ, Belver MT, Pascual CY, Martín Esteban M. The allergenic significance of legumes. Allergol Immunopathol (Madr). 2002;30(6):346–53. 10.1016/s0301-0546(02)79152-0
8 Laiseca García J, Alonso Díaz de Durana MD, Gonzalez Bravo L, Pineda de la Losa F, Macías Iglesias J, Rosado A. Allergy to white kidney beans with cross-reactivity to red kidney beans: Report of 2 cases in children. J Investig Allergol Clin Immunol. 2023;33(2):141–2. 10.18176/jiaci.0818
9 Pastorello EA, Pravettoni V, Farioli L, Primavesi L, Scibilia J, Piantanida M, et al. Green bean (Phaseolus vulgaris): A new source of IgE-binding lipid transfer protein. J Agric Food Chem. 2010 Apr 14;58(7):4513–6. 10.1021/jf100213g
10 Asero R, Mistrello G, Roncarolo D, Amato S, Falagiani P. Why do lipid transfer protein-hypersensitive patients tolerate bean (and other legumes)? Int Arch Allergy Immunol. 2005;137:236–40. Epub 13 Jun 2005. 10.1159/000086336
11 Asero R, Mistrello G, Roncarolo D, Amato S, Van Ree L. String bean-induced anaphylaxis. Allergy. 2001;56(3):259–60. 10.1034/j.1398-9995.2001.056003259.
12 Smits M, Verhoeckx K, Knulst A, Welsing P, De Jong A, Gaspari M, et al. Co-sensitization between legumes is frequently seen, but variable and not always clinically relevant. Front Allergy. 2023;Mar16:4:1115022. eCollection 2023. 10.3389/falgy.2023.1115022