
Download
ORIGINAL ARTICLE
Changes in serum periostin levels in uncontrolled asthma in children (DADO phase 2 study)
Alicia Habernau Menaa,b*, Maria Angela Gonzalo Garijoc, Victoria Del Pozo Abejónd, Francisco Félix Rodríguez Vidigalb
aDepartment of Allergology, Hospital de Mérida, Badajoz, Spain
bDepartment of Biological Sciences, University of Extremadura, Spain
cDepartament of Allergy, Complejo Hospitalario Universitario de Badajoz, Spain
dDepartment of Immunology, IIS-Fundación Jiménez Díaz, Madrid, Spain
Abstract
Objective: Asthma is an inflammatory airway condition and the most common chronic disease in children. However, there is a lack of biological markers for asthma, especially in children. This study aimed to analyze the changes in periostin levels in children with uncontrolled asthma after 12 months of optimized management. The secondary objectives were to evaluate the changes in symptoms, exacerbations, and other biomarkers after 12 months of follow-up.
Methods: This was an observational, prospective study of children aged 5 to 14 with uncontrolled asthma who visited the Hospital Materno Infantil of Badajoz’s Allergy Unit between September 2015 and June 2016. At the first visit and after a 12-month follow-up, lung function, asthma control test (ACT/cACT), quality of life by PAQLQ (Paediatric Asthma Quality of Life Questionnaire), blood eosinophils, total and specific IgE, and serum periostin levels were assessed. Periostin levels were also analyzed in a control group.
Results: After the 12-month follow-up, the percentage of symptoms, the proportion of patients with FEV1 <80%, and the levels of blood eosinophils decreased, whereas ACT and PAQLQ increased. Children with uncontrolled asthma showed high serum periostin concentrations on their first visit (901.48 ng/ml), which decreased after 12 months (67.93 ng/ml) (p<0.001). In the control group, periostin levels were 56.12 ng/ml. The sensitivity and specificity of periostin were 77.8% and 54.8%, respectively, for the diagnosis of controlled and uncontrolled asthma.
Conclusion: Our study showed that periostin levels in children with uncontrolled asthma decreased with the correct treatment after asthma control.
Key words: asthma, biomarkers, children, eosinophils, periostin
*Corresponding author: Alicia Habernau Mena, Hospital de Mérida, Polígono Nueva Ciudad s/n. 06800 Badajoz, Spain. Email address: [email protected]
Received 23 May 2024; Accepted 4 September 2024; Available online 1 January 2025
Copyright: Habernau Mena A, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Asthma is the most common chronic disease in children and adolescents, representing a major health problem worldwide.1 The prevalence of childhood asthma in Europe is around 10% (ISAAC study), and a high percentage of patients are not well diagnosed or treated.2 Asthmatic children visit emergency departments and are hospitalized more often than adults with asthma (TENOR study).3
Although asthma is an inflammatory airway disease, few biological markers can easily measure such inflammation in routine clinical practice, especially in children.4 In this regard, periostin is a biomarker of type 2 (T2) airway inflammation in adults with asthma.5 This extracellular matrix protein is secreted by the airway epithelial and fibroblast cells in response to interleukins IL-13 and IL-5, and when interacting with integrins, periostin induces cell proliferation and regeneration; in fact, its main function is to repair the connective tissue; it is involved in airway inflammation, and has an immunomodulatory role.6 It has been demonstrated that serum levels of periostin measurement are reproducible with a small coefficient of variation.6 Several studies have shown that periostin levels in children with asthma are higher than in healthy children and usually higher in children than adults, probably due to bone and tooth turnover.7-10 In a previous study, we found periostin levels were very high in children with uncontrolled asthma (median of 901.48 ng/ml),11 much higher than those reported for children with controlled asthma.7-10 However, the variation in periostin levels with asthma control is still unknown. Therefore, this study aimed to analyze the changes in periostin levels in children with uncontrolled asthma after following optimized management for 12 months according to Clinical Practice Guidelines (CPGs). In addition, the secondary objectives were to evaluate changes in symptoms, exacerbations, and other biomarkers after one year of follow-up.
Methods
Study design and patients
Our work is an observational, prospective, single-center study. It included children with asthma who attended the Allergy Unit of the Materno Infantil Hospital in Badajoz between September 2015 and June 2016. Inclusion criteria were children aged between 5 and 14 years, diagnosed with uncontrolled asthma, and able to read and understand Spanish. Conversely, those suffering from cardiopulmonary diseases, active cancer, or severe psychiatric disorders were excluded. A detailed clinical history and lung function testing with spirometry and post-BD bronchodilator testing were used to diagnose asthma. In addition, asthma treatment was prescribed according to guidelines,12,13 and a written asthma action plan was provided. A minimum of 4 visits for each child over 12 months was included in the study protocol.
To assess periostin levels in children without asthma, we included a control group of 25 children aged 5-14 years from the same health district, treated in the same allergy unit, with no history of asthma or wheezing.
The Ethics Committee for Clinical Research (ECCR) approved the study of the Infanta Cristina University Hospital, Badajoz. All parents or legal representatives of children over 12 years provided written informed consent.
Variables and measurements
The subsequent variables were documented on Case Report Forms (CRFs). At the initial visit, the patient’s demographic and clinical characteristics were recorded, including age, sex, body mass index (BMI), time of symptom onset, comorbidities, treatment, number of exacerbations, emergency visits, and annual hospital admissions. Furthermore, all patients underwent spirometry and a bronchodilator test (post-bronchodilator [PostBD]), as well as skin prick testing, an asthma control test (ACT/cACT), and exhaled nitric oxide measurement (FeNO), in addition to the administration of the Paediatric Asthma Quality of Life Questionnaire (PAQLQ). At the final visit, the number of exacerbations, emergency visits, and annual hospital admissions, along with the treatment, spirometry (FEV1), FeNO, ACT/cACT, and PAQLQ, were recorded. Furthermore, a venous blood sample was obtained at the initial and final visits to measure blood eosinophils, total and specific IgE, and serum periostin. A serum sample was obtained in the control group to assess periostin levels.
A positive result was recorded for the PostBD test if there was an increase in FEV1 of >9-12% or >200 cc;14 and for the skin prick test with aeroallergens and food allergens (Roxall, Bilbao, Spain), a positive result was indicated by the presence of papules larger than 3 mm.15 The measurement of FeNO was conducted using the NIOX Vero® (Thermo-Fisher, Massachusetts, USA), with a cut-off point of 30 ppb. Total and specific IgE were measured by InmunoCAP (Thermo-Ficher, Massachusetts, USA), with positive specific IgE defined as > 0.35 kU/l. The threshold for blood eosinophilia was set at a count of > 300 eosinophils/mm3. Serum samples were stored at -20°C for measurement of periostin. The levels of serum periostin were quantified using the Enzyme-Linked Immunosorbent Assay (ELISA), specifically the R&D Systems Human Periostin DuoSet ELISA (Cat# DY3548), according to the instructions provided by the manufacturer. Given the markedly elevated periostin levels in the serum samples, diluting some of the sera to a 1/10 and 1/100 ratio was necessary to achieve a more accurate measurement. The level of asthma control was assessed using the ACT (Asthma Control Test) in children aged 12 years and older and the cACT (Childhood Asthma Control Test) in children below the age of 12. The self-administered PAQLQ (Pediatric Asthma Quality of Life Questionnaire) evaluated the quality of life. The severity and control of asthma were assessed based on the patient’s medical history and the results of additional tests. An asthma exacerbation was defined as symptoms that necessitate an increased dose of inhaled corticosteroids or systemic corticosteroids. Additionally, all parents or legal representatives completed a questionnaire that collected several demographic and psychological factors, home characteristics, exposure to cigarette smoke, and personal and family medical history.
Statistics
Categorical variables are presented as frequencies and proportions, while continuous variables are presented with central tendency and dispersion measures: mean and SD, median and 25 and 75 percent, and extremes.
Contingency tables and the chi-square or Fisher’s exact test assessed the relationship between two categorical variables. The McNemar test for paired data was used to compare earlier and later outcomes. T-test, ANOVA, or the non-parametric tests Wilcoxon or Kruskal-Wallis test were used to assess the relationship between a continuous and a categorical variable. A T-test or Wilcoxon test on paired data was used to compare the results of the first and last visits. Pearson or Spearman correlations assessed the relationship between two numerical variables. The significance level for all tests was set at a bilateral alpha value of 0.05. Receiver operating characteristic (ROC) curves were plotted to analyze the usefulness of serum periostin and blood eosinophil levels for the diagnosis of asthma and to provide optimal cut-off values. All statistical analyses were performed using SAS® version 9.4.
Results
Patient characteristics
A total of 50 children with asthma and 25 children without asthma (control group) were included in the study. Table 1 summarizes the baseline characteristics of patients with uncontrolled asthma. Most of them were males, had started asthma symptoms during the first year of life, and were sensitized to aeroallergens. In addition, almost all patients presented with rhinitis, and more than half of them with atopic dermatitis. Moreover, many patients had exacerbations and limitations in daily life. Regarding the control group, the median (IQR) age was 8.9 (3.1) years, 14 (56.0%) children were males, and 9 (36.0%) presented with mild allergic rhinoconjunctivitis and/or atopic dermatitis.
Table 1 Baseline characteristics of patients with uncontrolled asthma.
| Sociodemographic | |
|---|---|
| Age (years), median (II) | 9.3 (3.5) |
| Males, n (%) | 36 (72.0) |
| Exposure to cigarette smoke, n (%) | 18 (36.0) |
| Clinical | |
| BMI (kg/m2), median (II) | 19.4 (4.2) |
| Onset of symptoms, n (%) | |
| The first year of life | 32 (64.0) |
| Preschool | 13 (26.0) |
| School | 5 (10.0) |
| Sensitization to aeroallergens, n (%) | 41 (82.0) |
| Pollen | 35 (70.0) |
| Mites | 25 (50.0) |
| Fungi | 20 (40.0) |
| Comorbidities, n (%) | |
| Rhinitis | 48 (96.0) |
| Overweight | 9 (18.0) |
| Food allergies | 16 (32.0) |
| Atopic dermatitis | 31 (62.0) |
| Biomarkers | |
| Total IgE (IU/ml), mean (SD) | 536 (682.0) |
| IgE >500 IU/ml, n (%) | 16 (32.0) |
| FENO >20 ppb, n (%) (n=41) | 28 (68.3) |
| Blood eosinophils >300/mcL, n (%) | 38 (76.0) |
Unless otherwise specified, the assessment corresponds to N=50. BMI: body mass index; FENO: fraction exhaled nitric oxide.
Changes in symptoms and lung function
After 12 months of follow-up and appropriate management and treatment, the frequencies of diurnal and nocturnal symptoms and limitations in daily living decreased by more than 50%, and constraints in sports activities decreased by 30%. Moreover, the children needed less school absenteeism, emergency assistance, and hospital admission. As for lung function, we also observed a decrease in the proportion of patients with an FEV1 <80% (on the first visit, 22% of children presented FEV1 <80% and only 6.1% of children on the last visit) (Table 2).
Table 2 Changes in symptoms, lung function, biomarkers, and asthma control and treatment between the first and the last visit. The McNemar test was used.
| First visit (N=50) |
Last visit (N=49) |
P value | |
|---|---|---|---|
| Clinical data, n (%) | |||
| Nocturnal symptoms | 49 (98.0) | 20 (40.8) | <0.0001 |
| Daily symptoms | 46 (92.0) | 18 (36.7) | <0.0001 |
| Limitations in daily activities | 36 (72.0) | 10 (20.4) | <0.0001 |
| Limitations in sports activity | 46 (92.0) | 30 (61.2) | 0.0006 |
| School absenteeism | 38 (76.0) | 18 (36.7) | <0.0001 |
| Parental absenteeism | 25 (50.0) | 4 (8.3) | <0.0001 |
| A&E visit | 44 (88.0) | 15 (30.6) | <0.0001 |
| Hospital admissions | 19 (38.0) | 2 (4.0) | <0.0001 |
| Lung function | |||
| FEV1, n (%) | |||
| >80% | 39 (78.0) | 46 (93.9) | 0.0460 |
| 80-70% | 7 (14.0) | 2 (4.1) | |
| <70% | 4 (8.0) | 1 (2.0) | |
| Biomarkers | |||
| Blood eosinophils (>300 eos/mm3), n (%) | 38 (76.0) | 20 (47.0) | 0.0076 |
| Periostin (ng/ml), mean (SD) | 901.48 (700.74) | 67.93 (27.47) | <0.0001 |
| Measuring tools | |||
| ACT/cACT score, n (%) | |||
| >19 | 14 (28.6)a | 33 (67.3) | <0.0001 |
| 14-19 | 19 (38.8)a | 15 (30.6) | |
| <14 | 16 (32.7)a | 1 (2.0%) | |
| PAQLQ score, mean (SD) | 4.3 (1.3) | 5.75 (0.88) | <0.0001 |
| Asthma control, n (%) | |||
| Uncontrolled asthma | 49 (98.0) | 13 (26.5) | <0.0001 |
| UcSA | 19 (38.0) | 3 (6.1) | |
| UcMA | 22 (44.0) | 5 (10.2) | |
| UcEA | 8 (16.0) | 5 (10.2) | |
| Treatment, n (%) | |||
| OC | 40/49 (81.6%) | 12 (24.5%) | <0.0001 |
| LABA + ICs | 19 (38.0%) | 46 (93.9%) | <0.0001 |
aN assessed: 49.
A&E: Accident and Emergency, ACT: Asthma Control Test, C-ACT: Children Asthma Control Test, FEV1: Forced expiratory volume, ICs: inhaled corticosteroids, LABA: Long acting beta agonist, OC: oral corticosteroids, PAQLQ: Pediatric Asthma Quality of Life Questionnaire, UcEA: Uncontrolled episodic asthma, UcMA: Uncontrolled moderated asthma, UcSA: Uncontrolled severe asthma.
Changes in severity and asthma control
In the last visit, 75% of asthmatic children had achieved disease control, and there were significant increases in PQLQ and ACT/cACT scores. In addition, the percentage of patients who used oral corticosteroids (OCs) significantly decreased, and the number of with inhaled corticosteroids (ICs) increased (Table 2).
Changes in biomarkers
Patients with uncontrolled asthma showed high periostin concentrations on their first visit. However, after 12 months, they experienced a more than 90% decrease in periostin levels (Table 2). Periostin levels increased with patients’ age, showing a moderate correlation (Spearman’s rho -0.). Additionally, on the first visit, most patients had more than 300 eosinophils/L in their blood. In contrast, on the last visit, less than half of the children (Table 2) had eosinophils > 300/mL. No correlation was found between serum periostin and total IgE levels, blood eosinophils, and FeNO values.
In the control group, the serum periostin average was 56.12 ng/ml, lower than in the case group (p<0.01) on the last visit, and there was no difference between atopic and non-atopic children.
Specificity and sensitivity of biomarkers
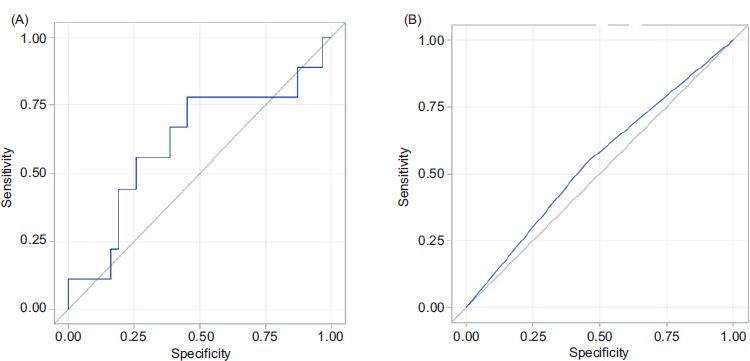
The area under the ROC curve (AUC) was 0.62 for serum periostin (Figure 1), and the optimal cut-off level for diagnosis of controlled and uncontrolled asthma was 64.5 ng/dL, which had a sensitivity of 77.8% and a specificity of 54.8% (95% CI). The area under the ROC curve (AUC) was 0.55 for blood eosinophils, and the cut-off level of 300 eosinophils/mcL in blood for diagnosis of controlled and uncontrolled asthma had a sensitivity of 53.8% and a specificity of 55.2% (95% CI).
Figure 1 (A) Periostinlevels and uncontrolled asthma. Area under ROC curve = 0.619. (B) Area under the ROC curve for blood eosinophils. Area under ROC curve = 0.5451.
Discussion
In this study analyzing the variation of periostin levels after a 12-month follow-up in children with uncontrolled asthma, we found that the percentage of symptoms and limitations decreased; lung function, control asthma, and quality of life increased; and serum periostin levels and blood eosinophils decreased. In addition, the sensitivity and specificity of periostin were greater than blood eosinophils for the diagnosis of controlled and uncontrolled asthma.
Our study group presented many symptoms, daily life limitations, and frequent emergency assistance and hospitalizations on the first visit. After adequate treatment and follow-up, we noticed a significant improvement in symptomatology and limitations both in daily life and in sports practice, on the one hand, and a decrease in the number of exacerbations, emergency assistance, and hospital admissions on the other. The following visits took place in different seasons to evaluate symptom variability over time and seasonal weather impact. The measurement of asthma control by the ACT and the quality of life (PQLQ) improved significantly throughout the study. At the beginning of the study, most children had an appropriate treatment according to the GPCs, and only one-third were treated with a combination of ICs and LABA. However, at the end of the study, we observed an increase in the percentage of children treated with LABA associated with ICs and a significant decrease in the percentage of children who required OC. It has been shown that the association of ICs and LABA reduces the number of exacerbations in patients with uncontrolled asthma treated only with ICs.12
In the study group, the presence of atopy and aeroallergen sensitization and high levels of total IgE, FeNO, blood eosinophilia, and periostin were noteworthy. Our main finding was the very high levels of serum periostin in children with uncontrolled asthma and inadequate treatment and their significant decrease after one year of follow-up and treatment according to the CPGs. Therefore, we think periostin levels could be higher in stages of chronic airway inflammation and decrease following adequate treatment. In our study, children with poorly controlled asthma had higher periostin levels (median 939.5 (901.48) ng/ml) than those previously reported (median 76 ng/ml,8 134 ng/ml,20 90 ng/ml21). Those publications may explain this difference, including patients with mild-moderate controlled asthma who received the correct treatment. In contrast, the children in our study were patients with uncontrolled moderate-severe asthma, and approximately 50% of children were not treated according to the GPC. However, the values of periostin in our control group (56.12 ng/ml) and our patients, once they achieved control (67.93 ng/ml), were similar to those published.7,8
Interestingly, within the study group, we identified two 6-year-old girls with severe early-onset uncontrolled asthma, low levels of total IgE serum, no sensitization to allergens, poor response to corticosteroids, poor evolution, and low serum periostin levels on the first and the last visit. We suspect this phenotype is not mediated by Th2 cells, whereas a paucigranulocytic or neutrophilic pattern could be possible. Studies in animal models show that a deficit of periostin leads to the loss of the ability to repair connective tissue, a decrease in the diameter of collagen fibers and elasticity decline, and neutrophilic inflammation.19
There are no valid biomarkers with established clinical value in children capable of monitoring disease progression, predicting the risk of exacerbations, or evaluating response to therapy. Blood eosinophils are related to disease severity in pediatric asthma but are not useful as a single biomarker.22 In our study, blood eosinophils decreased significantly after achieving asthma control but presented low sensitivity (53.8%) and specificity (55.2%) for asthma diagnosis. FENO could identify some phenotypes in children and confirm a good response to therapy with ICs.16,22 Eosinophils and neutrophils in sputum have low reproducibility in children,23 and bronchoalveolar lavage is not commonly used in children. Therefore, there is a need for a marker of airway inflammation related to the disease’s activity and the risk of exacerbation. Inoue et al.21 demonstrated that serum periostin was comparable with FENO or peripheral blood eosinophilia as a biomarker for diagnosing pediatric asthma (sensitivity and specificity of 75% and 59.3%, respectively). We found similar results for serum periostin (sensitivity 77.8% and specificity 54.8%), with a cut-off level for controlled and uncontrolled asthma diagnosis of 64.5 ng/dL. Some authors suggest that serum periostin could be an easily obtainable Th2 biomarker better than FENO or eosinophilia22 and that serum periostin alone or in combination with other biomarkers, such as eosinophil count and FENO could be useful to identify the risk of asthma exacerbations.24-26 Kato et al.27 found an association between higher serum periostin levels and poor asthma control after the reduction of ICs and proposed periostin as a possible predictive biomarker. Other studies have shown that corticosteroids28,29 and omalizumab30 are more effective in asthmatic adults with elevated periostin. Still, we do not know if these results could be extrapolated to the pediatric population. Several groups have recently reported an association between serum periostin levels and asthma severity in children31 and poor asthma control in adolescents.32
This study has some limitations. First, we could not determine FENO at the end of the follow-up, and, therefore, there are no data on FENO changes related to the clinical evolution of patients nor results of the possible relationship between FENO and other biomarkers. In addition, we could not assess the severity of the relationship between periostin and asthma. However, to our knowledge, this is the first study about periostin in children with uncontrolled asthma and the first that analyzed the changes in blood periostin levels in asthma control. Moreover, the cut-off point of periostin levels is not defined in children, and we do not know the variation in age or race. Moreover, periostin levels can change when children and adolescents grow and with other diseases, such as atopic dermatitis or upper airway infections.
Conclusions
In conclusion, our study showed that children with uncontrolled asthma experienced a decrease in serum periostin levels once asthma was controlled with proper treatment. Although the role of this protein as an asthma biomarker is currently under investigation, our results support the value of using serum periostin levels to study asthma phenotypes and assess the control of the disease and its response to treatment in childhood asthma. Future studies should consider other variables related to periostin levels, such as asthma severity, exacerbations, and ICS dose.
Acknowledgments
The authors thank i2e3 Biomedical Research Institute for providing medical writing assistance on behalf of Allergy Therapeutics (BEC-AT), Elizabeth Juniper (McMaster University Medical Centre Hamilton, Ontario, Canada) for authorizing the use of the PAQLQ and PACQLQ, and LetiPharma for statistical support and review the article.
Author Contributions
All authors contributed equally to this manuscript.
Conflict of Interest
The authors declare that they have no conflict of interest.
Funding
This research article has not had any financial funding.
REFERENCES
1 Levy ML, Bacharier LB, Bateman E, Boulet LP, Brightling C, Buhl R, Brusselle G, Cruz AA, et al. Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Prim Care Respir Med. 2023;33(1):7. 10.1038/s41533-023-00330-1
2 Urrutia I, Aguirre U, Sunyer J, Plana E, Muniozguren N, Martínez-Moratalla J, et al. Estudio de Salud Respiratoria de la Comunidad Europea. Cambios en la prevalencia de asma en la población española del Estudio de Salud Respiratoria de la Comunidad Europea (ECRHS-II) [Changes in the prevalence of asthma in the Spanish cohort of the European Community Respiratory Health Survey (ECRHS-II)]. Arch Bronconeumol. 2007;43(8):425–30. Spanish. https://doi.org/10.1016/s1579-2129(07)60098-6. Erratum In: Arch Bronconeumol. 2007 Oct;43(10):589.
3 Chipps BE, Haselkorn T, Rosén K, Mink DR, Trzaskoma BL, Luskin AT. Asthma exacerbations and triggers in children in tenor: impact on quality of life. J Allergy Clin Immunol Pract. 2018;6(1):169–76.e2. 10.1016/j.jaip.2017.05.027
4 Sánchez-García S, Habernau Mena A, Quirce S. Biomarkers in inflammometry pediatric asthma: utility in daily clinical practice. Eur Clin Respir J. 2017;4(1):1356160. 10.1080/20018525.2017.1356160
5 Matsumoto H. Serum periostin: a novel biomarker for asthma management. Allergol Int. 2014;63(2):153–60. 10.2332/allergolint.13-RAI-0678
6 Takayama G, Arima K, Kanaji T, Toda S, Tanaka H, Shoji S, McKenzie AN, et al. Periostin: a novel component of subepithelial fibrosis of bronchial asthma downstream of IL-4 and IL-13 signals. J Allergy Clin Immunol. 2006;118(1):98–104. 10.1016/j.jaci.2006.02.046
7 Anderson HM, Lemanske RF Jr, Arron JR, Holweg CTJ, Rajamanickam V, Gangnon RE, Gern JE, et al. Relationships among aeroallergen sensitization, peripheral blood eosinophils, and periostin in pediatric asthma development. J Allergy Clin Immunol. 2017;139(3):790–796. 10.1016/j.jaci.2016.05.033
8 Lopez-Guisa JM, Powers C, File D, Cochrane E, Jimenez N, Debley JS. Airway epithelial cells from asthmatic children differentially express pro-remodeling factors. J Allergy Clin Immunol. 2012;129(4):990–7.e6. 10.1016/j.jaci.2011.11.035
9 Song JS, You JS, Jeong SI, Yang S, Hwang IT, Im YG, Baek HS, et al. Serum periostin levels correlate with airway hyper-responsiveness to methacholine and mannitol in children with asthma. Allergy. 2015 Jun;70(6):674–81. 10.1111/all.12599
10 Inoue Y, Izuhara K, Ohta S, Ono J, Shimojo N. No increase in the serum periostin level is detected in elementary school-age children with allergic diseases. Allergol Int. 2015 Jul;64(3):289–90. 10.1016/j.alit.2015.04.001
11 Habernau MA, Del Pozo AV, Rodríguez VFF, Bobadilla GP. Role of Periostin in Uncontrolled Asthma in Children (DADO study). J Investig Allergol Clin Immunol. 2017; 27(5):291–98. 10.18176/jiaci.0144
12 Plaza V, Alobid I, Alvarez C, Blanco M, Ferreira J, García G, Gómez-Outes A, et al. Spanish Asthma Management Guidelines (GEMA) VERSION 5.1. Highlights and Controversies. Arch Bronconeumol. 2022 Feb 58(2):150–58. English, Spanish. 10.1016/j.arbres.2021.05.010
13 Chung KF, Wenzel SE, Brozek JL, Bush A, Castro M, Sterk PJ, Adcock IM, et al. International ERS/ATS guidelines on defining, evaluating, and treating severe asthma. Eur Respir J. 2014 Feb;43(2):343–73. 10.1183/09031936.00202013. Epub 2013 Dec Erratum In: Eur Respir J. 2014 Apr;43(4):1216. Dosage error in article text. Erratum in: Eur Respir J. 2018 Jul 27;52(1): Erratum in: Eur Respir J. 2022 Jun 9;59(6): PMid: 24337046.
14 Dundas I, Chan EY, Bridge PD, McKenzie SA. Diagnostic accuracy of bronchodilator responsiveness in wheezy children. Thorax. 2005 Jan;60(1):13–6. 10.1136/thx.2004.029934. PMid: 15618576; PMCID: PMC1747153.
15 Pastorello EA. Skin test for diagnosis of IgE mediated allergy. Allergy 1993; 48:57–62. 10.1111/j.1398-9995.1993.tb04758.x
16 Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO, Olin AC, et al. American Thoracic Society Committee on Interpretation of Exhaled Nitric Oxide Levels (FENO) for Clinical Applications. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011 Sep 1;184(5):602–15. 10.1164/rccm.9120-11ST
17 Liu AH, Zeiger RS, Sorkness CA, Ostrom NK, Chipps BE, Rosa K, Watson ME, et al. The Childhood Asthma Control Test: retrospective determination and clinical validation of a cut point to identify children with poorly controlled asthma. J Allergy Clin Immunol. 2010 Aug;126(2):267–73, 273.e1. 10.1016/j.jaci.2010.05.031
18 Juniper EF, Guyatt GH, Feeny DH, Ferrie PJ, Griffith LE, Townsend M. Measuring quality of life in children with asthma. Qual Life Res. 1996 Feb;5(1):35–46. 10.1007/BF00435967
19 Ontsuka K, Kotobuki Y, Shiraishi H, Serada S, Ohta S, Tanemura A, Yang L, et al. Periostin, a matricellular protein, accelerates cutaneous wound repair by activating dermal fibroblasts. Exp Dermatol. 2012 May;21(5):331–36. 10.1111/j.1600-0625.2012.01454.x
20 Konradsen JR, Skantz E, Nordlund B, Lidegran M, James A, Ono J, Ohta S, et al. Predicting asthma morbidity in children using proposed markers of Th2-type inflammation. Pediatr Allergy Immunol. 2015 Dec;26(8):772–79. 10.1111/pai.12457
21 Inoue T, Akashi K, Watanabe M, Ikeda Y, Ashizuka S, Motoki T, Suzuki R, et al. Periostin as a biomarker for the diagnosis of pediatric asthma. Pediatr Allergy Immunol. 2016 Aug;27(5):521–26. 10.1111/pai.12575
22 Silkoff PE, Laviolette M, Singh D, FitzGerald JM, Kelsen S, Backer V, et al. ADEPT Investigators. Longitudinal stability of asthma characteristics and biomarkers from the Airways Disease Endotyping for Personalized Therapeutics (ADEPT) study. Respir Res. 2016 Apr 23; 17:43. 10.1186/s12931-016-0360-5
23 Fleming L, Tsartsali L, Wilson N, Regamey N, Bush A. Sputum inflammatory phenotypes are not stable in children with asthma. Thorax. 2012 Aug;67(8):675–81. 10.1136/thoraxjnl-2011-201064
24 Nagasaki T, Matsumoto H, Izuhara K, KiHAC Respiratory Medicine Group. Utility of serum periostin in combination with exhaled nitric oxide in the management of asthma. Allergol Int. 2017 Jul;66(3):404–10. 10.1016/j.alit.2017.02.003
25 Heaney LG, Djukanovic R, Woodcock A, Walker S, Matthews JG, Pavord ID, Bradding P, et al. Research in progress: Medical Research Council United Kingdom Refractory Asthma Stratification Programme (RASP-UK). Thorax. 2016 Feb;71(2):187–89. 10.1136/thoraxjnl-2015-207326
26 Scichilone N, Crimi C, Benfante A, Battaglia S, Iemmolo M, Spatafora M, Crimi N. Higher serum levels of periostin and the risk of exacerbations in moderate asthmatics. Asthma Res Pract. 2016 Jan 4;2:1. 10.1186/s40733-015-0019-x
27 Kato G, Takahashi K, Izuhara K, Komiya K, Kimura S, Hayashi S. Markers that can Reflect Asthmatic Activity before and after Reduction of Inhaled Corticosteroids: A Pilot Study. Biomark Insights. 2013 Aug 4;8:97–105. 10.4137/BMI.S12537
28 Woodruff PG, Modrek B, Choy DF, Jia G, Abbas AR, Ellwanger A, Koth LL, et al. T-helper type 2-driven inflammation defines major subphenotypes of asthma. Am J Respir Crit Care Med. 2009 Sep 1;180(5):388–95. 10.1164/rccm.200903-0392OC. Epub 2009 May 29. Erratum In: Am J Respir Crit Care Med. 2009 Oct 15;180(8):796. PMid: 19483109; PMCID: PMC2742757.
29 Berry M, Morgan A, Shaw DE, Parker D, Green R, Brightling C, Bradding P, et al. Pathological features and inhaled corticosteroid response of eosinophilic and non-eosinophilic asthma. Thorax. 2007 Dec;62(12):1043–9. 10.1136/thx.2006.073429
30 Tajiri T, Matsumoto H, Gon Y, Ito R, Hashimoto S, Izuhara K, Suzukawa M, et al. Utility of serum periostin and free IgE levels in evaluating responsiveness to omalizumab in patients with severe asthma. Allergy. 2016 Oct;71(10):1472–79. 10.1111/all.12922
31 Yavuz ST, Bagci S, Bolat A, Akin O, Ganschow R. Association of serum periostin levels with clinical features in children with asthma. Pediatr Allergy Immunol. 2021 Jul;32(5):937–44. 10.1111/pai.13444
32 Choudhary S, Kumar P, Banerjee M, Singh K, Goyal JP. Relationship of Serum Periostin with Asthma Control in Children: Single Center Experience. Indian Pediatr. 2023 Oct 15;60(10):822–25. Epub 2023 May 30. PMid: 37260069. 10.1007/s13312-023-3012-0