
Download
ORIGINAL ARTICLE
Role of serum-specific immunoglobulin E in egg allergy: a comprehensive study of Portuguese pediatric patients
Pedro Simão Coelhoa,b*, Gonçalo Martins dos Santosa,b, Inês Sangalhoa,b, Sónia Rosaa,b, Paula Leiria Pintoa,c
aServiço de Imunoalergologia, Centro Hospitalar Universitário de Lisboa Central, Lisboa, Portugal
bCentro Clìnico Académico de Lisboa, Lisboa, Portugal
cComprehensive Health Research Center (CHRC), NOVA Medical School, Universidade Nova de Lisboa, Lisboa, Portugal
Abstract
Introduction: Food allergies represent a growing public health concern, particularly among children. This study aims to examine egg allergy in pediatric patients and analyze the value of serum-specific immunoglobulin E (sIgE) levels as predictive biomarkers for oral food challenge (OFC) outcomes.
Methods: Retrospective study, involving pediatric patients with suspected IgE-mediated egg allergy, conducted at a tertiary hospital.
Results: Data from 176 pediatric patients were analyzed, revealing a higher male prevalence (59.1%). Most cases (40.3%) presented symptoms in the first year of life, predominantly mucocutaneous symptoms (46%). OFC results varied across various forms of egg presentation, with cooked egg being the most frequently tested food. Positive OFCs were observed in 14.6% (n = 36) of cases. The study identified specific egg protein biomarkers for positive OFC, with ovalbumin for raw egg (sIgE > 1.28 KUA/L; area under the curve [AUC] = 0.917; sensitivity [S] 100%; and specificity [Sp] 92%), ovomucoid for cooked egg (sIgE > 0.99 KUA/L; AUC = 0.788, 95%; S: 79%; and Sp: 74%), and ovomucoid for baked egg (sIgE> 4.63 KUA/L; AUC = 0.870; S: 80%; and Sp: 85%) showing predictive capacities.
Conclusions: The findings underscore the importance of considering various forms of egg presentation in the diagnosis and management of egg allergy. The findings highlight the valuable discriminatory capacity and provided reliable biomarkers, such as ovalbumin for raw egg and ovomucoid for cooked and baked egg in risk assessment, aiding in predicting OFC outcomes and helping clinicians to make informed decisions in diagnosing and managing egg allergies, thus improving patient care and quality of life.
Key words: biomarker, egg allergy, immunoglobulin E, ovalbumin, ovomucoid, pediatric food allergy
*Corresponding author: Pedro Simão Coelho, Rua Jacinta Marto, 8A, 1169-045, Lisboa. Email address: [email protected]
Received 11 December 2023; Accepted 14 March 2024; Available online 1 May 2024
Copyright: Coelho PS, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Allergies are symptomatic overreactions by the immune system to otherwise harmless substances, known as allergens.1 Food allergies are common in children, particularly those allergic to cow's milk and hen's egg, and have become a growing public health concern in developed countries.2–4
Allergic reactions to food proteins are a common cause of life-threatening reactions in pediatric allergic patients and could persist throughout life.5 Food-allergic patients often worry about unintentional exposures and their consequences, especially anaphylaxis, facing multiple dietary and psychosocial restrictions.3
Eggs are a fundamental food of human diet, and together with cow’s milk, they are the most common food allergens in children.6 Prevalence of egg allergy ranges between 0.5% and 8.9% of the pediatric population.7 Although most children outgrow their egg allergy, it is crucial to accurately diagnose and manage the condition to prevent severe allergic reactions.7 Understanding the natural history of egg allergy is crucial for planning the next steps in management, whether it involves avoiding eggs entirely or considering the introduction of baked egg, which is less allergenic.3
Oral food challenge (OFC) is the gold standard for confirming the diagnosis and assessing tolerance to egg; however, OFC is not without risk.7 The role of serum-specific IgE (sIgE) in the pathogenesis of egg allergy is well-documented.8 As a widely utilized in vitro test, it has demonstrated efficacy in evaluating potential egg allergic patients and predicting clinical reactions during OFCs, with reduced exposure risks.8 However, different studies report variable optimal serum sIgE cut-offs.7,9–15 Identifying predictive biomarkers for OFC outcomes can aid in risk stratification and clinical decision-making.
This study aimed to investigate the characteristics of egg allergy in a cohort of pediatric patients and evaluate the predictive ability of serum sIgE levels as biomarkers for OFC outcomes.
Methods
Study design and participants
A single center retrospective study was conducted in the Allergy and Clinical Immunology Department of a tertiary hospital in Lisbon, Portugal.
All pediatric patients with suspected IgE-mediated egg allergy and on an egg eviction diet, who underwent OFC with hen egg between January 2017 and June 2023, and had available serum sIgE for egg allergens in 12 months prior to OFC, were included in the study. The clinical suspicion of egg allergy was established based on clinical history by consulting medical records and laboratory findings. Exclusion criteria were an inconclusive OFC or a non-IgE-mediated egg allergy.
This study was granted approval by the Central Ethics Committee of Centro Hospitalar Universitário de Lisboa.
Variables
Demographic characteristics, medical history, age at the time of OFC, time between serum sIgE measurement and OFC, total IgE, serum sIgE levels of egg white, egg yolk, ovalbumin, and ovomucoid (measured by standardized immunoenzymatic assay, ImmunoCAP), and OFC outcome were analyzed.
Oral food challenges were conducted as graded open challenges after obtaining written informed consent from legal guardians. OFCs were conducted by trained physicians, with raw egg, cooked egg, cooked egg yolk, or baked egg. OFCs were considered positive if objective symptoms were observed within 2 h of intake of egg.16 Anaphylaxis was classified according to the definition of the World Allergy Organization.17 According to OFC results, patients were divided in two groups (“Negative” OFC group vs “Positive” OFC group).
Statistical analysis
Categorical data were presented as frequencies and continuous variables as median, 25th percentile (P25), and 75th percentile (P75). Chi-square and Fisher’s tests were used to evaluate the association between categorical variables, and Mann–Whitney U test was used to evaluate association between categorical and continuous variables. Receiver operating characteristic (ROC) curves were generated to evaluate the diagnostic accuracy of identified biomarkers, serving as a metric for assessing a diagnostic test's ability to discriminate between classes. The area under the curve (AUC) reflects the performance in distinguishing between true positives and false positives, with values >0.7 considered acceptable. The Youden Index (the maximum potential effectiveness of a biomarker, J), derived from the ROC curve, aids in identifying the optimal cut-off value for a diagnostic test, signifying the best compromise between sensitivity and specificity, and thereby enhancing diagnostic accuracy. The level of significance considered was α = 0.05. All statistical analyses were performed using IBM SPSS Statistics version 28.
Results
Of 202 patients, 176 were enrolled in the study, out of which 30.7% (n = 54) underwent more than one OFC. Population characterization is presented on Table 1.
Table 1: Baseline characteristics of participants (n = 176).
| Patients (%) | |
|---|---|
| Males | 104 (59.1%) |
| Age at 1st episode (IQR) years | 0 (1) |
| 1st episode manifestations | |
| Mucocutaneous | 81 (46%) |
| Gastrointestinal | 19 (10.8%) |
| Anaphylaxis | 25 (14.2%) |
| Asymptomatic sensitization | 15 (8.5%) |
| No data | 36 (20.5%) |
| Personal history | |
| Respiratory allergy | 91 (51.7%) |
| Atopic dermatitis | 64 (36.4%) |
| Other food allergy | 70 (39.8%) |
| No atopic comorbidity | 34 (19.3%) |
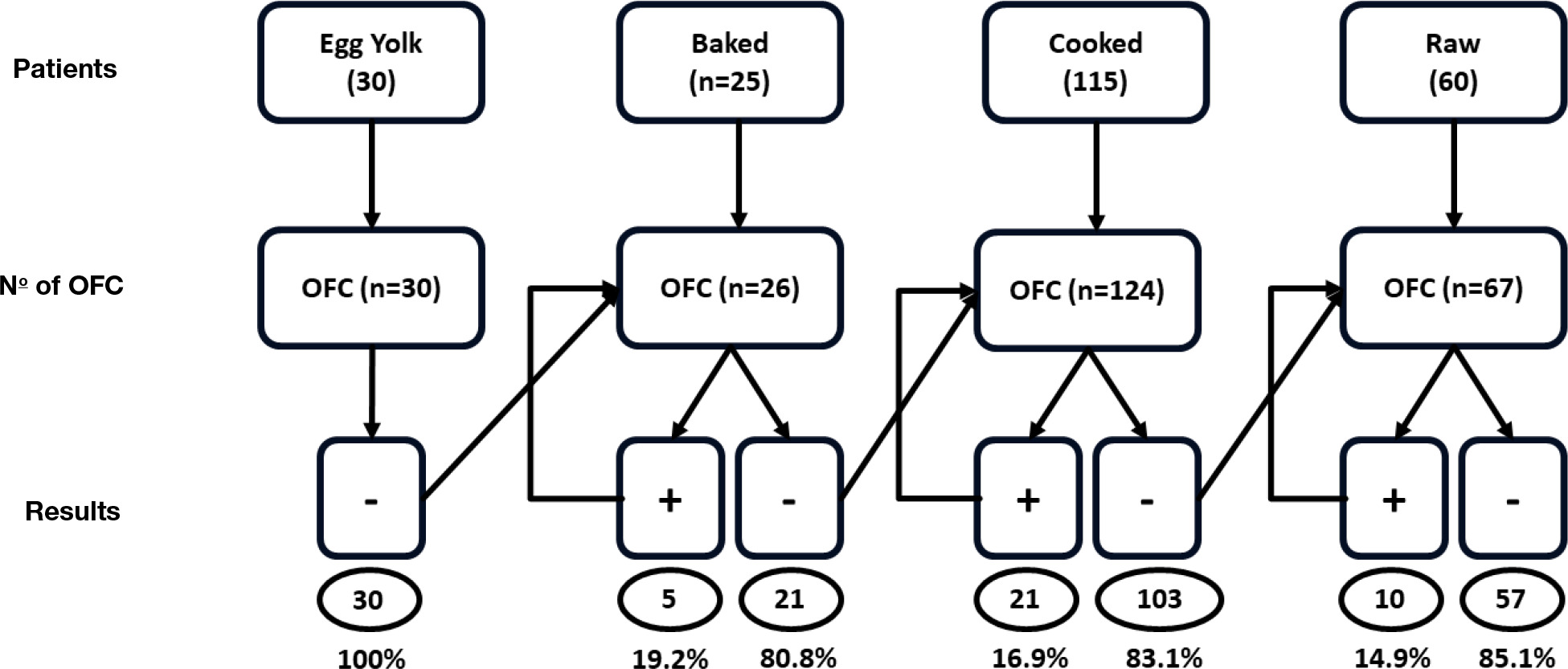
In all, 247 OFCs were conducted (Figure 1). Among these, 50.2% (n = 124) involved cooked egg, 27.1% (n = 67) raw egg, 12.1% (n = 30) cooked egg yolk, and 10.5% (n = 26) baked egg. The results showed that 14.6% (n = 36) of the OFCs yielded positive outcomes, without statistically significant differences among them, except for the cooked egg yolk group, where no positive OFC was observed. Among the patients sensitized to egg proteins, who had never experienced symptoms upon egg consumption, but were on egg eviction diet (n = 15), one patient (6.7%) exhibited a positive OFC to cooked egg. The remaining patients had negative OFCs with raw egg (n = 6, 40%), cooked egg (n = 4, 26.7%), cooked egg yolk (n = 3, 20%), and baked egg (n = 1, 6.7%).
Figure 1: Diagram of oral food challenges (OFC) performed (n = 247) and respective results (there were patients that underwent more than one OFC).
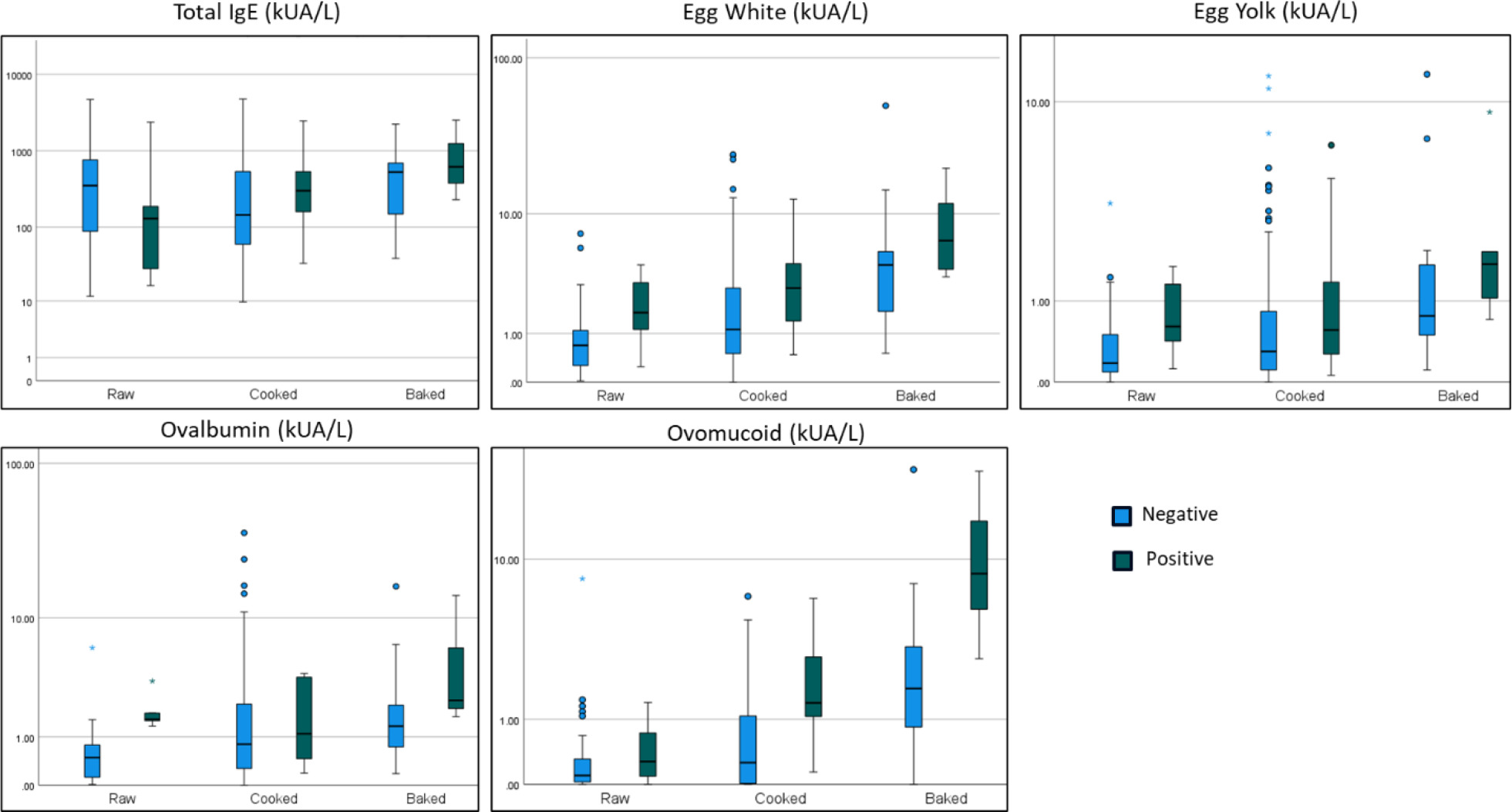
Comparisons between groups based on the OFC outcome are presented in Table 2 and Figure 2. Individuals with a positive OFC to raw egg demonstrated significantly higher serum sIgE levels for egg white, egg yolk, and ovalbumin. Patients with positive cooked egg OFCs were older in age and exhibited significantly elevated serum sIgE levels for egg white and ovomucoid. Furthermore, individuals with positive baked egg OFCs showed significantly higher levels of ovomucoid.
Figure 2: Total IgE and serum-specific IgE of egg proteins according to various forms of egg presentation and OFC outcomes.
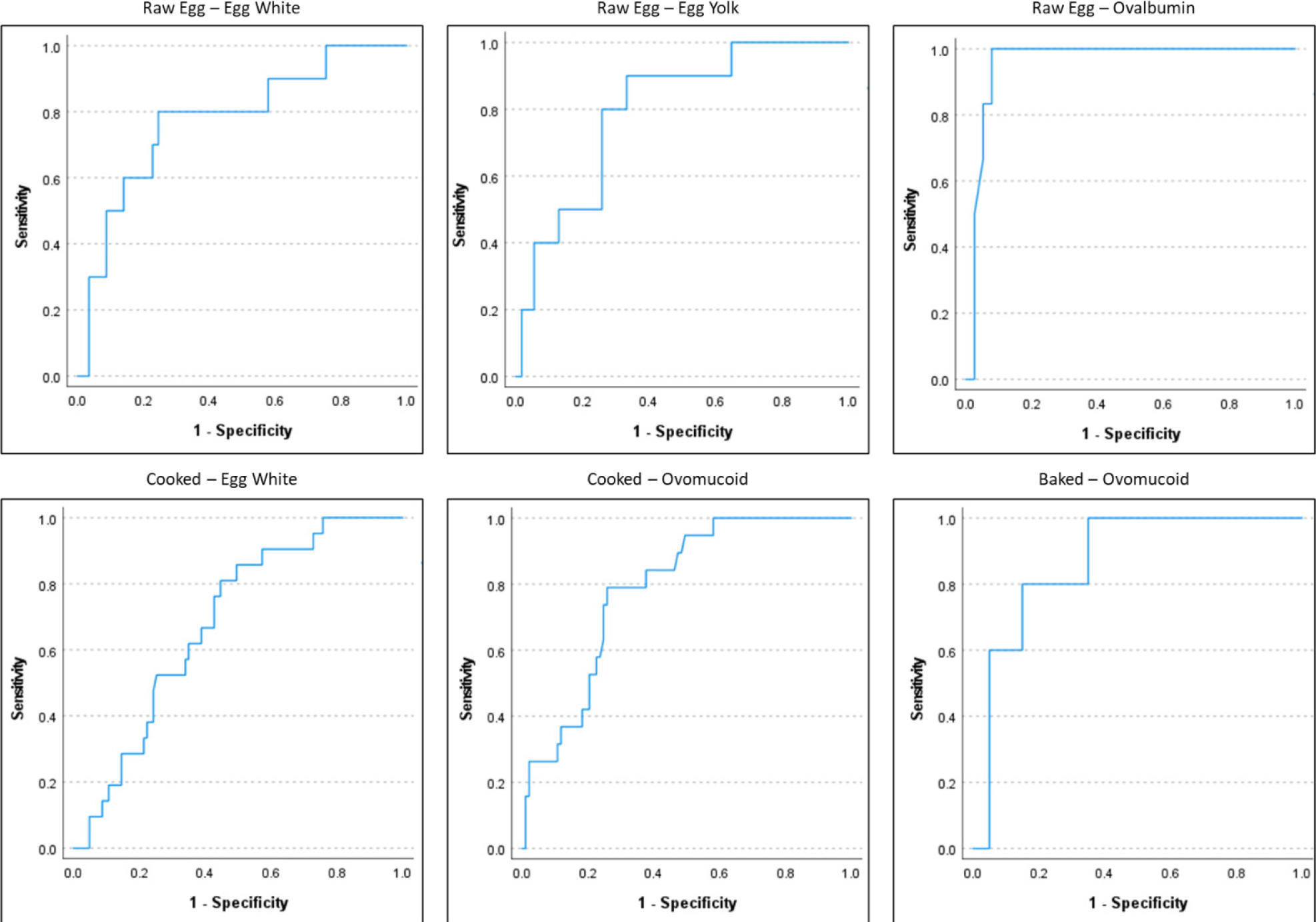
The ROC results are given in Table 3 and Figure 3.
Figure 3: Receiver operating characteristic curves to obtain optimal levels of serum sIgE.
Table 2: Comparison between groups according to the oral food challenge (OFC; n = 247) outcome.
| OFC | Raw (n = 67) | P | Cooked (n = 124) | P | Baked (n = 26)a | P | |||
|---|---|---|---|---|---|---|---|---|---|
| Negative (n = 57) | Positive (n = 10) | Negative (n = 103) | Positive (n = 21) | Negative (n = 21) | Positive (n = 5) | ||||
| Males | 29 (50.9%) | 6 (60.0%) | 0.736 | 64 (62.1%) | 15 (71.4%) | 0.420 | 10 (47.6%) | 2 (40.0%) | 1.000 |
| Age of OFC (IQR) years | 5 (6) | 5 (4) | 0.553 | 3 (3) | 4 (7) | 0.030 | 5 (5) | 9 (10) | 0.239 |
| Time IgE to OFC (IQR) months | 7 (9) | 6 (8) | 0.778 | 4 (5) | 4 (6) | 0.488 | 3 (4) | 8 (10) | 0.115 |
| Personal history | |||||||||
| Respiratory allergy | 35 (61.4%) | 4 (40%) | 0.299 | 52 (50.5%) | 12 (57.1%) | 0.578 | 11 (52.4%) | 3 (60%) | 1.000 |
| Atopic dermatitis | 19 (33.3%) | 2 (20%) | 0.487 | 34 (33%) | 12 (57.1%) | 0.037 | 11 (52.4%) | 1 (20%) | 0.330 |
| Other food allergy | 24 (42.1%) | 5 (50%) | 0.736 | 35 (34%) | 6 (28.6%) | 0.631 | 8 (38.1%) | 4 (80%) | 0.148 |
| Immunoglobulin E (IQR; KUA/L)b | |||||||||
| Total IgE | 352 (715) | 130 (1259) | 0.282 | 146 (491) | 302 (444) | 0.111 | 531 (582) | 620(-) | - |
| Egg white | 0.69 (0.87) | 1.7 (2.25) | 0.005 | 1.12 (2.33) | 2.82 (3.11) | 0.009 | 4.3 (4.15) | 6.5 (12.11) | 0.162 |
| Egg yolk | 0.18 (0.42) | 0.62 (0.98) | 0.003 | 0.3 (0.74) | 0.56 (1.50) | 0.074 | 0.76 (1.37) | 1.74 (4.68) | 0.135 |
| Ovalbumin | 0.49 (0.67) | 1.58 (0.75) | < 0.001 | 0.8 (1.94) | 1.09 (3.33) | 0.412 | 1.33 (1.82) | 2.38(-) | - |
| Ovomucoid | 0.10 (0.32) | 0.28 (0.73) | 0.230 | 0.26 (1.12) | 1.38 (2.57) | < 0.001 | 1.78 (2.64) | 8.43 (17.12) | 0.012 |
IQR: interquartile range; aIQR and P-value of total IgE and ovalbumin for baked egg group were not calculated due to insufficient results; bIgE values presented are median values.
Note: OFCs with egg yolk were not included because of the absence of positive results.
Table 3: Cut-off values of various serum sIgE egg proteins for positive OFC with sensitivity > 95%, optimal and specificity > 95%.
| Egg | IgE | Cut-off | Value | AUC (95% CI) | Sensitivity | Specificity | P |
|---|---|---|---|---|---|---|---|
| Raw | Egg white | S > 95% | 0.24 | - | 100% | 25% | |
| Optimal | 1.11 | 0.777 (0.617–0.937) | 80% | 72% | 0.001 | ||
| Sp > 95% | 3.07 | - | 30% | 97% | |||
| Egg yolk | S > 95% | 0.12 | - | 100% | 35% | ||
| Optimal | 0.28 | 0.796 (0.661–0.931) | 90% | 67% | < 0.001 | ||
| Sp > 95% | 1.4 | - | 20% | 96% | |||
| Ovalbumin | S > 95% | 1.28 | - | 100% | 92% | ||
| Optimal | 1.28 | 0.958 (0.900–1.017) | 100% | 92% | < 0.001 | ||
| Sp > 95% | 1.58 | - | 50% | 97% | |||
| Cooked | Egg white | S > 95% | 0.54 | - | 95% | 27% | |
| Optimal | 1.29 | 0.682 (0.575–0.788) | 81% | 55% | 0.001 | ||
| Sp > 95% | 11.15 | - | 10% | 95% | |||
| Ovomucoid | S > 95% | 0.27 | - | 95% | 50% | ||
| Optimal | 0.99 | 0.788 (0.694–0.882) | 79% | 74% | < 0.001 | ||
| Sp > 95% | 3.16 | - | 26% | 96% | |||
| Baked | Ovomucoid | S > 95% | 2.55 | - | 100% | 65% | |
| Optimal | 4.63 | 0.870 (0.718–1.022) | 80% | 85% | < 0.001 | ||
| Sp > 95% | 7.95 | - | 60% | 95% |
AUC: area under the curve; CI: confidence interval; S: sensitivity; Sp: specificity.
In the raw egg group, we identified ovalbumin as the most effective biomarker for predicting a positive OFC outcome (sIgE > 1.28 KUA/L). For the cooked egg group, ovomucoid emerged as the most predictive biomarker for a positive OFC result (sIgE > 0.99 KUA/L). In the baked egg group, ovomucoid displayed a significant predictive capacity for a positive OFC outcome (sIgE > 4.63 KUA/L).
Discussion
Our study showed that egg allergy was more frequent in males, which was similar to other studies that had identified male gender as an immutable risk factor for food allergy in children.4
In maximum cases, the occurrence that raised suspicion of egg allergy occurred in the first year of life, suggesting that egg allergy often manifests early in childhood, which was similar to the published studies, where the onset often occurred prior to the first birthday; this is partly associated with immature immune responses.6,8
Allergy is a multifactorial condition where the symptoms and onset can often mislead medical fraternity.1 In our population, mucocutaneous symptoms were the predominant clinical presentation, while gastrointestinal symptoms were reported in a smaller proportion. Anaphylaxis was reported in a significant number of patients; however, as mentioned, symptoms could be poorly understood by parents and attending physicians, leading to a poor association with a suspected allergic reaction.
A remarkable finding in our study was that a considerable subset of patients was referred solely based on positive serum sIgE to egg proteins without any associated symptoms on egg consumption, usually found while investigating other allergies, such as atopic dermatitis or other food allergies. Serum sIgE determination assays have good sensitivity but low specificity,15 highlighting the importance of considering sIgE testing only when an egg allergy is suspected, otherwise it can promote unnecessary evictions and have a deleterious impact on patients’ lives.
Respiratory allergy was observed in more than half of the patients (51.7%), indicating a possible co-occurrence of egg sensitization with other allergic conditions. Atopic dermatitis was also relatively common, affecting 36.4% of the participants, further emphasizing the complexity of allergies and their interplay in affected individuals. Additionally, other food allergies were reported in a significant proportion (39.8%), suggesting a broader pattern of allergic sensitization among the study cohort.
The development of atopic manifestations usually starts early in life, and tends to progress with time, and having one atopic disease is considered a risk factor for developing other atopic comorbidities Published results indicate that infants with a history of allergy and/or atopic diseases and sensitization to hen egg proteins are at higher risk of developing egg allergy.6 However, universal screening of high-risk infants and delayed egg introduction may paradoxically increase egg allergy diagnoses and healthcare costs.19
The distribution of the OFCs reflects the natural history of egg allergy, since tolerance to cooked egg precedes tolerance to raw egg,1 leading to food challenges with cooked egg being the most frequently tested food. A low proportion of positive OFC indicates accurate assessment by attending physicians and underscores that self-reported allergies often exceed true allergies, confirmed through OFCs.4
A noteworthy observation was the absence of positive OFCs in response to cooked egg yolk, a similar result obtained by Kido et al.,10 indicating that egg yolk might have a lower allergenic potential compared to other egg components.1,20
Egg allergens are composed of more than 20 types of proteins and glycoproteins, among which the most predominant are ovomucoid and ovalbumin from egg white, and alpha-livetin from egg yolk.8 Increasingly high serum sIgE levels indicate higher chances of clinical allergy; however, sensitivity is generally higher than specificity,4 which means that a proper evaluation of such results is imperative.
In the current literature, there is no universally accepted cut-off value for predicting egg allergy, because the population studied, the diagnostic methodology, and statistical analysis often differ, leading to different results. However, no cut-off value by itself may allow a firm diagnosis of egg allergy.15 It should instead be used to a better risk assessment, and complemented by a proper evaluation made by a qualified allergist.
In our population, the assessment of serum sIgE levels in response to different egg proteins yielded valuable breakthroughs into their discriminatory capacity in predicting positive OFC outcomes.
In the raw egg group, ovalbumin emerged as the most effective biomarker, exhibiting an impressive AUC of 0.958 for a cut-off value of 1.28 KUA/L. Most published studies had evaluated serum sIgE of egg white only, and not of different proteins.10,15 Studies in which ovalbumin was evaluated proposed cut-offs ranging from 1.3 KUA/L to 75 KUA/L,15 and as expected, their sensitivity and specificity vary greatly. The studies conducted by Vazquez-Ortiz et al.9,12 focused on identifying predictive values of ovalbumin serum sIgE for egg allergy in children aged >5 years, and showed a negative decision point of 0.30 KUA/L and a positive decision point of 2.01 KUA/L. In comparison, we verified that our optimal cut-off values were within their respective negative and positive decision points. Choosing a singular cut-off point, as opposed to an interval, helps mitigate uncertainty concerning sIgE values that were between negative and positive decision points. This approach enhanced the predictability of OFC results, contributing to a more robust risk assessment.
For the cooked egg group, ovomucoid demonstrated the best predictive ability with a good AUC and a cut-off value of 0.99 KUA/L. Concerning the current literature, most studies had focused on egg white serum sIgE, with values ranging from 24 KUA/L to 61 KUA/L to predict a positive OFC. These values allowed a high positive predictive value, but low in specificity,15 which means that many true allergic patients were catalogued as probably negative in OFC, leading to a poor risk evaluation. A study conducted by Kido et al.10 identified optimal predictive values of 10.1 KUA/L for a positive OFC of ovomucoid.
In the present study, patients had OFCs at an earlier age (median age approximately 2 years, while in our study the median age was 4 years) and the proportion of positive OFCs was remarkably higher (41.7% vs 14.9%). This favors the hypothesis that egg tolerance develops with age and is accompanied by a reduced serum sIgEs.21 A study conducted by Ando et al.13 proposed an optimal cut-off value of 4.40 KUA/L for ovomucoid to predict a positive OFC. Another study conducted by Vazquez-Ortiz et al. identified a negative decision point of 0.23 KUA/L and a positive decision point of 3.74 KUA/L for ovomucoid.9 The number of patients included in both studies was lower (n = 108 and 35, respectively) but had higher proportion of positive OFCs (35.2% and 58.8%, respectively). The higher cut-off values presented, in comparison to our study, might lead to some patients being incorrectly identified as nonallergic, with a higher probability of reacting during an OFC.
In the baked egg group, ovomucoid remained the only potentially interesting biomarker with a cut-off value of 4.63 KUA/L. A recent study conducted by Krawiec et al. discovered an optimal cut-off value of 0.55 KUA/L for ovomucoid.14 A study conducted by Caubet et al. identified an optimal cut-off value of 3.3 KUA/L for ovomucoid serum sIgE.11 Even though these studies had a higher number of patients, our results suggested that a more proactive approach could be considered safe with select children in which an OFC could be conducted safely, not requiring to wait for serum sIgE to drop further.
Our data emphasized the importance of considering different forms of egg presentation while evaluating specific IgE levels in the diagnosis and management of egg allergy. The variation in biomarker performance across egg forms emphasized the need for tailored approaches in clinical practice. These findings highlighted the potential clinical utility of serum sIgE measurements for ovalbumin and ovomucoid in predicting allergic reactions to different forms of egg presentation during OFC assessment. Moreover, the absence of positive OFCs in response to cooked egg yolk, associated with the statistically significant difference observed in egg yolk serum sIgE values between positive and negative groups for raw egg OFC, raised intriguing questions about the allergenicity and immunogenicity of this specific egg component, warranting further investigation.
The present study had several strengths that enhanced the significance and reliability of its findings. It included a well-defined cohort of pediatric patients, providing a focused and representative sample of individuals with suspected egg allergy, and evaluated a range of egg presentation forms, including cooked egg, raw egg, cooked egg yolk, and baked egg. This cohort allowed for an in-depth analysis and interpretation of serum sIgE across the various egg cooking methods. This comprehensive assessment allowed for a more nuanced understanding of allergenicity across various egg components. The study's findings had direct clinical relevance, aiding in the diagnosis and management of egg allergy. Identifying the most predictive biomarkers, such as ovalbumin and ovomucoid, could lead to a personalized patient care.
While the study provided valuable insights, it also had certain limitations. The study was conducted at a single center, potentially introducing biases related to the local population and practices, thereby limiting the ability to extrapolate our findings to the general population. The study’s retrospective nature might lead to inherent limitations, including incomplete or missing data, recall bias, and lack of control over confounding variables. Addressing these limitations in future investigations could enhance the comprehensiveness and applicability of findings, guiding clinicians to more accurate diagnosis and effective management of egg allergy.
Conclusion
The present study revealed significant insights into the epidemiology and diagnostic aspects of pediatric egg allergy. The evaluation of serum sIgE levels provided valuable discriminatory capacity, being of outmost importance during risk assessment by helping to predict positive OFC outcomes for different forms of egg presentation. The identification of reliable biomarkers, such as ovalbumin for raw egg and ovomucoid for cooked and baked egg, with well-defined cut-off values, could help clinicians in making informed decisions in diagnosing and managing egg allergies, ultimately improving patient care and quality of life. Future research in this area is crucial for refining our understanding of egg allergy pathophysiology and for optimizing diagnostic and therapeutic strategies.
Conflict of Interest
The authors declared that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
REFERENCES
1. Dona DW, Suphioglu C. Egg allergy: Diagnosis and immunotherapy. Int J Mol Sci. 2020;21(14):1–35. 10.3390/ijms21145010
2. Sirin Kose S, Asilsoy S, Uzuner N, Karaman O, Anal O. Outcomes of baked milk and egg challenge in cow’s milk and hen’s egg allergy: Can tolerance be predicted with allergen--specific IgE and prick-to-prick test? Int Arch Allergy Immunol. 2019;180(4):264–73. 10.1159/000502957
3. Anagnostou A. Optimizing patient care in egg allergy diagnosis and treatment. J Asthma Allergy. 2021;14:621–8. 10.2147/JAA.S283307
4. Sicherer SH, Sampson HA. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J Allergy Clin Immunol. 2018;141(1):41–58. 10.1016/j.jaci.2017.11.003
5. Valluzzi RL, Riccardi C, Arasi S, Piscitelli AL, Calandrelli V, Dahdah L, et al. Cow’s milk and egg protein threshold dose distributions in children tolerant to beef, baked milk, and baked egg. Allergy: European Journal of Allergy and Clinical Immunology. 2022;77(10):3052–60. 10.1111/all.15397
6. Caffarelli C, Giannetti A, Rossi A, Ricci G. Egg allergy in children and weaning diet. Nutrients. 2022;14(8):1540. 10.3390/nu14081540
7. Dodi G, Di Filippo P, Di Pillo S, Chiarelli F, Attanasi M. Total serum IgE levels as predictor of the acquisition of tolerance in children with food allergy: Findings from a pilot study. Front Pediatr. 2022;10:1013807. 10.3389/fped.2022.1013807
8. Zhang J, Shen Y, Li J, Li H, Si P. Component-resolved diagnostic study of egg allergy in northern Chinese children. Biomed Res Int. 2020;2020:3831087. 10.1155/2020/3831087
9. Vazquez-Ortiz M, Pascal M, Jiménez-Feijoo R, Lozano J, Giner MT, Alsina Let al. Ovalbumin-specific IgE/IgG4 ratio might improve the prediction of cooked and uncooked egg tolerance development in egg-allergic children. Clin Exp Allergy. 2014;44(4):579–88. 10.1111/cea.12273
10. Kido J, Nishi N, Matsumoto T. The oral provocation test for raw egg in patients with hen egg allergy. Int Arch Allergy Immunol. 2018;177(1):40–4. 10.1159/000489098
11. Caubet JC, Bencharitiwong R, Moshier E, Godbold JH, Sampson HA, Nowak-Wegrzyn A. Significance of ovomucoid-and ovalbumin-specific IgE/IgG 4 ratios in egg allergy. J Allergy Clin Immunol. 2012;129(3):739–47. 10.1016/j.jaci.2011.11.053
12. Vazquez-Ortiz M, Machinena-Spera A, Giner MT, Alvaro M, Piquer M, Dominguez O, et al. Ovalbumin-specific IgE/total IgE ratio improves the prediction of tolerance development in egg-allergic children aged ≥5 years. Pediat Allergy Immunol. 2015;26(6):580–3. 10.1111/pai.12417
13. Ando H, Movérare R, Kondo Y, Tsuge I, Tanaka A, Borres MP, et al. Utility of ovomucoid-specific IgE concentrations in predicting symptomatic egg allergy. J Allergy Clin Immunol. 2008;122(3):583–8. 10.1016/j.jaci.2008.06.016
14. Krawiec M, Radulovic S, Foong RX, Marques-Mejias A, Bartha I, Kwok M, et al. Diagnostic utility of allergy tests to predict baked egg and lightly cooked egg allergies compared to double-blind placebo-controlled food challenges. Allergy Eur J Allergy Clin Immunol. 2023 Sep;78(9):2510–22. 10.1111/all.15797
15. Calvani M, Arasi S, Bianchi A, Caimmi D, Cuomo B, Dondi A, et al. Is it possible to make a diagnosis of raw, heated, and baked egg allergy in children using cutoffs? A systematic review. Pediat Allergy Immunol. 2015;26(6):509–21. 10.1111/pai.12432
16. Muraro A, Werfel T, Hoffmann-Sommergruber K, Roberts G, Beyer K, Bindslev-Jensen C, et al. EAACI food allergy and anaphylaxis guidelines: Diagnosis and management of food allergy. Allergy Eur J Allergy Clin Immunol. 2014;69(8):1008–25. 10.1111/all.12429
17. Cardona V, Ansotegui IJ, Ebisawa M, El-Gamal Y, Fernandez-Rivas M, Fineman S, et al. World allergy organization anaphylaxis guidance 2020. World Allergy Organ J. 2020;13(10):100472. 10.1016/j.waojou.2020.100472
18. Suprun M, Getts R, Grishina G, Tsuang A, Suárez-Fariñas M, Sampson HA. Ovomucoid epitope-specific repertoire of IgE, IgG4, IgG1, IgA1, and IgD antibodies in egg-allergic children. Allergy Eur J Allergy Clin Immunol. 2020;75(10):2633–43. 10.1111/all.14357
19. Shaker M, Verma K, Greenhawt M. The health and economic outcomes of early egg introduction strategies. Allergy Eur J Allergy Clin Immunol. 2018;73(11):2214–23. 10.1111/all.13565
20. Dang TD, Peters RL, Koplin JJ, Dharmage SC, Gurrin LC, Ponsonby AL, et al. Egg allergen specific IgE diversity predicts resolution of egg allergy in the population cohort HealthNuts. Allergy Eur J Allergy Clin Immunol. 2019;74(2):318–26. 10.1111/all.13572
21. Andorf S, Bunning B, Tupa D, Cao S, Long AJ, Borres MP, et al. Trends in egg specific immunoglobulin levels during natural tolerance and oral immunotherapy. Allergy Eur J Allergy Clin Immunol. 2020;75(6):1454–56. 10.1111/all.14107