
Download
ORIGINAL ARTICLE
A real-world cross-sectional study evaluating the role of an oral amino acid-based supplement in nutrient intake by preschoolers on a cow’s milk elimination diet
Vanessa Cristina de Castro Rodriguesa, Thaysa Maués Cezarb, Camila Leonel Mendes de Abreuc, Adriana Sanudod, Mauro Batista de Moraise*
aPostgraduation Program in Nutrition, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, Brazil
bMedical Affairs Department, Danone Nutricia Brazil, São Paulo, Brazil
cIndependent Nutritionist, São Paulo, Brazil
dDepartment of Preventive Medicine, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, Brazil
eDivision of Pediatric Gastroenterology and Postgraduation Program in Nutrition, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, Brazil
Abstract
Introduction and Objectives: Food allergy has several negative nutritional consequences and may persist beyond the first year of lives. This study aimed to assess the role of a complete oral amino acid-based supplement in the diet of children on cow’s milk protein elimination diet because of food allergy.
Materials and Methods: This study included two groups of children aged 1–5 years paired by age and socioeconomic status: (1) study group, on cow’s milk protein elimination diet plus an oral amino acid-based supplement, and (2) control group, on cow’s milk protein elimination diet. Sociodemographic, clinical, anthropometric, and dietary data were obtained through online interviews. Two 24-h dietary recalls were collected on nonconsecutive days. Both groups comprised mostly boys.
Results: The study group presented lower values of body mass index. The frequency of feeding difficulties was similar between groups. The study group had a higher intake of energy, protein, carbohydrates, calcium, iron, zinc, phosphorus, magnesium, copper, selenium, vitamins D, E, B1, B2, B6, and B12, niacin, and folic acid compared to the control group. A higher proportion of children in the study group had adequate intake according to the recommendations made for energy, carbohydrates, iron, phosphorus, selenium, vitamins A, D, E, B1, B2, and B6, and folic acid.
Conclusions: The use of a complete oral amino acid-based supplement has a positive effect on the diet quality of preschoolers on cow’s milk elimination diet because of food allergy, promoting higher intake of energy, calcium, vitamin D, and other essential nutrients.
Key words: amino acid-based supplement, cow’s milk -elimination diet, dietary supplements, feeding difficulties, milk hypersensitivity (allergy)
*Corresponding author: Mauro Batista de Morais, MD, PhD, Division of Pediatric Gastroenterology, Rua dos Otonis, 839 São Paulo, SP 04040-032, Brazil. Email address: [email protected]
Received 6 January 2024; Accepted 18 March 2024; Available online 1 May 2024
Copyright: Rodrigues VCdC, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Cow’s milk protein allergy (CMPA) is common during the first year of birth.1–6 The control of clinical manifestations of CMPA by eliminating cow’s milk proteins from the diet and prescribing a hypoallergenic infant formula for those who are not breastfed are essential to achieve full growth and development of infants with CMPA. Complementary feeding should follow the recommendations for healthy infants, except for cow’s milk protein elimination from the diet. Several children with CMPA are expected to develop tolerance to cow’s milk proteins during the first and second years of lives. Tolerance acquisition is confirmed through a negative oral challenge test.3–6 In recent decades, alerts have emerged indicating an increased risk of CMPA persisting beyond the first year of birth. Therefore, several children aged >1 year still require a cow’s milk elimination diet.2,7–9
Negative nutritional consequences are a significant concern for infants and children with CMPA, both before and after implementing an elimination diet. Several published studies demonstrated deficits in height and weight.1,9–14 After the first year of birth, a high prevalence of feeding difficulties was observed.10,15–17
Several factors contribute to nutritional deficits in CMPA, including decreased appetite, low energy intake, elevated levels of inflammatory cytokines, intestinal malabsorption, and loss of nutrients through the intestinal epithelium.10 Insufficient intake of calcium, vitamins A and D, and iron, among other nutrients, can have negative consequences for the child.9–12 Therefore, it is crucial that the elimination diet controls the clinical manifestations of CMPA and reverses and prevents nutritional deficiency.
Amino acid-based formulas are free from allergenic epitopes, making them tolerable for infants and children with CMPA, regardless of the severity or presence of other food allergies. In several guidelines, amino acid-based infant formulas are recommended for the treatment of infants with severe CMPA. Amino acid-based infant formulas are also recommended for patients with moderate or mild CMPA who do not improve with the intake of an extensively hydrolyzed protein-based infant formula.3–6 An oral amino acid-based supplement that is nutritionally complete was developed and marketed to meet the nutritional needs of children aged ≥1 year with CMPA and/or other food allergies. This dietary supplement could be prescribed to preschoolers on cow’s milk protein elimination diet, regardless of having nutritional deficits and feeding difficulties or allergies to other proteins. To the best of our knowledge, no published studies have evaluated the effects of this supplement on the food intake of allergic preschoolers within the context of community standard clinical practice.
Therefore, this study aimed to assess the role of a complete oral amino acid-based supplement in preschoolers recruited from the community who were on cow’s milk protein elimination diet due to CMPA.
Materials and methods
Study design
This real-world cross-sectional study was conducted to compare preschoolers on cow’s milk protein elimination diet who received a nutritionally complete oral amino acid-based supplement to those who did not receive this supplement. Sociodemographic, clinical and feeding difficulties, anthropometric, and dietary intake information were obtained through individual online interviews. All guardians were aged ≥18 years and agreed to the conditions of the informed consent form. The parents or guardians of the subjects voluntarily provided online informed consent prior to enrollment. This study was evaluated and approved by a Brazilian Research Ethics Committee (CAAE 48787621.6.0000.0087).
Participants
The participants were recruited online from September 2021 to June 2022 according to two inclusion criteria: Children (1) aged between 1 and 5 years, and (2) being fed with cow’s milk protein elimination diet for at least 1 month, as prescribed by a physician, because of CMPA associated or not to allergy to others foods. The recruited participants were divided into two groups: (1) the study group, which comprised children who consumed a nutritionally complete oral amino acid-based supplement (Neoforte®, Danone, Liverpool, UK) for at least 1 month as well as regular cow’s milk elimination diet, and (2) the control group, which included children who were also on a cow’s milk elimination diet but not receiving the oral amino acid-based supplement. In both groups, children may have been consuming hypoallergenic formulas, plant-based drinks, or supplements containing vitamins and minerals as well as an elimination diet for proteins other than those in cow’s milk, as recommended by their physicians and effected by their caregivers. The children were assisted by several professionals responsible for their clinical and nutritional care. The diagnosis of CMPA was established by the physician of each patient according to their real-life clinical practice, considering the clinical manifestations and response to the elimination of cow’s milk protein in the majority of patients. Other clinical or laboratory data were used in case of some patients. Therefore, the information collected represented the community standard clinical practice.
The following exclusion criteria were considered: current breastfeeding (due to the lack of method to estimate the breast milk daily intake by preschoolers); birth weight < 2500 g; premature birth (except for late preterm, defined as gestational age ≥ 34–37 weeks); severe liver, heart, kidney, genetic, endocrine, or neurological diseases; cancer and severe neuropsychomotor development delay; diseases that require dietary modifications, such as diabetes mellitus, celiac disease, fructose intolerance, and galactosemia; tube or gastrostomy feeding; and hospitalization within 30 days before the study.
The sample size estimative was based on calcium consumption. The expected increment in calcium intake in the study group was 177 mg per day (equivalent to the calcium content in a 150-mL serving of the oral amino acid-based supplement). The standard deviation (SD) of the mean daily calcium intake was based on a previous study comprising Brazilian children without dietary restrictions.12 Therefore, considering the difference between the groups of 177 mg and the SD of 260 mg (alpha = 5% and power = 80%), each group should have 35 children.
Parents of the children with CMPA on a milk-free diet were invited to join the study through the following: social media, a website about CMPA (alergiaaoleitedevaca.com.br), and pediatricians. Parents interested to join the study were directed to a landing page via a link to access the Informed Consent Form. After expressing their understanding and agreement, they filled the online form. Subsequently, the participants were contacted by a nutritionist to schedule online interviews.
At the end of the data collection period, the expected sample size for the study group was not reached, and hence a proportion of two paired (by age and socioeconomic status) controls for each case was adopted. Therefore, the study (with amino acid-based supplement) and control groups comprised 17 and 34 children, respectively.
Demographic, clinical, and anthropometric data
The following information was collected: birth date, gender, vaginal or cesarean delivery, birth weight, gestational age, duration of exclusive and total breastfeeding, number of foods eliminated from the diet, and duration of elimination diet. Data about geographic region of residence, maternal education, and socioeconomic class were also recorded.
The Montreal Children’s Hospital Feeding Scale18 translated and validated for Brazilian Portuguese19 was used for screening feeding difficulties (>45 points).
Information concerning weight and height was also collected. Only measurements recorded on the child’s health card by a pediatrician or other healthcare professional within 90 days before or after inclusion were accepted. The z-scores for weight-for-age, height-for-age, and body mass index (BMI)-for-age were calculated using the Anthro software version 3.2.2 and Anthro plus version 1.0.4 (World Health Organization).
Interviews
The interviews were conducted via video calls. During the first interview, eligibility was confirmed, and the first 24-h dietary recall was collected.20 Data on the quantities, brands, and preparation methods of all foods, formulas, beverages, and vitamin or mineral supplements that the child had consumed on the previous day were collected, including those consumed during night time. The study group was also asked about the amount of oral amino acid-based supplement that children had consumed. For greater accuracy in recording the weights of portions and the composition of mixed dishes, the nutritionist or participant provided video footage of household measurements, food labels, and patient package inserts for vitamins and minerals supplements, as well as information on the quantities of each ingredient and the yield of homemade recipes. The report ended by checking whether all foods or drinks were recorded. For portion measurement, Brazilian manuals on portion quantification were consulted.21–22
During the second interview, the second 24-h dietary recall was collected using the same criteria and collection method that was used in the first interview.
All contacts and data collection were performed by a single nutritionist researcher. An attempt was made to distribute dietary recall data proportionally across days of the week.20 If necessary, the demographic, clinical, and anthropometric data were reviewed in the interviews.
Assessment of nutrient intake
The data from each dietary recall were transcribed into four separate spreadsheets as specified below:
-
Milk substitutes: The brands of formulas and plant-based drinks used to replace cow’s milk, along with their respective home preparation methods in terms of measurements, volume, and/or number of measuring scoops used, were transcribed in this document.
-
Complete oral amino acid-based supplement: This included information on the volume and number of measuring scoops recorded in each dietary recall. The oral supplement Neoforte® (Danone, Liverpool, UK), available in vanilla and strawberry flavors, evaluated in this study was nutritionally complete, based on free amino acids. The nutritional composition is presented in Table 1.
-
Other foods and beverages: These included all other foods and beverages reported in each dietary recall, including details of preparation methods, brands of processed foods, household measurements, number of servings, and/or volumes consumed.
-
Vitamin and mineral supplements: These included information about the brands of supplements and the doses prescribed.
Table 1 Nutritional composition of the complete oral amino acid-based supplement (vanilla flavor).
| Nutrients | 100-g powder | 100 mL (21.8-g powder + 80-mL water) |
|---|---|---|
| Energy | 459 Kcal | 100 Kcal |
| Carbohydrates | 51 g | 11 g |
| Sugars | 11 g | 2.4 g |
| Protein | 16 g | 3.5 g |
| Total fat | 21 g | 4.6 g |
| Saturated fat | 7.9 g | 1.7 g |
| Fiber | 1.9 g | 0.4 g |
| Sodium | 230 mg | 50 mg |
| Potassium | 653 mg | 142 mg |
| Chloride | 349 mg | 76 mg |
| Calcium | 542 mg | 118 mg |
| Iron | 7.4 mg | 1.6 mg |
| Phosphorus | 367 mg | 80 mg |
| Magnesium | 77 mg | 17 mg |
| Zinc | 4.7 mg | 1.0 mg |
| Copper | 530 mg | 115 µg |
| Manganese | 0.62 mg | 0.14 mg |
| Molybdenum | 22 µg | 4.7 µg |
| Selenium | 18 µg | 4.0 µg |
| Chromium | 18 µg | 3.9 µg |
| Iodine | 85 µg | 19 µg |
| Vitamin A | 276 µg - RE | 60 µg - RE |
| Vitamin D | 9.1 µg | 2.0 µg |
| Vitamin E | 6.4 µg - α TE | 1.4 mg - α TE |
| Vitamin K | 19 µg | 4.2 µg |
| Vitamin B1 | 0.48 mg | 0.10 mg |
| Vitamin B2 | 0.92 mg | 0.20 mg |
| Niacin | 4.3 mg - NE | 0.94 mg - NE |
| Pantothenic acid | 1.9 mg | 0.41 mg |
| Vitamin B6 | 0.48 mg | 0.10 mg |
| Folic acid | 143 µg | 31 µg |
| Vitamin B12 | 1.8 µg | 0.39 µg |
| Biotin | 14 µg | 3.0 µg |
| Vitamin C | 45 mg | 9.7 mg |
| Choline | 143 mg | 31 mg |
| Carnitine | 15 mg | 3.3 mg |
| Inositol | 105 mg | 23 mg |
| Taurine | 30 mg | 6.5 mg |
Sources of macronutrients: carbohydrates: 86% glucose syrup and 14% sucrose. Proteins: 100% free amino acids. Fats: 100% vegetable oils (35% medium chain triglycerides). Does not contain trans fatty acids. Fibers: inulin, and oligofructose.
These independent spreadsheets did not contain any additional information about children’s identification. They were analyzed separately. A nutritionist who was not involved in data collection and transcription of these documents calculated the intake of energy and nutrients, resulting in four separate databases corresponding to the above-listed four food groups.
The mean intake from two dietary recalls was calculated for each child, except in cases where only one recall was possible due to child’s illness or unavailability of caregiver for the second interview. The acceptable macronutrient distribution ranges (AMDRs) and recommended dietary allowances (RDAs) or adequate intakes (AI) from the dietary reference intakes (DRIs) of the Institute of Medicine were considered to assess the adequacy of daily nutrient intake for macronutrients, vitamins, and minerals.23 The recommendations of the Food and Agriculture Organization/World Health Organization/United Nations University (FAO/WHO/UNU, 2004) were followed for energy.24 The minimum recommended daily dietary fiber intake was “age + 5” grams.25
The following sources were used for the calculation of energy and nutrient intake: Brazilian Table of Food Composition (Tabela Brasileira de Composição de Alimentos [TBCA]),26 Food Composition Table of the Brazilian Institute of Geography and Statistics (Instituto Brasileiro de Geografia e Estatística),27 TBCA from the State University of Campinas (Universidade Estadual de Campinas),28 and the food composition table of the Agricultural Research Service of the US Department of Agriculture.29 Measurement details reported on manufacturers’ websites or packaging were also considered for processed foods, vitamin or mineral supplements, and the complete oral amino acid-based supplement.
Statistical analyses
The statistical analyses were performed using the Stata/SE 15.1 software (StataCorp, 2017; StataCorp LLC) and Jamovi version 2.3 (The Jamovi Project; 2022 [computer software]; https://www.jamovi.org).
Results
General, clinical, feeding difficulties, and -anthropometric data
The mean age of the children, predominantly comprising boys, was 3 years (Table 2). Maternal educational level was similar between the groups, with most of the mothers having completed a college degree. Children from all five regions of Brazil participated in this study. Most of the children belonged to the higher socioeconomic strata (classes A and B). No differences were discovered between the groups concerning delivery type, late preterm birth, birth weight, duration of exclusive and total breastfeeding, number of eliminated foods from the diet, and duration of elimination diet. The proportion of children with feeding difficulties, as evaluated by the Montreal Children’s Hospital Feeding Scale, was similar in both groups. The weight-for-age and BMI-for-age z-scores were lower in the study group, compared to the control group. However, the difference in weight-for-age z-score was not statistically significant. No difference was observed in height-for-age z-scores (Table 2).
Table 2 Demographic, neonatal, and feeding difficulties, and anthropometric data of the study group (oral amino acid-based supplement) and the control group.
| Amino acid-based supplement group | P | ||
|---|---|---|---|
| Yes (n = 17) | No (n = 34) | ||
| Age (years) | 3.0 ± 1.2 | 3.1 ± 1.2 | 0.685a |
| Gender (male) | 12 (70.6%) | 23 (67.7%) | 1.000b |
| Maternal education | 0.450b | ||
| Completed undergraduate degree | 10 (58.8%) | 18 (52.9%) | |
| Completed high school education | 7 (41.2%) | 13 (38.2%) | |
| Elementary school | 0 (0.0%) | 3 (8.8%) | |
| Brazilian geographic region | 0.590b | ||
| North | 1 (2.9%) | 2 (11.8%) | |
| Northeast | 10 (29.4%) | 6 (35.3%) | |
| Midwest | 1 (2.9%) | 1 (5.9%) | |
| South | 5 (14.7%) | 1 (5.9%) | |
| Southeast | 17 (50.0%) | 7 (41.2%) | |
| Socioeconomic statusc | 0.820b | ||
| A | 5 (29.4%) | 8 (23.5%) | |
| B | 11 (64.7%) | 22 (64.7%) | |
| C | 1 (5.9%) | 4 (11.8%) | |
| Neonatal data | |||
| Vaginal delivery | 1 (5.9%) | 7 (20.6%) | 0.242b |
| Late preterm birth | 3 (17.7%) | 2 (5.9%) | 0.318b |
| Birth weight (g) | 3092 ± 396 | 3365 ± 551 | 0.108d |
| Dietary information | |||
| Exclusive breastfeeding duration (months) | 4.1 ± 2.3 | 4.7 ± 2.1 | 0.474d |
| Total breastfeeding duration (months) | 16.4 ± 14.7 | 16.9 ± 11.8 | 0.542d |
| Number of foods currently eliminated from the diet | 2.2 ± 2.5 | 2.0 ± 1.7 | 0.911d |
| Duration of elimination diet (months) | 25.3 ± 18.6 | 27.2 ± 16.1 | 0.614d |
| Montreal Children’s Hospital Feeding Scale | |||
| Frequency of feeding difficulty | 4/15 (26.7%) | 6/31 (19.4%) | 0.706b |
| Anthropometric indicators (z-scores) | |||
| Weight-for-age | −0.42 ± 0.99 | +0.22 ± 1.27 | 0.088a |
| Height-for-age | +0.03 ± 1.10 | +0.04 ± 1.43 | 0.738d |
| Body mass index (BMI) for age | −0.71 ± 1.04 | +0.27 ± 1.40 | 0.022a |
aMean ± standard deviation (Mann–Whitney U test); bNumber (percentage) (Fisher’s exact test); cSocioeconomic status: Brazil criterion (06/01/2021) from the “ABEP Associação Brasileira de Empresas de Pesquisa (http://www.abep.org/criterio-brasil); dMean ± standard deviation (Student’s t test).
Energy and macronutrient intake
The study group consumed 56–659 mL of oral amino acid-based supplement per day, with a mean consumption of 266 ± 147 mL.
The study group had a higher total daily intake of energy, protein, carbohydrates, and fats, compared to the control group (Table 3). This increase in intake was due to the contribution of the oral amino acid-based supplement, as intake from other sources, such as milk substitutes, and other foods, and beverages, was similar between the groups, except for proteins. Considering the daily recommended intake, the study group had a higher proportion of children with adequate intake of energy and carbohydrates. Furthermore, no difference was observed between the groups concerning dietary fiber intake.
Table 3 Energy and macronutrient intakes of the study (oral amino acid-based supplement) and control groups
| Amino acid-based supplement group | P | |||
|---|---|---|---|---|
| Yes (n = 17) | No (n = 34) | |||
| Energy (kcal) | Total | 1359.3 ± 341.3 | 1051.2 ± 261.4 | 0.002a |
| Milk substitutes | 182.1 ± 224.6 | 213.4 ± 201.3 | 0.566a | |
| Oral amino acid-based supplement | 265.8 ± 146.9 | - | - | |
| Other foods and beverages | 910.7 ± 332.0 | 837.8 ± 292.7 | 0.426b | |
| Energy intake ≥ recommendation for age and gender by WHO | 14 (82.4%) | 14 (41.2%) | 0.007c,d | |
| Protein (g) | Total | 57.1 ± 13.6 | 40.3 ± 12.4 | < 0.001b |
| Milk substitutes | 4.8 ± 5.9 | 5.9 ± 6. | 0.531a | |
| Oral amino acid-based supplement | 9.3 ± 5.1 | - | - | |
| Other foods and beverages | 43.0 ± 15.2 | 34.5 ± 13.3 | 0.044b | |
| Protein intake < AMDR of the DRIs | 0 (0.0%) | 2 (5.9%) | ||
| Protein intake within the AMDR range of DRIs | 15 (88.2%) | 30 (88.2%) | 0.638c,e | |
| Protein intake > AMDR of DRIs | 2 (11.8%) | 2 (5.9%) | ||
| Carbohydrate (g) | Total | 186.6 ± 45.4 | 158.4 ± 39.3 | 0.016a |
| Milk substitutes | 23.6 ± 31.5 | 25.1 ± 24.2 | 0.665a | |
| Oral amino acid-based supplement | 29.5 ± 16.3 | - | - | |
| Other foods and beverages | 133.4 ± 44.5 | 133.3 ± 44.0 | 0.996b | |
| Carbohydrate intake within the AMDR range of DRIs | 17 (100.0%) | 24 (70.6%) | 0.021c,e | |
| Carbohydrate intake > AMDR of DRIs | 0 (0.0%) | 10 (29.4%) | ||
| Fat (g) | Total | 46.7 ± 15.1 | 31.8 ± 13.6 | < 0.001b |
| Milk substitutes | 7.7 ± 9.3 | 10.0 ± 9.8 | 0.526a | |
| Oral amino acid-based supplement | 12.2 ± 6.7 | - | ||
| Other foods and beverages | 26.8 ± 14.8 | 21.8 ± 13.7 | 0.297a | |
| Fat intake < AMDR of DRIs | 7 (41.2%) | 21 (61.8%) | ||
| Fat intake within the AMDR range of DRIs | 8 (47.1%) | 12 (35.3%) | 0.204c,e | |
| Fat intake > AMDR of DRIs | 2 (11.8%) | 1 (2.9%) | ||
| Dietary fiber (g) | Total | 15.2 ± 6.8 | 12.4 ± 3.8 | 0.279a |
| Milk substitutes | 1.1 ± 2.4 | 0.6 ± 1.4 | 0.210a | |
| Oral amino acid-based supplement | 1.1 ± 0.6 | - | - | |
| Other foods and beverages | 13.0 ± 6.6 | 11.8 ± 3.6 | 0.774a | |
| Fiber intake below the recommendation of “age + 5 g” | 2 (11.8%) | 3 (8.8%) | 1.000c,f | |
aMean values and standard deviation (Mann–Whitney U test); bmean values and standard deviation (Student’s t-test); cNumber (percentage) (Fisher’s exact test); cEnergy recommendation based on age and gender (FAO/WHO/UNU, 2004); eAge-specific recommendations based on the percentage of total denergy intake (acceptable macronutrient distribution ranges [AMDRs], dietary reference intakes [DRIs], Institute of Medicine): protein, 5–20% for 1–3 years and 10–30% for 4–18 years; carbohydrates, 45–65% for 1–18 years; lipids, 30–40% for 1–3 years and 25–35% for 4–18 years; fminimum fiber intake recommendation: age (in years) + 5 g (Williams et al., 1995). No child had a carbohydrate intake below the AMDR-recommended range.
Calcium and other mineral intake
The study group had a higher daily intake of calcium, compared to the control group (Table 4). The intake of calcium from milk substitutes, other foods and beverages, and supplements was similar, indicating that increase in total daily intake in the study group was due to the consumption of complete oral amino acid-based supplement. Although the study group had twice the proportion of children with adequate calcium intake (35.7%), compared to the control group (14.7%), the difference was not statistically significant (P = 0.17) (Figure 1).
Table 4 Mineral and trace element intake in the study (oral amino acid-based supplement) and control groups.
| Amino acid-based supplement group | P | |||
|---|---|---|---|---|
| Yes (n = 17) | No (n = 34) | |||
| Calcium (mg): | Total | 700.9 ± 166.0 | 405.2 ± 277.7 | < 0.001a |
| Milk substitutes | 211.5 ± 181.2 | 266.8 ± 268.8 | 0.650a | |
| Oral amino acid-based supplement | 313.9 ± 173.5 | - | - | |
| Other foods and beverages | 131.7 ± 70.4 | 118.0 ± 113.7 | 0.186a | |
| Calcium provided by other supplements | 43.8 ± 101.2 | 20.4 ± 56.1 | 0.545a | |
| Phosphorus (mg): | Total | 758.1 ± 196.1 | 525.4 ± 211.6 | < 0.001a |
| Milk substitutes | 79.0 ± 117.1 | 141.0 ± 189.3 | 0.274a | |
| Oral amino acid-based supplement | 212.6 ± 117.5 | - | - | |
| Other foods and beverages | 466.5 ± 182.1 | 384.4 ± 140.6 | 0.084a | |
| Iron (mg): | Total | 16.6 ± 11.8 | 13.0 ± 19.7 | 0.003a |
| Milk substitutes | 1.4 ± 1.9 | 2.4 ± 3.3 | 0.493a | |
| Oral amino acid-based supplement | 4.3 ± 2.4 | - | - | |
| Other foods and beverages | 6.4 ± 3.2 | 4.8 ± 2.1 | 0.092a | |
| Iron provided by other supplements | 4.5 ± 11.2 | 5.7 ± 20.0 | 0.964a | |
| Zinc (mg): | Total | 11.4 ± 3.8 | 8.0 ± 4.5 | 0.001a |
| Milk substitutes | 1.25 ± 1.59 | 2.27 ± 2.62 | 0.184a | |
| Oral amino acid-based supplement | 2.7 ± 1.5 | - | - | |
| Other foods and beverages | 6.3 ± 2.9 | 4.9 ± 2.6 | 0.061a | |
| Zinc provided by other supplements | 1.10 ± 2.62 | 0.84 ± 3.46 | 0.420a | |
| Magnesium (mg): | Total | 190.0 ± 53.2 | 135.8 ± 42.4 | < 0.001b |
| Milk substitutes | 16.4 ± 28.0 | 21.8 ± 27.1 | 0.520a | |
| Oral amino acid-based supplement | 44.6 ± 24.6 | - | - | |
| Other foods and beverages | 129.0 ± 45.9 | 114.1 ± 40.6 | 0.241b | |
| Cooper (mg): | Total | 1.13 ± 0.35 | 1.03 ± 0.97 | 0.016a |
| Milk substitutes | 0.10 ± 0.15 | 0.16 ± 0.18 | 0.340a | |
| Oral amino acid-based supplement | 0.31 ± 0.17 | - | - | |
| Other foods and beverages | 0.70 ± 0.33 | 0.87 ± 0.94 | 0.729a | |
| Selenium (mcg): | Total | 27.0 ± 7.2 | 16.7 ± 10.2 | < 0.001a |
| Milk substitutes | 3.9 ± 6.2 | 4.0 ± 5.3 | 0.782a | |
| Oral amino acid-based supplement | 10.4 ± 5.8 | - | - | |
| Other foods and beverages | 12.1 ± 8.2 | 12.9 ± 10.1 | 0.824a | |
aMean values and standard deviation (Mann–Whitney U test); bmean values and standard deviation (Student’s t-test). The values of copper and selenium in mineral supplements are not provided because only one child used a supplement containing these elements. However, the total daily intake included the copper and selenium provided by these mineral supplements. No child used mineral supplements that contained phosphorus and magnesium.
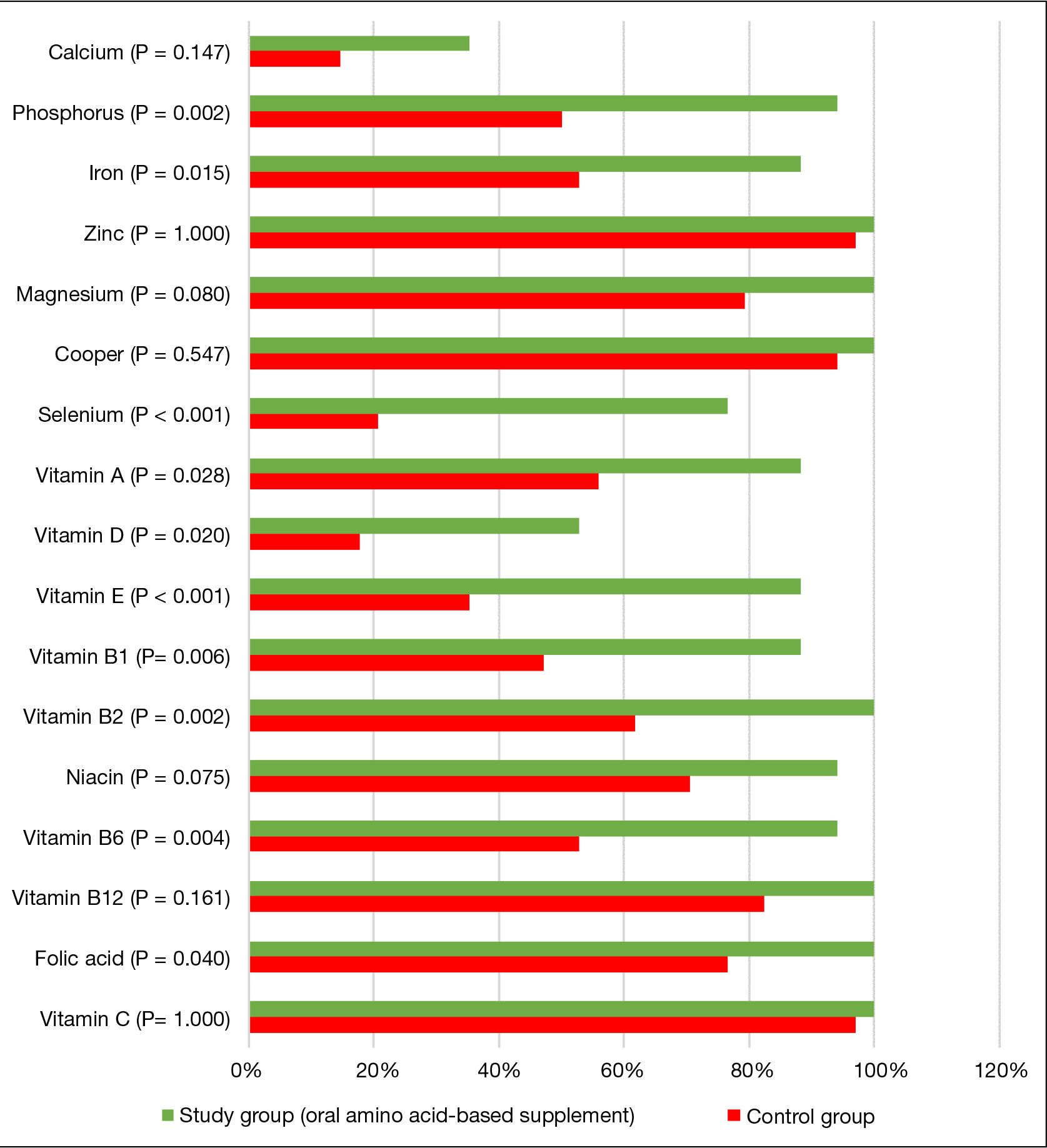
Figure 1 Percentage of children with mineral and vitamin intakes meeting the recommended dietary allowances (RDAs) or adequate intakes (AIs), dietary reference intakes (DRIs), Institute of Medicine (calcium, 700 mg for 1–3 years and 1000 mg for 4–8 years; phosphorus, 460 mg for 1–3 years and 500 mg for 4–8 years; iron, 7 mg for 1–3 years and 10 mg for 4–8 years; zinc, 3 mg for 1–3 years and 5 mg for 4–8 years; magnesium, 80 mg for 1–3 years and 130 mg for 4–8 years; copper, 0.34 mg for 1–3 years and 0.44 mg for 4–8 years; selenium, 20 mcg for 1–3 years and 30 mcg for 4–8 years; vitamin A, 300 mcg for 1–3 years and 400 mcg for 4–8 years; vitamin D, 15 mcg for 1–8 years; vitamin E, 6 mg for 1–3 years and 7 mg for 4–8 years; vitamin B1, 0.5 mg for 1–3 years and 0.6 mg for 4–8 years; vitamin B2, 0.5 mg for 1–3 years and 0.6 mg for 4–8 years; niacin, 6 mg for 1–3 years and 8 mg for 4–8 years; vitamin B6, 0.5 mg for 1–3 years and 0.6 mg for 4–8 years; vitamin B12, 0.9 mcg for 1–3 years and 1.2 mcg for 4–8 years; folic acid, 150 mcg for 1–3 years and 200 mcg for 4–8 years; vitamin C, 15 mg for 1–3 years and 25 mg for 4–8 years). Results are expressed as percentage (Fisher’s exact test).
For the other seven minerals evaluated, the study group had a higher total daily intake than the control group (Table 4). This increase in intake was due to the contribution of oral supplement, as intake from other sources (milk substitutes, other foods and beverages, and minerals provided by supplements) was similar between the groups. In the case of iron, phosphorus, and zinc, the contribution from other foods and beverages was higher in the study group, compared to the control group. However, this difference was also not statistically significant. The frequency of children meeting the RDA for iron, phosphorus, and selenium was higher in the study group than in the control group (Figure 1).
Vitamin intake
Higher daily intake of vitamins D, E, B1, B2, B6, and B12, niacin, and folic acid was observed in the study group (Table 5). A higher frequency of compliance with the daily intake recommendations was observed in the study group for all vitamins, except for vitamins C and B12. In the case of niacin, a higher frequency of compliance with recommendations was observed, but the difference was not statistically significant (Figure 1). The contribution of milk substitutes, other foods and beverages, and vitamin supplements to vitamin consumption was similar between the groups, indicating that the increase in intake was due to the complete oral amino acid-based supplement. Notably, the study group had a higher vitamin D intake through supplements, compared to the control group, but the difference was not statistically significant.
Table 5 Vitamin intake in the study (oral amino acid-based supplement) and control groups.
| Amino acid-based supplement group | P | |||
|---|---|---|---|---|
| Yes (n = 17) | No (n = 34) | |||
| Vitamin A (mcg RAE): | Total | 664.6 ± 350.0 | 786.8 ± 1046.9 | 0.117a |
| Milk substitutes | 109.6 ± 137.3 | 199.4 ± 246.6 | 0.283a | |
| Oral amino acid-based supplement | 159.9 ± 88.3 | - | - | |
| Other foods and beverages | 281.1 ± 235.0 | 444.9 ± 970.5 | 0.458a | |
| Vitamin A provided by other supplements | 114.1 ± 218.4 | 142.5 ± 404.4 | 0.453a | |
| Vitamin D (mcg): | Total | 14.76 ± 6.89 | 8.63 ± 8.23 | 0.001a |
| Milk substitutes | 2.49 ± 2.89 | 3.64 ± 4.08 | 0.430a | |
| Oral amino acid-based supplement | 5.27 ± 2.91 | - | - | |
| Other foods and beverages | 1.09 ± 0.94 | 1.31 ± 1.98 | 0.976a | |
| Vitamin D provided by other supplements | 5.91 ± 6.30 | 3.68 ± 7.72 | 0.063a | |
| Vitamin E (mg): | Total | 9.11 ± 2.81 | 5.41 ± 3.62 | 0.047a |
| Milk substitutes | 1.93 ± 2.31 | 2.46 ± 3.36 | 0.924a | |
| Oral amino acid-based supplement | 3.71 ± 2.05 | - | - | |
| Other foods and beverages | 3.02 ± 1.41 | 2.95 ± 1.72 | 0.600a | |
| Vitamin B1 (mg): | Total | 0.79 ± 0.24 | 0.56 ± 0.30 | < 0.001a |
| Milk substitutes | 0.12 ± 0.18 | 0.15 ± 0.16 | 0.476a | |
| Oral amino acid-based supplement | 0.28 ± 0.15 | - | - | |
| Other foods and beverages | 0.38 ± 0.19 | 0.42 ± 0.32 | 0.945a | |
| Vitamin B2 (mg): | Total | 1.21 ± 0.35 | 0.78 ± 0.50 | 0.002b |
| Milk substitutes | 0.22 ± 0.27 | 0.38 ± 0.48 | 0.382a | |
| Oral amino acid-based supplement | 0.53 ± 0.29 | - | - | |
| Other foods and beverages | 0.40 ± 0.20 | 0.36 ± 0.26 | 0.229a | |
| Niacin (mg): | Total | 11.65 ± 3.31 | 8.55 ± 3.09 | 0.002b |
| Milk substitutes | 1.50 ± 2.31 | 1.54 ± 1.94 | 0.684a | |
| Oral amino acid-based supplement | 2.49 ± 1.38 | - | - | |
| Other foods and beverages | 6.95 ± 3.19 | 6.52 ± 2.78 | 0.619b | |
| Vitamin B6 (mg): | Total | 0.82 ± 0.27 | 0.64 ± 0.43 | 0.004a |
| Milk substitutes | 0.16 ± 0.22 | 0.20 ± 0.21 | 0.333a | |
| Oral amino acid-based supplement | 0.28 ± 0.15 | - | - | |
| Other foods and beverages | 0.32 ± 0.17 | 0.41 ± 0.40 | 0.867a | |
| Vitamin B12 (mcg): | Total | 3.78 ± 1.63 | 3.28 ± 4.16 | 0.011a |
| Milk substitutes | 0.47 ± 0.52 | 0.88 ± 1.20 | 0.361a | |
| Oral amino acid-based supplement | 1.04 ± 0.58 | - | - | |
| Other foods and beverages | 2.11 ± 1.48 | 2.30 ± 4.06 | 0.132a | |
| Folic acid (mcg): | Total | 326.6 ± 67.0 | 226.9 ± 81.8 | < 0.001b |
| Milk substitutes | 25.3 ± 27.5 | 31.5 ± 32.9 | 0.644a | |
| Oral amino acid-based supplement | 82.8 ± 45.8 | - | - | |
| Other foods and beverages | 206.7 ± 71.9 | 188.1 ± 78.2 | 0.262a | |
| Vitamin C (mg): | Total | 272.0 ± 361.8 | 176.1 ± 203.1 | 0.113a |
| Milk substitutes | 16.1 ± 26.2 | 25.0 ± 36.1 | 0.466a | |
| Oral amino acid-based supplement | 26.1 ± 14.4 | - | - | |
| Other foods and beverages | 211.7 ± 371.2 | 143.0 ± 191.0 | 0.929a | |
| Vitamin C provided by other supplements | 18.2 ± 41.1 | 8.0 ± 25.4 | 0.221a | |
aMean values and standard deviation (Mann–Whitney U test); bmean values and standard deviation (Student’s t-test). The consumption of vitamins provided by supplements of vitamins E, B1, B2, B6, and B12, niacin, and folic acid was similar between the groups. Their data are not presented due to the low number of children who consumed these supplements (< 10). However, the total daily intake included the supply of these vitamins through these supplements.
Discussion
This study assessed the effectiveness of a nutritionally complete oral supplement containing amino acids in the diet of preschoolers on cow’s milk elimination diet because of CMPA associated or not to allergy to other food(s). The oral supplement was used as recommended by their physicians and in accordance with standard community practices. The use of a complete oral amino acid-based supplement was associated with increased intake of energy, proteins, carbohydrates, lipids, calcium, iron, zinc, vitamin D, and other micronutrients. The intake of amino acid-based supplement was also associated with a higher proportion of children within the recommendations for energy, carbohydrates, and various minerals and vitamins.
Cow’s milk protein allergy is caused due to different immunological mechanisms (Immunoglobulin E [IgE], non-IgE, and mixed) and has a wide spectrum of clinical manifestations. Depending on the mechanisms and clinical manifestation, different nutritional consequences and different probabilities subsist for the early development of oral tolerance. However, elimination of allergenic protein(s) from the diet is the most important treatment for all types of CMPA in infants and preschoolers. Ideally, elimination diets must be free of residual allergenic epitopes and must fulfill all nutritional requirements. In real life, patients may have a dietary improvement by receiving oral supplements of amino acids, as demonstrated in our study.
The study participants were recruited from all Brazilian geographical regions. Boys dominated the study, similar to other studies with pediatric patients with CMPA.9,11,13,16 The high proportion of cesarean and premature births was similar to another study conducted with Brazilian infants.30 In the present study, the average BMI-for-age z-scores of the children in the study group were approximately 1.0 SD lower than of the control group. Weight deficit could be one of the reasons for physicians to prescribe complete oral amino acid-based supplement for patients with food allergies.31 Deficit in height-for-age was the more frequent anthropometric impairment described in CMPA.1,10,11,14 However, in this study, the height-for-age z scores were similar to the reference values. This finding could be explained if the elimination diet for CMPA treatment is being indicated earlier in the present32 than in the past,1,10,11,14 reducing the negative effect of a delayed nutritional treatment of CMPA on growth. This hypothesis should be evaluated in the future studies.
Another nutritional effect observed in food allergies, besides anthropometric deficits, which may require the prescription of complete oral supplements, is low intake of energy, minerals, and vitamins. Therefore, a complete oral nutritional supplement is typically prescribed to children at nutritional risk because of diseases that result in insufficient nutrient intake and/or impaired weight and height.31 Children with food allergies may have a low intake of energy, macronutrients, and various micronutrients, such as calcium, zinc, iron, vitamins A, D, and B complex, and folic acid.10–12 The risk of deficiencies in these micronutrients has been documented as well. However, a deficiency status is not always associated with low intake.10 In this context, data from the control group of the present study are consistent with the literature and reveal high proportion of inadequate intake of energy (59.2%), calcium (85.3%), phosphorus (50.0%), iron (47.1%), selenium (79.4%), vitamins A (44.1%), D (82.3%), E (64.7%), B1 (52.9%), B2 (38.2%), and B6 (47.1%), and niacin (29.4%). The study group, in turn, demonstrated higher intake of energy, macronutrients, and micronutrients. Increase in dietary intake of these nutrients was mainly due to the consumption of oral amino acid-based supplement, as intake from other food sources was similar between groups for all nutrients evaluated, except for proteins.
This suggests that consuming a complete oral amino acid-based supplement does not result in sufficient satiety to reduce the intake of other foods and beverages, which can be a concern when prescribing a dietary supplement. Similar results were observed in two recent clinical trials that evaluated preschoolers with picky eating but no food allergies. A study conducted in Brazil demonstrated an increase in appetite after the children were provided a complete oral nutritional supplement.33 In India, consumption of an oral nutritional supplement improved the nutritional adequacy of children without interfering with regular food consumption patterns.34
Another indication for complete oral nutritional supplements is feeding difficulties.31,33–38 Studies have demonstrated that children with food allergies may experience higher levels of feeding difficulties.10,15–17 Possible causes of feeding difficulties in children with CMPA may include limited food options because of multiple dietary restrictions, delayed introduction of new foods and textures, and reduced enjoyment of eating because of pain and discomfort caused by CMPA manifestations.10,15–17 In the present study, the frequency of feeding difficulties assessed by the Montreal Children’s Hospital Feeding Scale was higher in the study group (26.7%), compared to the control group (19.4%), but the difference was not statistically significant (P = 0.706). The prevalence of feeding difficulties according to the Montreal Children’s Hospital Feeding Scale18 in both groups of this study matched those of another study conducted in Brazil.16 The long-term effect of using a complete oral amino acid-based supplement on the nutritional parameters and body composition of children on an elimination diet because of CMPA should be evaluated in the future studies as evaluated in picky eaters without food allergy.33
One of the strengths of the present study was the inclusion of children with CMPA from all geographic regions of the country who were being treated by their respective pediatricians, reflecting real-life standard care. Another strength of the study was the evaluation of nutrient intake that was conducted blindly for four components of the 24-h food record (cow’s milk substitutes, complete oral amino acid-based supplement, other foods and beverages, and mineral and/or vitamin supplements). Therefore, the dietary surveys were calculated without knowing the identity or group of included patients. In spite of the high risk of nutritional deficiencies in patients with food allergy,10 the present study was the first to evaluate the effectiveness of using a complete oral nutritional supplement.
One limitation of this study was that a smaller number of children than planned were recruited for the study group. However, notably, the sample size was sufficient to demonstrate the nutritional relevance of oral amino acid supplement for improving the quality of the diet, with statistically significant difference for the main nutritional parameters. One-third of the patients (data not shown) were not included in the study because they were breastfeeding, demonstrating that several Brazilian mothers recognized the importance of natural breastfeeding even after the first year of birth.
Conclusions
Preschoolers on cow’s milk elimination diet demonstrated increased intake of energy, macronutrients, calcium, iron, vitamins, and minerals when receiving a nutritionally complete oral amino acid-based supplement. The use of the oral amino acid-based supplement had a positive effect on the quality of diet without reducing the intake of nutrients from other foods and beverages. The future prospective studies should evaluate the long-term effects of using a complete oral amino acid-based supplement on the body composition of children on an elimination diet.
Declaration of interest
Adriana Sanudo, Vanessa Cristina de Castro Rodrigues, and Mauro Batista de Morais received personal fees to develop this study. Thaysa Maués Cezar works the Medical Affairs Division of Danone Nutricia Brazil, and Camila Leonel Mendes de Abreu was working in the Medical Affairs Division of Danone Nutricia Brazil when this study was developed.
Acknowledgments
The authors acknowledge Milena Guimarães de Campos Amado Ferreira de Mello, Giovanna Albuquerque Rufo, and Renata Lucats Fidalgo for their contribution to the development of this study and Danone Nutricia Brazil for financing the project.
REFERENCES
1. Vieira MC, Morais MB, Spolidoro JVN, Toporovski MS, Cardoso AL, Araujo GTB, et al. A survey on clinical presentation and nutritional status of infants with suspected cow’ milk allergy. BMC Pediatr. 2010;10:25. 10.1186/1471-2431-10-25
2. Savage J, Johns CB. Food allergy: Epidemiology and natural history. Immunol Allergy Clin North Am. 2015;35:45–59. 10.1016/j.iac.2014.09.004
3. Vandenplas Y, Broekaert I, Domellöf M, Indrio F, Lapillonne A, Pienar C, et al. An ESPGHAN position paper on the diagnosis, management and prevention of cow’s milk allergy. J Pediatr Gastroenterol Nutr. 2023. 10.1097/MPG.0000000000003897. Online ahead of print.
4. Toca MC, Morais MB, Vásquez-Frias R, Becker-Cuevas DJ, Boggio-Marzet CG, Delgado-Carbajal L, et al. Consensus on the diagnosis and treatment of cow’s milk protein allergy of the Latin American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Rev Gastroenterol Mex (Engl Ed). 2022; 87:235–50. 10.1016/j.rgmxen.2022.01.002. Epub May 24, 2022.
5. Solé D, Silva LR, Cocco RR, Ferreira CT, Sarni RO, Oliveira LC, et al. Brazilian consensus on food allergy: 2018—Part 2—Diagnosis, treatment and prevention. Joint Position Paper of the Brazilian Society of Pediatrics and the Brazilian Association of Allergy and Immunology. Arq Asma Alerg Imunol. 2018;2: 39–82. 10.5935/2526-5393.20180005
6. Meyer R, Venter C, Bognanni A, Szajewska H, Shamir R, Nowak-Wegrzyn A, et al. World Allergy Organization (WAO) Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA) Guideline update—VII—Milk elimination and reintroduction in the diagnostic process of cow’s milk allergy. World Allergy Organ J. 2023;16:100785. 10.1016/j.waojou.2023.100785. eCollection July 2023.
7. Dias A, Santos A, Pinheiro JA. Persistence of cow’s milk allergy beyond two years of age. Allergol Immunopathol (Madr). 2010;38:8–12., 10.1016/j.aller.2009.07.005. Epub Oct 22, 2009.
8. Prescott S, Allen KJ. Food allergy: Riding the second wave of the allergy epidemic. Pediatr Allergy Immunol. 2011;22: 155–60. 10.1111/j.1399-3038.2011.01145.x
9. de Faria DPB, Sillos MD, Speridião PGL, Morais MB. Outcome of food intake and nutritional status after discontinuation of a cow’s-milk-free diet post negative oral food challenge in infants and children. Allergol Immunopathol (Madr). 2022;50:1–8. 10.15586/aei.v50i1.471
10. Meyer R. Nutritional disorders resulting from food allergy in children. Pediatr Allergy Immunol. 2018;29:689–704. 10.1111/pai.12960
11. Medeiros LC, Speridião PG, Sdepanian VL, Fagundes-Neto U, Morais MB. Nutrient intake and nutritional status of children following a diet free from cow’s milk and cow’s milk by--products. J Pediatr (Rio J). 2004;80:363–70. https://pubmed.ncbi.nlm.nih.gov/15505731/
12. Boaventura RM, Mendonça RB, Fonseca FA, Mallozi M, Souza FS, Sarni ROS. Nutritional status and food intake of children with cows’milk allergy. Allergol Immunopathol (Madr). 2019;47:544–50. 10.1016/j.aller.2019.03.003
13. de Faria DPF, Sillos MD, Speridião PGL, Morais MB. Real-life data on the effectiveness of extensively hydrolyzed protein-based formula and amino acid-based formula in regaining weight and height in infants on a cow’s milk protein elimination diet. Allergol Immunopathol (Madr). 2023 Mar 1;51(2): 177–83. 10.15586/aei.v51i2.768. eCollection 2023. https://all-imm.com/index.php/aei/article/view/768
14. Meyer R, Wright K, Vieira MC, Chong KW, Chatchatee P, Vlieg-Boerstra BJ, et al. International survey on growth indices and impacting factors in children with food allergies. J Hum Nutr Diet. 2019;32:175–84. 10.1111/jhn.12610
15. Meyer R, Rommel N, Van Oudenhove L, Fleming C, Dziubak R, Shah N. Feeding difficulties in children with food protein--induced gastrointestinal allergies. J Gastroenterol Hepatol. 2014;29:1764–9. 10.1111/jgh.12593
16. Rodrigues VCC, Speridião PGL, Sanudo A, Morais MB. Feeding difficulties in children fed a cows’ milk elimination diet. Br J Nutr. 2022;128:1190–9. 10.1017/s0007114521004165
17. Maslin K, Dean T, Arshad SH, Venter C. Fussy eating and feeding difficulties in infants and toddlers consuming a cows’ milk exclusion diet. Pediatr Allergy Immunol. 2015;26:503–8. 10.1111/pai.12427
18. Ramsay M, Martel C, Porporino M, Zygmuntowicz C. The Montreal Children’s Hospital Feeding Scale: A brief bilingual screening tool for identifying feeding problems. Paediatr Child Health 2011;16:147–51. 10.1093/pch/16.3.147
19. Diniz PB, Fagondes SC, Ramsay M. Cross-cultural adaptation and validation of the Montreal Children’s Hospital Feeding Scale into Brazilian Portuguese. Rev Paul Pediatr. 2021;39:e2019377. 10.1590/1984-0462/2021/39/2019377
20. Gibson RS, Ferguson EL. An interactive 24-hour recall for assessing the adequacy of iron and zinc intakes in developing countries. HarvestPlus Technical Monograph 8. Washington, DC International Food Policy Research Institute (IFPRI) and International Center for Tropical Agriculture (CIAT). © HarvestPlus; 2008, 157 p. https://ebrary.ifpri.org/digital/collection/p15738coll2/id/128218
21. Crispim SP, Kac G, Lacerda EMA, Castro IRR. Manual fotográfico de quantificação alimentar infantil. Curitiba, Brazil: Universidade Federal do Paraná; 2018, 160 p.
22. Pinheiro ABV, Lacerda EMA, Benzecry EH, Gomes MCS, Costa VM. Tabela Para Avaliação de consumo alimentar em medidas caseiras, 5th ed. Rio de Janeiro, Brazil: Atheneu; 2004, 131 p.
23. National Academies of Sciences, Engineering, and Medicine. Dietary reference intakes for sodium and potassium. Washington, DC: The National Academies Press; 2019. 10.17226/25353
24. Food and Agriculture Organization/World Health Organization/United Nations University (FAO/WHO/UNU). Human energy requirements. Report of a Joint FAO/WHO/UNU Expert Consultation. Food and Nutrition Technical Report Series 1. Rome, Italy: FAO; 2004. Available from: https://www.fao.org/3/y5686e/y5686e00.htm#Contents
25. Williams CL, Bollella M, Wynder EL. A new recommendation for dietary fiber in childhood. Pediatrics. 1995;96:985–88. https://pubmed.ncbi.nlm.nih.gov/7494677/
26. Brazilian Food Composition Data Network. Tabela Brasileira de Composição de Alimentos (TBCA), Versão 7.2. São Paulo, Brazil: Universidade de São Paulo (USP) and Food Research Center (FoRC); 2023. Available from: http://www.fcf.usp.br/tbca
27. Brazilian Institute of Geography and Statistics (IBGE). Estudo Nacional de Despesa Familiar (National Study on Family Expenditures; ENDEF). Tabelas de composição de alimentos, 5th ed. Rio de Janeiro, Brazil: IBGE; 1999, 137 p. Available from: ,https://biblioteca.ibge.gov.br/visualizacao/livros/liv6934.pdf
28. Center for Studies and Research in Food of the State University of Campinas (NEPA–UNICAMP). Tabela Brasileira de composição de alimentos (TACO), 4th ed. Campinas, Brazil: NEPA–UNICAMP; 2011, 161 p. Available from: https://www.nepa.unicamp.br/taco/tabela.php?ativo=tabela
29. US Department of Agriculture, Agricultural Research Service. Food Data Central, 2019. Available from: https://fdc.nal.usda.gov/
30. Morais MB, Toporovski MS, Tofoli MHC, Barros KV, Ferreira CHT, Silva LR. Breastfeeding in infants seen in private pediatric practices and its relation with type of delivery and history of prematurity. J Pediatr (Rio J). 2022;98:241–7. 10.1016/j.jped.2021.06.009
31. Braegger C, Decsi T, Dias JA, Hartman C, Kolacek S, Koletzko B, et al. Practical approach to paediatric enteral nutrition: A comment by the ESPGHAN committee on nutrition. J Pediatr Gastroenterol Nutr. 2010;51:110–22. 10.1097/mpg.0b013e3181d336d2
32. Frizzo J, Rodrigues VCC, Speridião PGL, Morais MB. Evaluation of the complementary feeding practices, dietary intake, and nutritional status of infants on a cow’s milk protein elimination diet. J Pediatr (Rio J). 2022;98:256–63. 10.1016/j.jped.2021.06.005
33. Nogueira-de-Almeida CA, Del Ciampo LA, Martinez EZ, Contini AA, Nogueira-de-Almeida ME, Ferraz IS, et al. Clinical evolution of preschool picky eater children receiving oral nutritional supplementation during six months: A prospective controlled clinical trial. Children. 2023;10:495. 10.3390/children10030495
34. Anwar F, Yalawar M, Suryawanshi P, Ghosh A, Jog P, Khadilkar AV, et al. Effect of oral nutritional supplementation on adequacy of nutrient intake among picky-eating children at nutritional risk in India: A randomized double-blind-clinical trial. Nutrients. 2023;15:2528. 10.3390/nu15112528
35. Nogueira-de-Almeida CA, Mello ED de, Ribas Filho D, Maximino P, Fisberg M. Consensus of the Brazilian Association of Nutrology on the use of food supplements to children with eating disorders. IJN 2022;11:4–15. 10.1055/s-0038-1670717
36. Ghosh AK, Kishore B, Shaikh I, Satyavrat V, Kumar A., Shah, T., et al. Effect of oral nutritional supplementation on growth and recurrent upper respiratory tract infections in picky eating children at nutritional risk: A randomized, controlled trial. J Int Med Res. 2018;46:2186–201. 10.1177/0300060518757355
37. Ghosh AK, Kishore B, Shaikh I, Satyavrat V, Kumar A, Shah T, et al. Continuation of oral nutritional supplementation supports continued growth in nutritionally at-risk children with picky eating behaviour: A post-intervention, observational follow-up study. J Int Med Res. 2018;46:2615–32. 10.1177/0300060518766982
38. Sheng X, Tong M, Zhao D, Leung TF, Zhang F, Hays NP, et al. Randomized controlled trial to compare growth parameters and nutrient adequacy in children with picky eating behaviors who received nutritional counseling with or without an oral nutritional supplement. Nutr Metab Insights. 2014;7:85–94. 10.4137/nmi.s15097