
Download
ORIGINAL ARTICLE
Managing children with frequent respiratory infections and associated wheezing: a preliminary randomized study with a new multicomponent nasal spray
Maria Angela Toscaa, Attilio Varricchiob, Irene Schiavettic, Matteo Nasoa, Valerio Damianid, Giorgio Ciprandie*
aAllergy Center, IRCCS Istituto Giannina Gaslini, Genoa, Italy
bENT Department, University of Molise, Campobasso, Italy
cHealth Science Department, University of Genoa, Italy
dMedical Department, D.M.G., Pomezia, Italy
eAllergy Clinic, Casa di Cura Villa Montallegro, Genoa, Italy
Abstract
Background: Preschoolers frequently have respiratory infections (RIs), which may cause wheezing in some subjects. Type 2 polarization may favor increased susceptibility to RIs and associated wheezing. Non-pharmacological remedies are garnering increasing interest as possible add-on therapies. The present preliminary study investigated the efficacy and safety of a new multi-component nasal spray in preschoolers with frequent RIs and associated wheezing.
Methods: Some preschoolers with these characteristics randomly took this product, containing lactoferrin, dipotassium glycyrrhizinate, carboxymethyl-beta-glucan, and vitamins C and D3 (Saflovir), two sprays per nostril twice daily for 3 months. Other children were randomly treated only with standard therapy. Outcomes included the number of RIs and wheezing episodes, use of medications, and severity of clinical manifestations.
Results: Preschoolers treated add-on with this multicomponent product experienced fewer RIs and used fewer beta-2 agonists than untreated children (P = 0.01 and 0.029, respectively).
Conclusions: This preliminary study demonstrated that a multicomponent product, administered add-on as a nasal spray, could reduce the incidence of RIs and use of symptomatic drugs for relieving wheezing in children.
Key words: beta-glucans, glycyrrhetic acid, lactoferrin, medications’ use, preschoolers, respiratory infections, symptoms, vitamin C, vitamin D3, wheezing
*Corresponding author: Giorgio Ciprandi, Allergy Clinic, Casa di Cura Villa Montallegro, 16145 Genoa, Italy. Email address: [email protected]
Received 15 November 2023; Accepted 5 February 2024; Available online 1 May 2024
Copyright: Tosca M.A., et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Children often get sick, especially by contracting respiratory infections (RIs). This heightened susceptibility to infection depends on the relative weakness of the immune system1, that is, the immune system requires some years to become strong. As a result, the first years of life are characterized by a partial immaturity of immunity that makes children prone to have various infections. Moreover, RIs significantly affect morbidity, healthcare burden, overmedication (mostly with antibiotics), and quality of life of both child and family. In addition, some children present a particularly pronounced predisposition to have frequent RIs.2,3 This susceptibility subtends some risk factors, such as early age, nursery school attendance, exposure to a relevant quantity of indoor and outdoor pollutants, second-hand smoke, poor economic conditions, and allergic disorders.4 In this regard, allergy represents an intriguing risk factor. As mentioned above, the immune system is weak in the early childhood, as it is oriented toward type 2 immunity. This type 2 polarization has a finalistic reason. The fetus is per se a non-self-antigen for the mother, hence to avoid maternal rejection, the fetus grows in a protective environment, such as type 2-oriented environs.4 However, the type 2 polarization entails defective type 1 immunity, typically deputed to fight infections. These phenomena explain the sustained susceptibility to infections in the childhood.
Moreover, acute RIs represent a common cause of wheezing in some preschoolers.5 Wheezing is an acute and continuous sound emitted from the thorax, not only during exhalation but also during inhalation. It is caused by the narrowing of intrathoracic (inferior) airway and is characterized by limited expiration.6 Preschool wheezing is frequent, as about one-third of European and the US children, aged 1–6 years, had wheezing in the preceding 6 months, and almost 50% of children had reported at least one wheezing episode in the first 6 years of life.7 A wheezing episode usually follows an acute viral RI.8 In particular, the number of previous wheezing attacks is a relevant risk factor for further wheezing episodes.9 Consequently, preventing RIs and associated wheezing episodes could be an attractive perspective in managing preschoolers in clinical practice. Many products have been tested in this regard, including probiotics, food supplements, vitamins, oligo--elements, thermal water, and drugs.10–16
Recently, a new multicomponent medical device has been introduced (Saflovir). This product is administered as a nasal spray and contains lactoferrin (LF), dipotassium glycyrrhizinate, carboxymethyl-beta-glucan, and vitamins C and D3. This product exerts chelating and lubricant activities. In addition, this multicomponent product cleans and protects the nasal cavity from external agents, including viruses and bacteria.
A previous in vitro study demonstrated that this product inhibited the growth of P. aeruginosa; thus, it has been proposed that it could be used to prevent respiratory nasal infections.17
On the other hand, it is underlined that the real-life management of RIs in children is a common burden by excessive use of medications. In this regard, even if frequently inappropriate (most infections are caused by viral agents), antibiotics are prescribed in children with acute RI. In addition, a symptomatic treatment is usually used to relieve the irritating symptoms associated with acute infections, such as fever, malaise, headache, and myalgia. Usually, nonsteroidal anti-inflammatory drugs (NSAIDs) are used to hinder these symptoms. Nasal obstruction is an irritating ailment that could significantly affect or disturb the child. Allergic children mainly suffer from this phenomenon. Thus, antihistamines are prescribed to decrease the intensity of nasal obstruction.
If wheezing appears during an acute RI, it requires an adequate therapy, which includes inhaled and/or oral corticosteroids and bronchodilators, namely short-acting beta-2 agonists (SABAs).
Moreover, it has to be emphasized that children with acute RIs are not able to attend nursery school. Consequently, the parents are also often absent from working.
Therefore, based on these considerations, this preliminary study was designed to demonstrate the effectiveness and safety of this product in preventing RIs and associated wheezing in a limited group of preschoolers.
Materials and Methods
The present study, with randomized and controlled design, explored the possible prevention of RIs in preschoolers with frequent RIs and associated wheezing.
As this was a preliminary study, the number of enrolled subjects was limited to 15 per arm.
The inclusion criteria were as follows: (i) aged between 2 and 6 years, (ii) both genders, and (iii) history of frequent RIs (at least six RIs) and associated wheezing episodes (at least two episodes) in the past year. The exclusion criteria were as follows: (i) congenital or acquired immunodeficiency, (ii) craniofacial abnormalities, (iii) sleep apnea syndrome, (iv) Down’s syndrome, (v) chronic disease (including metabolic disorders, cystic fibrosis, cancer, etc.), (vi) clinically relevant passive smoking, and (vii) previous (last 3 months) or current administration of drugs that could have interfered the study (e.g., immunomodulators, probiotics, vitamins, oligo-elements, or systemic corticosteroids for at least 2 consecutive weeks).
The local Ethics Committee (IGG) approved the study in the context of prevention and control of bronchial obstruction (No.: 22253/2017). Parents signed an informed consent.
All children were treated with standard treatment for any infection during the study period. As the children were managed by their primary care physicians for acute infections, antibiotics and NSAIDs were chosen and prescribed by these medicos. Accordingly, symptomatic treatments for respiratory complaints, mainly concerning wheezing and nasal obstruction, were determined by primary care pediatricians.
The children were randomly (ratio 1:1) and consecutively subdivided into two groups at baseline. The first group, considered the active group, was treated with Saflovir, two sprays per nostril twice daily for 3 months. The second group, considered the control group, was treated only if required for RIs and wheezing episodes with the standard therapy.
Saflovir is a medical device containing lactoferrin (1%), dipotassium glycyrrhizinate (2.5%), carboxymethyl-beta-glucan (0.2%), vitamins C and D3, and dexpantenol (3.5%). These components are diluted in a buffered solution at pH 7.2. The device contains 20-mL solution and is available as a nasal spray.
The primary outcome was the number of RIs observed globally during the study period. RI was diagnosed based on the symptoms reported by the parents as defined previously in detail.18 The diagnosis of RI was made when at least two symptoms or fever (axillary temperature > 38°C), in addition to one other symptom as mentioned below, were present for at least 48 h. The symptoms were mucopurulent rhinorrhea, stuffy or dripping nose or both, sore throat, cough (dry or productive), otalgia, fever, dyspnea, and mucopurulent phlegm. RI was classified as upper respiratory infection (URI), such as common cold, rhinosinusitis, pharyngitis, otitis, laryngitis, or lower respiratory infection (LRI), such as tracheitis, bronchitis, and pneumonia.
Secondary outcomes were as follows: (i) number of wheezing episodes during the study period, (ii) use of required medications, such as antibiotics, inhaled and oral corticosteroids, Beta-2 agonists, NSAIDs, antihistamines, (iii) nasal obstruction intensity, and (iv) perception of severity of symptoms.
The use of medications was scored as absent (0), rare (1), or for each infection (2).
Parents and physicians assessed the perception of severity of symptoms using visual analog scale (VAS) according to the methods described in a previous study.19 Similarly, sleep quality was measured by parents using VAS.
Visual analog scale is a psychometric measure used widely in many diseases. In particular, VAS evaluates the subjective perception of a symptom and reflects the point of view of the patient. This scale consists of one ruler involving symptom perception.19 In this study, VAS was a 10-cm vertical segment on which 0 implied the most severe respiratory symptoms, while 10 accorded to no respiratory symptoms. Initially, parents were instructed to put a mark on the line indicating their symptom perception at that moment. Thus, the lower the numerical score the patient (or doctor) marks, the greater the perceived severity of symptoms. With a movable marker, the parent or doctor could mark any point on the 10-cm segment that best described his/her perception of severity of symptoms. No interval marker was visible on the line. Therefore, the VAS score ranged from 10 (no symptoms) to 0 (worst symptoms).
The study was conducted between September 2022 and June 2023.
As this study was designed as a pilot content, the sample size was not determined. Any pre- or post- differences in each variable within the group were assessed using Wilcoxon’s signed rank test. Mann–Whitney U-test was used to identify any differences in the change of each variable over time between the two groups. All analyses were performed using SPSS® version 25.0 (IBM Corp., Armonk, NY, USA).
Results
The present study included 30 children: 15 in the Saflovir group (seven females and eight males, mean age: 3.7+1.16 years) and 15 in the control group (eight females and seven males, mean age: 3.5+1.06 years). All children attended pre-schools, so exposure to microbes was homogenous.
Table 1 summarizes the investigated parameters of both groups in the past and present years.
Table 1: Clinical data in treated and untreated children in previous and current years.
| Control group (N = 15)a | Saflovir group (N = 15) | Comparison between groups | |||||
|---|---|---|---|---|---|---|---|
| Past year | Present year | P | Past year | Present year | P | ||
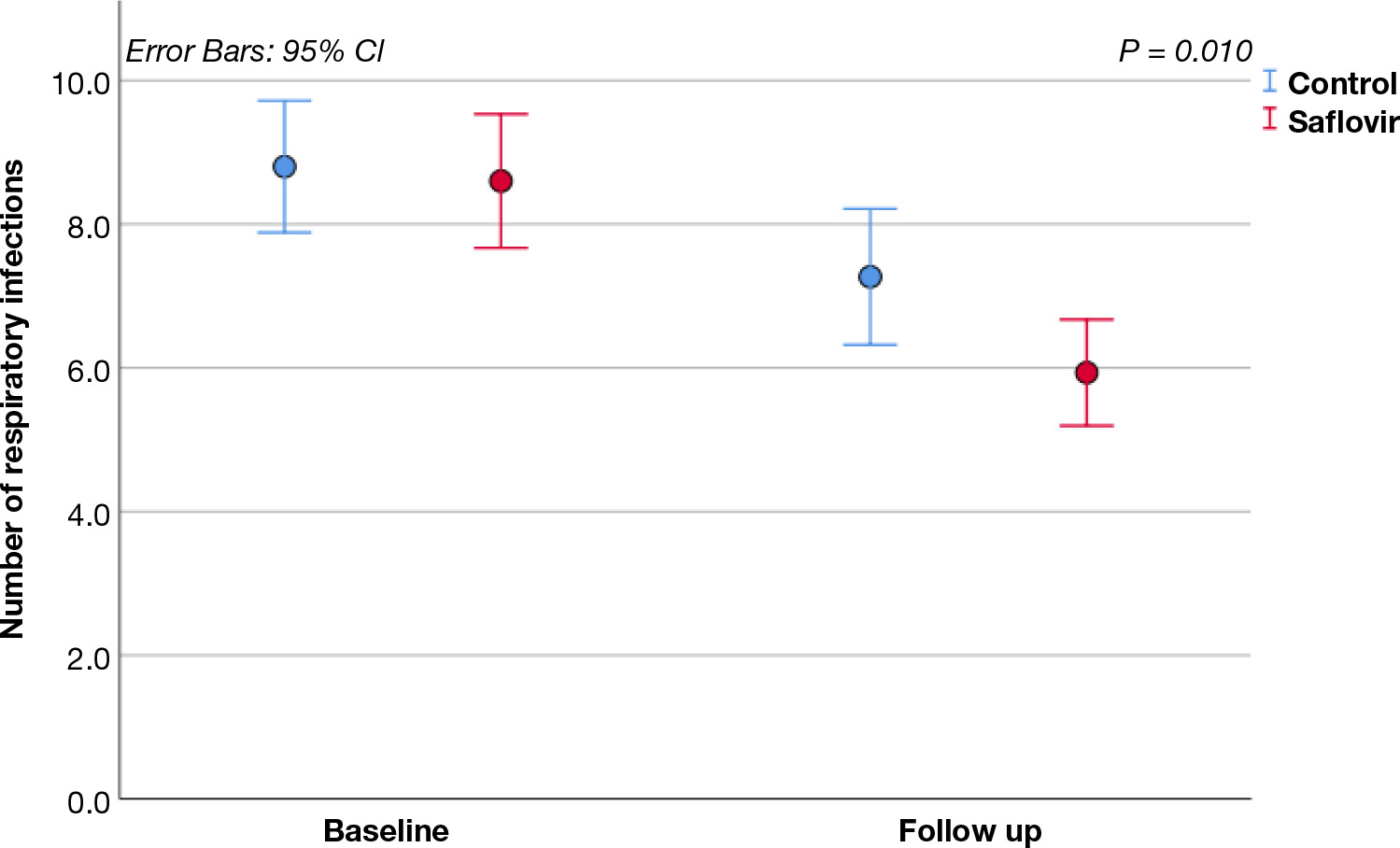
| Number of respiratory infections | 9.0 (8.0–10.0) | 8.0 (6.0–8.0) | < 0.001* | 9.0 (7.0–10.0) | 6.0 (5.0–7.0) | 0.001* | 0.01* |
| Number of wheezing episodes | 5.0 (3.0–7.0) | 4.0 (3.0–5.0) | 0.02* | 5.0 (2.0–8.0) | 4.0 (2.0–4.0) | 0.01* | 0.62 |
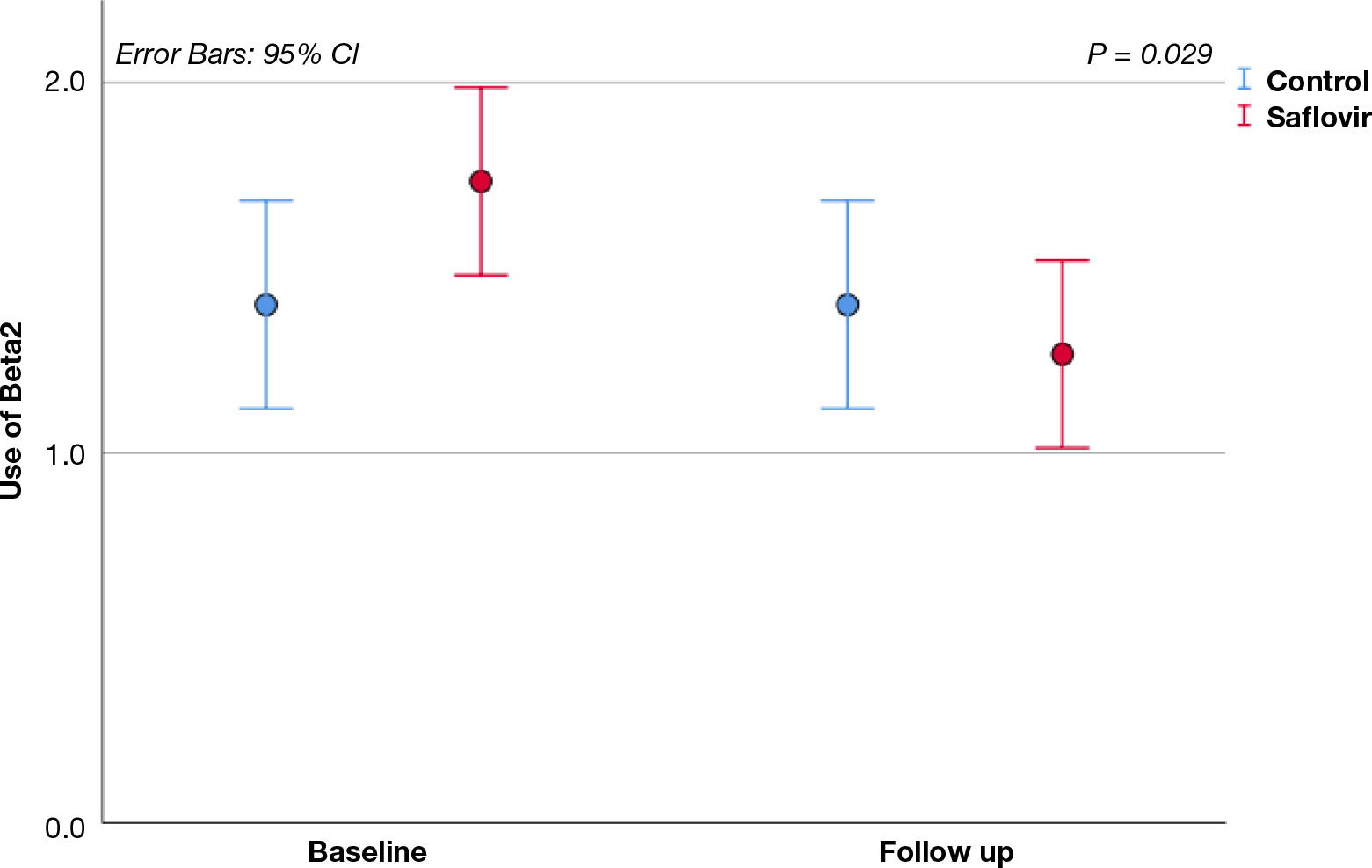
| Beta 2-agonist use | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.99 | 2.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.01* | 0.03* |
| Inhaled corticosteroids use | 2.0 (1.0–3.0) | 2.0 (1.0–2.0) | 0.10 | 2.0 (2.0–3.0) | 2.0 (1.0–2.0) | 0.01* | 0.29 |
| Oral corticosteroids use | 1.0 (0.0–2.0) | 1.0 (0.0–1.0) | 0.26 | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) | 0.08 | 0.90 |
| Antibiotic use | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) | 0.16 | 1.0 (0.0–1.0) | 0.0 (0.0–1.0) | 0.046* | 0.54 |
| NSAIDs useb | 1.0 (1.0 –2.0) | 1.0 (1.0–1.0) | 0.32 | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 0.16 | 0.78 |
| Antihistamine use | 1.0 (0.0 –1.0) | 1.0 (0.0–2.0) | 0.32 | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) | 0.32 | 0.57 |
| Nasal obstruction | 1.0 (1.0 –2.0) | 2.0 (1.0–2.0) | 0.41 | 1.0 (1.0–2.0) | 1.0 (1.0–2.0) | 0.046* | 0.13 |
| Parents’ VASc | 8.0 (6.0 –8.0) | 8.0 (7.0–8.0) | 0.41 | 7.0 (6.0–9.0) | 8.0 (8.0–9.0) | 0.01* | 0.27 |
| Doctors’ VAS | 7.0 (7.0 –8.0) | 7.0 (7.0–8.0) | 0.046* | 7.0 (6.0–8.0) | 8.0 (7.0–9.0) | 0.01* | 0.12 |
| Sleeping VAS | 7.0 (6.0 –8.0) | 7.0 (6.0–8.0) | 0.99 | 7.0 (6.0–8.0) | 8.0 (7.0–8.0) | 0.02* | 0.07 |
aNumber, bnonsteroidal anti-inflammatory drugs (NSAIDs), cVisual analog scale (VAS), *Statistically Significant.
Intragroup analysis
Patients in the control group experienced significantly fewer RI and wheezing episodes in the current year. The doctors’ perception of severity of symptoms was more favorable in the current year than in the previous one.
Saflovir therapy induced a significantly less number of RIs and wheezing episodes as well as less use of Beta-2 agonists, inhaled corticosteroids, and antibiotics. In addition, the use of Saflovir is associated with less intense nasal obstruction. Finally, Saflovir improved the perceptions detected by parents and doctors concerning intensity of symptoms; accordingly, the sleep quality perception improved significantly.
Intergroup analysis
The comparison between groups showed a significant effect of Saflovir on the number of RIs (Figure 1) and the use of Beta-2 agonists (Figure 2).
Figure 1 Number of respiratory infections in control and Saflovir groups in the past and current years.
Figure 2 Use of β2 agonists in control and Saflovir groups in the past and current years.
Safety
The tested product was well tolerated, and no clinically relevant adverse reactions were reported.
Discussion
Frequent RIs are a load for child, family, and society.20 Admittedly, children with acute RIs require adequate cure and expensive treatment, fail to attend their nursery school, and parents have to take care of their children and are consequently absent from work. Thus, it is evident that RIs display a relevant burden on direct and indirect expenditures.
Moreover, RIs in childhood constitute the leading cause for antibiotic prescription, even though frequently inappropriate, as most RIs are of viral origin.21 Accordingly, antibiotic abuse and overuse cause increased antibiotic resistance.22 Also, RIs are associated with frequent doctor and emergency room visits and parental work burden.23
A well-aimed innate and adaptive immunity guarantees an efficient response to pathogens. In addition, a well--functioning immune system assures microbial clearance and inflammation dampening.24 However, young children have not yet developed strong immunity and therefore have frequent respiratory tract infections.
Respiratory infections damage the mucosa and create local inflammation that promotes wheezing, such as bronchial obstruction, in predisposed children.
Modulating the immune system could be an intriguing option for preschoolers with frequent RIs and associated wheezing. A recent randomized controlled trial demonstrated that a probiotic mixture significantly reduced wheezing episodes in children.25 Reduced RIs were possible by using different products, such a elder extract, zinc, glucans, vitamin D3 (VD), resveratrol, palmitoyl ethanolamine, docosahexaenoic acid, and thermal water.11,13,15,16 Considerable interest was observed in developing new products that modulate the immune system in preventing RIs. In this regard, a new multicomponent nasal spray could be a valuable option.
Different components of Saflovir offer attractive clinical advantages.
Lactoferrin, at 1% concentration, is a polyfunctional glycoprotein present in external secretions, including saliva, droplets, milk, nasal, bronchial, and gastrointestinal secretions, and urine.
It is an important constituent of the neutrophilic granules of leukocytes.26 Interestingly, LF is an extremely multifaceted protein produced by vertebrates.27 It was identified in 1939 as a “red protein” in whey.28 In mammals, human and bovine milk represent the most abundant source of LF.29 Notably, concentration of LF in milk changes with form of lactation, that is, colostrums, the first form of breastmilk contains up to 8 mg/mL whereas mature milk (phase 3) contains about 2–3 mg/mL of LF.
From a biochemical point of view, LF is a glycosylated globular iron-binding protein captured through the sequestration of Fe2+ and Fe3+ free ions, therefore included in the metalloproteins family.30 Glandular epithelial cells and neutrophils, lymphocytes, and macrophages produce LF.31
However, LF is secreted profusely and rapidly during inflammatory effects.32 This extraordinary ability underlines its multitasking activities on metabolism, innate and adaptive immune response, infections (against bacteria, viruses, parasites, and fungi), oxidative events, inflammation, and tissue repair.32
Notably, LF modulates innate and adaptive immunity, mainly stimulating the maturation of the immune system during the first stages of life.30 Adequate LF intake assures the physiological plasticity of immune response and defends infections.26 In particular, LF activates antigen-allocation and B cells, modulating adaptive immune response by producing immunoglobulin G (IgG) and immunoglobulin A (IgA).33 In addition, LF enhances type 1 response and dampens type 2 inflammation.34
Lactoferrin down-regulates pro-inflammatory mediators, thereby facilitating in resolving acute inflammation.33,34 Thus, LF supplementation could provide beneficial anti-inflammatory effects.32
In addition, LF exerts a double antibacterial activity of being bacteriostatic and bactericidal. The bacteriostatic effect occurs by chelating Fe3+. On the other hand, the bactericidal activity takes place by disrupting the cellular wall of pathogens and increasing the permeability of membranes, resulting in bacterial death.27 LF counteracts bacterial adhesion to the enteric mucosa, thus reducing virulence.35 A recent randomized controlled trial (RCT) demonstrated that LF supplementation in anemic infants significantly reduced the morbidity of RIs and diarrhea.36 These findings were underscored by a meta-analysis of RCTs that supported LF fortification in infant formula and LF supplementation in managing patients with RIs.37
Beta-glucans (0.2%), natural polysaccharides with highly conserved structures, act as pathogen-associated molecular patterns (PAMPs).38 Glucans exert immunomodulatory activity, mainly on cellular immunity. Glucans recognize macrophages, monocytes, dendritic cells, and natural killer (NK) cells as primary target and modulate transcription factors and reduce the production of pro-inflammatory cytokines, such as IL-6, IL-8, and TNF-α39 Glucans support type 1 immune response by increasing interferon production, opposing the infections.40
Glycyrrhetic acid (GA) at 2.5%, the most active glycyrrhizin component, is a glycoside alkaloid present in glycyrrhiza glabra roots.41 GA inhibits the high-mobility group box 1 protein (HMGB1), an alarmin, and chemotactic and mitogenic functions without impeding DNA binding, thus making for relevant anti-inflammatory effects.42
Vitamin C is an antioxidant agent that counterpoints oxidative stress. Typically, vitamin C is helpful in infections, as activated phagocytes release an abundant quantity of oxidizing substances, such as reactive oxygen species.43 Moreover, vitamin C promotes interferon production, enhancing response to infective pathogens.44
Vitamin D3 is a hormone exerting pleiotropic effects, including anti-inflammatory activity.45 Many cell types express VD receptor (VDR) and enzyme 1α-hydroxylase, pivotal for its metabolism.45 Evidence shows that vitamin D deficiency is associated with increased incidence and severity of RI in children.46 Accordingly, low vitamin D (< 50 nmol/L) is an independent risk factor for unsatisfactory response to treatments and prolonged recovery from relevant lower RIs in children.47 Vitamin D supplementation positively modulates innate and adaptive immunity and opposes infections.48
Panthenol (3.5%) is a pro-vitamin of vitamin B5. Panthenol is a moisturizer and improves wound healing.49 Moreover, panthenol guarantees adequate mucosal hydration and reduces inflammatory processes.50
Consequently, this multicomponent product could be a reliable option for managing children with frequent RIs and associated wheezing, thanks to these multiple activities. The present preliminary study tested this hypothesis.
The findings of the present study showed that this adds-on strategy provided less RIs than the standard therapy alone. In addition, this product reduced the use of bronchodilators, an indirect marker of wheezing impact, and inhaled corticosteroids. Patients in the control group also experienced less RI episodes and wheezing attacks.
However, a possible explanation is the increased age. It is well known that RI susceptibility, and consequently wheezing episodes, is significantly reduced year after year.51
Interestingly, the intergroup analysis outlined a significant effect provided by the tested product on RIs, namely, patients in the active group experienced about one-third fewer infections compared to the previous year whereas patients in the control group had about 10% fewer infections. Conversely, the absolute number of wheezing episodes was superimposable between groups. However, using bronchodilators and inhaled corticosteroids was significantly inferior in the active group compared to the control group. This significant difference could mean that wheezing episodes were less clinically relevant because they required less use of symptomatic and anti-inflammatory drugs (bronchodilators and inhaled corticosteroids). Consistently, children in the active group used fewer antibiotics than used in the previous year whereas the antibiotic use in the control group did not change in the year of treatment.
In addition, the product slightly reduced the nasal obstruction score. This effect may depend on the decongestant characteristics exerted by GA because it effectively exerts anti-inflammatory activity as discussed above.
In addition, the relevance of symptoms, perceived by parents, improved significantly in adds-on-treated children alone. Similarly, physicians perceived a reduced burden of RIs in both groups, more evident in the active group. Finally, parents’ perception of children’s sleep improved in the active group only. As a result, these findings showed an interesting effect of multicomponent Saflovir on RIs and wheezing. Even if the significant intergroup difference only referred to the number of RIs and use of bronchodilators, this preliminary occurrence suggested that Saflovir improved response to infections. Unfortunately, no other study has investigated Saflovir in this application model. Only one study has evaluated this multicomponent medical device in children with allergic rhinitis.52 Hence, this pilot study demonstrated that Saflovir reduced the severity of nasal symptoms.
The results of the present study substantially confirmed previous studies on the RI model using non-pharmacological remedies. Indeed, non-pharmacological remedies effectively and safely provide a valuable option in managing children with frequent RIs as reported in the literature.11–16
Giannattasio and colleagues evaluated a cohort of 298 children with recurrent respiratory infections (RRI) in a real-world study conducted during the COVID-19 pandemic.11 A multicomponent food supplement (containing Sambucus nigra extract, β-glucan, zinc, and vitamin D3) was randomly prescribed to 160 children for daily use for 4 months, while the remaining 138 children with RRI were treated for RIs with standard therapy and considered as a control group. In the follow-up period, the prescribed multicomponent product had significantly reduced RI episodes distressing both upper and lower airways. Moreover, children treated with this food supplement experienced shorter RI duration during the treatment and follow-up, and their parents perceived less severe symptoms and better treatment efficacy. Finally, the prescribed product was well tolerated.
As reviewed recently, OM-85 (Broncho-Vaxom), an immunostimulant, displayed a robust evidence about its efficacy and safety in preventing RIs in children.12 In particular, this compound stimulated innate and type 1 immunity, thereby reinforcing the defense against microbial agents.
Another study conducted in a primary care investigated the preventive effects of a multicomponent product containing Lactobacillus rhamnosus GG ATCC 53103, docosahexaenoic acid (DHA), and vitamin D3.13 This study included 186 children with RRI. All children were treated with standard treatment for intercurrent infections. The children were stratified into two groups: 93 children were supplemented with the food supplement (1 mL/day to children aged up to 2 years and 2 mL/day to children aged >2 years) for 3 months consecutively. The remaining children were treated with a standard therapy. Children treated with the food supplement had less infections and less symptoms than the control children treated with a standard therapy. The supplementation was safe and well tolerated.
Another attractive option is represented by local bacteriotherapy, such as intranasal or oral administration of saprophytic bacteria, that prevented pathogen infections.14 This interesting topic has been extensively presented and discussed in an updated review.14
Resveratrol is a valuable natural compound having beneficial effects, such as anti-inflammatory, antioxidant, antibacterial, and antiviral activity. A previous real-life study recruited 82 children with acute rhinopharyngitis and RRI.15 Half of these children were treated with resveratrol plus carboxymethyl-β-glucan nasal spray administered for 20 days. This medical device significantly reduced the number of days with nasal obstruction, rhinorrhea, sneezing, cough, fever, intensity of medication use, medical visits, and absence from school.
Thermal water could also be considered a reliable therapy for children with RRI. A study investigated the possible effects of salso-sulphide thermal water in preventing RRI in children.16 This study included 107 children divided into two groups: treatment group inhaled crenotherapy with salso-sulphide water or isotonic saline (NaCl 0.9%) for 12 days. The results showed that crenotherapy diminished the number of RIs, nasal complaints, nasal infiltrate (count of neutrophils and bacteria), turbinate and adenoidal hypertrophy, biofilm distribution, and obstruction to ostiomeatal complex (OCM).
Another group of investigated non-pharmacological compounds included probiotics, bacteriotherapy, and bacterial lysates. Concerning the preventive effects provided by probiotics, three systematic reviews and meta-analyses examined this issue.53–55 The first study evaluated the impact of prebiotics, synbiotics, and short-chain fatty acids on RRIs with 58 trials.53 This analysis concluded that oligosaccharide supplementation was effective in infants and children. The second study analyzed probiotic-fermented dairy products, selecting 22 randomized controlled trials.54 This study demonstrated that these compounds significantly decreased RRIs in children, mainly URIs (risk ratio [RR] = 0.82). The last meta-analysis included 16 studies on synbiotics.55 Finally, a recent review confirmed the preventive effectiveness of probiotics in preventing asthma exacerbations in children.56 It is to be noted that these clinical conditions usually follow acute viral RIs in children.57 Therefore, this literature evidences confirmed that these products could effectively and safely prevent RRIs.
As reviewed recently, bacteriotherapy, such as administering saprophytic bacteria harboring in the airways, could productively prevent URI.58 Evidence has demonstrated that local or oral supplementation with Streptococcus oralis 89a and Streptococcus salivarius 24SMB could significantly prevent RIs, considering their number and severity, use of antibiotics, and absence from school.
Bacterial lysates are a heterogeneous class of modified bacteria.59 Usually, these lysates consist of a mixture of bacterial cultures modified by mechanical or chemical lysis. A recent systematic review and meta-analysis evaluated their role in preventing wheezing episodes and asthma exacerbations in children.60 The cited study included 22 trials and showed that bacterial lysates significantly reduced the number and duration of respiratory exacerbations and antibiotic use.60
Therefore, the literature supported the potential use of non-pharmacological remedies in managing children with RRI and was consistent with the present outcomes.
However, it has to be noted that the present study had some limitations, such as a low number of recruited children, need for precise diagnostic assays and measurement of biomarkers, and its open design. Consequently, the results were interpreted prudently. Anyway, the outcomes can reflect what may occur in real-life, such as in the primary care setting.
Further studies must be conducted with a rigorous methodology to confirm this preliminary analysis. The present study, although preliminary, is consistent with other studies that endorse the use of food supplements modulating immune response and fight against RIs.61–65
Conclusions
The present preliminary study suggested that a multicomponent product, administered as a nasal spray, could reduce the incidence of RIs and the use of symptomatic drugs for relieving wheezing in children.
REFERENCES
1. Pieren DKJ, Boer MC, De Wit J. The adaptive immune system in early life: The shift makes it count. Front Immunol. 2022;13:1031924. 10.3389/fimmu.2022.1031924
2. Niederman MS, Torres A. Respiratory infections. Eur Respir Rev. 2022;31(166):220150. 10.1183/16000617.0150-2022
3. Ameli F, Brocchetti F. Mignosi S, Tosca MA, Gallo F, Ciprandi G. Recurrent respiratory infections in children: A study in clinical practice. Acta Biomed. 2020;91(4):e2020179.
4. Varricchio A, La Mantia I, Brunese FP, Ciprandi G. Inflammation, infection, and allergy of upper airways: New insights from national and real-world studies. Ital J Pediatr. 2020;46(1):18. 10.1186/s13052-020-0782-z
5. Doss AMA, Stokes JR. Viral infections and wheezing in preschool children. Immunol Allergy Clin North Am. 2022;42(4):727–41. 10.1016/j.iac.2022.05.004
6. Tenero L, Tezza G, Cattazzo E, Piacentini G. Wheezing in-preschool children. Early Hum Develop. 2013;89:S13–7. 10.1016/j.earlhumdev.2013.07.017
7. Ducharme FM, Tse SM, Chauhan B. Diagnosis, management, and prognosis of preschool wheeze. Lancet. 2014;383:1593–604. 10.1016/S0140-6736(14)60615-2
8. Makrinioti H, Hasegawa K, Lakoumentas J, Xepapadaki P, Tsolia M, Castro-Rodriguez JA, et al. The role of respiratory syncytial virus-and rhinovirus-induced bronchiolitis in recurrent wheeze and asthma—A systematic review and meta-analysis. Pediatr Allergy Immunol. 2022;33(3):e13741. 10.1111/pai.13741
9. Ciprandi G, Cioffi L, Schiavetti I, Miraglia Del Giudice M, Tosca MA. Factors associated with wheezing recurrence in clinical practice. J Asthma. 2023;60(4):843–44. 10.1080/02770903.2022.2087187
10. Ciprandi G, Tosca MA. Non-pharmacological remedies for the common cold. Minerva Pediatr (Torino). 2023;75(1):75–86. 10.23736/S2724-5276.21.06312-6
11. Giannattasio A, Poggi E, Trapani G, Muia C, Zanino L, Landi M, et al. Primary care experience on Stimunex® gocce in children with recurrent respiratory infections: A real-world study during the COVID-19 pandemic era. Allergol Immunopathol (Madr). 2022;50(3):8–14. 10.15586/aei.v50i3.562
12. Marseglia GL, Benazzo M, Biasci P, Blasi F, Cricelli C, Doria M, et al. OM-85 in the prevention of respiratory infections: State-of-the-art and future perspectives in clinical practice. J Biol Regul Homeost Agents. 2021;35(3):847–63.
13. Poggi E, Giannattasio A, Cartosio ME, Campus R, Ciprandi G. Primary care experience on Rinfodim 3® in children with recurrent respiratory infections. J Biol Regul Homeost Agents. 2020;34(6):2365–73.
14. Ciprandi G, La Mantia I, Damiani V, Passali D. Local bacteriotherapy—A promising preventive tool in recurrent respiratory infections. Expert Rev Clin Immunol. 2020;16(11):1047–52. 10.1080/1744666X.2021.1833720
15. Varricchio AM, Capasso M, Della Volpe A, Malafronte L, Mansi N, Varricchio A, et al. Resveratrol plus carboxymethyl-β-glucan in children with recurrent respiratory infections: A preliminary and real-life experience. Ital J Pediatr. 2014;40:93. 10.1186/s13052-014-0093-3
16. Varricchio A, Giuliano M, Capasso M, Del Gaizo D, Ascione E, De Lucia A, et al. Salso-sulphide thermal water in the prevention of recurrent respiratory infections in children. Int J Immunopathol Pharmacol. ,2013;26(4):941–52. , 10.1177/039463201302600412
17. Passali D, Ionescu A, Brambilla E, Bellussi LM, Ciprandi G, Mattina R, et al. Can pseudomonas aeruginosa growth be modulated by natural compounds? J Biol Regul Homeost Agents. 2021;35(1, Suppl. 2):21–5.
18. Ameli F, Ciprandi G. Sinerga may prevent recurrent respiratory infections in allergic children. J Biol Regul Homeost Agents. 2019;33:601–7.
19. Tosca MA, Del Barba P, Licari A, Ciprandi G. The measurement of asthma and allergic rhinitis control in children and adolescents. Children (Basel). 2020;7(5):43. 10.3390/children7050043
20. Wang X, Li Y, O’Brien KL, Madhi SA, Widdowson MA, Byass P, et al. Global burden of respiratory infections associated with seasonal influenza in children under 5 years in 2018: A systematic review and modelling study. Lancet Glob Health. 2020;8(4):e497–510.
21. Principi N, Esposito S. Antibiotic-related adverse events in paediatrics: Unique characteristics. Expert Opin Drug Saf. 2019;18(9):795–802. 10.1080/14740338.2019.1640678
22. Subramaniam G, Girish M. Antibiotic resistance—A cause for re-emergence of infections. Indian J Pediatr. 2020;87(11):937–44. 10.1007/s12098-019-03180-3
23. Villani L, D’Ambrosio D, Ricciardi R, De Waure C, Calabrò GE. Seasonal influenza in children: Costs for the health system and society in Europe. Influenza Other Respir Viruses. 2022;16(5):820–31. 10.1111/irv.12991
24. Sattler S. The role of the immune system beyond the fight against infection. Adv Exp Med Biol. 2017;1003:3–14. 10.1007/978-3-319-57613-8_1
25. Drago L, Cioffi L, Giuliano M, Pane M, Amoruso A, Schiavetti I. The PRObiotics in pediatric asthma management (PROPAM) study in the primary care setting: A randomized, controlled, double-blind trial with Ligilactobacillus Salivarius LS01 (DSM 22775) and Bifidobacterium Breve B632 (DSM 24706). J Immunol Res. 2022;2022:3837418. 10.1155/2022/3837418
26. Legrand D. Overview of lactoferrin as a natural immune modulator. J Pediatr. 2016;173S:S10–5. 10.1016/j.jpeds.2016.02.071
27. Dierick M, Vanrompay D, Devriendt B, Cox E. Lactoferrin, a versatile natural antimicrobial glycoprotein which modulates host innate immunity. Biochem Cell Biol. 2021;99(1):61–5. 10.1139/bcb-2020-0080
28. Sorensen M, Sorensen S. The proteins in whey. Compte rendu des Travaux du Laboratoire de Carlsberg Ser Chim. 1940;23(7):55–99.
29. Wang B, Timilsena YP, Blanch E, Adhikari B. Lactoferrin: Structure, function, denaturation and digestion. Crit Rev Food Sci Nutr. 2019;59:580–96. 10.1080/10408398.2017.1381583
30. Moreno-Exposito L, Illesca-Montes R, Meguizo-Rodriguez L, Ruiz C, Ramos-Torrecillas J, De Luna-Bertos E. Multifunctional capacity and therapeutic potential of lactoferrin. Life Sci. 2018;195:61–4. 10.1016/j.lfs.2018.01.002
31. Kell DB, Heyden EL, Pretorius E. The biology of lactoferrin, an iron-binding protein that can help defend against viruses and bacteria. Front Immunol. 2020;11:1221. 10.3389/fimmu.2020.01221
32. Lepanto MS, Rosa L, Paesano R, Valenti P, Cutone A. Lactoferrin in aseptic and septic inflammation. Molecules. 2019;24:1323. 10.3390/molecules24071323
33. Actor JK, Hwang SA, Kruzel ML. Lactoferrin as a natural immune modulator. Curr Pharm Des. 2009;15:1956–73. 10.2174/138161209788453202
34. Drago-Serrano ME, Campos-Rodríguez R, Carrero JC, De la Garza M. Lactoferrin: Balancing ups and downs of inflammation due to microbial infections. Int J Mol Sci. 2017;18:501. 10.3390/ijms18030501
35. Reyes-Cortes R, Acosta-Smith E, Mondragón-Flores R, Nazmi K, Bolscher JGM, Canizalez-Roman A. Antibacterial and cell penetrating effects of LFcin17–30, LFampin265–284, and LF chimera on enteroaggregative Escherichia coli. Biochem Cell Biol. 2017;95:76–81. 10.1139/bcb-2016-0088
36. Chen K, Jin S, Chen H, Cao Y, Dong X, Li H, et al. Dose effect of bovine lactoferrin fortification on diarrhea and respiratory tract infections in weaned infants with anemia: A randomized, controlled trial. Nutrition. 2021;90:111288. 10.1016/j.nut.2021.111288
37. Ali AS, Hasan SS, Kow CS, Merchant HA. Lactoferrin reduces the risk of respiratory tract infections: A meta-analysis of randomized controlled trials. Clin Nutr ESPEN. 2021;45:26–32. 10.1016/j.clnesp.2021.08.019
38. Vetvicka V, Vannucci L, Sima P, Richter J. Beta-glucan: Supplement or drug? From laboratory to clinical trials. Molecules. 2019;24:1251. 10.3390/molecules24071251
39. Ali MF, Driscoll CB, Walters PR, Limper AH, Carmona EM. Beta-glucan-activated human B lymphocytes participate in innate immune responses by releasing pro-inflammatory cytokines and stimulating neutrophil chemotaxis. J Immunol. 2015;195:5318–26. 10.4049/jimmunol.1500559
40. Talbott SM, Talbott JA, Talbott TL, Dingler E. Beta glucan supplementation, allergy symptoms, and quality of life in self-described ragweed allergy sufferers. Food Sci Nutr. 2013;1:90–101. 10.1002/fsn3.11
41. Ciprandi G, Bellussi LM, Passali GC, Damiani V, Passali D. HMGB1 in nasal inflammatory diseases: A reappraisal 30 years after its discovery. Exp Rev Clin Immunol. 2020;16:457–63. 10.1080/1744666X.2020.1752668
42. Bellussi LM, Cocca S, Passali GC, Passali D. HMGB1 in the pathogenesis of nasal inflammatory diseases and its inhibition as a new therapeutic approach: A review from the literature. Int Arch Otorhinolaryngol. 2017;21:390–8. 10.1055/s-0036-1597665
43. Hemila H. Vitamin C and infections. Nutrients. 2017;9:339. 10.3390/nu9040339
44. Webb AL, Villamor E. Update: Effects of antioxidant and non-antioxidant vitamin supplementation on immune function. Nutr Rev. 2007;65:181–217. 10.1111/j.1753-4887.2007.tb00298.x
45. Sassi F, Tamone C, D’Amelio P. Vitamin D: Nutrient, hormone, and immunomodulator. Nutrients. 2018;10:1656. 10.3390/nu10111656
46. Holick MF. Vitamin D deficiency. New Engl J Med. 2007;357:266–81. 10.1056/NEJMra070553
47. Camargo CA Jr, Ingham T, Wickens K, Thadhani R, Silvers KM, Epton MJ. Cord-blood 25-hydroxyvitamin D levels and risk of respiratory infection, wheezing, and asthma. Pediatrics. 2011;127:180–7. 10.1542/peds.2010-0442
48. Saggese G. Vitamin D in pediatric age: Consensus of the Italian Pediatric Society and the Italian Society of Preventive and Social Pediatrics, jointly with the Italian Federation of Pediatricians. Ital J Pediatr. 2018;44:51. 10.1186/s13052-018-0488-7
49. Proksch E, De Bony R, Trapp S, Boudon S. Topical use of dexpanthenol: A 70th-anniversary article. J Dermatol Treat. 2017;28:766–73. 10.1080/09546634.2017.1325310
50. Kelly GS. Pantothenic acid. Monograph. Altern Med Rev. 2011;16:263–74.
51. Li Y, Wang X, Blau DM, Caballero MT, Feikin DR, Gill CJ, et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet. 2022;399(10340):2047–64. 10.1016/S0140-6736(22)00478-0
52. Tosca MA, Schiavetti I, Varricchio A, Ciprandi G. Managing children with allergic rhinitis: A preliminary experience with a new multicomponent nasal spray. Indian J Pediatr. 2024;91(4):411. 10.1007/s12098-023-04907-z
53. Williams LM, Stoodley IL, Berthon BS, Wood LG. The effects of prebiotics, synbiotics, and short-chain fatty acids on respiratory tract infections and immune function: A systematic review and meta-analysis. Adv Nutr. 2022;13(1):167–92. 10.1093/advances/nmab114
54. Rashidi K, Razi B, Darand M, Dehghani A, Janmohammadi P, Alizadeh S. Effect of probiotic fermented dairy products on incidence of respiratory tract infections: A systematic review and meta-analysis of randomized clinical trials. Nutr J. 2021;20(1):61. 10.1186/s12937-021-00718-0
55. Chan CKY, Tao J, Chan OS, Li HB, Pang H. Preventing respiratory tract infections by synbiotic interventions: A systematic review and meta-analysis of randomized controlled trials. Adv Nutr. 2020;11(4):979–88. 10.1093/advances/nmaa003
56. Ciprandi G, Tosca MA. Probiotics in children with asthma. Children. 2022;9(7):978. 10.3390/children.9070978
57. Romero-Tapia SJ, Guzmán Priego CG, Del-Río-Navarro BE, Sánchez-Solis M. Advances in the relationship between respiratory viruses and asthma. J Clin Med. 2023;12(17):5501. 10.3390/jcm12175501
58. Ciprandi G, La Mantia I, Damiani V, Passali D. Local bacteriotherapy—A promising preventive tool in recurrent respiratory infections. Expert Rev Clin Immunol. 2020;16(11):1047–52. 10.1080/1744666X.2021.1833720
59. Puggioni F, Alves-Correia M, Manar-Farouk M, Stomeo N, Mager R, Marinoni M, et al. Immunostimulants in respiratory diseases: Focus on pidotimod. Multidisc Resp Med. 2019;14:31. 10.1186/s40248-019-0195-2
60. De Boer GM, Żółkiewicz J, Strzelec KP, Ruszczyński M, Hendriks RW, Braunstahl GJ, et al. Bacterial lysate therapy for the prevention of wheezing episodes and asthma exacerbations: A systematic review and meta--analysis. Eur Respir Rev. 2020;29(158):190175. 10.1183/16000617.0175-2019
61. Hałasa M, Skonieczna-Żydecka K, Machaliński B, Bühner L, Baśkiewicz-Hałasa M. Six weeks of supplementation with bovine colostrum effectively reduces URTIs symptoms frequency and gravity for up to 20 weeks in pre-school children. Nutrients. 2023;15(16):3626. 10.3390/nu15163626
62. Binks MJ, Bleakley AS, Pizzutto SJ, D’Antoine H, Licciardi PV, Snelling T, et al. Randomised controlled trial of perinatal vitamin D supplementation to prevent early--onset acute respiratory infections among Australian First Nations children: The “D-Kids” study protocol. BMJ Open Respir Res. 2023;10(1):e001646. 10.1136/bmjresp-2023-001646
63. Buendía JA, Patino DG, Lindarte EF. Effectiveness of high-dose vitamin D supplementation to reduce the incidence rate of repeat episodes of pneumonia in children: A systematic review. Pediatr Pulmonol. 2023;58(10):2972–5. 10.1002/ppul.26585
64. Loddo F, Nauleau S, Lapalus D, Tardieu S, Bernard O, Boubred F. Association of maternal gestational vitamin D supplementation with respiratory health of young children. Nutrients. 2023;15(10):2380. 10.3390/nu15102380
65. Shi Y, Lei Q, Liu H, Han Q. The role of vitamin A and zinc supplementation in pediatric pneumonia: A protocol for systematic review and network meta-analysis. Medicine (Baltimore). 2022;101(51):e32183. 10.1097/MD.0000000000032183