
Download
CASE REPORT
Omalizumab in the treatment of Morbihan syndrome in an adolescent girl – case report and literature review
Zofia Mazurek-Durlak*, Katarzyna Mularczyk, Przemko Kwinta, Grzegorz Lis, Ewa Cichocka-Jarosz
Faculty of Medicine, Department of Pediatrics, Jagiellonian University Medical College, 265, Wielicka Str. 30-663 Krakow, Poland
Abstract
Morbihan syndrome (MS) is characterized by solid facial edema, usually related to rosacea or acne vulgaris. The facial edema deforms the patient’s features, can impair peripheral vision, and affects quality of life. Its pathophysiology remains unclear. The disease usually has a slow and chronic course. MS most commonly affects middle-aged Caucasian men with rosacea and is rare in people below 20 years of age. MS is a diagnosis of exclusion. There is no standard treatment for MS, though systemic isotretinoin and antihistamines are mainly used. We present the case of an adolescent girl with MS nonresponding to 19 months of isotretinoin treatment with add-on antihistamines. Therapy with monthly administration of omalizumab (anti-IgE) for 6 months was an effective therapeutic option, improving the quality of life. Our case is the second description of omalizumab use in Morbihan syndrome, the first in an adolescent.
Key words: Adolescent, anti-IgE, solid facial edema, Morbihan syndrome, omalizumab
*Corresponding author: Zofia Mazurek-Durlak, Faculty of Medicine, Department of Pediatrics, Jagiellonian University Medical College, 265, Wielicka Str. 30-663 Krakow, Poland. Email address: [email protected]
Received 19 August 2023; Accepted 15 December 2023; Available online 1 March 2024
Copyright: Mazurek-Durlak Z, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Morbihan’s syndrome (MS) was described in 1957 by Robert Degos.1 It was named after the Bretagne region in France, where one of the first patients came from. Schimpf described four similar clinical cases between 1956 and 1960. So he is the first physician to report Morbihan syndrome, using the term Dermatitis frontalis granulomatosa.2 MS is also known as Morbihan disease, lymphedema rosacea, lymphedematous rosacea, or idiopathic solid facial edema.2 MS is a rare disease, and its etiology remains unclear. To date, approximately 170 cases of MS have been described, but not all of them include a histopathology report.1–5 About 70% of patients are male, usually middle-aged Caucasian.2,3,4 Just recently, a few cases from East Asia were described.6,7 According to the recent publications of the systematic review and UK case series, the age of onset ranges from 14 to 88, and the mean age of onset of symptoms is around 50.2,5,8 Most patients with MS are in their forties, fifties, or sixties. In people below 30 years of age, MS is more often connected with acne than rosacea. Descriptions of patients aged 18 and less are the minority.2,9
The disease’s main symptom is a nonitchy, cohesive, erythematous swelling of the upper- and mid-face, deforming the patient’s features and often restricting the visual field.1,2,3,10 The skin lesions are usually symmetrical and exceptionally unilateral.11,12 Pathophysiology is believed to be related to rosacea or acne vulgaris, as one of them is present in most cases of MS before the onset of the swelling.9,13 Disease usually has a slow and chronic course and doesn’t disappear without treatment. The aim of the study was to present the case of a 15-year-old MS patient, resistant to anti-acne therapy, who was successfully treated with anti-IgE omalizumab. This is one of the youngest reported pediatric cases, the second patient treated with omalizumab, and the first adolescent with MS treated with omalizumab.
Case Report
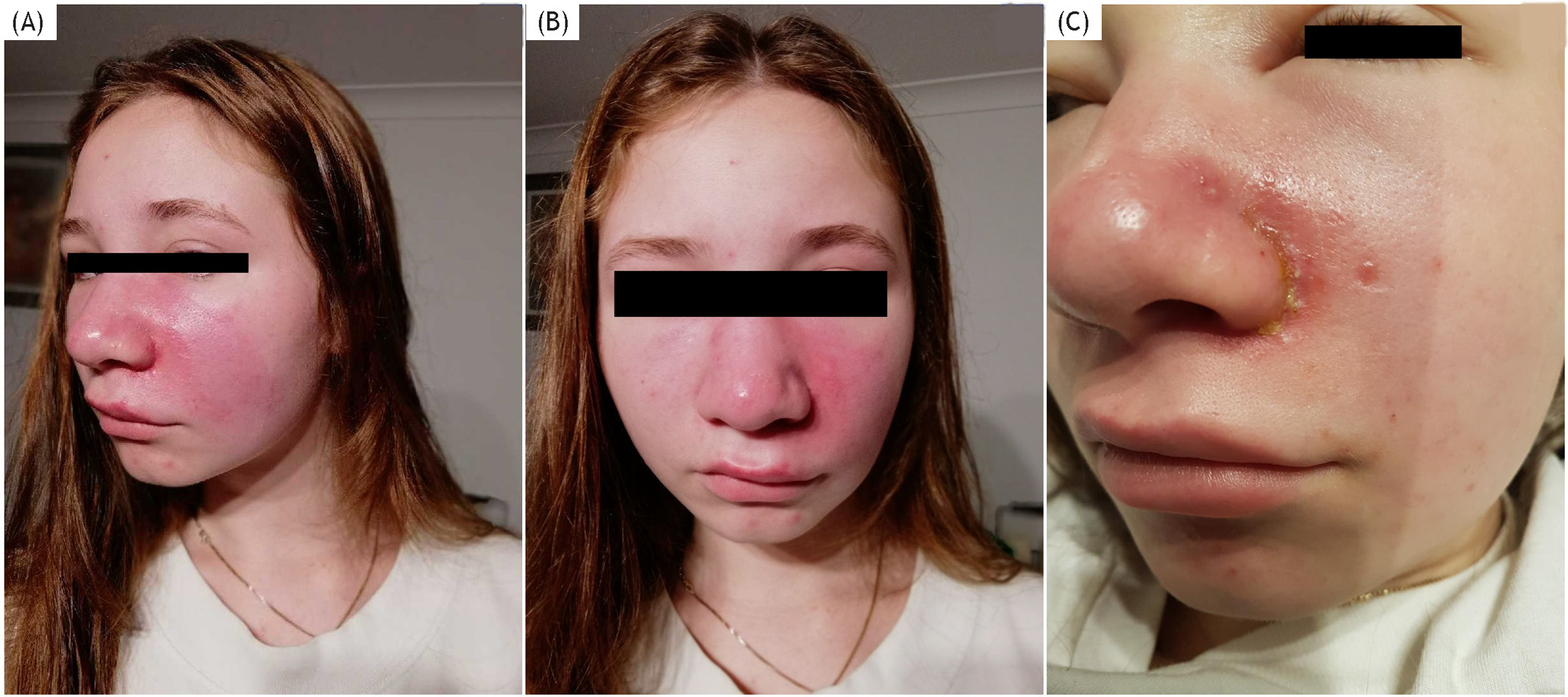
A 15-year-old girl presented to the University Children’s Hospital due to facial swelling of variable intensity that had persisted for several months. Since December 2018, the patient has been under dermatological care due to mild juvenile comedogenic acne treated with standard topical treatment / adapalene. After 2 months, the persistent facial erythema appeared, later accompanied by chronic solid swelling of the left periocular area, nose bridge, left cheek, and upper lip (Figure 1A). Subsequently, the swelling expanded bilaterally, including both eyelids, cheeks, nose, and mouth area, with smoothing of the nasolabial folds (Figure 1B). The lesions were not painful or itchy. The erythema was solid, nonpitting, and nontender. The area’s temperature wasn’t increased in physical examination except for periods of unilateral exacerbation.
The typical characteristics of rosacea were absent: no telangiectasia, no demodex tails, and no demodex follicular openings on dermoscopy. Open and closed comedones were observed on dermoscopy, with no desquamation or vesiculation. The follicle orifices were not enlarged. The diascopy was positive for blanching; no apple jelly sign was observed. There were a few papules. Periodically, the intensification of the edema resulted in the narrowing of the palpebral fissure with impaired vision and difficulty in opening the eyes. In addition, there were transient purulent acne lesions on the face, which worsened during upper respiratory tract infection. It was the single time of oozing lesions and improved after antibiotic treatment with cefuroxime for 16 days (Figure 1C).
Figure 1 (A–C) Face presentation in the course of disease (multipanel)
The skin lesions deteriorated after exposure to the sun. Skin symptoms were independent of the menstrual cycle. Facial edema persisted. In the beginning, lesions were exacerbated twice a month.
Skin lesions of the face significantly worsened the quality of life, caused a decrease in self-esteem, and reduced social contact. Dermatological Quality of Life Index (DLQI) showed a moderate effect on the patient’s life: 10 points, and during exacerbation 13 points (very large effect on the quality of life). In addition, in the 6 months before assessment in the University Children’s Hospital, the patient had observed hair loss and weight gain of 9 kg, possibly because of reduced physical activity and unsuccessful treatment of MS with systemic corticosteroids. In the past, she had two episodes of IgA-mediated vasculitis (in 2012 and 2018) during upper respiratory tract infections. She was also under the care of an ophthalmologist for myopia. Her personal history of atopy was negative. Her mother had a history of Hashimoto’s disease, and her mother and two brothers had allergic rhinoconjunctivitis. The patient was hospitalized several times, and during the aggravations of symptoms, the patient sought help at the emergency department. At first, as the symptoms emerged, erysipelas, nephrotic syndrome, and acquired and hereditary angioedema were suspected, not Morbihan syndrome (the dermatologist did not assess the patient then). At that time, the patient was treated empirically as a superficial skin infection with edema with systemic antibiotics (doxy-cycline, amoxicillin with clavulanic acid, metronidazole, and clindamycin recommended by different physicians) and as acquired, histaminergic angioedema with systemic glucocorticoids, with no marked improvement. A trial of treatment with rupatidine was performed in a double- and then fourfold dose, without improvement.
As Morbihan syndrome is a diagnosis of exclusion, other possible causes of facial edema and pseudo-angioedema were taken into consideration2,4,14. Basic laboratory tests showed no abnormalities. Normal thyroid and sex hormones, kidney, liver, and pancreatic enzymes were found, allowing the exclusion of thyroid diseases and nephrotic syndrome. The absence of vascular changes in the microscopic capillaroscopy of the nail fold and normal complement components made the diagnosis of systemic lupus erythematosus (SLE) unlikely. In the differential diagnosis, allergy to inhalants and food allergens (negative skin prick tests—Supplementary Tables S1–S2), and allergic contact dermatitis were excluded (negative patch test performed in adult reference allergy center), as were (clinically and laboratory) humoral and cellular immunity disorders (Tables 1 and 214,18–22). Dental and otorhinolaryngological (CT of the head and sinuses, MRI of the craniofacial region) evaluation did not reveal foci of infection. Abdominal ultrasound and chest X-ray were normal. Doppler ultrasound examination of the carotid arteries revealed no abnormalities. As the patient connected sun exposure with symptoms worsening, direct immunofluorescence (“lupus band test”) from healthy and lesional skin was performed. Differential diagnosis included autoimmune diseases: cutaneous lupus erythematosus and dermatomyositis.
Table 1. Results of diagnostic laboratory findings
| ANCA profile: proteinase3 | <0.10 (negative <1.0) |
| Lactoferrin | <0.10 (negative <1.0) |
| Myeloperoxidase | 0.2 (negative <1.0) |
| Elastase | 0.1 (negative <1.0) |
| Catepsin G | 0.1(negative <1.0) |
| BPI | 0.5 (negative <1.0) |
| Complement C3c | 1.25 g/l (N: 0.90–1.80) |
| Complement C4 | 0.17 g/l (N: 0.13–0.40) |
| C1 inhibitor concentration | 0.24 g/l (N: 0.18–0,32) |
| Immunoglobulin G | 12.30 g/l (N: 6.3.8–17.00) |
| Immunoglobulin A | 1.04 g/l (N: 0.67–3.67) |
| Immunoglobulin M | 0.73 g/l (N: 0.41–2.03) |
| Immunoglobulin E | 426 IU/ml (N: 0.00–100.00) |
| Lymphocyte subset counts | WBC 6370/ul (N: 3840–9840) Lymphocytes 38% (N: 16.4–52.7) 2421/ul (N: 970–3330) Lymphocytes T CD3 76% (N: 56–84) 1840 (N: 1000–2200) Lymphocytes CD4 53% (N: 31–52) 1283/ul (N: 530–1300) Lymphocytes CD8 18% (N: 18–35) 436/ul (N: 330–920) Lymphocytes CD19 16% (N: 6–23) 387/ul (N: 110–570) NK Cells7% (N: 3–22) 169/ul (N: 70–480) |
| Antinuclear antibodies + titer | Fluorescence type: grainy, titer: 1:100 |
| Anti-TPO antibodies | Negative |
| 17-OH progesterone | 3.70 ng/ml (N: 1.0–4.5) |
| Alpha-fetoprotein | <1.3ng/ml (N: <15) |
| Prolactin | 198.2 uIU/ml (N: 60–620) |
| Testosterone | 0.26 ng/ml (N: −0.084–0.481) |
| DHEA-s | 142.9 ug/ml (N: 75–350) |
| Beta hCG | <2 mIU/ml (N: <10) |
BPI – bactericidal permeability increasing protein, TPO – thyroid peroxidase
Table 2. Modification of European Standard Series, Polish Standard Series with added benzalkonium chloride was used for patch testing
| Name | Concentration | |
|---|---|---|
| 1. | Potassium dichromate | 0.5% pet |
| 2. | p-Phenylendiamine (PPD) | 1.0% pet |
| 3. | Thiuram mix | 1.0% pet |
| 4. | Neomycin sulfate | 20.0% pet |
| 5. | Cobalt(II)chloride hexahydrate | 1.0% pet |
| 6. | Caine mix III | 10.0% pet |
| 7. | Nickel(II)sulfate hexahydrate | 5.0% pet |
| 8. | 2-Hydroxyethyl methacrylate | 2.0% pet |
| 9. | Colophonum | 20.0% pet |
| 10. | Paraben mix | 16.0% pet |
| 11. | Gentamycin sulfate | 20.0% pet |
| 12. | Lanolin alcohol | 30.0% pet |
| 13. | Epoxy resin, Bisphenol A | 1.0% pet |
| 14. | Peru balsam | 25.0% pet |
| 15. | 2-Mercaptobenzothiazole (MBT) | 2.0% pet |
| 16. | Formaldehyde | 2.0% aq |
| 17. | Fragrance mix I | 8.0% pet |
| 18. | Sodium tetrahydropalladate (II) hydrate | 3.0% pet |
| 19. | Quaternium 15 | 1.0% pet |
| 20. | Propolis | 10.0% pet |
| 21. | Methylisothiazolinone + Metylchloroisothiazolinone | 0.01% pet |
| 22. | Budesonide | 0.01% pet |
| 23. | Tixocortol-21-pivalate | 0.1% pet |
| 24. | Hydroperoxides of linalool | 0.5% pet |
| 25. | Hydroperoxides of limonene | 0.2% pet |
| 26. | Methyldibromoglutaronitrile | 0.5% pet |
| 27. | Fragrance mix II | 14.0% pet |
| 28. | Hydroxyisohexyl 3-cyclohexene carboxaldehyde | 5.0% pet |
| 29. | Methylisothiazolinone | 0.2% aq |
| 30. | Textile dye mix | 6.6% pet |
| 31. | Benzalkonium chloride | 0,1% aq |
| Producent: Chemotechnique | Pet-petroleum, Aq-water solution |
Direct immunofluorescence revealed a single weak band of granular structures consisting of IgM, IgA, and C4 located below the epidermal-dermal junction. Immunofluorescence of IgG, C1q, and C3c deposits was negative. The titer of antinuclear antibodies in the blood was not clinically significant (1:100), as the patient didn’t have any other signs and symptoms suggesting rheumatological disease, except photo-aggravated symptoms.
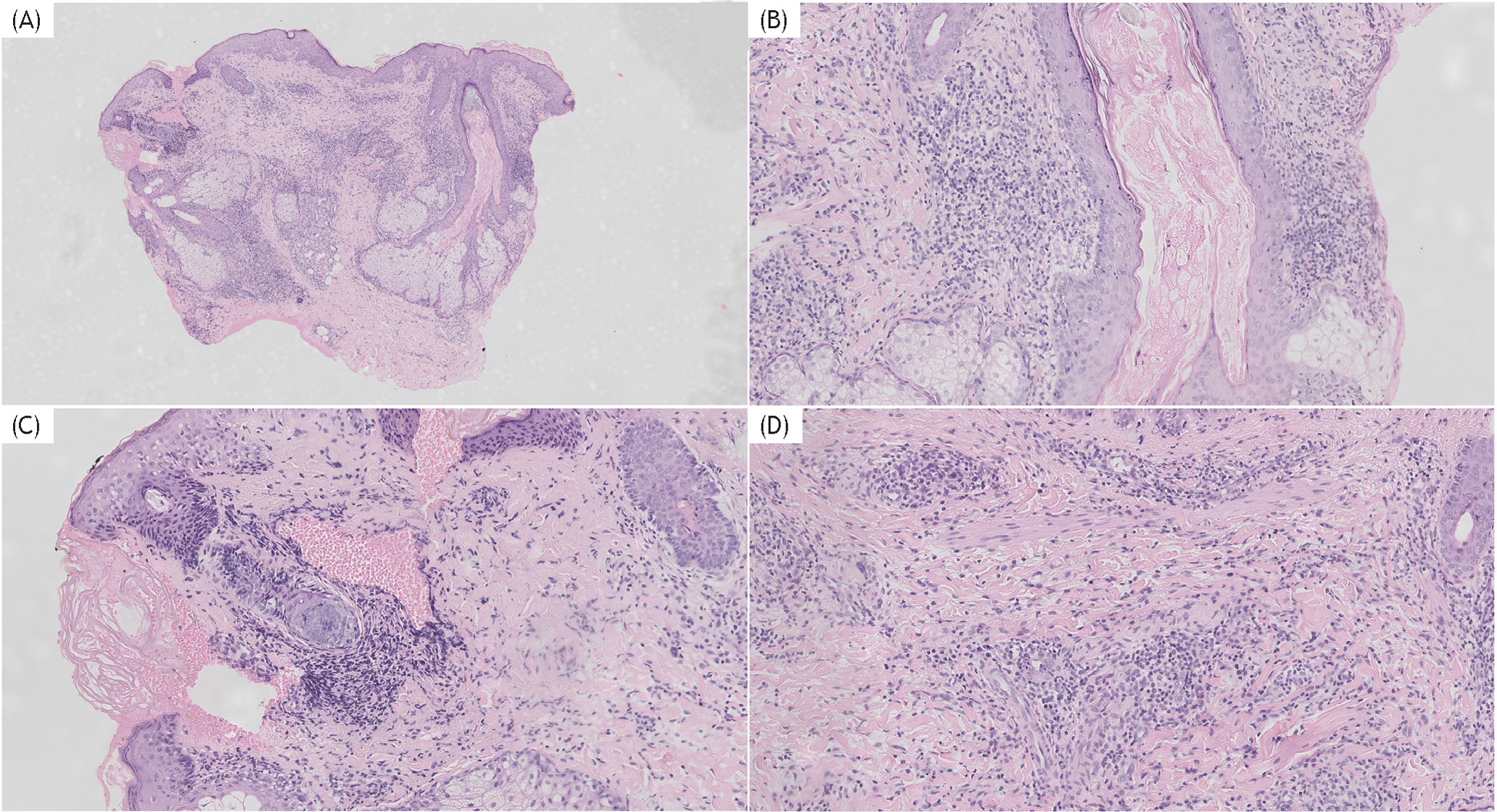
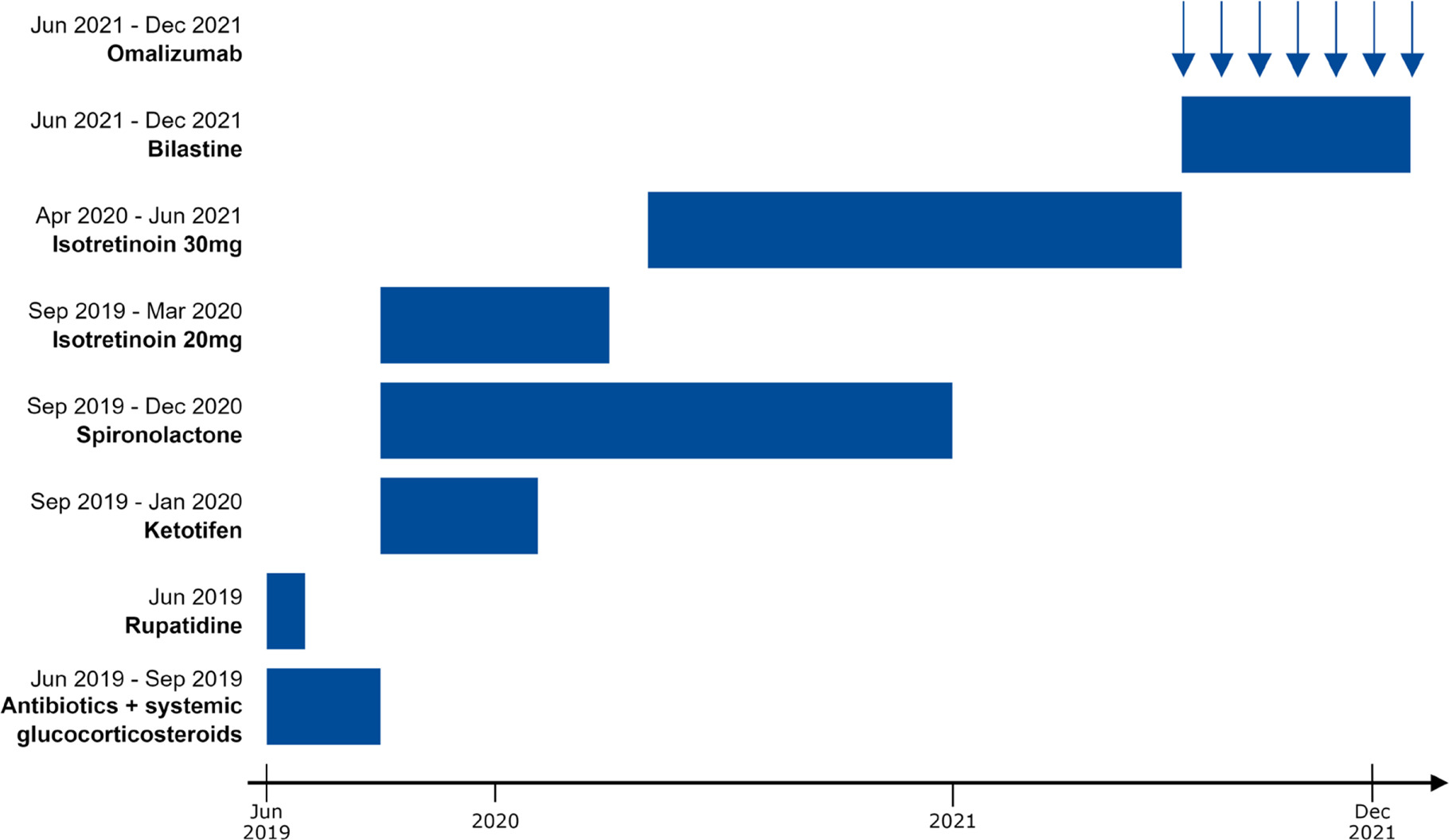
The histopathological examination was performed to rule out differential diagnoses, especially the ones that cannot be diagnosed without biopsy: skin lymphoma and granulomatous diseases (sarcoidosis, tuberculosis, Melkersson-Rosenthal syndrome). Skin biopsy from the lesion of the cheek was assessed after hematoxylin–eosin staining. Enlarged sebaceous glands with lymphohistiocytic and lymphoplasmatic infiltrates around the pilosebaceous unit and blood vessels and fibrosis were prominent. No demodex mites were seen. No spongiosis or epidermal changes were noted. The histopathological pictures of the lesion were within the spectrum of MS, showing dermatitis and periadnexitis (Figure 2). The time from the patient’s first visit to the diagnosis was 10 months. After MS diagnosis, due to acne lesions accompanied by edema, systemic treatment with isotretinoin 20 mg/day, ketotifen, and spironolactone was started in September 2019. Topical therapy with pimecrolimus caused local skin irritation and was stopped quickly. In addition, manual lymph drainage was performed, and after training, it was regularly self-applied. Partial improvement was obtained: periods of exacerbation of edema subsided, but solid facial edema persisted, and the patients’ facial features did not return to their pre--disease state. Ketotifen was used for 5 months and discontinued. After 6 months of isotretinoin treatment at 20 mg/day, the dose was increased to 30 mg (with a maximum daily dose of 40 mg, as 20 and 40 mg were alternated) (Figure 3). Acne lesions (papules, comedones) resolved entirely, and episodes of severe edema were less frequent. Spironolactone was discontinued in December 2020. After the discontinuation of ketotifen and spironolctone, no deterioration was observed. Isotretinoin was continued. Despite a long period of treatment with isotretinoin (19 months), many months of additional use of oral antihistamines (ketotifen, bilastine), temporary use of diuretics (antiandrogen spironolactone) and calcineurin inhibitors, modest improvement was achieved. As the cumulative dose of isotretinoin reached 200 mg per kilogram of body weight and exceeded the standard doses recommended in acne guidelines and used in MS in the past, no further improvement was noted.
Figure 2 Skin biopsy images (multipanel). (A) Low power magnification (H&E ×10) shows dermatitis and periadnexitis. (B–C) High power (H&E ×40) magnification shows periadnexal lymphoplasmacytic inflammation. (D) (H&E ×40) High power magnification shows perivascular lymphoplasmacytic inflammation
Figure 3 Treatment schedule
Still, the swelling of the facial skin, including eyelids, nose, mouth, and cheeks, and the deformation of the patient’s face persisted. None of the introduced drugs resulted in complete remission of symptoms, which prompted the search for nonstandard treatment methods. Due to the case report of MS treatment with omalizumab15, the team of specialists decided to administer omalizumab off-label. Biological drugs are given and paid for by public insurance in registered indications as part of the drug treatment programs in Poland. The off-label use of omalizumab was approved by the allergist consultant of the province, the insurance provider (National Health Fund), and the local university Bioethics Committee.
The IgE concentration before treatment was elevated (426 IU/mL). In the case reported by Kafi et al.,15 the authors used an initial dose of omalizumab 450 mg, followed by 300 mg every 2 months. In our case, we used the urticaria dosage of 300 mg every month, as there are some similarities in pathophysiology, and this dosing regimen is well-studied in children and adolescents.16
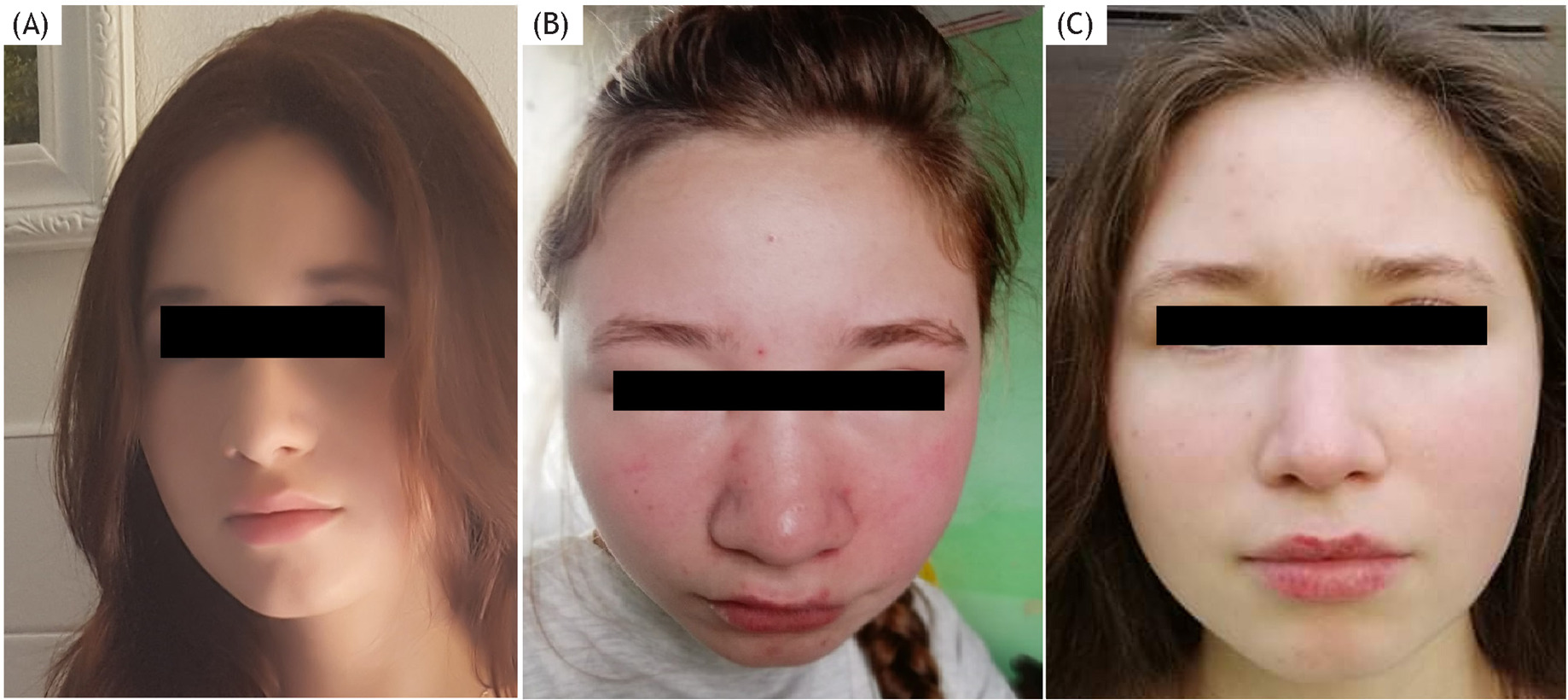
Omalizumab was administered at 300 mg (fractionated 2 × 150 mg s.c.) every 4 weeks. In the period from June 2021 to December 2021, a total of seven doses of the drug were administered (Figure 3). Despite the biological treatment, the facial features did not return to how they were before the disease (Figure 4A)—especially the nose is still more prominent and mild edema of the face exists. Isotretinoin was discontinued during omalizumab therapy.
Figure 4 (A) Face presentation before the disease, (B) Face presentation before omalizumab treatment. (C) Face presentation after 6 months of omalizumab therapy (multipanel).
However, compared to the time before the omalizumab introduction (Figure 4B), a substantial improvement in the skin condition and edema reduction was achieved (Figure 4C), both in the doctor’s opinion and the patient’s opinion. The patient’s DLQI improved to 6 points. The quality of life is still moderately impacted, which can be explained by the patient’s expectation of disease clearance. The improvement in clinical presentation and quality of life persists to date.
Discussion
It is postulated that the term “Morbihan syndrome” should be used because facial edema, unrelated to systemic disease, may have a different etiopathogenesis. Morbihan disease is usually described as rosacea-related face edema, while acne-related edema is named both Morbihan syndrome and solid facial edema9.
It is postulated that inflammation disturbs the lymphatic circulation, and local fibrosis develops with time, causing permanent swelling.3,4,15,17 Destruction of perivascular elastin fibers promotes vascular wall damage and exudation. Inflammation can be exacerbated by contact allergy to cosmetics and infestation of Demodex folliculorum in rosacea. Various mediators (bradykinin, IL-1b, and histamine) released in the inflammatory process from mast cells, granulocytes, macrophages, and T lymphocytes are involved in edema development.3,4,17 The edema initially fluctuates but stabilizes over time, becoming chronic and does not tend to disappear without treatment. Acne vulgaris and rosacea lesions are usually mild, even with prominent edema. Facial edema, typically symmetrical, deforms the patient’s facial features, affects daily functioning, and deteriorates the patient’s quality of life. However, this problem has not been the subject of publications so far.10,11 Our patient, though almost the youngest among those being described, presented with all typical symptoms. Usually, the diagnosis of MS is made after the exclusion of other potential causes of swelling. There are no specific biochemical or histopathological findings of MD. In Morbihan disease, no additional staining is needed if the hematoxylin–eosin staining does not suggest any different diagnosis (i.e., lymphoproliferative disease.)
Basic laboratory test results are usually within normal limits, which was also the case with our patient. When seen in the acute setting, Morbihan syndrome can be mistaken for angioedema. The differential diagnoses of MS include pseudo-angioedema, acute diseases present with facial edema.14 Often, the first diseases clinically suspected are erysipelas, dental and sinus abscesses, nephrotic syndrome, hereditary angioedema (HAE), and acquired histaminergic angioedema, that is, in patients with venom allergy after bee/wasp sting.14 The differential diagnosis should also include acquired angioedema related to autoimmune diseases, as well as allergic angioedema and superior vena cava syndrome (Table 2).14,18–22 Skin biopsy is a recommended diagnostic procedure to exclude conditions with characteristic histopathological findings: skin neoplasms, Melkersson-Rosenthal syndrome, contact dermatitis, and sarcoidosis.18-23 The histopathologic findings of MD are not pathognomonic for the disease and include perivascular dermal edema, lymphohistiocytic infiltration, mast cell infiltration to the periadnexal tissues of the lymph vessels, dilation of lymphatic vessels, fibrosis, and sebaceous gland hyperplasia.3–5,17,24 Noncaseating granulomas typical of sarcoidosis and Melkersson-Rosenthal syndrome are usually absent. The immunological deposits on direct immunofluorescence are absent, nonspecific, or weak, not forming bands.
There are some recent data on the usefulness of the reflective confocal microscope in diagnoses of MS.24 This method allows for the observation of the entire thickness of the epidermis and dermis, usually to the depth of the papillary layer (depending on the area being assessed) without biopsy. In many cases, it can allow for the avoidance of dermatosurgical intervention. According to different publications, the time to diagnosis of MS usually ranges from 5 months to 5 years,6,9,26–28 reaching in extreme cases up to 15 years.10
As the disease is extremely rare, there are no randomized trials. It is suggested that the later treatment starts, the lower the chances of a full recovery.2 The first-line treatment of MS, described as beneficial, includes drugs typically used in rosacea (permethrin, brimonidine, and metronidazole), acne (oral isotretinoin, systemic doxycycline), oral antihistamines (e.g., ketotifen, desloratadine), and systemic corticosteroids.2,3,9,23,29–32 The combination therapy of low-dose isotretinoin (below 0.5 mg/kg) plus antihistamine is the treatment of choice. In the resistant cases, multiple additional options can be considered: intralesional triamcinolone, complex decongestive therapy, omalizumab, CO2 laser blepharoplasty with surgical eyelid debulking in cases of prominent eye-edema with bulking eyelids causing visual field narrowing.2,3,7,8,13,23,24 Complex decongestive therapy (CDT) includes manual lymphatic drainage, compression therapy, decongestive kinesitherapy, and proper skin care, aiming to increase the transport capacity of the lymphatic system.13 Single reports on successful lymphaticovenular anastomosis were published.33 Recently, two cases of Chinese adult patients treated successfully off-label with tofacitinib (Janus-activated kinase inhibitor) have been described.6
Isotretinoin is a synthetic vitamin A derivative (a stereoisomer of all-trans-retinoic acid) that causes, among others, the reduction of activity, involution and normalization of differentiation of the sebaceous glands. The proliferation of sebaceous glands, fibroblasts, and other connective tissue elements is inhibited. In addition, isotretinoin has a weak anti-inflammatory effect. Both high-dose and ultra-low-dose34 regimens are used in the treatment of MS. It is suggested that isotretinoin treatment in MS should last at least 12 months.27 Combination therapy with the addition of anti--inflammatory drugs (topical corticosteroids or calcineurin inhibitors) and antihistamines is often used. In two patients aged 18 and 20 years with facial edema associated with acne, treatment with external retinoids did not lead to improvement.9 Still, in the older one, the lesions regressed after systemic treatment with isotretinoin (20 mg/day) in combination with an antihistamine (not specified), while in the younger, after the combination treatment with the same dose of isotretinoin for 2 months and prednisone 2 mg/kg for 12 days.9 Isotretinoin is a teratogenic drug that demands birth control in women. The most common side effects are skin and mucus membranes dryness and abnormal liver function markers. In the presented patient, systemic isotretinoin was used for 22 months, with a cumulative dose of 200 mg per kg, with improved acne lesions and stabilization of the facial edema but not total clearance of MS.
In a systematic review including 89 patients with MS, male gender correlated with a lack of complete response to treatment, while the presence of papules or pustules among skin lesions correlated with a complete response. The longer antibiotic duration was associated with response to treatment, and mean antibiotic duration in patients who responded equalled 4.43 months; it was 2 months longer in the complete responders. Oral corticosteroids, isotretinoin, and combination therapies did not correlate with treatment response.2
Omalizumab is a humanized monoclonal antibody against IgE, produced by recombinant DNA technology from a Chinese hamster ovary cell line. It binds to the Fc fragment of free IgE to form biologically inactive complexes and prevents binding to the FcERI receptor on mast cells and basophils. This results in a decrease in free IgE. Omalizumab also contributes to decreased expression of FcERI receptors on mast cells and basophils, thereby increasing their reactivity threshold (stabilization). It is successfully used to treat atopic asthma and chronic spontaneous urticaria in adults and children.16,35 In 2014, omalizumab was approved by the US Food and Drug Administration and the European Medicines Agency for the treatment of chronic spontaneous urticaria (CSU) refractory to antihistamine therapy in adults and children at 12 years of age and older. In CSU, the drug dose is fixed and does not depend on the total IgE concentration. The dose registered for treatment in Europe is 300 mg, administered every 4 weeks.36 In treatment-resistant cases, the dose may be increased to a maximum of 600 mcg every 2 weeks.36 In recent years, numerous papers have been published on the use of omalizumab in other indications with pathogenesis potentially related to IgE, refractory to standard therapy such as eosinophilic esophagitis, bronchopulmonary aspergillosis, food allergy, contact eczema, eosinophilic granulomatosis with polyangiitis, autoimmune progesterone dermatitis, and bullous pemphigoid.16,37,38 The beneficial effect of omalizumab as a second-line treatment for MS has been described in one adult case, where due to lack of improvement after 4 months of isotretinoin treatment, omalizumab at an initial dose of 450 mg followed by 150 mg was introduced, with significant improvement.15 Our 15-year-old patient would be the youngest reported case of MS, successfully treated with off-label omalizumab at the standard CSU dose.
It is thought that urticaria and histaminergic angioedema have some pathophysiological similarities with Morbihan syndrome and rosacea through an elevated number or reactivity of mast cells. The immunohistochemical staining for mast cells in MS is not routinely used, as there is no similarity between the skin mastocytosis and MS histopathology. Fujimoto presumes that the presence and severity of mast cell infiltrate may explain the severity of edema, inflammation, and clinical response.39 The mast cells are not always present in MS; increased mast cell infiltrates are believed to cause dermal fibrosis. The presence of dermal fibrosis can explain why, in some cases, the edema can be reduced but not reverted without surgical or laser intervention.
The mechanism of action of omalizumab in MS has yet to be better described. It is presumed that by interfering with the binding of IgE to its receptor and downregulating FcεRI expression, omalizumab helps to reduce the activation of mast cells and basophils. This, in turn, leads to a decrease in the release of histamine and other inflammatory mediators contributing to edema development.16,35–38
The fact that the quality of life is still impaired after treatment is striking. The connection of low quality of life in skin diseases, independent of their severity, is well described. The possible explanation is the presence of the disease in the areas of the body always seen during social contact, in the mirror, etc., and the lack of possibility of camouflage. Patients with another skin disease, psoriasis, more often have depression and have a lower quality of life if the disease affects “special areas” defined as face, scalp, hands, and genitalia, even if the disease surface and severity are lower than in patients without special areas involved. 41
Conclusion
Morbihan syndrome is a challenge regarding diagnosis and treatment, regardless of patients’ age. This disease should also be considered in children and adolescents with persistent, solid face edema. Extensive diagnostic procedures, including skin biopsy, are recommended. It should be considered that disease significantly impacts the patient’s quality of life, especially in the sensitive period of adolescence. Regardless of young age and a short history of the disease, adolescents with MS may not respond to anti-acne treatment. Our case is the second description of omalizumab use in Morbihan syndrome, the first in adolescence. Omalizumab therapy is an effective and safe therapeutic option. Further studies are needed to determine the disease’s pathophysiology and develop effective treatment plans. Newly available drugs, such as anti-IgE antibodies and JAK inhibitors, give new insights into the pathophysiology of known diseases and show common features in different medical areas.
REFERENCES
1. Vasconcelos RC, Eid NT, Eid RT, Moriya FS, Braga BB, Michalany AO. Morbihan syndrome: A case report and literature review. An Bras Dermatol. 2016 Sep–Oct;91(5 Suppl 1):157–59. 10.1590/abd1806-4841.20164291
2. Boparai RS, Levin AM, Lelli GJ Jr. Morbihan disease treatment: two case reports and a systematic literature review. Ophthalmic Plast Reconstr Surg. 2019 Mar/Apr;35(2):126–32. 10.1097/IOP.0000000000001229
3. Mayur O, Martinez R, McNichol MC, McGee JS. Clinical and histological features and treatment outcomes of patients with Morbihan disease: A systematic review. Arch Dermatol Res. 2023 Apr 16;315:2427–429. 10.1007/s00403-023-02621-6
4. Ramirez-Bellver JL, Pérez-González YC, Chen KR, Díaz-Recuero JL, Requena L, Carlson JA, et al. Clinicopathological and Immunohistochemical study of 14 cases of morbihan disease: an insight into its pathogenesis. Am J Dermatopathol. 2019 Oct;41(10):701–10. 10.1097/DAD.0000000000001378
5. van der Linden MM, Arents BW, van Zuuren EJ. Diagnosis and treatment of Morbihan’s disease: a practical approach based on review of the Literature. J Clin Aesthet Dermatol. 2023 Oct;16(10):22–30.
6. Li ZY, Chi CC, Cai SQ. Case report: Morbihan disease treated with tofacitinib successfully. Front Immunol. 2023 Jun 5;14:1177316. 10.3389/fimmu.2023.1177316
7. Kim JH. Treatment of Morbihan disease. Arch Craniofac Surg. 2021 Jun;22(3):131–34. 10.7181/acfs.2021.00185
8. Yvon C, Mudhar HS, Fayers T, Siah WF, Malhotra R, Currie Z, et al. Morbihan Syndrome, a UK Case Series. Ophthalmic Plast Reconstr Surg. 2020 Sep–Oct;36(5):438–43. 10.1097/IOP.0000000000001589
9. Kuhn-Régnier S, Mangana J, Kerl K, Kamarachev J, French LE, Cozzio A, et al. A report of two cases of solid facial edema in acne. Dermatol Ther (Heidelb). 2017 Mar;7(1):167–174. 10.1007/s13555-017-0173-6
10. Zhang L, Yan S, Pan L, Wu SF. Progressive disfiguring facial masses with pupillary axis obstruction from Morbihan syndrome: A case report. World J Clin Cases. 2021 Aug 26;9(24):7163–68. 10.12998/wjcc.v9.i24.7163
11. Macca L, Li Pomi F, Motolese A, Broganelli P, Borgia F. Unilateral Morbihan syndrome. Dermatol Reports. 2021 Aug 5;14(2):9270. 10.4081/dr.2021.9270
12. Weeraman S, Birnie A. Rosacea causing unilateral Morbihan syndrome. BMJ Case Rep. 2019 Oct 25;12(10):e231074. 10.1136/bcr-2019-231074
13. Çinar GN, Özgül S, Nakip G, Üzelpasaci E, Baran E, Gürşen C, et al. Complex decongestive therapy in the physical therapist management of rosacea-related edema (morbus morbihan syndrome): A case report with a new approach. Phys Ther. 2021 Sep 1;101(9):pzab133.
14. Michelle Fog Andersen, Hilary J. Longhurst, Eva Rye Rasmussen, Anette Bygum. How not to be misled by disorders mimicking angioedema: A review of pseudoangioedema. Int Arch Allergy Immunol 1 June 2016; 169 (3):163–170. 10.1159/000445835
15. Kafi P, Edén I, Swartling C. Morbihan syndrome successfully treated with omalizumab. Acta Derm Venereol. 2019 Jun 1;99(7):677–78. 10.2340/00015555-3168
16. Yu L, Zhang H, Pan J, Ye L. Pediatric usage of Omalizumab: A promising one. World Allergy Organ J. 2021 Dec 11;14(12):100614. 10.1016/j.waojou.2021.100614
17. Nagasaka T, Koyama T, Matsumura K, Chen KR. Persistent lymphoedema in Morbihan disease: formation of perilymphatic epithelioid cell granulomas as a possible pathogenesis. Clin Exp Dermatol. 2008 Nov;33(6):764–67. 10.1111/j.1365-2230.2008.02892.x
18. García-Arpa M, Rodríguez-Vázquez M, Bellido-Pastrana D, Villasanti-Rivas N, Carmona-Rodríguez M. Persistent facial oedema and erythema in a woman, an uncommon manifestation of chronic cutaneous lupus erythematosus. Eur J Case Rep Inter Med 2020; Feb 12;7(3):1462.
19. Wohlrab J, Lueftl M, Marsch WC. Persistent erythema and oedema of the midthird and upper aspect of the face (morbus morbihan): evidence of hidden immunologic contact urticaria and impaired lymphatic drainage. J Am Acad Dermatol. 2005 Apr;52(4):595–602. 10.1016/j.jaad.2004.08.061
20. Veraldi S, Persico M, Francia C. Morbihan syndrome. Indian Dermatology Online Journal. 2013;Apr-Jun 4(2):122–24. 10.4103/2229-5178.110639
21. Tonkin R, Sladden C. What lies downstream? A case of superior vena cava syndrome presenting in the dermatology clinic: A case report. SAGE Open Med Case Rep. 2020 May 20;8:2050313X20. 10.1177/2050313X20919618
22. Kuraitis D, Coscarart A, Williams L, Wang A. Morbihan disease: A case report and differentiation from Melkersson-Rosenthal syndrome. Dermatol Online J. 2020 Jun 15;26(6):13030. 10.5070/D3266049317
23. Donthi D, Nenow J, Samia A, Phillips C, Papalas J, Prenshaw K. Morbihan disease: A diagnostic dilemma: two cases with successful resolution. SAGE Open Med Case Rep. 2021 Jun 11;9:2050313X211023655. 10.1177/2050313X211023655
24. Jerković Gulin S, Ljubojević Hadžavdić S. Morbihan disease–An old and rare entity still difficult to treat. Acta Dermatovenerol Croat. 2020 Aug;28(2):118–9.
25. Rizzo A, Fiorani D, Lazzeri L, Taddeucci P, Rubegni P, Flori ML, et al. Usefulness of in vivo reflectance confocal microscopy in Morbihan syndrome. Skin Res Technol. 2021 Sep;27(5):974–76. 10.1111/srt.13002
26. Guimarães MJ, Lopes AG, Vieira AP. Morbihan disease: A diagnostic and therapeutic challenge. Acta Med Port. 2023 Jun 28. 10.20344/amp.19904
27. Kim JE, Sim CY, Park AY, Hong SA, Park YL, Jang SY, et al. Case series of Morbihan disease (Extreme eyelid edema associated with rosacea): Diagnostic and Therapeutic Approaches. Ann Dermatol. 2019 Apr;31(2):196–200. 10.5021/ad.2019.31.2.196
28. Olvera-Cortés V, Pulido-Díaz N. Effective treatment of Morbihan’s disease with long-term isotretinoin: A report of three cases. J Clin Aesthet Dermatol. 2019 Jan;12(1):32–4.
29. Bagatin E, Costa CS, Rocha MADD, Picosse FR, Kamamoto CSL, Pirmez R, et al. Consensus on the use of oral isotretinoin in dermatology–Brazilian Society of Dermatology. An Bras Dermatol. 2020 Nov-Dec;95 Suppl 1(Suppl 1):19–38. 10.1016/j.abd.2020.09.001
30. Cribier B. Rosacea: Treatment targets based on new physiopathology data. Ann Dermatol Venereol. 2022 Jun;149(2):99–107. 10.1016/j.annder.2021.11.001
31. Borman P, Yaman A. Successful treatment for the different and rare cause of facial lymphedema: Morbus Morbihan disease. Int J Dermatol. 2022 Jan;61(1):103–105. 10.1111/ijd.15643
32. Anderson MS, Nadkarni A, Cardwell LA, Alinia H, Feldman SR. Spotlight on brimonidine topical gel 0.33% for facial erythema of rosacea: safety, efficacy, and patient acceptability. Patient Prefer Adherence. 2017 Jul 6;11:1143–150. 10.2147/PPA.S115708
33. Hong JH, Yi CC, Lee JW, Bae YC, Kim RS, Kim JH. Lymphaticovenular anastomosis for Morbihan disease: A case report. Arch Craniofac Surg. 2023 Jun;24(3):124–28. 10.7181/acfs.2022.01067
34. Welsch K, Schaller M. Combination of ultra-low-dose isotretinoin and antihistamines in treating Morbihan disease–A new long-term approach with excellent results and a minimum of side effects. J Dermatolog Treat. 2021 Dec;32(8):941–44. 10.1080/09546634.2020.1721417
35. Skander D, Allenova A, Maurer M, Kolkhir P. Omalizumab is effective in patients with chronic spontaneous urticaria plus multiple chronic inducible urticaria. Eur Ann Allergy Clin Immunol. 2021 Mar;53(2):91–3. 10.23822/EurAnnACI.1764-1489.153
36. Zuberbier T, Maurer M. Omalizumab for the treatment of chronic urticaria. Expert Rev Clin Immunol. 2015 Feb;11(2):171–80. 10.1586/1744666X.2015.993971
37. Varghese A, Paul T, Kim H, Van Uum S, Vadas P, Azzola A. Effect of omalizumab for autoimmune progesterone dermatitis refractory to bilateral oophorectomy: A case report. Allergy Asthma Clin Immunol. 2021 Jun 13;17(1):58. 10.1186/s13223-021-00561-2
38. Sarrazin M, Jouen F, Duvert-Lehembre S. Refractory bullous pemphigoid with IgE anti-BP230 and IgG anti-p200 antibodies successfully treated with omalizumab. Ann Dermatol Venereol. 2021 Mar;148(1):60–62. 10.1016/j.annder.2020.08.053
39. Fujimoto N, Mitsuru M, Tanaka T. Successful treatment of Morbihan disease with long-term minocycline and its association with mast cell infiltration. Acta Derm Venereol. 2015 Mar;95(3):368–69. 10.2340/00015555-1954
40. Blauvelt A, Gondo GC, Bell S, et al. Psoriasis Involving special areas is associated with worse quality of life, depression, and limitations in the ability to participate in social roles and activities. Journal of Psoriasis and Psoriatic Arthritis. 2023;8(3):100–106. 10.1177/24755303231160683
Supplementary
Table S1. Skin prick test results, brand: Allergopharma GmbH & Co. KG
| Skin prick test – inhalant allergens | |
| Name of the allergen | Diameter of wheal in mm |
| Negative control | 0×0 |
| Histamine | 4×4 |
| Grass | 0×0 |
| Mugwort | 0×0 |
| Birch | 0×0 |
| Alder | 0×0 |
| Hazel | 0×0 |
| Rye | 0×0 |
| Plantago major | 0×0 |
| D. pteronyssinus | 0×0 |
| Skin prick test – food allergens | |
| Name of the allergen | Diameter of wheal in mm |
| Negative control | 0×0 |
| Histamine | 4×4 |
| Chicken meat | 0×0 |
| Beef | 0×0 |
| Pork | 0×0 |
| Cod | 0×0 |
| Carp | 0×0 |
| Orange | 0×0 |
| Banana | 0×0 |
| Peanuts | 0×0 |
| Hazelnuts | 0×0 |
| Tomato | 0×0 |
| Rye flour | 0×0 |
| Wheat flour | 0×0 |
| Cow milk | 0×0 |
| Chicken egg | 0×0 |
Table S2. Differential diagnoses of facial oedema and Morbihan syndrome5,14, 18-22
| Differential diagnoses of facial oedema | |
|---|---|
| Infectious disease | Erysipelas Tuberculosis Leprosy Leishmaniasis |
| Autoimmune disease | Systemic lupus erythematosus Dermatomyositis Granulomatosis with polyangitiis Melkersson-Rosenthal syndrome |
| Allergic disease | Urticaria Allergic contact dermatitis Angioedema (hereditary and acquired), histaminergic, and bradykinin-induced |
| Neoplastic disease | Cutaneous lymphoma Leukemias Angiosarcomas Lymphosarcomas |
| Congenital disease | Mucopolysaccharidosis (Hurler’s syndrome) Congenital hemifacial hyperplasia Sturge-Weber syndrome |
| Other diseases | Nephrotic syndrome Sarcoidosis Amyloidosis Hypothyroidism (with Myxedema) |