
Download

ORIGINAL ARTICLE
Mexican consensus on cow’s milk protein allergy
Ramírez Mayans Jaime Alfonsoa, Ignorosa Arellano Karen Rubía*, Toro Monjaraz Erick Manuela, Cervantes Bustamante Robertoa, Ruiz Castillo Marlene Alejandrab, Medina Vera Isabel de Jesúsc, Ayala Germán Ana Gabrielad, Bacarreza Nogales Dante Vladimire, Casas Guzik Lucíaf, Chávez Barrera José Antoniog, Díaz Madero Sergioh, Flores Fong Laura Estheri, Galaz Pantoja Méndez Manuel Enriquej, Gris Calvo Judith Ileanak, Huerta Hernández Rosa Elenal, Limón Rojas Ana Elenam, Macías Avilés Héctorn, Méndez Nieto Carloso, Ortega Martell José Antoniol, Oyervides García Carlos Ivánp, Peña Vélez Rubénq, Reynés Manzur José Nicolásr, Saez de Ocariz Gutiérrez María del Mars, Sagols Méndez Gerardot, Uriquidi Rivera Martha Eugeniau, Worona Dibner Lilianav, Wakida Kusunoki Guillermo Hideow, Vandenplas Yvanx
aPediatric Gastroenterology and Nutrition Department, Instituto Nacional de Pediatria, Mexico City
bPediatric Gastroenterology, Hospital del Niño DIF, Hidalgo México
cResearch Methodology Department, Instituto Nacional de Pediatria, Mexico City
dPediatric Gastroenterology, Hospital General Agustín O Haran, Mérida, Yucatán, México
ePediatric Gastroenterology, Hospital General Zona 1 IMSS, Tijuana, México
fPediatric Gastroenterology, Hospital Infantil de Morelia Eva Sámano de López Mateos, Morelia, México
gPediatric Gastroenterology, Hospital General del Centro Médico Nacional La Raza, IMSS, Mexico City
hPediatric Gastroenterology, Hospital Español, Mexico City
iPediatric Gastroenterology, Hospital Civil de Guadalajara, Mexico
jPediatric Gastroenterology, Hospital General Chiapas, Mexico
kGastroenterology and Nutrition Service, Instituto Nacional de Pediatria, Mexico City
lClínica de Alergia Pediátrica, Pachuca, Hidalgo, Mexico
mPediatrics, Secretaría Clínica Facultad de Medicina, UNAM, Mexico City
nPediatric Neonatology, Instituto Nacional de Pediatria, Mexico City
oPediatric Gastroenterology, Hospital Infantil de Especialidades, Ciudad Juárez, Mexico
pPediatric Gastroenterology, Hospital del Niño Dr. Federico Gómez Santos, Saltillo, Coahuila, Mexico
qPediatric Gastroenterology, Hospital General de Puebla Dr. Eduardo Vázquez N., Puebla, Mexico
rInternal Medicine, Instituto Nacional de Pediatria, Mexico City
sPediatric Dermatologist, Instituto Nacional de Pediatria, Mexico City
tPediatric Gastroenterology, Clínica de Mérida, SA de CV, Merida, Mexico
uPediatric Gastroenterology, ISSSTE Hospital Regional Monterrey, Nuevo León, Mexico
vPediatric Gastroenterology, Hospital Infantil de México Federico Gómez, Mexico City
wPediatric Allergy and Immunology, Hospital Central Sur de Alta Especialidad de Petróleos Mexicanos, Mexico City
xPediatric Gastroenterology, KidZ Health Castle, UZ Brussel; Vrije Universiteit Brussel, Brussels, Belgium
*Corresponding author: Karen Rubí Ignorosa Arellano, Pediatric Gastroenterology and Nutrition Department, Instituto Nacional de Pediatria, Mexico City, Insurgentes Sur 3700-C, Insurgentes Cuicuilco, Coyoacán, CP 04530, Ciudad de México. Email address: [email protected]
Abstract
Background: The aim of this study is to present the current views of a diverse group of experts on the diagnosis and treatment of Cow’s Milk Protein Allergy (CMPA) in children under 2 years of age in Mexico.
Material and methods: The study, led by a scientific committee of five experts in CMPA, was divided into six phases, including a modified Delphi process. A total of 20 panelists, all of whom were pediatric specialists, participated in administering a comprehensive 38-item questionnaire. The questionnaire was divided into two blocks: Diagnosis and Treatment (20 items each).
Results: Consensus was reached on all the proposed items, with an agreement rate of over 70% for each of them. As a result, a diagnostic and treatment algorithm was developed that emphasized the reduction of unnecessary diagnostic studies and encouraged breastfeeding whenever possible. In cases where breast milk is not available, appropriate use of hypoallergenic formulas was recommended. In addition, recommendations on treatment duration and gradual reintroduction of cow’s milk protein were provided.
Conclusions: The recommendations endorsed by 20 Mexican pediatricians through this study are applicable to everyday clinical practice, thereby enhancing the diagnosis and treatment of children under 2 years of age with CMPA. This, in turn, will foster improved health outcomes and optimize the utilization of healthcare resources.
Key words: Consensus, Cow’s Milk Protein Allergy, Delphi, Hypoallergenic Formulas, Tolerance
Received 17 July 2023; Accepted 4 October 2023; Available online 1 January 2024
Copyright: Ramírez Mayans JA, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Cow’s milk protein allergy (CMPA) can be described as a repeated immune response that occurs in the presence of cow’s milk-derived proteins, and is the most prevalent form of allergy seen in infants and young children.1 It is recognized as the outcome of an atypical immune response, encompassing IgE-mediated, non-IgE-mediated, or mixed reactions, to proteins found in cow’s milk (CMP).2 The IgE-mediated immune response is characterized by an immediate onset (within the first 2 h after contact with the allergen), predominantly featuring cutaneous and respiratory symptoms, as well as the presence of specific IgE antibodies in the blood or positive results from skin tests (prick test).2 In contrast, the non-IgE-mediated response manifests later and primarily involves digestive symptoms. Reliable diagnostic methods have not been established for all cases, as this response is caused by various cells and cytokines. It covers conditions such as food protein-induced allergic proctocolitis (FPIAP), food protein-induced enterocolitis syndrome (FPIES), food protein-induced enteropathy syndrome (FPE), and eosinophilic gastrointestinal disorders (EGID), including eosinophilic esophagitis (EoE). Some manifestations are less specific and can be confused with functional disorders of the brain–gut axis, such as regurgitation, colic, and constipation.2
The prevalence of this allergy fluctuates depending on age, geographic location, and the specific risk groups involved.3 Prior to the 1950s, it is worth noting that diagnosis of CMPA was rare.4 However, since the 1970s, an increase in its incidence has been observed, and currently there are reports indicating prevalence ranging from 1.8 to 7.5%.4 This wide variation and discrepancy in prevalence is due to several factors, including the different methods used as diagnostic criteria for assessing the immune response, as well as the clinical criteria used in each study.5 In addition, the high degree of heterogeneity present in populations and geographic areas could also contribute to this variability.5
According to the European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN),6 approximately 50% of children with CMPA develop tolerance to cow’s milk proteins by the age of 12 months, more than 75% by the age of 3 and 90% by the age of 6 years. CMPA manifests widely, affecting different organs, from colic and gastroesophageal reflux to gastrointestinal bleeding (hematochezia).7 A comprehensive understanding of these clinical manifestations is crucial for general practitioners, pediatricians, neonatologists, allergists, gastroenterologists, dermatologists, and nutritionists who provide care for the infant population.
The World Allergy Organization (WAO) published the first guidelines (DRACMA) on CMPA in 2010,8 laying the foundation for the development of subsequent guidelines. In recent years, numerous guidelines and papers have been published, providing recommendations for diagnosing and treating CMPA. Specifically, in Latin America, a consensus was published in 2014.9 However, due to the unique characteristics of the Mexican healthcare context—shaped by a mixed health system, traditional dietary patterns, economic considerations, regional variations in medical training, cultural beliefs, and country-specific guidelines10—it is essential to reach an expert consensus on this issue. This would promote the efficient use of healthcare resources, inform clinicians, benefit patients, and support public policies.
The aim of the present consensus is to develop a practical and useful guide for diagnosing and treating CMPA in Mexican children under 2 years of age, considering local realities and applicable to both primary and specialized care centers.
Material and Methods
Study design
The study was designed using the modified Delphi consensus method, a structured technique widely used in various areas to gather relevant information on a specific topic.11 This method involves formulating a series of questions addressed to experts in the field of study. This approach’s distinctive and fundamental characteristics are the anonymous response by participants and controlled feedback.12
Study phases
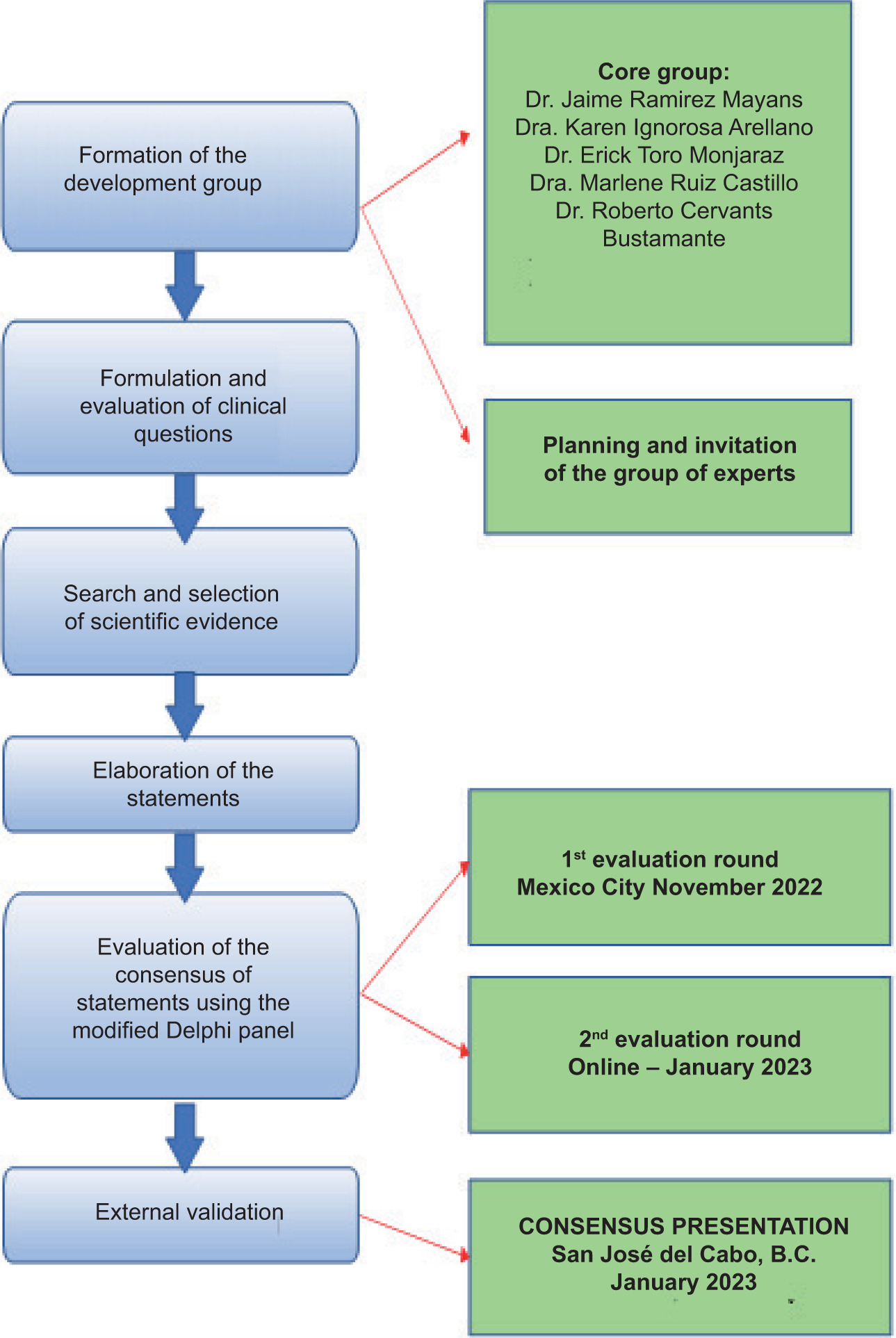
The study was conducted by following a series of defined steps (Figure 1).
Figure 1 Study developments phases.
Formation of the development group
This phase involved establishing a scientific committee comprising pediatric gastroenterologists. The committee members engaged in remote work meetings utilizing online platforms. These meetings served to define the work approach, set deadlines, and distribute responsibilities. Additionally, the essential aspects of the overall scope of the consensus were agreed upon. Following the establishment of initial points, another meeting was convened to generate a list of structured clinical questions that addressed crucial areas of clinical importance aligned with the consensus’s objective.
Formulation and evaluation of clinical questions
The scientific committee identified the topics to be addressed in the consensus, considering relevant aspects of the Mexican health context. The structured clinical questions were developed by consensus, and a panel of Mexican experts in pediatrics from various subspecialties was formed.
Search and selection of scientific evidence
An exhaustive search of scientific evidence published during the last 10 years, since June 22, 2022, was conducted. MeSH (Medical Subject Headings) terms including “Cow’s milk protein allergy,” “hypoallergenic formulas,” and “tolerance” were used in accordance with the clinical questions, and filters for “Child (birth-18 years)” and “human” studies were applied. The search was carried out in Pubmed or Medline in English; LILACS in Spanish; and the Cochrane Library, Cochrane Central Register of Controlled Trials, and Cochrane Database of Systematic Reviews.
Elaboration of the statements
The questions were assigned to the experts according to their experience, and the statements were drafted according the scientific evidence analyzed and the group of experts’ clinical experience.
Evaluation of the consensus of statements using the modified Delphi Panel
After gathering the statements for each clinical question, they were consolidated into a unified document, and the panel of experts was assembled for evaluation. The evaluation process consisted of two rounds. The first round took place face-to-face on November 4, 2022, where an oral summary of the evidence chosen for each statement was presented. The second round was conducted online through the Survey Monkey platform in January 2023. Subsequently, on January 26, 2023, the scientific committee convened in person to assess the voting outcomes.
External validation
External validation took place during a keynote presentation by Dr. Jaime Alfonso Ramírez Mayans, Dr. Karen Rubí Ignorosa Arellano, Dr. Erick Toro Monjaraz, Dr. Marlene Ruiz Castillo and Dr. Isabel Medina Vera during an event for pediatricians in January 2023. This event took place in the city of San José del Cabo, BCS, Mexico.
Scientific committee
The project’s leadership was entrusted to a scientific committee consisting of a distinguished team of five pediatric specialists from various medical centers located throughout Mexico. These professionals stand out for their extensive knowledge of the pediatric care process of CMPA.
Panel of experts
A select group of 20 experts in pediatrics was convened to ensure an exhaustive representation of all the country’s regions. The criteria for their selection were based on their professional competence and their vast experience in the field of pediatric CMPA. Supplementary Table 1 shows the names and affiliations of the panelists involved in this consensus.
Table 1 Recommendations for the diagnosis of CMPA in children under 2 years of age in the Mexican health context (Block I).
| Recommendation | Median | % | |
|---|---|---|---|
| Q1 | When regurgitations persist and do not improve after correcting feeding technique, use of thickeners or even with the usual pharmacological treatment, or when irritability is present, or associated with other allergic symptoms, such as atopic dermatitis, the diagnosis of CMPA should be considered. | 8 (7–9) | 100 |
| Q2 | In infants with colic as the only symptom, CMPA is a rare diagnosis. | 8 (7–9) | 100 |
| Q3 | In infants with constipation, who do not respond to conventional treatment, CMPA should be considered as a possible cause. | 8 (7–9) | 92 |
| Q4 | The association of sleep disorders with CMPA is an area of opportunity for research, since in practice it is reported by caregivers, but there is not enough scientific evidence to support this association. | 8 (8–9) | 100 |
| Q5 | The use of the CoMiSS questionnaire is not sufficient for the diagnosis of CMPA. | 9 (8–9) | 88 |
| Q6 | The oral elimination and challenge test is considered the “gold standard” for diagnosing food allergy, as it can minimize false positives. | 8 (7–9) | 88 |
| Q7 | The challenge test carries the risk of a severe reaction in a patient who is highly sensitive (with severe symptoms) to cow’s milk proteins, so it should not be performed routinely in daily practice, but only in specialized centers with the expertise and equipment to perform or treat it. | 8 (6.5–9) | 76 |
| Q7 | The double-blind, placebo-controlled challenge is considered the gold standard in the diagnosis of CMPA, but in practice only an open challenge is performed. | 8 (6.5–9) | 76 |
| Q8 | The patient with suspected CMPA should follow an exclusion diet for 2–4 weeks; formula-fed infants will be started on extensively hydrolyzed whey or casein formula, or hydrolyzed rice formula, and exclusively breastfeeding mothers will implement a cow’s milk protein-free diet. If CMPA is present, the clinical manifestations will disappear. | 8(8–9) | 100 |
| Q9 | Family history of allergic disease (atopy), history of other allergic diseases in the patient (allergic asthma, allergic rhinitis, allergic atopic dermatitis), early onset (minutes to 4 h) of symptoms after exposure to milk, and the type of clinical manifestations (urticaria, bronchospasm, anaphylaxis) may further orient toward suspicion of IgE-mediated allergy in children under 2 years of age. | 8 (8–9) | 96 |
| Q10 | Demonstrating an IgE-dependent mechanism in the first year of life allows for the establishment of early dietary interventions, thus decreasing the progression of the allergic march. | 8 (7–9) | 92 |
| Q10 | Determination of specific IgE to cow’s milk proteins, especially casein, lactoglobulin, and lactalbumin, by PRICK and immunocap tests is necessary to demonstrate an IgE-mediated allergy. | 8 (7–9) | 92 |
| Q11 | Patch tests have been used to try to diagnose non-IgE-mediated CMPA allergy; however, the results reported in the literature have been variable and contradictory, probably due to the lack of standardization in the tests. | 8 (7–9) | 88 |
| Q11 | Patch tests have not shown to be useful in diagnosing non-IgE-mediated CMPA. | 8 (7–9) | 88 |
| Q12 | Currently, measurement of IgE specific to allergenic components of milk may help to find cross-reactivity between components, which may be important in making decisions about the type of milk a patient can tolerate or not. These studies require experience for proper interpretation. | 8 (7–9) | 92 |
| Q12 | The elevation of total IgE is not a useful or exclusive marker of allergic sensitization and can only indicate a genetic predisposition to respond with this antibody to different environmental stimuli (atopy). | 8 (7–9) | 92 |
| Q13 | Fecal calprotectin determination is not recommended for diagnosis and follow-up in patients with CMPA. | 9 (8–9) | 100 |
| Q14 | The determination of reducing sugars in stool is not valid for the diagnosis of patients with suspected CMPA. | 9 (7.5–9) | 96 |
| Q15 | Endoscopy and colonoscopy can be useful to rule out other differential diagnoses or when the evolution of symptoms is not as expected after adequate dietary treatment. | 9 (8–9) | 96 |
| Q15 | The most common diseases with which CMPA in children under 2 years of age can be confused are eosinophilic disorders of the gastrointestinal tract such as esophagitis, gastroenteritis, or eosinophilic colitis, in which mucosal infiltration by eosinophils is observed. Other differential diagnoses include celiac disease, H. pylori infection and gastroesophageal reflux disease. | 8 (8–9) | 96 |
Definition of consensus
The statements included in the Delphi were answered on a nine-point Likert-type scale, divided into three sections, “disagree” (scores 1–3), “neutral” (scores 4–6), and “agree” (scores 7–9). A median of 7 and a percentage of at least 70% of experts in the “agree” section were established as minimum consensus criteria. If any recommendation did not meet these criteria, the clinical arguments provided by the experts were considered in order to make modifications and present them in the second round of evaluation.
Data analysis
SPSS software for MAC (version 25.00, SPSS Inc., Chicago, IL) was used to create and analyze the database. The median, and 25th and 75th percentile, and the percentage of responses in the range of 7–9 were calculated and used to define the consensus.
Results
The scientific committee devised a total of 40 statements distributed into two blocks, diagnosis (Block I, 20 statements; Table 1), and treatment (Block II, 20 statements; Table 2). Of the 20 experts invited to participate in the Delphi process, all of them responded to the questionnaire (100%). The panel’s experts reached a consensus of “agreement” on all the proposed statements.
Table 2 Recommendations for the treatment of CMPA in children under 2 years of age in the Mexican health context (Block II).
| Recommendation | Median | % | |
|---|---|---|---|
| Q16 | The mother on a cow’s milk protein exclusion diet should supplement her diet with vitamin D and calcium. | 9 (8–9) | 100 |
| Q16 | The mother on cow’s milk protein elimination diet should be supplemented with a vitamin D dose of 400–800 IU and 1000 mg/day of calcium. | 9 (8–9) | 100 |
| Q16 | Vitamin D and calcium supplements should be monitored to ensure that they are not contaminated with cow’s milk protein. | 9 (8–9) | 100 |
| Q16 | The diet of the mother on a cow’s milk protein restriction diet should be guided by a nutrition specialist to avoid detrimental diets. | 9 (8–9) | 100 |
| Q17 | For the treatment of CMPA, extensively hydrolyzed cow’s milk protein (EHF) formulas are considered the first therapeutic option in patients with CMPA, especially in those with mild or moderate involvement. However, up to 10% of infants may not tolerate this type of formulas and other types should be considered. | 8 (8–9) | 100 |
| Q17 | So far, there are no clinical trials comparing the benefits of EHF formulas formulated with casein with those of whey, so there is no recommendation on their preference in the treatment of CMPA in infants. | 9 (8–9) | 100 |
| Q18 | In the treatment of CMPA, partial and extensively hydrolyzed rice formulas are a first-line option for management, as they have been shown to be safe, without nutritional risks and efficient compared to conventional treatment. | 9 (8–9) | 96 |
| Q18 | Arsenic levels contained in an average daily volume of hydrolyzed rice formula (600–800 ml) do not imply a risk for the treatment of infants with CMPA, as they account for 0.16–0.23 μg/kg, amounts 10 times lower than the limits established by WHO (0.10 mg/kg). | 9 (8–9) | 96 |
| Q19 | Amino acid–based formulas (AAF) are indicated as first line in infants at risk of adverse reaction to extensively hydrolyzed formulas, or severe initial clinical picture (anaphylaxis or Heiner’s syndrome, multiple food allergies, severe atopic dermatitis, rectal bleeding with hemodynamic instability, hypoproteinemia, eosinophilic esophagitis, severe anemia, or significant nutritional deterioration). | 9 (8–9) | 100 |
| Q19 | AAF are recommended as second-line therapy in case of treatment failure with extensively hydrolyzed formulas in children with CMPA. | 9 (8–9) | 100 |
| Q19 | AAF are not the formula of first choice in infants with CMPA due to their high cost, lower palatability and higher osmolarity. | 9 (8–9) | 100 |
| Q20 | Soy formulas can be considered as a safe second-line option in the management of infants with CMPA, in cases where they require an alternative, do not accept the bitter taste of hydrolyzed or amino-acid formulas, or in cases where the high cost of these formulas is a limiting factor. | 8 (7–9) | 80 |
| Q20 | Current soy formulas can be considered nutritionally complete, as they are supplemented with methionine, iodine, carnitine, taurine, choline, inositol, LCPUFA, and micronutrients to avoid deficiencies. | 9 (8–9) | 100 |
| Q20 | Industrial soy-based beverages are totally inadequate to meet the nutritional needs of the infant with CMPA allergy and therefore should not be used. | 9 (8–9) | 100 |
| Q21 | It is not recommended to use partially hydrolyzed formulas in the treatment of CMPA. | 8 (7.5–9) | 88 |
| Q22 | More studies are needed to be able to recommend prebiotics, in the prevention and treatment of CMPA. | 9 (8–9) | 96 |
| Q23 | More studies are needed to be able to recommend probiotics in the prevention and treatment of pediatric CMPA. | 9 (7–9) | 92 |
| Q24 | More studies are needed to be able to recommend symbiotics in the prevention and treatment of pediatric CMPA. | 9 (7–9) | 96 |
| Q25 | It is recommended to maintain a cow’s milk protein elimination diet for at least 6 months or until 9–12 months of age. In children with CMPA allergy with severe immediate IgE-mediated reactions, it may be extended from 12 to 18 months. | 8 (8–9) | 88 |
| Q26 | Patients with persistent CMPA may benefit from the introduction of baked milk; several studies suggest that the introduction of baked milk products may increase the likelihood of CMPA resolution and/or accelerate the process. This strategy is part of what is now known as the milk ladder. | 8 (8–9) | 88 |
Discussion
The clinical management of children under 2 years of age with CMPA in Mexico was addressed for the first time through this consensus. A total of 20 physicians, specialists in pediatrics, validated the recommendations through a modified Delphi methodology. The experts reached a consensus on various aspects of diagnosis (Block I) and treatment (Block II), which will guide various medical specialists in their clinical decision-making for managing patients under 2 years of age with CMPA.
Based on the results of this consensus, we developed a summary of the signs and symptoms associated with CMPA (Table 3) and a simplified algorithm for diagnosing and treating CMPA (Figure 2).
Table 3 Summary of clinical signs and symptoms of CMPMA in children under 2 years of age.
| Non-IgE mediated | IgE mediated | |
|---|---|---|
| General | Colic Irritability Growth arrest |
Anaphylaxis |
| Gastrointestinal | Feeding refusal Dysphagia Regurgitation Vomiting diarrhea Constipation Perianal erythema Hematochezia |
Regurgitation Vomiting Diarrhea |
| General | Rhinitis Wheezing Chronic cough |
Rhinitis and/or conjunctivitis Asthma Dysphonia |
| Gastrointestinal | Atopic dermatitis | Atopic dermatitis Urticaria Angioedema Oral allergy syndrome |
Figure 2 Alogrithm for diagnosing and treating CMPA in children under 2 years of age in the Mexican health context.
*1–2 weeks for children with late clinical reactions (e.g. atopic dermatitis, rectal bleeding); CMP = Cow’s Milk Protein; CPMA = Cow’s milk protein allergy; HM: human milk; SPT = skin prick test.
Diagnostic block (Block I)
Symptoms
CMPA can exhibit symptoms similar to those found in infants with functional gastrointestinal disorders (FGID), such as colic, gastroesophageal reflux, and constipation.11 Therefore, in this consensus, it was deemed essential to address this matter and provide a set of clinical recommendations that help to distinguish between either condition. The diagnosis of CMPA should be considered when there is persistent regurgitation that does not improve with thickening agents or standard pharmacological treatment, alongside irritability or other allergy symptoms such as atopic dermatitis. This consensus statement is in line with the clinical practice guidelines for pediatric gastroesophageal reflux by the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) and the ESPGHAN. These guidelines recommend considering the diagnosis of CMPA when overfeeding has been excluded or when thickening treatments have been ineffective.13
Colic is a common gastrointestinal issue in children and can be associated with both CMPA and FGID.14 However, CMPA is an infrequent diagnosis in infants who only present with colic as the symptom,15 as agreed upon by the expert group. Therefore, the presence of colic alone should not be considered a definitive symptom of CMPA, and cow’s milk protein elimination diet is not routinely recommended in mothers of exclusively breastfed infants with colic as the only manifestation.16
Constipation is another frequent disorder in young children.17 PLV is a food allergen that can affect gastrointestinal motility and is involved in constipation.18 For this reason, several recommendations on this topic have been made in this consensus. In particular, it was agreed that in infants with constipation who do not respond to conventional treatment, CMPA should be considered a possible cause of constipation. This statement can be supported by studies citing CMPA as a cause of constipation.19
Sleep disturbance is another symptom that has been associated in some studies with CMPA’s presence in children.20–22 However, it is important to note that the existing evidence in this regard is limited. The expert panel reached a consensus on this statement and acknowledged the need for further exploration in this area, given that caregivers of children with CMPA often report these sleep-related issues.
Diagnostic tests
The CoMISS questionnaire, developed in 2015, enables the evaluation of children with suspected CMPA through a questionnaire of general, dermatological, respiratory and gastrointestinal symptoms.23 Voting by participants resulted in the consensus that the CoMISS questionnaire is not the only tool needed for diagnosing CMPA. This statement is in line with publications indicating that the CoMiSS questionnaire has clinical utility, as it can serve as a tool for awareness of possible CMPA when the score is ≥12, but it needs to be complemented with more clinical data and tests for diagnosing CMPA.23,24
Among the diagnostic tests for CMPA are the oral food challenges (OFCs). Expert opinion resulted in agreement that the OFC should be considered the “gold standard” for diagnosing food allergy. Using this test to confirm or exclude the diagnosis of CMPA has also been recommended by other clinical guidelines for all patients with suspected CMPA.6,25–28 The DRACMA guideline in its 2010 edition indicated that this test should be considered the “gold standard,”8 also indicating some weaknesses that should be considered by clinicians in its latest update.29 Among this test’s weaknesses is the patient’s exposure to the potential allergen, with the consequent possibility of triggering an allergic reaction. The expert consensus highlights the potential risk of severe reactions in patients who are highly sensitive to CMP, and therefore advises against the routine use of this test in daily practice for individuals with severe symptoms. Instead, it recommends that such testing be conducted exclusively in specialized centers equipped with the necessary expertise and resources to manage and treat severe reactions, should they occur. Other guidelines have previously indicated this need, not only for medical supervision but also for performing OFC in centers with the necessary facilities.8,25,28 Large-scale studies on the prevalence of life-threatening reactions to CMP are currently lacking; however, Badina et al. observed a prevalence of 6.3% of patients experiencing life-threatening reactions within their pediatric cohort of individuals with CMPA.30 Given the substantial number of patients diagnosed with CMPA, the potential for a significant proportion of individuals to experience such life-threatening reactions becomes evident, underscoring this recommendation’s critical importance. If there is a history suggestive of FPIES or if severe associated symptoms are present, performing an oral challenge for diagnosis is not necessary. While the ideal time to perform an oral challenge for FPIES has not been systematically studied and varies between countries, most data suggest that the test can be conducted between 12 and 18 months after diagnosis.16,31
While the double-blind, placebo-controlled challenge test (DBPCFC) is widely regarded as the “gold standard” for diagnosing CMPA,30,31 experts have reached a consensus that, in practical terms, the OFC is more commonly employed. The double-blind, placebo-controlled challenge is the only test that blinds the parent and the physician to the introduction of CMP and is therefore considered the only objective measure for making a diagnosis of CMPA.32 Unfortunately, it involves carrying out a process that is complex, expensive, time-consuming, and demanding in terms of preparation and execution.33 As a result, it is recommended that alternative approaches, such as the OFC, be utilized in routine clinical practice due to their practicality and compatibility with available resources. The OFC method offers a simpler and quicker process, reducing the strain on healthcare resources.32
Elimination diet
Regarding the duration and content of the elimination diet for diagnosing CMPA, the experts reached a consensus that the patient with suspected CMPA should follow an exclusion diet for a period of 2–4 weeks. This period is in line with other published guidelines.6,33 However, it should be noted that the ESPGHAN guidelines suggest a shorter period (1–2 weeks) for children experiencing late clinical reactions, such as atopic dermatitis or rectal bleeding.6
Diagnosis of CMPA subtype
Regarding the subtype of CMPA presented by the child, the experts agreed that it is important to study whether it is an IgE-dependent mechanism from the first two years of life, because this could help to reduce the progression of allergic diseases (allergic march). They also agreed that a family history of allergic disease (atopy), a history of other allergic diseases in the patient (allergic asthma, allergic rhinitis, allergic atopic dermatitis), early presentation (minutes to the first 4 h) of symptoms after exposure to milk and various types of clinical manifestations (urticaria, bronchospasm, anaphylaxis) are more common in IgE-mediated CMPA patients and should therefore be a clinical suspicion. This suspicion is not sufficient for diagnosis, but the determination of specific IgE to cow’s milk proteins, especially casein, lactoglobulin, and lactalbumin, is necessary for demonstrating an IgE-mediated allergy. This determination can be conducted in vivo by skin prick testing or in vitro by quantification of serum levels of IgE specific to these proteins (ImmunoCAP).
Experts agreed not to recommend patch tests for diagnosing non-IgE-mediated allergy. The explanation for this statement is that the results reported in literature on the subject are variable and contradictory, probably due to the lack of standardization in the tests.2 Future studies will be necessary for validating this test. Experts also do not recommend measuring specific IgG antibodies or using other nonstandardized tests, such as determining IgG subclasses against cow’s milk proteins, as there is no evidence that these can establish the diagnosis of non-IgE-mediated allergy.31
Total IgE levels can be elevated by infections caused by helminths, fungi, or viruses, as well as by autoimmune, neoplastic, or immunodeficiency diseases, in addition to allergic diseases.34 Elevation of total IgE, that is, serum total IgE, is neither a useful nor an exclusive marker for diagnosing allergic sensitization,35 as was agreed by experts. Total IgE is a type of antibody that is associated with allergic responses, but its elevation does not definitively indicate the presence of a specific allergy.
Other diagnostic tests
Fecal calprotectin, a cytosolic protein that increases when there is inflammation in the intestinal mucosa, could be a possible biomarker of CMPA.36 However, the current evidence is not sufficient to confirm its usefulness either for diagnosis and follow-up of CMPA or for prediction of allergic diseases.36 Experts agreed not to recommend fecal calprotectin determination for diagnosis and follow-up in patients with CMPA. Further clinical and laboratory investigations may provide more information in the future on this biomarker’s clinical use in the context of CMPA.
Because the symptoms of lactose intolerance and CMPA are similar, cases of CMPA are sometimes confused with and misdiagnosed as lactose intolerance.37 This is because lactose intolerance is more common than CMPA in terms of prevalence.37 The reducing sugar test is able to detect (in patients’ stools) the presence of lactose and other sugars from the same family.37 This test should not be used to diagnose CMPA according to the experts’ consensus, because the presence of this type of sugar is not related to the presence of CMPA in patients but to other diseases such as lactose intolerance or in children with short bowel syndrome to differentiate the origin of diarrhea.
Regarding the use of endoscopy and/or colonoscopy or rectosigmoidoscopy in children with CMPA, there is insufficient scientific evidence to support the existence of histological signs characteristic of patients with CMPA.38 Macroscopic or histopathological lesions such as inflammation, villous atrophy, or infiltration with eosinophils are not specific for diagnosing CMPA.38 However, histologic lesions are typical of diseases of the gastrointestinal tract, with symptoms shared by pediatric patients with CMPA.39,40 Experts agreed that endoscopy and colonoscopy can be useful tools for excluding other diseases or when the evolution of symptoms is not as expected after adequate dietary treatment. Therefore, these tests can be used as differential diagnostic tests for CMPA.
Treatment block (Block II)
Supplementation of the lactating mother’s diet with vitamin D and calcium
During the cow’s milk protein elimination diet, the mother may reduce her intake of foods that are high in vitamin D and calcium, such as dairy products.41 As a result, there may be a risk of deficiency of these nutrients if measures are not taken to compensate for this reduction.41 To date, evidence is limited to a single publication by Adams et al., which studied the impact of food allergy elimination diets on maternal health.42 The results indicated that anthropometric and bone density measurements, as well as indices of iron, protein, and lipid metabolism, and trace elements, were comparable and within the normal range between the two groups.42 However, despite supplementation with 1000 mg of calcium, bone turnover increased, as indicated by the C-terminal propeptide of type I collagen (ICTP), N-terminal propeptide of type III collagen, and osteocalcin. These markers were significantly higher in lactating mothers with dietary restrictions compared to those without dietary restrictions.42 The role of vitamin D and phosphate was not analyzed in this publication. Therefore, unnecessary elimination diets should be avoided as they may be detrimental to the mother.16
Supplementation of vitamin D and calcium in a mother on a cow’s milk protein elimination diet aims to ensure that both nutrients are adequately available to both mother and infant through breast milk. The supplementation recommendation made in this consensus regarding vitamin D and calcium is in line with other guidelines.5,6,43,44 When selecting vitamin D and calcium supplements, it is critical to ensure that they are free of cow’s milk protein. This is because even small amounts of cow’s milk protein can trigger an allergic reaction in the infant.45 Therefore, it is important to read supplement labels carefully and look for supplements that are labeled “cow’s milk protein-free” or “suitable for people with cow’s milk allergy.” When a mother has to follow a cow’s milk protein restriction diet because of her child’s food allergy, it is important to have the guidance and supervision of a dietitian or nutritionist. Although there are no published data reporting the quality of life of breastfeeding mothers on an elimination diet for non-IgE-mediated food allergy, health professionals should be aware of the additional burden and impact on quality of life of following an elimination diet for the mother and patient, and nutritional support for families should be ensured.16 These health professionals are experts at planning balanced diets and can help ensure that the mother receives all necessary nutrients during this period, and provide information about inappropriate foods that may decrease calcium and vitamin D absorption.46,47
Extensively hydrolyzed formulas (EHF)
EHF formulas are composed of extensively hydrolyzed casein and/or cow’s milk whey protein.48 This involves breaking the proteins into smaller fragments, which helps to decrease their ability to trigger an allergic response in people with CMPA.48 Several guidelines, as well as this consensus’s panelists, consider that they should be the first therapeutic option in patients with CMPA, especially in those with mild to moderate involvement.6,9,29,49 Nevertheless, the vast majority of patients with CMPA, approximately 90%, demonstrate tolerance to these formulas, as demonstrated by international guidelines establishing their hypoallergenic nature.50,51 Consequently, a small subset, around 10% of patients, may require alternative formulas for treatment. To date, there have been no clinical trials that directly compare the benefits of EHF formulated with casein and those formulated with whey for treating infants with CMPA. As a result, there is currently a lack of scientific evidence to provide definitive recommendations regarding the preference for one type over the other in this context. This agreement among the consulted experts recognizes the absence of clear scientific evidence regarding the comparison of benefits between casein-formulated and whey-formulated EHF formulas for treating infants with CMPA.
Partially and extensively hydrolyzed rice formulas (HRF)
Another nutritional alternative for pediatric patients with CMPA is the use of partially and extensively hydrolyzed rice formulas (HRF).48 The panelists agreed that these formulas are a first-line option, as they have been shown to be safe, with no nutritional risks and are effective compared to conventional treatment (EHF). Several clinical trials support this claim,52–55 and the DRACMA guidelines have also indicated HRF as an equivalent alternative to EHF.29 The main concern about using these formulations is their arsenic levels, since rice (Oryza sativa) plants accumulate arsenic in greater quantities than similar cereal crops.56 However, the arsenic level present in an average daily intake of HFR (600–800 ml) is 0.16–0.23 μg/kg, amounts 10 times lower than the limit established by the World Health Organization (WHO; 0.10 mg/kg for children aged 0–3 years). Thus, there is no risk of exposure to arsenic when HRF treatment with CMPA is used in children, as agreed by the experts participating in this consensus.
Amino acid–based formulas (AAF)
AAF is another option in the arsenal available for feeding infants with CMPA. Elemental or amino acid-based formulas are the only ones that completely eliminate residual allergenicity and allow growth similar to that of AAF.57 However, due to their high cost, lower palatability, and higher osmolarity, experts do not consider them as the first choice for treating children with CMPA. Experts have agreed on this formulation’s use in several conditions. It is recommended for use as second-line therapy in case EHF/RHF treatment is ineffective and as the first choice in certain cases such as infants at risk of adverse reactions to EHF and severe initial clinical presentation, including anaphylaxis or Heiner’s syndrome, multiple food allergies, severe atopic dermatitis, rectal bleeding with hemodynamic instability, hypoproteinemia, eosinophilic esophagitis, severe anemia, or significant nutritional impairment. This consensus is in line with a recently published expert consensus focusing on this type of formulation.58 Other guidelines and consensuses have also recommended AAF as a second option or as first line, considering various situations.8,29,59,60
Soy formulas
Modern soy formulas can be considered a safe second-choice option for feeding infants who require an alternative and do not accept the bitter taste of hydrolyzed or amino-acid formulas or in cases where the high cost of these formulas is a limiting factor.
These soy formulas are fortified with nutrients such as methionine, iodine, carnitine, taurine, choline, inositol, long-chain polyunsaturated fatty acids (LCPUFAs), and micronutrients to avoid nutritional deficiencies, and meet the recommendations of the American Academy of Pediatrics and the Infant Formula Act for infants. This assertion is based on the fact that soy formula-fed infants exhibit similar growth patterns, bone health, and metabolic, reproductive, endocrine, immune, and neurologic functions as infants fed with milk formula or human milk.61 Emphasizing the need for close medical supervision in all cases is crucial due to the potential risk of developing an allergy to soy protein. While most infants with CMPA generally exhibit tolerance, there is a possibility of reactions to soy protein in up to approximately 14% of cases,62 with a higher likelihood among infants younger than 6 months.63
Finally, experts have agreed that industrial soy beverages are not adequate for meeting infants’ nutritional needs and therefore should not be used for managing CMPA, or in children under 2 years of age.
Partially hydrolyzed formula (PHF)
With regard to PHF formulas, the experts agreed not to recommend their use for pediatric patients with CMPA. These formulas contain substantially higher amounts of residual allergens than EHF, so there is a greater likelihood of allergic reactions than when using other formulas.64,65 The ESPGHAN guidelines also concluded with the following recommendation.6
Prebiotics, probiotics, and synbiotics
Prebiotics and probiotics have an impact on the intestinal microbiota’s composition, both directly and indirectly, and may have the potential to modulate the development of allergic diseases.66 Synbiotics, combining prebiotics and probiotics, aim to achieve a joint and synergistic effect.66 Experts agreed that using these substances cannot be recommended for preventing and/or treating CMPA in children. For the time being, the evidence on their efficacy is limited and future studies may provide more information on whether they can be used clinically.67
Recovery of CMPA tolerance
Once the diagnosis of CMPA has been confirmed, a CMPA elimination diet should be carried out. In this study, it was agreed that this diet’s duration should be at least 6 months or until 9–12 months of age, and that in children with CMPA with severe immediate IgE-mediated reactions, it can be extended from 12 to 18 months. This recommendation is in line with the recommendations in the ESPGHAN guidelines.6 The introduction of baked milk in the diet was also recommended as a possible inducer of CMPA resolution. The results from several clinical studies support this conclusion.68–70
Conclusions
CMPA in children is a highly relevant clinical condition due to its high frequency and significant clinical manifestations that occur during the first months of life. This study’s objective is to present the current perspectives of a diverse group of experts regarding the diagnosis and treatment of CMPA in children under 2 years of age within the Mexican healthcare context. An algorithm for diagnosis and treatment was developed, with a particular focus on minimizing unnecessary tests and promoting breastfeeding whenever possible. When breast milk is not available, the appropriate use of hypoallergenic formulas is recommended. Additionally, recommendations are provided for the treatment’s duration and the gradual reintroduction of cow’s milk protein. These recommendations, endorsed by 20 Mexican pediatricians, may be applied in everyday clinical practice, and contribute to improving the diagnosis and treatment of children under 2 years of age with CMPA, leading to enhanced health outcomes and a more efficient utilization of healthcare resources.
Strengths and limitations
The foremost strength of this study is its pioneering nature, being the inaugural Mexican Consensus on CMPA for children under 2 years of age in Mexico, filling a crucial gap in the literature in this field. Additionally, the study consulted a robust sample of 25 experts using the Delphi consensus method, exceeding the minimum recommended sample size of 12 experts, and was further bolstered by external validation by other experts.71 The broad agreement among experts is evident as a high percentage consensus was achieved on all statements, signifying a strong accord on the central issues surrounding CMPA in this age group within Mexico.
However, some limitations should be considered when interpreting the results of this study. The primary constraint arises from the limited available literature on this topic, especially as many studies do not specify the breastfeeding status of the infants, introducing potential interpretation challenges. Moreover, while our findings provide critical insights for the Mexican healthcare context, they are specifically tailored to the unique intricacies of Mexico and might not be directly applicable to other healthcare environments.
Conflicts of Interest
All authors declare that they have no conflicts of interest.
Acknowledgments
The authors thank to all the participants of the consensus.
REFERENCES
1. Mousan G, Kamat D. Cow’s milk protein allergy. Clin Pediatr (Phila). 2016;55(11):1054–63. 10.1177/0009922816664512
2. Calvani M, Anania C, Cuomo B, D’Auria E, Decimo F, Indirli GC, et al. Non-IgE-or mixed IgE/non-IgE-mediated gastrointestinal food allergies in the first years of life: Old and new tools for diagnosis. Nutrients. 2021;13(1):226. 10.3390/nu13010226
3. Flom JD, Sicherer SH. Epidemiology of cow’s milk allergy. Nutrients. 2019;11(5):1051. 10.3390/nu11051051
4. Giannetti A, Toschi Vespasiani G, Ricci G, Miniaci A, di Palmo E, Pession A. Cow’s milk protein allergy as a model of food allergies. Nutrients. 2021;13(5):1525. 10.3390/nu13051525
5. Vandenplas Y, Koletzko S, Isolauri E, Hill D, Oranje AP, Brueton M, et al. Guidelines for the diagnosis and management of cow’s milk protein allergy in infants. Arch Dis Child. 2007;92(10):902–8. 10.1136/adc.2006.110999
6. Koletzko S, Niggemann B, Arato A, Dias JA, Heuschkel R, Husby S, et al. Diagnostic approach and management of cow’s-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines. J Pediatr Gastroenterol Nutr. 2012;55(2):221–9. 10.1097/MPG.0b013e31825c9482
7. De Greef E, Hauser B, Devreker T, Veereman-Wauters G, Vandenplas Y. Diagnosis and management of cow’s milk protein allergy in infants. World J Pediatr. 2012;8(1):19–24. 10.1007/s12519-012-0332-x
8. Fiocchi A, Brozek J, Schünemann H, Bahna SL, von Berg A, Beyer K, et al. World Allergy Organization (WAO) Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA) guidelines. Pediatr Allergy Immunol. 2010;21 Suppl 2:1–125. 10.1111/j.1399-3038.2010.01068.x
9. Montijo-Barrios E, López-Ugalde MV, Ramírez-Mayans J, Anaya-Flórez MS, Arredondo-García JL, Azevedo-Tenorio I, et al. [Guía latinoamericana para el diagnóstico y tratamiento de alergia a las proteínas de la leche de vaca (GL-APLV)]. Rev Investig Clin organo del Hosp Enfermedades la Nutr. 2014;66 Suppl 2:S9–72.
10. Dantés OG, Sesma S, Becerril VM, Knaul FM, Arreola H, Frenk J. Sistema de salud de México. Salud Publica Mex. 2011;53(Suppl 2):s220–32.
11. Salvatore S, Agosti M, Baldassarre ME, D’Auria E, Pensabene L, Nosetti L, et al. Cow’s milk allergy or gastroesophageal reflux disease—Can we solve the dilemma in infants? Nutrients. 2021;13(2):297. 10.3390/nu13020297
12. Niederberger M, Spranger J. Delphi technique in health sciences: A map. Front Public Healh. 2020; 8:457. 10.3389/fpubh.2020.00457
13. Rosen R, Vandenplas Y, Singendonk M, Cabana M, DiLorenzo C, Gottrand F, et al. Pediatric gastroesophageal reflux clinical practice guidelines: Joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutriti. J Pediatr Gastroenterol Nutr. 2018;66(3):516–54. 10.1097/MPG.0000000000001889
14. Sung V. Infantile colic. Aust Prescr. 2018;41(4):105–10. 10.18773/austprescr.2018.033
15. Yu M-C, Tsai C-L, Yang Y-J, Yang S-S, Wang L-H, Lee C-T, et al. Allergic colitis in infants related to cow’s milk: Clinical characteristics, pathologic changes, and immunologic findings. Pediatr Neonatol. 2013;54(1):49–55. 10.1016/j.pedneo.2012.11.006
16. Meyer R, Chebar Lozinsky A, Fleischer DM, Vieira MC, Du Toit G, Vandenplas Y, et al. Diagnosis and management of non-IgE gastrointestinal allergies in breastfed infants—An EAACI Position Paper. Allergy. 2020;75(1):14–32. 10.1111/all.13947
17. Rajindrajith S, Devanarayana NM. Constipation in children: Novel insight into epidemiology, pathophysiology and management. J Neurogastroenterol Motil. 2011;17(1):35–47. 10.5056/jnm.2011.17.1.35
18. Connor F, Salvatore S, D’Auria E, Baldassarre ME, Acunzo M, Di Bella G, et al. Cows’ milk allergy–associated constipation: When to look for it? A narrative review. Nutrients. 2022;14(6):1317. 10.3390/nu14061317
19. Kamer B, Dółka E, Pyziak K, Blomberg A. [Food allergy as a cause of constipation in children in the first three years of life—Own observations]. Med Wieku Rozwoj. 2011;15(2):157–61.
20. Kahn A, Mozin MJ, Casimir G, Montauk L, Blum D. Insomnia and cow’s milk allergy in infants. Pediatrics. 1985;76(6):880–4. 10.1542/peds.76.6.880
21. Kahn A, Rebuffat E, Blum D, Casimir G, Duchateau J, Mozin MJ, et al. Difficulty in initiating and maintaining sleep associated with cow’s milk allergy in infants. Sleep. 1987;10(2):116–21. 10.1093/sleep/10.2.116
22. Lendvai-Emmert D, Emmert V, Fusz K, Prémusz V, Tóth G. P319 The unexpected behavioural changes in children with cows milk protein allergy. Arch Dis Child. 2019;104(Suppl 3):A285. 10.1136/archdischild-2019-epa.668
23. El-Shafie AM, Omar ZA, El Zefzaf HMS, Basma EM, Al Sabbagh NM, Bahbah WA. Evaluation of Cow’s Milk Related Symptom Score [CoMiSS] accuracy in cow’s milk allergy diagnosis. Pediatr Res. 2023;94(3):987–95. 10.1038/s41390-023-02539-9
24. Ursino FG, Orsi M, Mehaudy R, Micheletti ME, Parisi C, Petriz N, et al. Cultural adaptation and validation of the Spanish version of the Cow’s Milk-related Symptom Score (CoMiSS) for cow’s milk protein allergy. Rev Gastroenterol México. 2023;88(1):44–9. 10.1016/j.rgmxen.2021.11.016
25. Caffarelli C, Baldi F, Bendandi B, Calzone L, Marani M, Pasquinelli P. Cow’s milk protein allergy in children: A practical guide. Ital J Pediatr. 2010;36:5. 10.1186/1824-7288-36-5
26. Matthai J, Sathiasekharan M, Poddar U, Sibal A, Srivastava A, Waikar Y, et al. Guidelines on diagnosis and management of cow’s milk protein allergy. Indian Pediatr. 2020;57(8):723–9. 10.1007/s13312-020-1916-5
27. Pelkonen AS, Kuitunen M, Dunder T, Reijonen T, Valovirta E, Mäkelä MJ. Allergy in children: Practical recommendations of the Finnish Allergy Programme 2008–2018 for prevention, diagnosis, and treatment. Pediatr Allergy Immunol. 2012;23(2):103–16. 10.1111/j.1399-3038.2012.01298.x
28. Luyt D, Ball H, Makwana N, Green MR, Bravin K, Nasser SM, et al. BSACI guideline for the diagnosis and management of cow’s milk allergy. Clin Exp Allergy. 2014;44(5):642–72. 10.1111/cea.12302
29. Fiocchi A, Bognanni A, Brożek J, Ebisawa M, Schünemann H. World Allergy Organization (WAO) Diagnosis and Rationale for Action against Cow’s Milk Allergy (DRACMA) Guidelines update-I—Plan and definitions. World Allergy Organ J. 2022;15(1):100609. 10.1016/j.waojou.2021.100609
30. Badina L, Burlo F, Belluzzi B, Babich S, Berti I, Barbi E. Life-threatening anaphylaxis in children with cow’s milk allergy during oral immunotherapy and after treatment failure. Immunity Inflamm Dis. 2022;10(4):e607. 10.1002/iid3.607
31. Vandenplas Y, Broekaert I, Domellöf M, Indrio F, Lapillonne A, Pienar C, et al. An ESPGHAN position paper on the diagnosis, management and prevention of cow’s milk allergy. J Pediatr Gastroenterol Nutr. 2023. 10.1097/MPG.0000000000003897
32. de Weger WW, Sprikkelman AB, Herpertz CEM, van der Meulen GN, Vonk JM, Kamps AWA, et al. The dilemma of open or double-blind food challenges in diagnosing food allergy in children: Design of the ALDORADO trial. Pediatr Allergy Immunol. 2022;33(1):e13654. 10.1111/pai.13654
33. Vandenplas Y, Brough HA, Fiocchi A, Miqdady M, Munasir Z, Salvatore S, et al. Current guidelines and future strategies for the management of cow’s milk allergy. J Asthma Allergy. 2021;14:1243–56. 10.2147/JAA.S276992
34. Chin A, Balasubramanyam S, Davis CM. Very elevated IgE, atopy, and severe infection: A genomics-based diagnostic approach to a spectrum of diseases. Case Reports Immunol. 2021;2021:2767012. 10.1155/2021/2767012
35. Ansotegui IJ, Melioli G, Canonica GW, Caraballo L, Villa E, Ebisawa M, et al. IgE allergy diagnostics and other relevant tests in allergy, a World Allergy Organization position paper. World Allergy Organ J. 2020;13(2):100080. 10.1016/j.waojou.2019.100080
36. Xiong L-J, Xie X-L, Li Y, Deng X-Z. Current status of fecal calprotectin as a diagnostic or monitoring biomarker for cow’s milk protein allergy in children: A scoping review. World J Pediatr. 2021;17(1):63–70. 10.1007/s12519-020-00364-2
37. Heine RG, AlRefaee F, Bachina P, De Leon JC, Geng L, Gong S, et al. Lactose intolerance and gastrointestinal cow’s milk allergy in infants and children—Common misconceptions revisited. World Allergy Organ J. 2017;10(1):41. 10.1186/s40413-017-0173-0
38. Nielsen RG, Fenger C, Bindslev-Jensen C, Husby S. Eosinophilia in the upper gastrointestinal tract is not a characteristic feature in cow’s milk sensitive gastro-oesophageal reflux disease. Measurement by two methodologies. J Clin Pathol. 2006;59(1):89–94. 10.1136/jcp.2004.024513
39. Hong SM, Baek DH. A Review of colonoscopy in intestinal diseases. Diagnostics (Basel). 2023;13(7):1262. 10.3390/diagnostics13071262
40. Boese A, Wex C, Croner R, Liehr UB, Wendler JJ, Weigt J, et al. Endoscopic imaging technology today. Diagnostics (Basel). 2022;12(5):1262. 10.3390/diagnostics12051262
41. Al-Beltagi M, Saeed NK, Bediwy AS, Elbeltagi R. Cow’s milk-induced gastrointestinal disorders: From infancy to adulthood. World J Clin Pediatr. 2022;11(6): 437–54. 10.5409/wjcp.v11.i6.437
42. Adams J, Voutilainen H, Ullner PM, Järvinen KM. The safety of maternal elimination diets in breastfeeding mothers with food-allergic infants. Breastfeed Med. 2014;9(10):555–6. 10.1089/bfm.2014.0118
43. Zamanillo-Campos R, Coto Alonso L, Fuentes Martín MJ, Nevot Escusa P, Tejón Fernández M. Nutritional counseling for cow’s milk protein allergy in infants from birth to 2 y of ages: Scoping review. Nutrition. 2022;98:111633. 10.1016/j.nut.2022.111633
44. Bravo P. Actualización en manejo de Alergia a la proteína de leche de vaca: Fórmulas lácteas disponibles y otros brebajes. Rev Chil Pediatría. 2019;90(6):690. 10.32641/andespediatr.v90i6.1425
45. Darwin AH, Carroll MP, Galvis Noda SD, Perez Perez SF, Mhaskar RS, Spoto-Cannons AC, et al. Calcium and vitamin D intake in allergic versus non-allergic children and corresponding parental attitudes towards dairy products. World Allergy Organ J. 2021;14(9):100579. 10.1016/j.waojou.2021.100579
46. Kovacs CS. Maternal mineral and bone metabolism during pregnancy, lactation, and post-weaning recovery. Physiol Rev. 2016;96(2):449–547. 10.1152/physrev.00027.2015
47. Ramasamy I. Vitamin D metabolism and guidelines for vitamin D supplementation. Clin Biochem Rev. 2020;41(3):103–26. 10.33176/AACB-20-00006
48. Maryniak NZ, Sancho AI, Hansen EB, Bøgh KL. Alternatives to cow’s milk-based infant formulas in the prevention and management of cow’s milk allergy. Foods. 2022;11(7):926. 10.3390/foods11070926
49. Kansu A, Yüce A, Dalgıç B, Şekerel BE, Çullu-Çokuğraş F, Çokuğraş H. Consensus statement on diagnosis, treatment and follow-up of cow’s milk protein allergy among infants and children in Turkey. Turk J Pediatr. 2016;58(1):1–11. 10.24953/turkjped.2016.01.001
50. Høst A, Koletzko B, Dreborg S, Muraro A, Wahn U, Aggett P, et al. Dietary products used in infants for treatment and prevention of food allergy. Joint Statement of the European Society for Paediatric Allergology and Clinical Immunology (ESPACI) Committee on Hypoallergenic Formulas and the European Society for Paediatri. Arch Dis Child. 1999;81(1): 80–4. 10.1136/adc.81.1.80
51. Niggemann B, von Berg A, Bollrath C, Berdel D, Schauer U, Rieger C, et al. Safety and efficacy of a new extensively hydrolyzed formula for infants with cow’s milk protein allergy. Pediatr Allergy Immunol. 2008;19(4):348–54. 10.1111/j.1399-3038.2007.00653.x
52. Fiocchi A, Restani P, Bernardini R, Lucarelli S, Lombardi G, Magazzù G, et al. A hydrolysed rice-based formula is tolerated by children with cow’s milk allergy: A multi-centre study. Clin Exp Allergy. 2006;36(3):311–6. 10.1111/j.1365-2222.2006.02428.x
53. Reche M, Pascual C, Fiandor A, Polanco I, Rivero-Urgell M, Chifre R, et al. The effect of a partially hydrolysed formula based on rice protein in the treatment of infants with cow’s milk protein allergy. Pediatr Allergy Immunol. 2010;21(4 Pt 1):577–85. 10.1111/j.1399-3038.2010.00991.x
54. Vandenplas Y, De Greef E, Hauser B. Safety and tolerance of a new extensively hydrolyzed rice protein-based formula in the management of infants with cow’s milk protein allergy. Eur J Pediatr. 2014;173(9):1209–16. 10.1007/s00431-014-2308-4
55. Vandenplas Y, De Greef E, Hauser B, Group PS. An extensively hydrolysed rice protein-based formula in the management of infants with cow’s milk protein allergy: Preliminary results after 1 month. Arch Dis Child. 2014;99(10):933–6. 10.1136/archdischild-2013-304727
56. Hite AH. Arsenic and rice: A call for regulation. Nutrition. 2013;29(1):353. 10.1016/j.nut.2012.10.001
57. Kipfer S, Goldman RD. Formula choices in infants with cow’s milk allergy. Can Fam Physician. 2021;67(3):180–2. 10.46747/cfp.6703180
58. Ribes-Koninckx C, Amil-Dias J, Espin B, Molina M, Segarra O, Diaz-Martin JJ. The use of amino acid formulas in pediatric patients with allergy to cow’s milk proteins: Recommendations from a group of experts. Front Pediatr. 2023;11:1110380. 10.3389/fped.2023.1110380
59. Toca MC, Morais MB, Vázquez-Frias R, Becker-Cuevas DJ, Boggio-Marzet CG, Delgado-Carbajal L, et al. Consenso sobre el diagnóstico y el tratamiento de la alergia a las proteínas de la leche de vaca de la Sociedad Latinoamericana de Gastroenterología, Hepatología y Nutrición. Rev Gastroenterol México. 2022;87(2):235–50. 10.1016/j.rgmx.2022.03.007
60. Alonso-Lebrero E, Bento L, Martorell-Aragonés A, Ribeiro L. Iberian consensus on cow’s milk allergy: The CIBAL Study. Allergol Immunopathol (Madr). 2018;46(6):517–32. 10.1016/j.aller.2017.10.003
61. Westmark CJ. Soy-based therapeutic baby formulas: Testable hypotheses regarding the pros and cons. Front Nutr. 2016;3:59. 10.3389/fnut.2016.00059
62. Verduci E, Di Profio E, Cerrato L, Nuzzi G, Riva L, Vizzari G, et al. Use of soy-based formulas and cow’s milk allergy: Lights and shadows. Front Pediatr. 2020;8:591988. 10.3389/fped.2020.591988
63. Klemola T, Vanto T, Juntunen-Backman K, Kalimo K, Korpela R, Varjonen E. Allergy to soy formula and to extensively hydrolyzed whey formula in infants with cow’s milk allergy: A prospective, randomized study with a follow-up to the age of 2 years. J Pediatr. 2002;140(2):219–24. 10.1067/mpd.2002.121935
64. Vanderhoof JA, Murray ND, Kaufman SS, Mack DR, Antonson DL, Corkins MR, et al. Intolerance to protein hydrolysate infant formulas: An underrecognized cause of gastrointestinal symptoms in infants. J Pediatr. 1997;131(5):741–4. 10.1016/S0022-3476(97)70103-3
65. Ragno V, Giampietro PG, Bruno G, Businco L. Allergenicity of milk protein hydrolysate formulae in children with cow’s milk allergy. Eur J Pediatr. 1993;152(9):760–2. 10.1007/BF01953996
66. Markowiak P, Śliżewska K. Effects of probiotics, prebiotics, and synbiotics on human health. Nutrients. 2017;9(9):1021. 10.3390/nu9091021
67. Fox A, Bird JA, Fiocchi A, Knol J, Meyer R, Salminen S, et al. The potential for pre-, pro-and synbiotics in the management of infants at risk of cow’s milk allergy or with cow’s milk allergy: An exploration of the rationale, available evidence and remaining questions. World Allergy Organ J. 2019;12(5):100034. 10.1016/j.waojou.2019.100034
68. Kim JS, Nowak-Węgrzyn A, Sicherer SH, Noone S, Moshier EL, Sampson HA. Dietary baked milk accelerates the resolution of cow’s milk allergy in children. J Allergy Clin Immunol. 2011;128(1):125–131.e2. 10.1016/j.jaci.2011.04.036
69. Dantzer J, Dunlop J, Psoter KJ, Keet C, Wood R. Efficacy and safety of baked milk oral immunotherapy in children with severe milk allergy: A randomized, double-blind, placebo-controlled phase 2 trial. J Allergy Clin Immunol. 2022;149(4):1383–1391.e17. 10.1016/j.jaci.2021.10.023
70. Nowak-Węgrzyn A, Sampson HA. Future therapies for food allergies. J Allergy Clin Immunol. 2011;127(3):555–8. 10.1016/j.jaci.2010.12.1098
71. Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CF, Askham J, et al. Consensus development methods, and their use in clinical guideline development. Health Technol Assess. 1998;2(3):i–iv, 1–88. 10.3310/hta2030
Supplementary
Table S1 Panel of experts.
| Name | Affiliation |
|---|---|
| Rubén Peña Vélez | Pediatric Gastroenterologist, Hospital General de Puebla Dr. Eduardo Vázquez N. |
| Gerardo Sagols Méndez | Pediatric Gastroenterologist, Clínica de Mérida SA de CV |
| Ana Elena Limón Rojas | Pediatrician, Secretaría Clínica Facultad de Medicina, UNAM, Mexico City |
| Manuel Enrique Galaz Pantoja Méndez | Pediatric Gastroenterologist, Hospital General Chiapas |
| José Antonio Ortega Martell | Pediatric allergist and immunologist, Clínica de Alergia Pediátrica, Pachuca, Hidalgo. Mexico |
| Rosa Elena Huerta Hernández | Pediatric allergist and immunologist, Clínica de Alergia Pediátrica, Pachuca, Hidalgo. Mexico |
| María del Mar Sáez de Ocariz Gutiérrez | Pediatric Dermatologist, Instituto Nacional de Pediatría |
| Héctor Macías Avilés | Pediatric Neonatologist, Instituto Nacional de Pediatría, Mexico City |
| José Reynes Manzur | Pediatrician, Internal Medicine, Instituto Nacional de Pediatría, Mexico City |
| Ana Gabriela Ayala Germán | Pediatric Gastroenterologist, Hospital General Agustín O Haran, Mérida, Yucatán |
| Lucía Casas Guzik | Pediatric Gastroenterologist, Hospital Infantil de Morelia Eva Sámano de López Mateos |
| Martha E. Urquidi Rivera | Pediatric Gastroenterologist, Centro Médico del Niño de la Ciudad de Monterrey, Nuevo León |
| Carlos Méndez Nieto | Pediatric Gastroenterologist, Hospital Infantil de Especialidades, Cd. Juárez |
| Laura E. Flores Fong | Pediatric Gastroenterologist, Hospital Civil de Guadalajara |
| Carlos Iván Oyervides García | Pediatric Gastroenterologist, Hospital del Niño Dr. Federico Gómez Santos, Saltillo, Coahuila |
| Sergio Díaz Madero | Pediatric Gastroenterologist, Hospital Español, Mexico City |
| Liliana Worona Dibner | Pediatric Gastroenterologist, Hospital Infantil de Mexico Federico Gómez, Mexico City |
| José Antonio Chávez Barrera | Pediatric Gastroenterologist, Hospital General del Centro Médico Nacional La Raza, IMSS, Mexico City |
| Dante V. Bacarreza Nogales | Pediatric Gastroenterologist, Hospital General Zona 1 IMSS, Tijuana |
| Judith I. Gris Calvo | Pediatric Nutritionist, Instituto Nacional de Pediatría, Mexico City |
| Guillermo Hideo Wakida Kusunoki* | Pediatric allergist and immunologist, Hospital Central Sur de Alta Especialidad de Petróleos Mexicanos |
| Yvan Vandenplas** | Pediatric Gastroenterologist, the KidZ Health Castle, UZ Brussel, Vrije Universiteit Brussel, Brussels, Belgium |
*National observer; ** International observer.