
Download
ORIGINAL ARTICLE
PSTPIP2 is associated with disease severity in patients with pressure ulcer sepsis and has anti-inflammatory effects
Xiaoxia Wanga, Youli Wangb*, Jianjun Luoa, Lipeng Wanga, Liye Guoa, Xinxin Zhua
aDepartment of Critical Care Medicine, The 903rd Hospital of the Joint Logistics Support Force of the Chinese People’s Liberation Army, Hangzhou, Zhejiang Province, China
bDepartment of Dermatology, Zhuji Traditional Chinese Medicine Hospital, Shaoxing, Zhejiang Province, China
Abstract
Background: One of the common adverse reactions in patients with pressure ulcers (PU) is sepsis, which is mainly related to microbial infections caused by pathogenic organisms. The activation of nuclear factor kappa-B (NF-κB) frequently occurs in conjunction with pathogenic microbial infections. Proline-serine-threonine-phosphatase-interacting protein 2 (PSTPIP2) is closely related to inflammatory disorders. The role and mechanism of PSTPIP2 in sepsis because of pressure ulcers is unclear. In this study, we discovered that PSTPIP2 was lowly expressed in peripheral blood of patients with sepsis induced by pressure ulcers.
Methods: Peripheral blood was collected from 20 patients with sepsis due to pressure ulcers and 10 healthy controls, and the expression of PSTPIP2 in peripheral blood was discovered by polymerase chain reaction and Western blot analysis. Information on the clinical characteristics of patients was summarized, and the expression data of PSTPIP2 were correlated with the patients’ acute physiology and chronic health evaluation (APACHE) II score, sequential organ failure assessment (SOFA) score, and C-reactive protein (CRP) and procalcitonin (PCT) scores by Spearman’s correlation analysis. One of the main mediators of Gram-negative sepsis is lipopolysaccharide (LPS). In order to establish an in vitro sepsis model, THP-1 cells were treated with LPS, and the cells were transfected with PSTPIP2. Contents of interleukin 6 (IL-6), interleukin 1β (IL-1β), and tumor necrosis factor-α (TNF-α) in each group of cells were detected by enzyme-linked--immunosorbent serologic assay, and NF-κB-related proteins were detected by Western blot analysis.
Results: When compared to healthy controls, the peripheral blood of patients with pressure sepsis had lower PSTPIP2 expression, which had a negative correlation with the APACHE II, SOFA, CRP, and PCT scores. LPS-induced THP-1 cells expressed less PSTPIP2 than the untreated control cells, and PSTPIP2 transfection decreased IL-6, IL-1β, and TNF-α levels and inhibited the activation of NF-κB pathway.
Conclusion: PSTPIP2 is associated with disease severity in patients with pressure ulcer sepsis and has anti-inflammatory effects.
Key words: correlation, Inflammation, NF-κB, patients with -pressure ulcer sepsis, PSTPIP2
*Corresponding author: Youli Wang, Department of Dermatology, Zhuji Traditional Chinese Medicine Hospital, No. 521, East Second Road, Zhuji City, Zhejiang Province 311800, China. Email address: [email protected]
Received 13 June 2023; Accepted 4 July 2023; Available online 1 September 2023
Copyright: Wang X, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Pressure ulcers (PU) are a form of skin damage primarily caused by prolonged pressure on the skin and subcutaneous tissues. Pressure ulcers are a common complication in patients with loss of motor function, such as those who have suffered spinal cord or brain injuries and are unable to move on their own. This prolonged immobility causes blood flow to become stagnated, which in turn causes pressure ulcers. Sepsis is the most prevalent complication linked with pressure sores because the process is accompanied by pathogenic microbial infections.1–4
Sepsis is a life-threatening organ dysfunction syndrome, and despite advances in intensive care medicine, mortality rate remains high due to complex pathophysiology of sepsis. Therefore, it is crucial to find sepsis-related specific targets at the molecular level.5
The most important finding for pathogenesis of sepsis is inflammatory imbalance, which persists throughout the course of the disease. Pathogens that cause reactions include bacterial, fungal, parasitic, and viral species. The phagocytosis of the pathogen by macrophages during the initial acute host response to an invading pathogen typically results in the generation of a variety of pro--inflammatory cytokines, which triggers a cytokine storm and activates the innate immune system.6 Initiating a series of activations in immune cells by damage-associated molecular patterns (DAMP) or pathogen-associated molecular patterns (PAMP), pattern recognition receptors (PRRs) appear to be a key player in the activation of the innate immune system. As a result, they increase the expression of genes related to inflammation.7,8
Proline-serine-threonine-phosphatase-interacting protein 2 (PSTPIP2) is a member of Pombe Cdc15 homology (PCH) family of proteins, and is located on chromosome 18. PSTPIP2 has been implicated in immunological and auto--inflammatory diseases. It is expressed not only in several tissues and organs, such as the heart, liver and lungs but also expressed in monocytes, mast cells, lymphocytes, granulocytes.9 It has been demonstrated that PSTPIP2 plays a significant role in inflammatory disorders. PSTPIP2 suppresses osteoarthritis in rats by lowering cartilage degradation and synovial inflammation.10 In mice, PSTPIP2 inhibits inflammation and ameliorates liver fibrosis.11 PSTPIP2 is closely associated with nuclear factor kappa-B (NF-κB) signaling pathway and suppresses synovial fibroblast growth and inflammation.12
Activation of NF-κB signaling pathway is closely associated with pathogenic microbial infections,13 and studies have shown that NF-κB activity was significantly higher in patients who died of sepsis than in surviving patients.14 Inhibition of the NF-κB signaling pathway was able to improve mortality in septic animals.15
Analyzing PSTPIP2 and the mechanisms at play in sepsis are critical, because the involvement of PSTPIP2 in sepsis has not yet been reported. To study the role of PSTPIP2 in sepsis, we first checked its expression level. We found that PSTPIP2 was lowly expressed in the peripheral blood of septic patients and had a negative correlation with patients’ acute physiology and chronic health evaluation II (APACHE II), sequential organ failure assessment (SOFA), C-reactive protein (CRP), and procalcitonin (PCT) scores. According to in vitro tests, PSTPIP2 had a low level of expression in lipopolysaccharide (LPS)-induced cells, and its overexpression suppressed the NF-κB signaling pathway and inflammatory factors. Therefore, PSTPIP2 has the potential to be explored as a therapeutic target for sepsis.
Materials and methods
Patients
In all, 20 patients with pressure ulcer sepsis were enrolled for the study from the 903rd Hospital of the Joint Logistics Support Force of the Chinese People’s Liberation Army. According to international guidelines for the diagnosis of sepsis, patients diagnosed with pressure ulcer sepsis and aged more than 18 years were included in the study. Patients who had a malignant tumor or an autoimmune deficiency disease, or had recently undergone treatment with immunosuppressive drugs, and pregnant and nursing females were excluded. In addition, 10 healthy controls of comparable age from a hospital medical examination center with normal manifestations were also included in the study. Ethical approval was obtained from the Medical Research Ethics Committee of the 903rd Hospital of the Joint Logistics Support Force of the Chinese People’s Liberation Army (Approval No. 202206240601001). The study was conducted according to the Declaration of Helsinki. All participants provided their informed consent, and written informed permission was obtained from legally authorized representative(s) for anonymized patient information to be published in this article.
Data collection
Blood samples were collected from septic patients and healthy controls within 24 h of admission. Septic patients were evaluated for SOFA and APACHE II scores, with higher scores denoting more severe disease. Clinical characteristics, including age, gender, plasma CRP, and PCT, were observed.
Acquisition of peripheral blood mononuclear cells
Peripheral venous blood samples were collected in heparinized tubes, and peripheral blood mononuclear cells (PBMC) were isolated by density gradient centrifugation as follows: the blood sample was mixed with balanced salt solution (BSS) in equal volumes at a ratio of 1:1, spread on Ficoll–Paque solution (Cedarlane, Burlington, NC, USA) and centrifuged at 400× g for 30 min at 20°C. The PBMC layer obtained was transferred in a centrifuge tube The PBMC was obtained by washing with BSS, centrifuging again, and removing the supernatant.
THP-1 cell culture and transfection
THP-1 cells were acquired from ATCC (Manassas, VA, USA) and kept in Roswell Park Memorial Institute (RPMI) 1640 medium (Thermo Fisher Scientific, MA, USA) supplemented with 10-µ/mL penicillin-streptomycin, 2-mM L-glutamine, and 10% fetal bovine serum (FBS) at 37°C and 5% CO2. For the experiments, cells in the logarithmic growth phase were utilized. THP-1 cells were treated with 1-µg/mL LPS for 24 h.16 Following LPS treatment. A PSTPIP2 overexpression plasmid/vector was transfected into THP-1 cells using lipofectamine 3000 (Invitrogen, CA, USA).
Enzyme-linked-immunosorbent serologic assay (ELISA) assay
ELISA assay was applied according to the manufacturer’s instructions for IL-6 (Abcam, Cambridge, UK), IL-1β (Abcam), and TNF-α (Abcam). The cell culture medium was centrifuged at 2000× g for 10 min to remove debris, and the supernatant was collected. Supernatant or standard, 50 µL, was added to 96-well plates, and 50-µL corresponding antibody was added to each well. The plates were sealed, and the plate shaker was set to 400 rpm at room temperature. After each well was washed and dried, 100-µL tetramethylbenzidine (TMB) developer was added, incubated for 10 min, and 100-µL stop solution was added to each well and optical density (OD) was recorded at 450 nm.
Quantitative real-time polymerase chain reaction (qRT-PCR)
Following the manufacturer’s instructions, PrimeScriptTM RT kit (Takara, Shiga, Japan) was used to complete reverse transcription process after total RNA was isolated from PBMC using TRIzol reagent (Invitrogen). qRT-PCR was accomplished using SYBR Green™ Premix Ex Taq™ (Takara) on LightCycler 480 II (Roche, South San Francisco, USA). Primer sequences (Sangon Biotech, Shanghai, China) were as follows: PSTPIP2: 5'-TAAGGTCCGAGAAGAGTGGCAGAG-3', (forward) and 5'-GATGGGTGCTGGTGGAATCTGTC-3' (reverse); β-actin: 5'-TGGCACCCAGCACAATGAA-3' (forward) and 5’'-CTAAGTCATAGTCCGCCTAGAAGCA-3' (reverse). Quantifi-cation was performed by the 2−ΔΔCt method.
Western blot analysis
Proteins in PBMCs were extracted with radioimmunoprecipitation assay (RIPA) lysis buffer (Beyotime Biotechnology, China), and quantified with Bicinchoninic acid assay (BCA) kit (Abcam). Proteins were separated using 10% sodium dodecyl sulfate–polyacrylamide gel electrophoresis (SDS-PAGE) and transferred to polyvinylidene fluoride (PVDF) membranes, which were placed in 5% skimmed milk powder for 2 h, washed thrice with tris buffered saline with tween (TBST) and incubated overnight at 4°C in primary antibodies (Abcam).17 Antibody dilution ratios were as follows: PSTPIP2 (ab155543, 1:2000), p65 (ab32536, 1:1000), p-p65 (ab76302, 1:1000), inhibitor of nuclear factor -kappa-B kinase subunit beta (IκBα; ab32518, 1:5000), p-IκBα (ab133462, 1:1000), and β-actin (ab8227, 1:5000). After incubation, PVDF membranes were washed thrice with TBST and incubated with horseradish peroxidase (HRP)-labeled secondary antibody (ab6721, 1:10,000) for 2 h. Final development was performed by enhanced chemiluminescence (ECL) kit (Thermo Scientific).
Statistical analysis
Statistical analysis was performed using SPSS 22.0. Continuous values with normal distribution were expressed as mean ± standard Deviation (SD) and analyzed by Student’s t-test or analysis of variance (ANOVA) followed by Dunn’s post hoc test for multiple groups. Differences were considered statistically significant at P < 0.05.
Results
Low expression of PSTPIP2 in patients with pressure ulcer sepsis
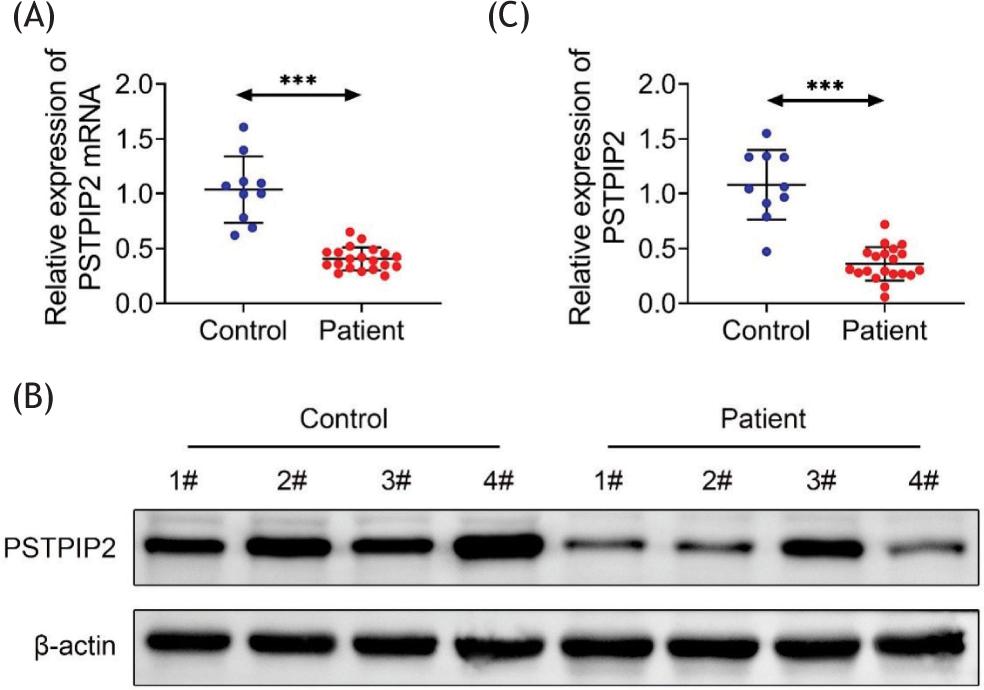
In all, 30 participants were enrolled in this study, including 20 patients with pressure ulcer sepsis and 10 healthy controls, whose clinical information is shown in Table 1 for comparison. We examined PSTPIP2 expression in PBMC of pressure ulcer sepsis patients and healthy controls by PCR and Western blot assays to investigate its potential relevance as a biomarker in patients with pressure ulcer sepsis. The findings demonstrated that PBMC in pressure ulcer sepsis patients had lower levels of PSTPIP2 messenger RNA (mRNA; Figure 1A) and protein (Figures 1B and 1C) expressions than healthy controls.
Table 1 Clinical characteristic of participants.
| Parameter | Control (N = 10) | Patients (N = 20) | P value |
|---|---|---|---|
| Age (years) | 65 ± 5.64 | 69.35 ± 10.01 | 0.2144 |
| Gender Male Female |
6 4 |
11 9 |
0.794 |
| APACHE II score | 20.55 ± 6.95 | ||
| SOFA score | 7.15 ± 2.66 | ||
| CRP (mg/L) | 5.09 ± 1.90 | 104.49 ± 16.44 | <0.001*** |
| PCT (ng/mL) | 0.04 ± 0.02 | 16.01 ± 0.32 | <0.001*** |
SOFA: sequential organ failure assessment; CRP: C-reactive protein; PCT: procalcitonin; APACHE II: acute physiology and chronic health evaluation; N: number; Y: year.
Data are presented as mean ± standard error of mean (SEM).
*P < 0.05, **P < 0.01, ***P < 0.001
Figure 1 Low expression of PSTPIP2 in patients with pressure ulcer sepsis. (A) PSTPIP2 mRNA expression in peripheral blood mononuclear cells from healthy controls and patients with pressure sepsis. (B) PSTPIP2 protein expression in peripheral blood mononuclear cells from healthy controls and patients with pressure sepsis. (C) Relative quantification of PSTPIP2 protein expression. ***P < 0.001.
PSTPIP2 levels correlate with disease severity and sepsis biomarkers
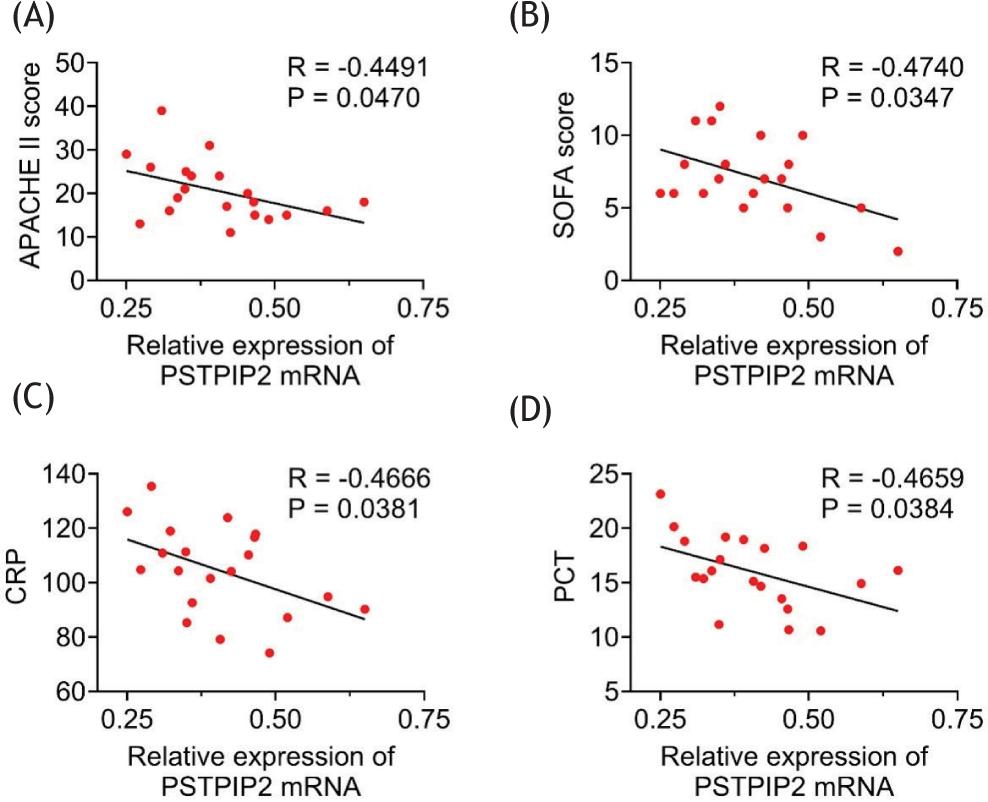
Spearman’s correlation analysis was carried out between PSTPIP2 mRNA expression data and APACHE II, SOFA, CRP, and PCT scores in sepsis patients to elaborate the clinical significance of PSTPIP2 expression in sepsis. The findings revealed a negative correlation between PSTPIP2 and the APACHE II (Figure 2A) and SOFA scores (Figure 2B), which measure the severity of sepsis. The sepsis biomarkers PCT (Figure 2C) and CRP (Figure 2D) were also negatively correlated with PSTPIP2.
Figure 2 PSTPIP2 levels correlate with disease severity and sepsis biomarkers. (A) Correlation analysis of PSTPIP2 mRNA expression levels with APACHE II scores. (B) Correlation analysis of PSTPIP2 mRNA expression levels with SOFA scores. (C) Correlation analysis of PSTPIP2 mRNA expression levels with CRP. (D) Correlation analysis of PSTPIP2 mRNA expression levels with PCT.
PSTPIP2 inhibits LPS-induced inflammatory responses in vitro
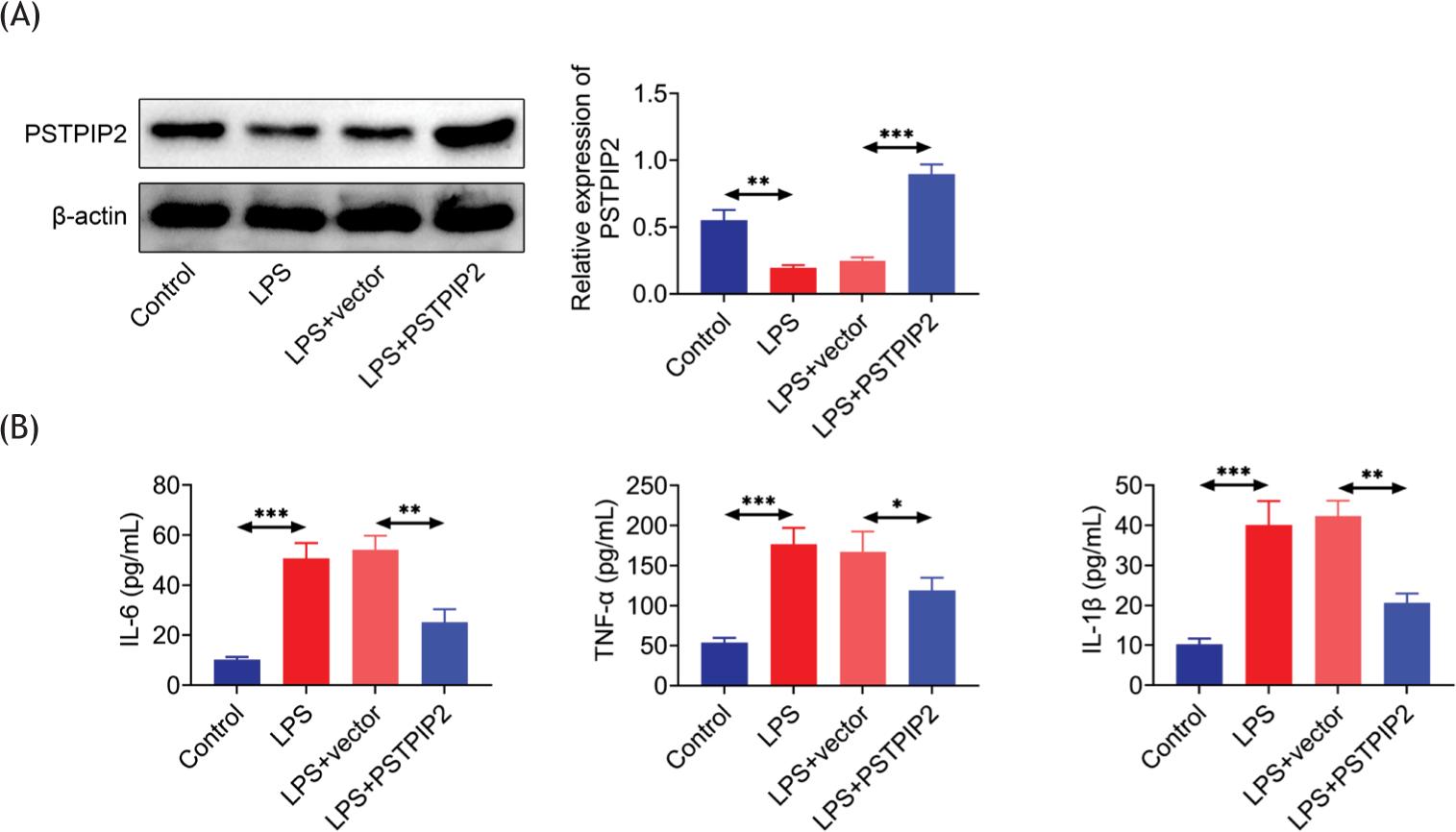
We treated THP-1 cells with LPS to create a sepsis cell model to investigate further the function of PSTPIP2 in sepsis. The findings demonstrated that PSTPIP2 expression was reduced in LPS-induced cells (Figure 3A), and the contents of IL-6, IL-1, and TNF-α were elevated, compared to the control group, and decreased following transfection with PSTPIP2 (Figure 3B). This suggests that PSTPIP2 inhibits the production of inflammatory factors.
Figure 3 PSTPIP2 inhibits LPS-induced inflammatory responses in vitro. (A) Expression of PSTPIP2 in each group of cells. (B) Levels of IL-6, TNF-α, and IL-1β in each group of cells. *P < 0.05, **P < 0.01, ***P < 0.001.
PSTPIP2 inhibits NF-κB signaling pathway
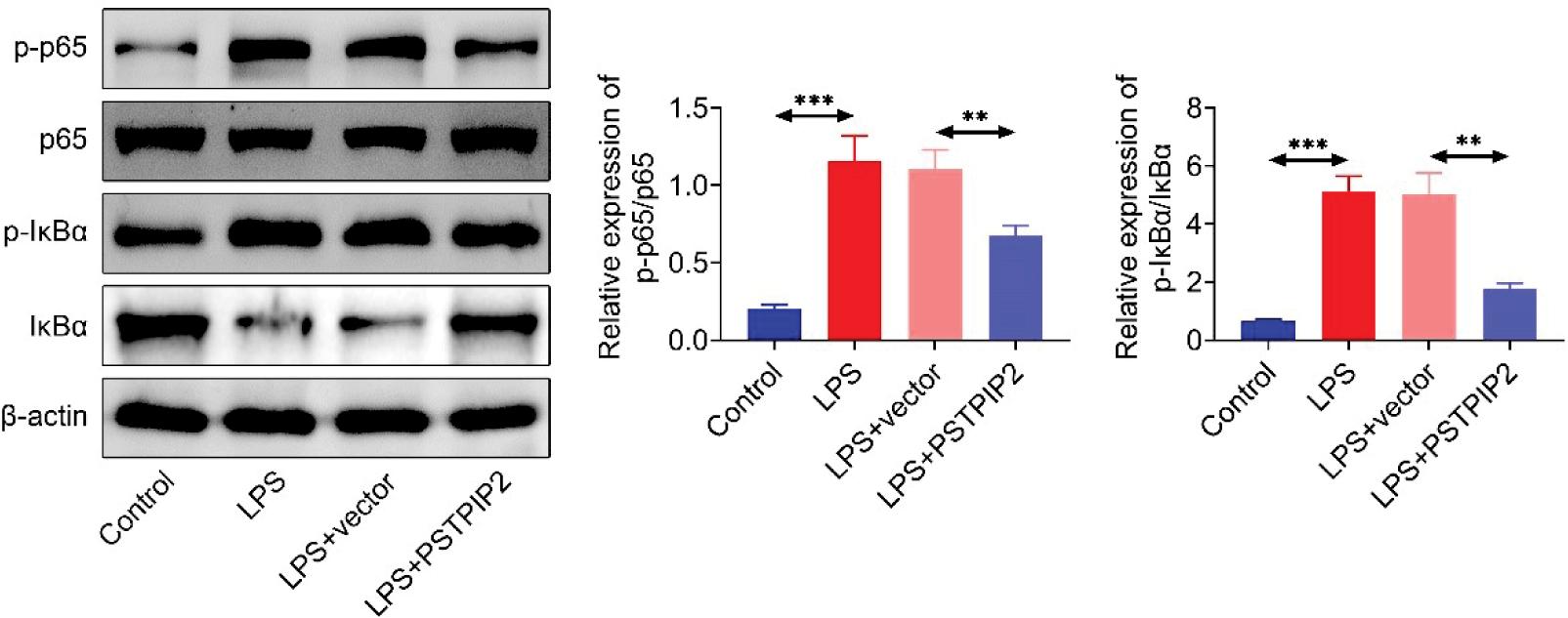
In order to explore the mechanisms associated with the inhibition of inflammation by PSTPIP2, we examined the NF-κB signaling pathway-related proteins. LPS treatment resulted in increased expression of p-p65 and p-IκBα, compared to controls, whereas p-p65 and p-IκBα expressions were decreased after transfection with PSTPIP2 (Figure 4). Thus, these results indicated that regulation of inflammatory factors by PSTPIP2 could be closely related to the NF-κB pathway.
Figure 4 PSTPIP2 inhibits the NF-κB pathway. Expression levels of p65, p-p65, IκBα, and p-IκBα proteins in each group of cells.
Discussion
Patients who are bedridden for extended periods frequently experience pressure ulcers, which could lead to sepsis in severe cases. Patients with sepsis experience various tissue and organ failure, and their prognosis is poor. There is an urgent requirement to search for novel biomarkers to enhance the prognosis of sepsis. It has been demonstrated that PSTPIP2 is involved in the activation of macrophages and neutrophils, and lack of PSTPIP2 in inflammatory diseases.18
In the present study, we investigated the association between pressure ulcer sepsis and PSTPIP2. We discovered that PSTPIP2 the expression of PSTPIP2 was decreased in PBMC cells of the patients with pressure ulcer sepsis and negatively related to APACHE II, SOFA, CRP, and PCT scores. Therefore, it was speculated that PSTPIP2 could have a protective role in pressure ulcer sepsis.
In sepsis, an invasive pathogen triggers an immune response that ultimately results in prolonged hyperinflammation and immunosuppression by failing to return to equilibrium in vivo. Activated macrophages play a crucial part in host defense during sepsis by releasing huge amounts of pro-inflammatory cytokines, such as TNF-α, IL-1β, and IL-6 in response to invasive infections and injured tissues. In addition, excessive pro-inflammatory cytokines lead to multiple organs failure and cardiovascular collapse, which is one of the key factors contributing to sepsis’ high fatality rate.19 In this study, we established an inflammation model with LPS-treated THP-1 cells and determined that PSTPIP2 reduced TNF-α, IL-1β, and IL-6 levels, suggesting that inflammation in sepsis is inhibited by PSTPIP2.
TNF-α, IL-1β, and IL-6 are pro-inflammatory factors that can be controlled through a number of signaling pathways, including the NF-κB pathway. This makes NF-κB an appropriate target for developing novel anti--inflammatory drugs.20 In unstimulated cells, NF-κB protein is present in the cytoplasm and when cells are exposed to LPS, the NF-κB pathway is activated. Upon activation of NF-κB, degradation of IκB phosphorylation leads to phosphorylation of NF-κB p65 subunit and translocation from the cytoplasm to the nucleus to increase transcription of various inflammation-related genes, including TNF-α, IL-6, and other factors.21,22 In order to further understand the anti--inflammatory mechanism of PSTPIP2, we examined how it affected the NF-κB pathway. The results revealed that PSTPIP2 had an inhibitory effect on the NF-κB pathway, as it was able to reduce the production of p-p65 and p-IκBα proteins in LPS-stimulated THP-1 cells.
In conclusion, our findings suggest that PSTPIP2 is associated with sepsis and can control inflammatory factor expression by modifying the NF-κB pathway. However, there are still some limitations to our study. Our sample size was small, and the research direction was not comprehensive enough, but our results can still serve as a reference for the molecular targets of sepsis. The future study would focus on the association between PSTPIP2 and pressure ulcer patient prognosis.
Competing interests
The authors stated that they had no conflict of interest to declare.
Data availability
All data supporting the findings of this study are available in the paper, and any raw data can be obtained from the corresponding author upon request.
Author Contributions
Xiaoxia Wang and Youli Wang designed and carried out the. Xiaoxia Wang, Youli Wang, Jianjun Luo, Lipeng Wang, Liye Guo, and Xinxin Zhu supervised collection, analysis, and interpretation of the data. All the authors were involved in preparing and reviewing the draft of the manuscript for publication. All authors read and approved the final manuscript.
REFERENCES
1. Okamoto S, Ogai K, Mukai K, Sugama J. Association of skin microbiome with the onset and recurrence of pressure injury in bedridden elderly people. Microorganisms. 2021;9(8):1603. 10.3390/microorganisms9081603
2. Kumar S, Theis T, Tschang M, Nagaraj V, Berthiaume F. Reactive oxygen species and pressure ulcer formation after traumatic injury to spinal cord and brain. Antioxidants (Basel, Switzerland). 2021;10(7): 1013. 10.3390/antiox10071013
3. Espejo E, Andrés M, Borrallo RM, Padilla E, Garcia-Restoy E, Bella F. Bacteremia associated with pressure ulcers: A prospective cohort study. Eur J Clin Microbiol Infect Dis. 2018;37(5):969–75. 10.1007/s10096-018-3216-8
4. Schiffman J, Golinko MS, Yan A, Flattau A, Tomic-Canic M, Brem H. Operative debridement of pressure ulcers. World J Surg. 2009;33(7):1396–402. 10.1007/s00268-009-0024-4
5. Kim Y, Lee J, Lee S, Kim W. Use of quick sequential organ failure assessment score-based sepsis clinical decision support system may be helpful to predict sepsis development. Signa Vitae. 2021;17(5):86–94. 10.22514/sv.2021.082
6. D’Elia RV, Harrison K, Oyston PC, Lukaszewski RA, Clark GC. Targeting the “cytokine storm” for therapeutic benefit. Clin Vaccine Immunol (CVI). 2013;20(3):319–27. 10.1128/CVI.00636-12
7. Raymond SL, Holden DC, Mira JC, Stortz JA, Loftus TJ, Mohr AM, et al. Microbial recognition and danger signals in sepsis and trauma. Biochim Biophys Acta Mol Basis Dis. 2017;1863(10, Pt B):2564–73. 10.1016/j.bbadis.2017.01.013
8. Huang M, Cai S, Su J. The pathogenesis of sepsis and potential therapeutic targets. Int J Mol Sci. 2019;20(21): e420-e427. 10.3390/ijms20215376
9. Zhu H, Jiang W, Zhao H, He C, Tang X, Xu S, et al. PSTPIP2 inhibits cisplatin-induced acute kidney injury by suppressing apoptosis of renal tubular epithelial cells. Cell Death Dis. 2020;11(12):1057. 10.1038/s41419-020-03267-2
10. Li M, Xiao YB, Wang XT, Zhuang JP, Zhou CL. Proline-serine-threonine phosphatase-interacting protein 2 alleviates diabetes mellitus-osteoarthritis in rats through attenuating synovial inflammation and cartilage injury. Orthop Surg. 2021;13(4):1398–407. 10.1111/os.13000
11. Yang Y, Wu XQ, Li WX, Huang HM, Li HD, Pan XY, et al. PSTPIP2 connects DNA methylation to macrophage polarization in CCL4-induced mouse model of hepatic fibrosis. Oncogene. 2018;37(47):6119–35. 10.1038/s41388-018-0383-0
12. Yao Y, Yu H, Liu Y, Xu Q, Li X, Meng X, et al. PSTPIP2 inhibits the inflammatory response and proliferation of fibroblast--like synoviocytes in vitro. Front Pharmacol. 2018;9:1432. 10.3389/fphar.2018.01432
13. Cao L, Zhu T, Lang X, Jia S, Yang Y, Zhu C, et al. Inhibiting DNA methylation improves survival in severe sepsis by regulating nf-κb pathway. Front Immunol. 2020;11:1360. 10.3389/fimmu.2020.01360
14. Böhrer H, Qiu F, Zimmermann T, Zhang Y, Jllmer T, Männel D, et al. Role of NF-kappaB in the mortality of sepsis. J Clin Invest. 1997;100(5):972–85. 10.1172/JCI119648
15. Ikezoe T, Yang Y, Heber D, Taguchi H, Koeffler HP. PC-SPES: A potent inhibitor of nuclear factor-kappa B rescues mice from lipopolysaccharide-induced septic shock. Mol Pharmacol. 2003;64(6):1521–9. 10.1124/mol.64.6.1521
16. Ling P, Tang R, Wang H, Deng X, Chen J. miR-1184 Regulates inflammatory responses and cell apoptosis by targeting TRADD in an LPS-induced cell model of sepsis. Exp Ther Med. 2021;21(6):630. 10.3892/etm.2021.10062
17. Lai K, Song C, Gao M, Deng Y, Lu Z, Li N, et al. Uridine-alleviates sepsis-induced acute lung injury by inhibiting ferroptosis of macrophage. Int J Mol Sci. 2023;24(6):5093. 10.3390/ijms24065093
18. Liao HJ, Chyuan IT, Wu CS, Lin SW, Chen KH, Tsai HF, et al. Increased neutrophil infiltration, IL-1 production and a SAPHO syndrome-like phenotype in PSTPIP2-deficient mice. Rheumatology (Oxford, England). 2015;54(7):1317–26. 10.1093/rheumatology/keu481
19. Liu L, Zhang S, Wang Y, Bao W, Zhou Y, Dang W, et al. BIG1 controls macrophage pro-inflammatory responses through ARF3-mediated PI(4,5)P2 synthesis. Cell Death Dis. 2020;11(5):374. 10.1038/s41419-020-2590-1
20. Philip S, Tom G, Balakrishnan Nair P, Sundaram S, Velikkakathu Vasumathy A. Tinospora cordifolia chloroform extract inhibits LPS-induced inflammation via NF-κB inactivation in THP-1 cells and improves survival in sepsis. BMC Complement Med Ther. 2021;21(1):97. 10.1186/s12906-021-03244-y
21. Bisht A, Dickens M, Rutherfurd-Markwick K, Thota R, Mutukumira AN, Singh H. Chlorogenic acid potentiates the anti-inflammatory activity of curcumin in LPS-stimulated THP-1 cells. Nutrients. 2020;12(9): 2706. 10.3390/nu12092706
22. Li Y, Lin B. Icariside II regulates TLR4/NF-κB signaling pathway to improve septic lung injury. Signa Vitae. 2021;17(6): 136–42. 10.22514/sv.2021.216