
Download
ORIGINAL ARTICLE
Clinical outcome and component-specific antibody levels in egg allergic children after lightened oral immunotherapy
Anna Kofferta*, Jussi Liippoa, Eliisa Löyttyniemib, Johannes Savolainenc,d
aDepartment of Dermatology, University of Turku and Turku University Hospital, Turku, Finland
bDepartment of Biostatistics, University of Turku, Turku, Finland
cDepartment of Pulmonary Diseases and Clinical Allergology, University of Turku and Turku University Hospital, Turku, Finland
dDepartment of Pediatrics, Turku University Hospital, Turku, Finland
*Corresponding author: Anna Koffert, Department of Dermatology, Dermatologist and Clinical Allergologist, Turku University Hospital, T-Sairaala, Hämeentie 11, 20520 Turku, Finland. Email address: [email protected]
Abstract
Objective: To evaluate the clinical outcome of lightened version of egg oral immunotherapy (OIT) and to analyze egg allergen component-specific antibody levels during short up-dosing with egg white powder and maintenance by egg in daily diet.
Patients and methods: Eighteen egg-allergic children received egg powder with short up--dosing and they maintained tolerance using egg in daily diet. Seventeen egg-allergic children served as a control group. Component-resolved analysis of serum immunoglobulin E (IgE), IgA1, IgA2, and IgG4 levels were determined at inclusion, after up-dosing and after 1 year of immunotherapy. Skin-prick tests were performed at inclusion and after 1 year of therapy.
Results: All 18 patients in the egg OIT group were successfully desensitized. Desensitization was achieved on average in 4.5 months. In the control group, only two children tolerated egg in oral food challenge after 1 year. Of the measured immune markers, smaller wheal diameters in skin-prick testing, reduction in component-specific IgE levels, and increase in component-specific IgA1, IgA2, and IgG4 levels were associated with desensitization.
Conclusion: A lightened egg OIT is effective and safe in children with egg allergy. Increase in all egg component-specific IgA1, IgA2 and IgG4 levels and decrease in all egg component--specific IgE levels were observed after 12 months of OIT.
Key words: Egg Allergy, Iga, Ige, Igg4, Oral Immunotherapy
Received 2 December 2022; Accepted 7 April 2023; Available online 1 January 2024
Copyright: Koffert A, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Among young children, the prevalence of hen’s egg, cow’s milk, and wheat allergies is 1–4% in Western countries.1 Egg allergy usually develops within the first 2 years and 34% of these children do not tolerate egg by 5 years of age.2 Avoidance diet has traditionally been the main treatment for food allergy, but it has many negative effects on the quality of life (QoL).3 Occasional diet failures contain a significant risk of anaphylaxis,4 while long-lasting and strict avoidance diets may prevent the development of normal tolerance.5,6 Recent guidelines suggest that induction of specific oral tolerance provides a treatment option in children with food allergy if performed in specialized clinical centers.7
Egg oral immunotherapy (OIT) has been an effective treatment in children allergic to egg in several studies.8–12 Most previous egg OIT studies have been conducted using high doses (1–4 g) of dried egg white (EW powder in up--dosing and during the maintenance phase.8,9,11 The aim of this study was to evaluate whether good clinical outcome could be achieved with a lightened version of egg OIT, where a short up-dosing phase is followed by egg as a part of normal daily diet. In addition, we analyzed whether any changes in specific immunoglobulin E (IgE), IgA1, IgA2, and IgG4 responses against egg components could be checked with the lightened OIT protocol.
Methods
Study subjects
The study was approved by the Ethical Committee of the Hospital District of South Western Finland (§63/March 16, 2010). The study recruited 50 children that were on egg-avoidance diet based on their previously diagnosed egg allergy. Eligibility criteria were: (1) age 6–16 years, and (2) elevated serum levels of egg-specific IgE (≥5 kU/l) or a positive skin-prick test to egg (≥5 mm).
Prior to conducting oral food challenge (OFC) with hen’s egg, levels of serum IgE to hen’s egg antigens were quantified and skin-prick tests with egg allergens were carried on.
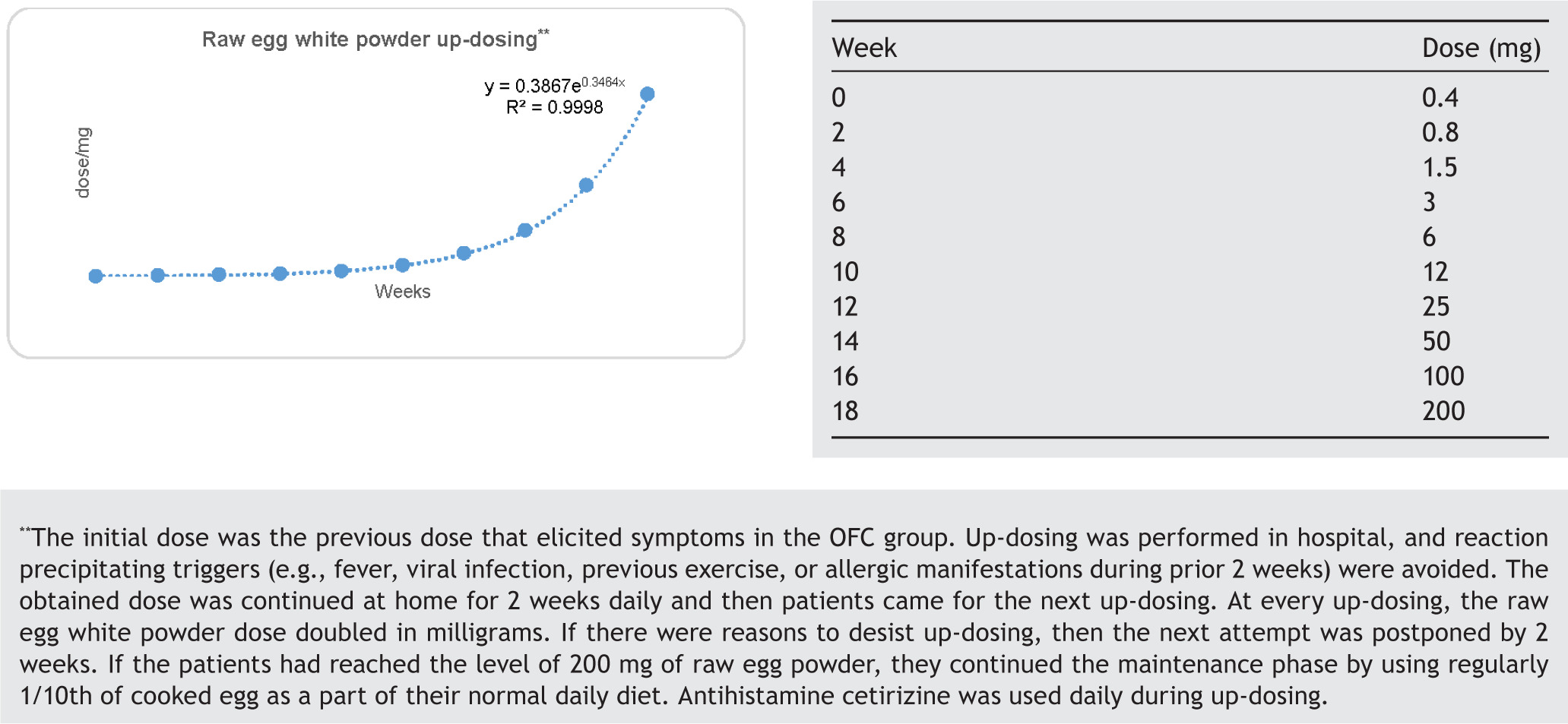
The OFC with hen’s egg started with a dose of 0.8 mg raw egg white powder. Doses were doubled until objective clinical reactivity or 200-mg dose was achieved. Reactivity assessment resembled practical allergy (PRACTALL) guidelines.13
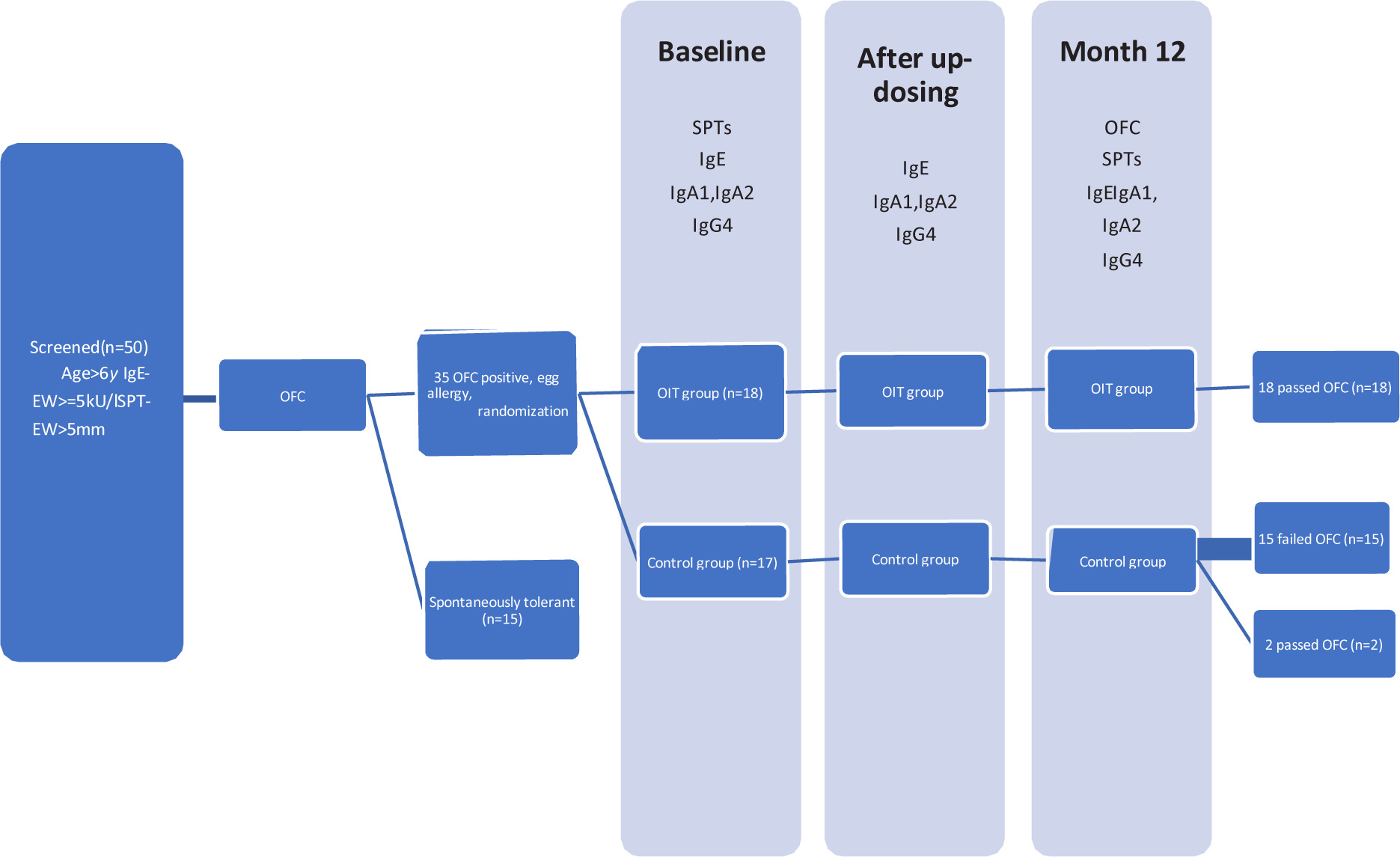
The subjects with a positive OFC were randomized to tolerance induction (OIT) group receiving oral desensitization (n = 18) or to a control group to be followed on an avoidance diet (n = 17). Subjects with negative OFC (n = 15) formed the control group for baseline comparison.
Specific oral immunotherapy
Egg OIT was started with raw egg white powder (containing 80% of protein; Valkuaisjauhe, Scanegg Suomi Oy, Piispanristi, Finland), which was the previous dose that elicited symptoms in OFC; then, the amount was gradually increased until the dose of 200-mg raw egg powder was reached. The maintenance phase was carried out with egg-containing foods as a part of normal daily diet starting with 1/10th of egg. Thereafter, the study subjects were encouraged to increase gradually the amount of daily egg intake. Antihistamine cetirizine was used daily during up-dosing phase.
Skin-prick tests were conducted at inclusion and after 1 year of therapy.
Component-resolved analysis of serum IgE, IgA1, IgA2, and IgG4 levels were determined at inclusion, after up-dosing, and after 1 year of immunotherapy.
Study flow chart and open OFC and raw egg powder up-dosing protocols are presented in Supplementary Figure 1 and Table 1.
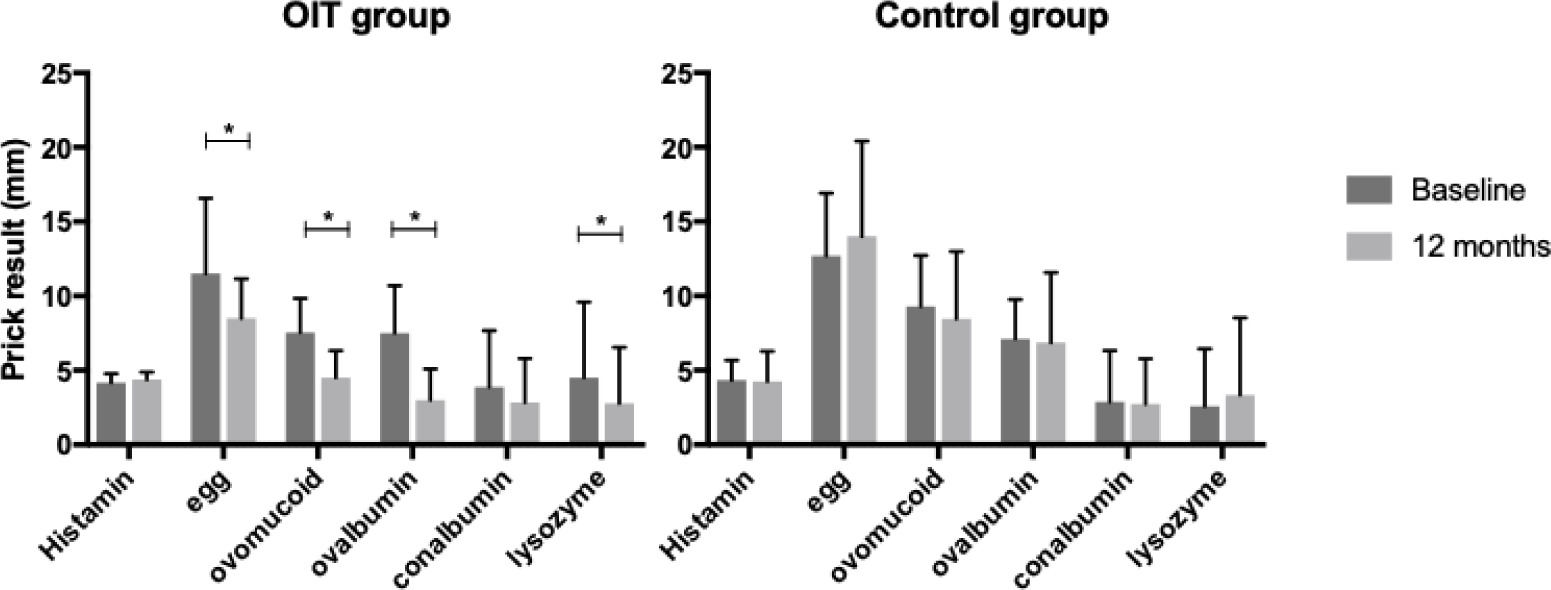
Figure 1 Specific skin-prick test (sSPT) prior to and after OIT. sSPT results with egg white, ovomucoid, ovalbumin, conalbumin, and lysozyme at the commencement of the study (baseline) and after 1 year (12 months) of treatment in the OIT and control groups. Data are expressed as mean (SD). Comparisons performed with linear mixed models for repeated measurements. *P < 0.02.
Table 1 Demographics and clinical information of 50 children screened at baseline.
| OIT group (n = 18) | Control group (n = 17) | P-valuea | Spontaneously tolerant (n = 15) | P-valueb | |
|---|---|---|---|---|---|
| Male | 10 (56%) | 12 (71%) | – | 10 (67) | – |
| Age at inclusion, mean (range), years | 9 (6–15) | 9 (6–14) | – | 10 (6–16) | – |
| Serum IgE, mean (range), kU/L | |||||
| Hen’s egg (egg white [EW]) | 55.1 (2.0–460) | 28.9 (3.4–100) | 0.19 | 14 (0.34–120) | 0.192 |
| Ovomucoid (OVM) | 45.9 (0.64–273) | 13.4 (2.2–45.9) | 0.07 | 6.8 (0.34–16.6) | 0.14 |
| Ovalbumin (OVA) | 46.2 (1–288) | 19.5 (1.1–64.2) | 0.14 | 7.4 (0.34–61.4) | 0.15 |
| Conalbumin (CONA) | 32 (0.34–70.1) | 10.7 (0.34–23.7) | 0.15 | 2.2 (0.34–13.4) | 0.19 |
| Lysozyme (LZM) | 10.1 (0.34–70.1) | 3.6 (0.34–23.7) | 0.12 | 6.3 (0.34–85) | 0.89 |
| Skin-prick test, mean (range), mm | |||||
| Hen’s egg (EW) | 11.5 (5–21) | 12.7 (6–20) | 0.23 | 8.7 (0–14) | 0.008 |
| Ovomucoid (OVM) | 7.6 (4–13) | 9.3 (3–16) | 0.04 | 5.5 (0–14) | 0.005 |
| Ovalbumin (OVA) | 7.5 (3–13) | 7.1 (3–12) | 0.35 | 4.7 (0–8) | 0.003 |
| Conalbumin (CONA) | 3.9 (0–11) | 2.9 (0–10) | 0.21 | 0.8 (0–5) | 0.01 |
| Lysozyme (LZM) | 4.5 (0–16) | 2.6 (0–11) | 0.11 | 1.9 (0–10) | 0.19 |
| OFC dose, mean (range), mg | 6.35 (0.8–25) | 19.4 (1.5–96) | – | 150 (50–200) | – |
| Symptoms in OFC | |||||
| 1 organ system | 12 (67%) | 9 (53%) | – | – | – |
| 2 or more organ systems | 6 (33%) | 8 (47%) | – | – | – |
| Other atopic diseases | |||||
| Asthma | 8 (44%) | 9 (53%) | – | – | – |
| Food allergies | 9 (50%) | 11 (65%) | – | – | – |
| Atopic dermatitis | 7 (39%) | 12 (71%) | – | – | – |
Notes:aP values between OIT and control groups; bP values between egg allergic (OIT + control) and spontaneously tolerant.
Allergen preparations
Egg white and allergen components ovalbumin (OVA, Gal d 2), conalbumin (CONA, Gal d 3), lysozyme (LZM, Gal d 4), and ovomucoid (OVM, Gal d 1) were commercially available (Sigma-Aldrich, St Louis, MO, USA). Allergen components were cleaned with Detoxi-Gel Endotoxin Removal Gel columns (Thermo Scientific Pierce Chemicals) to remove endotoxins.
Skin-prick tests
Skin-prick test extracts were in-home preparations prepared at the MediCity Research Laboratory of the University of Turku from commercial egg components (Sigma-Aldrich). Skin-prick tests were performed with egg white and egg white components according to European standards,14,15 and accredited by the Finnish Allergy Program.16
Egg-specific IgE and IgG4 responses
Egg white and egg white component-specific IgE and IgG4 antibodies were analyzed by ImmunoCap assays using the ImmunoCAP 100 instrument (Thermo Fisher Scientific) according to the manufacturer’s instructions.
Egg-specific IgA1 and IgA2 responses
Nunc MaxiSorp (Thermo Fisher Scientific Invitrogen) flat--bottomed 96-well enzyme-linked immunosorbent serologic assay (ELISA) plates coated with ovalbumin, ovomucoid, conalbumin, and lysozyme were used to measure the egg component--specific IgA1 and IgA2 antibodies. Detailed description of the assay is presented in Supplementary Figure 2.
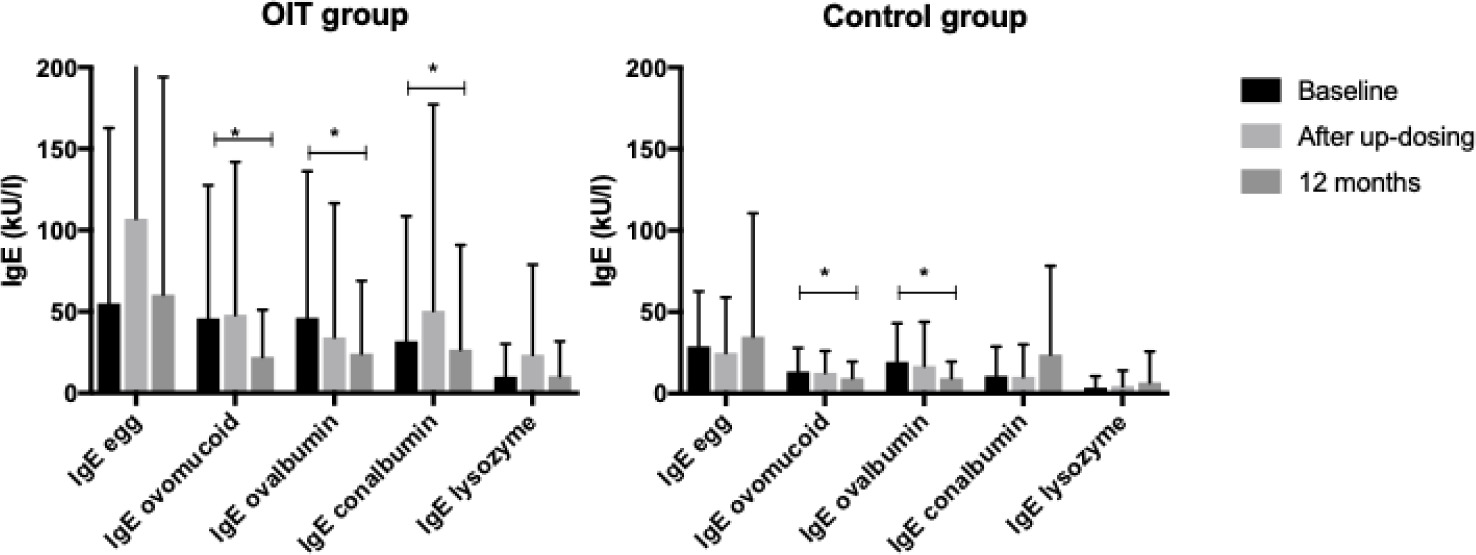
Figure 2 Changes in specific IgE levels during OIT. Changes in specific IgE levels against egg white, ovomucoid, ovalbumin, conalbumin, and lysozyme at the commencement of the study (baseline), and after up-dosing and 1 year (12 months) of treatment. There were no constant differences in component-specific IgE levels over time between OIT and control groups. Data are expressed as mean (SD). Comparisons were performed with linear mixed models for repeated measurements. *P < 0.03
Statistical analysis
The key outcome of interest was immunological comparison between OIT-treated subjects and the control group. Differences between the groups in continuous variables over time were assessed by using linear mixed model for repeated measurements. The model included group, time (within factor), and group by time interaction. If interaction was statistically significant, contrasts were programmed to study whether mean changes differed between 0 and 6 months, 0 and 12 months, or 6 and 12 months. Baseline levels were tested with the same model. Logarithmic transformation was performed to achieve assumption for normality. Confidence intervals of 95% (CI 95%) were calculated and significance level of 0.05 (two-tailed) was used. The data analysis for this study was generated using the SAS software, version 9.4 of the SAS System for Windows (SAS Institute Inc., Cary, NC, USA).
Results
Demographics and clinical outcome
Demographic data of the screened 50 children are presented in Table 1. All 18 patients in the OIT group were successfully desensitized. Desensitization was achieved on average in 4.5 months (1.5–8 months). Adverse events during the up-dosing were abdominal pain and mild diarrhea reported in six patients (33%), oropharyngeal pruritus in four patients (22%), and perioral urticaria in one patient (5.5%). Adverse reactions were treated with oral antihistamines. Seven patients (39%) had no adverse events. At the 1-year follow-up visit, all patients in the OIT group passed the OFC consisting 200-mg (cumulative dose) of egg white powder and subsequently tolerated egg as a part of normal diet. The amount of egg that these patients used daily varied between 1/10th of egg (six patients, 33%), 1/5th–1/4th of egg (six patients, 33%) to the unlimited use of egg (six patients, 33%). There were no reported accidental allergic reactions to egg in the OIT group during the follow-up period. Seven patients (41%) in the control group experienced unintentional allergic reaction to egg during the 1-year follow-up. Only two children in the control group tolerated 200 mg of egg white powder in OFC after 1 year.
Egg white and component specific skin-prick tests (sSPT)
Skin-prick test results are presented in Figure 1. The mean sSPT wheal diameters in the OIT group decreased from baseline to 1-year follow-up visit: EW, OVM, OVA, and LZM (P < 0.02). No changes were observed in sSPT diameters during follow-up in the control group.
Egg white and component-specific IgE antibody levels
Immunoglobulin E results are presented in Figure 2. In the OIT group, a decrease was observed in IgE against OVM, OVA, and CONA (P < 0.003) at 1-year follow-up. In the control group, IgE decreased against OVM and OVA (P < 0.03) but increased against EW (P = 0.05). No significant differences were observed in component-specific IgE levels between the OIT and control groups at any time point.
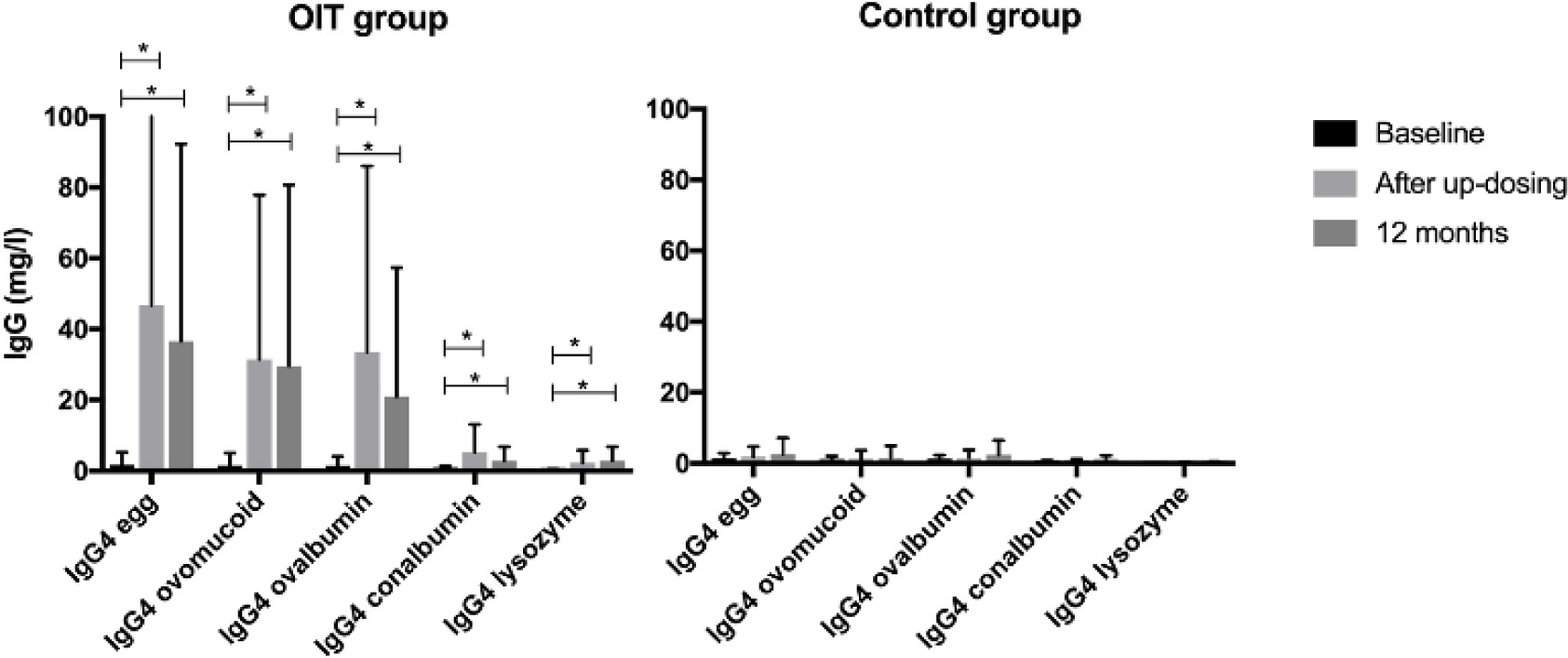
Egg white and component-specific IgG4 levels
IgG4 results are presented in Figure 3. Specific IgG4 antibody levels against egg white and all components increased sharply during up-dosing in the OIT group and demonstrated sustained increase at 1-year follow-up: EW, OVM, OVA, and LZM (P < 0.0001) and CONA (P = 0.03).
Figure 3 Changes in specific IgG4 levels during OIT. Specific IgG4 levels against egg white, ovomucoid, ovalbumin, conalbumin, and lysozyme at the commencement of the study (baseline), and after up-dosing and 1 year (12 months) of treatment (OIT group) or follow-up (control group). Comparisons were performed with linear mixed models for repeated measurements (*IgG4 increase in OIT group, P < 0.0001). Data are expressed as mean (SD)
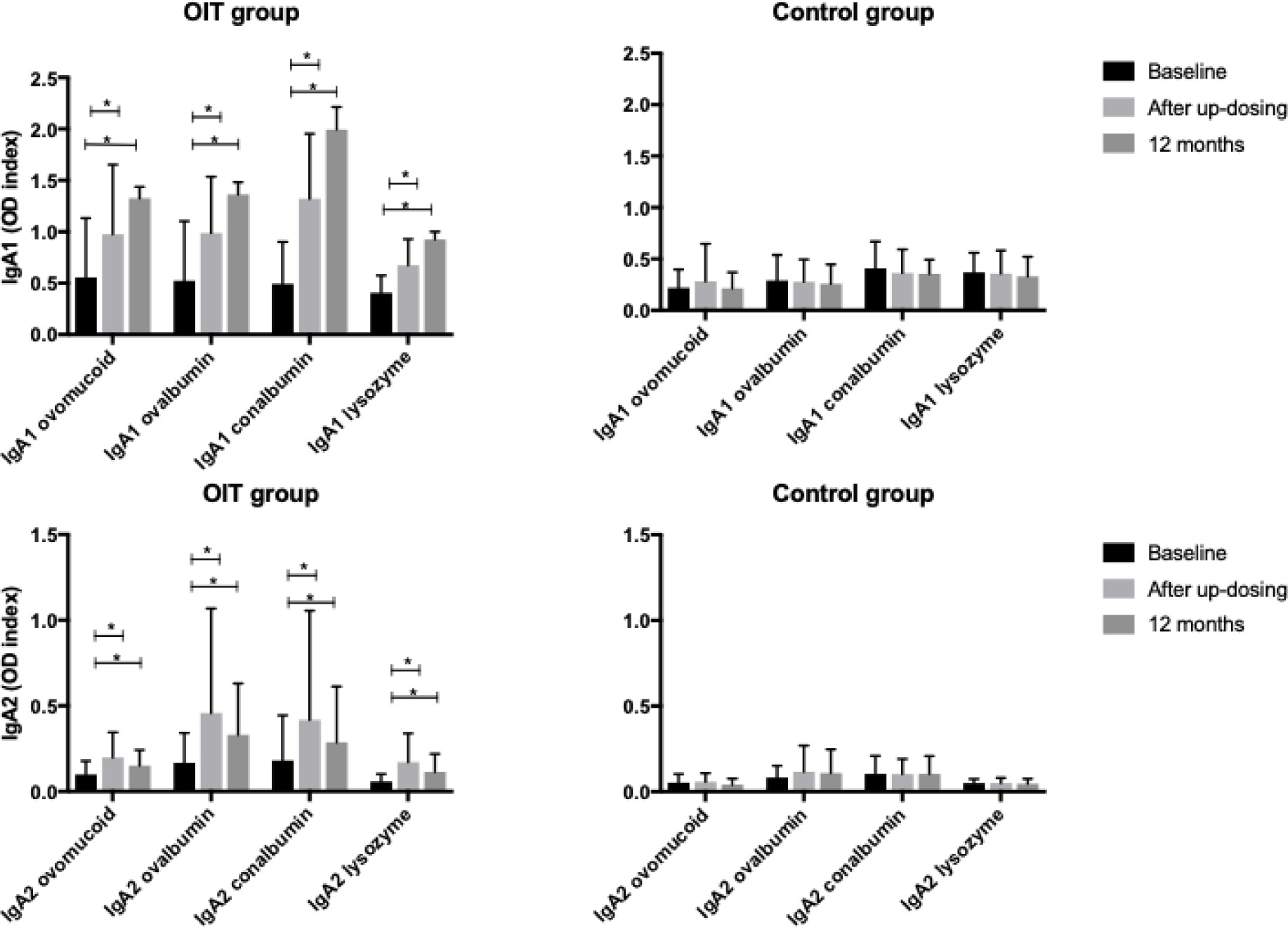
Component-specific IgA1 and IgA2 levels
IgA1 and IgA2 results are presented in Figure 4. In the OIT group, all component-specific IgA1 and IgA2 antibody levels increased during up-dosing and demonstrated sustained increase during 1-year follow-up: (P < 0.0002). No increase was observed in the control group (P = 0.22).
Figure 4 Changes in specific IgA levels during OIT. Component-specific IgA1 and IgA2 antibody levels (mean OD index) against egg white, ovomucoid, ovalbumin, conalbumin, and lysozyme at the commencement of the study (baseline), and after up-dosing and 1 year (12 months) of treatment (OIT group) or follow-up (control group). Comparisons in the OIT and control groups were performed with linear mixed models for repeated measurements. *P < 0.05
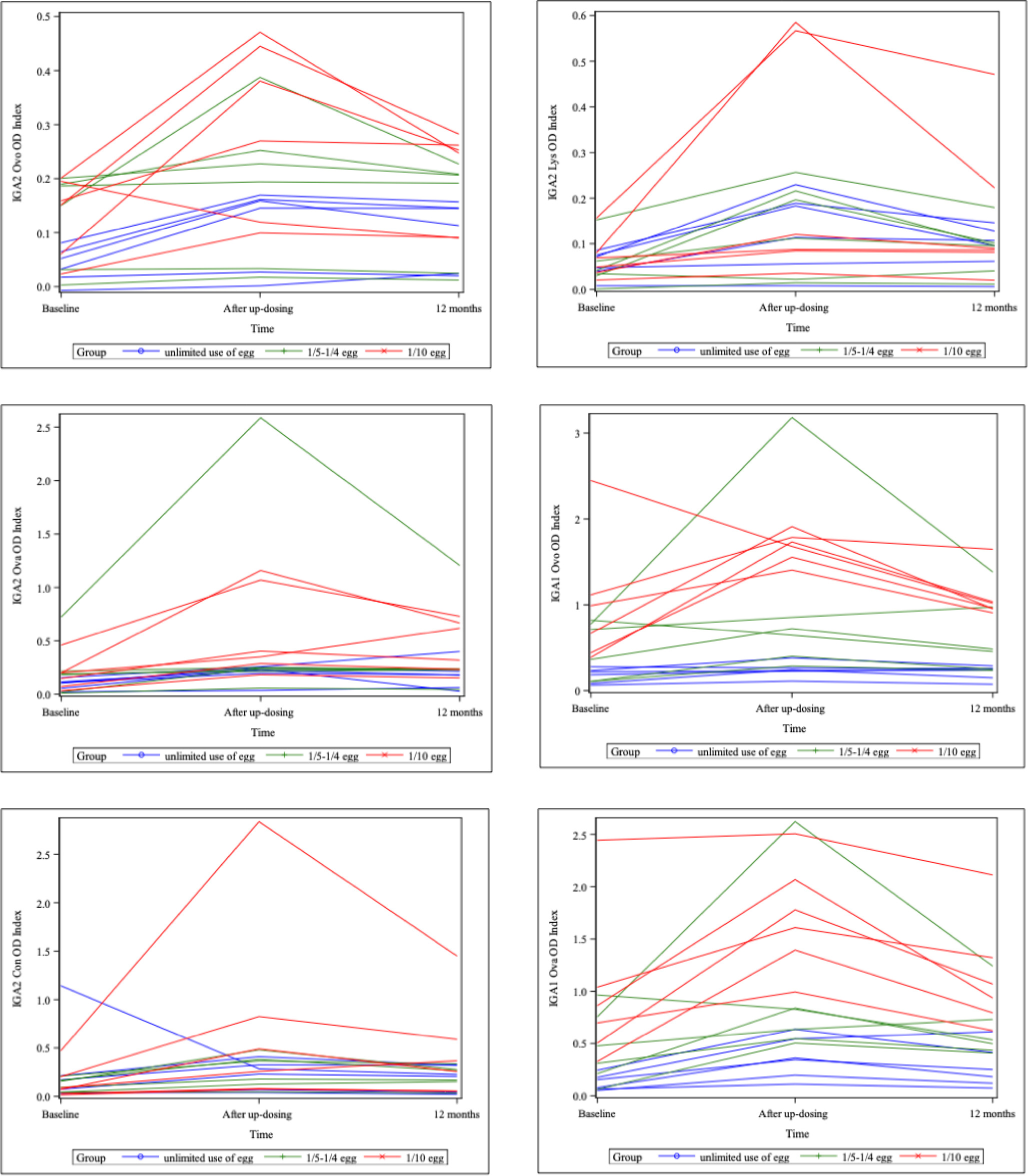
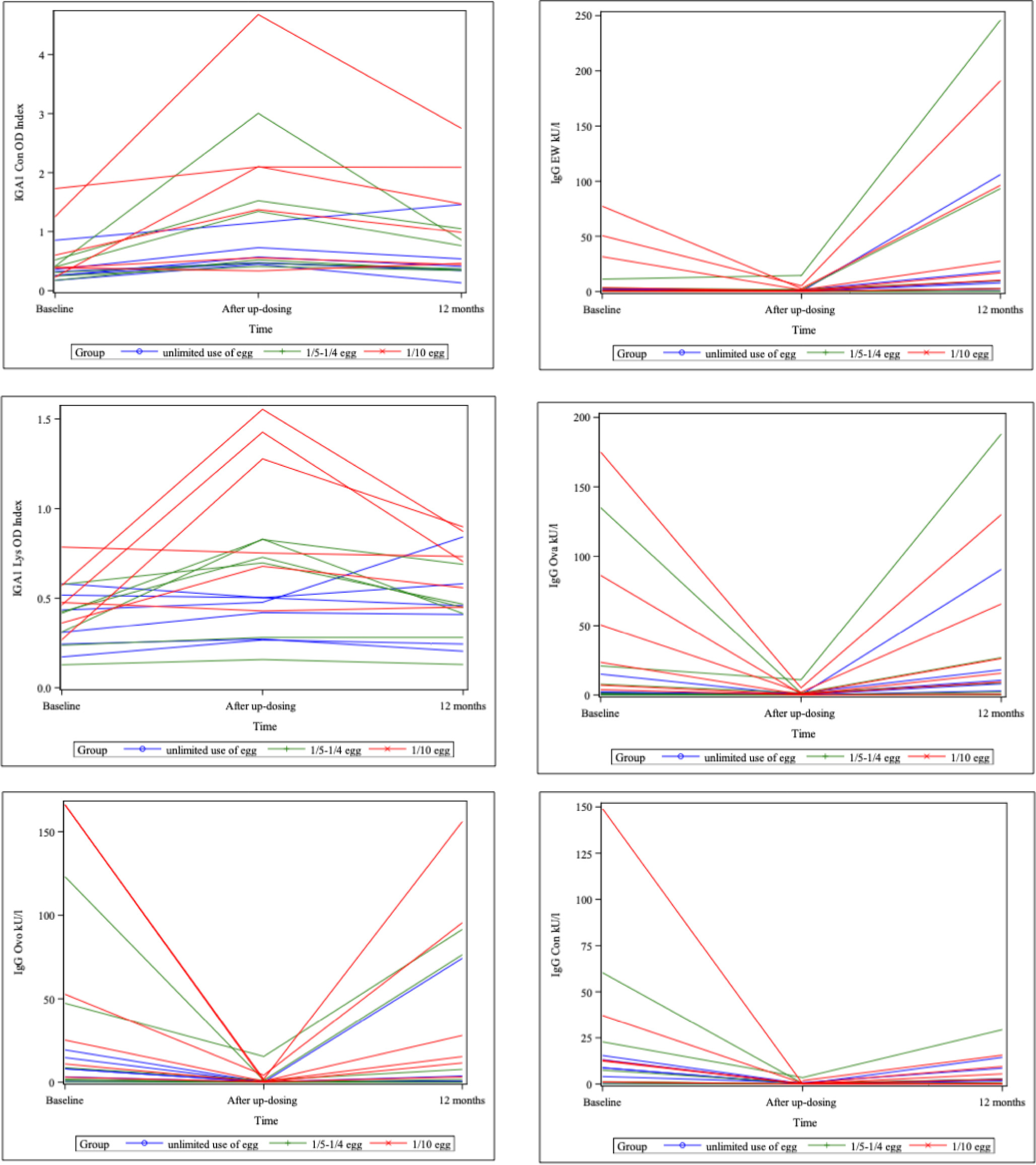
Antibody levels in subgroups
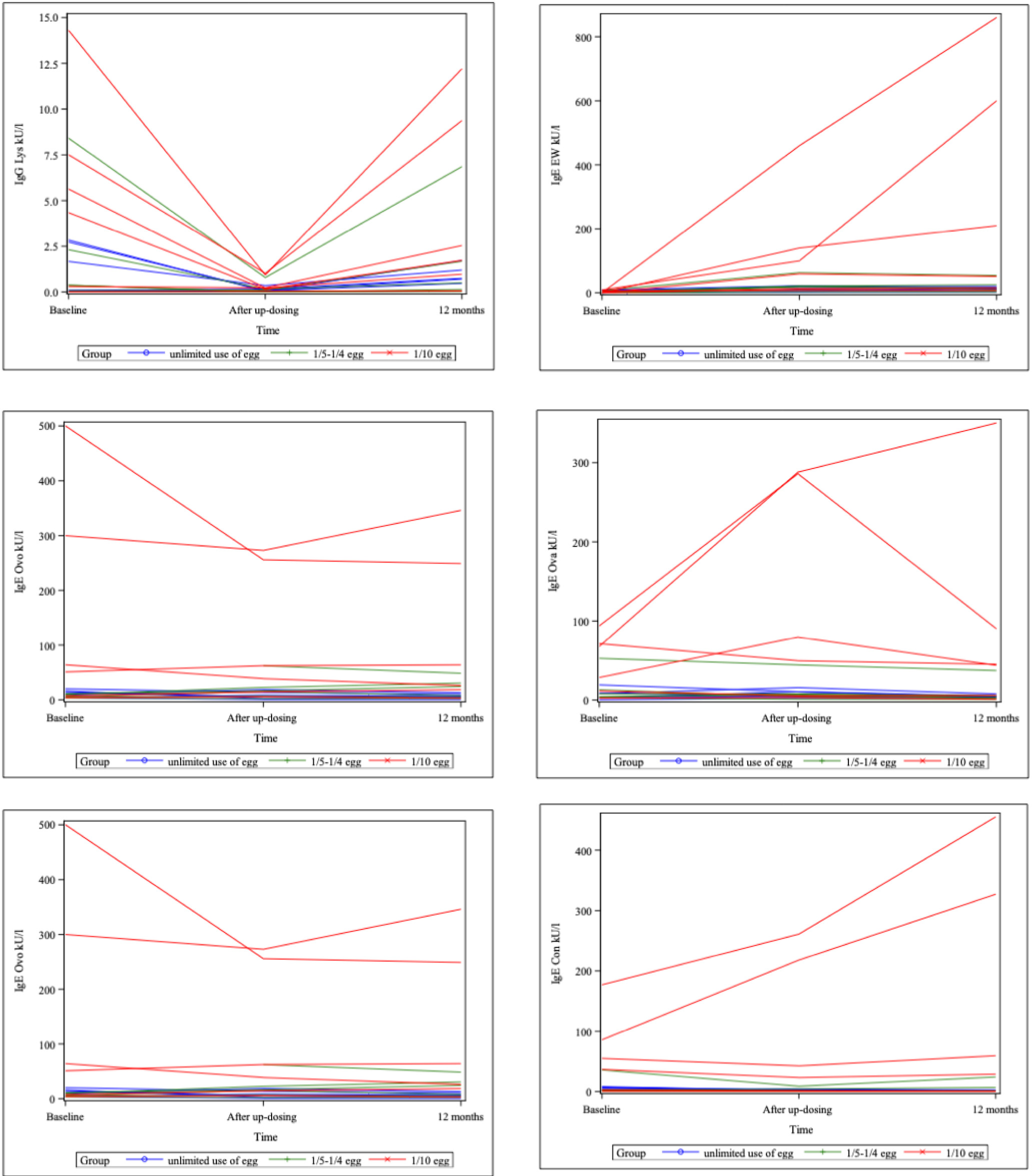
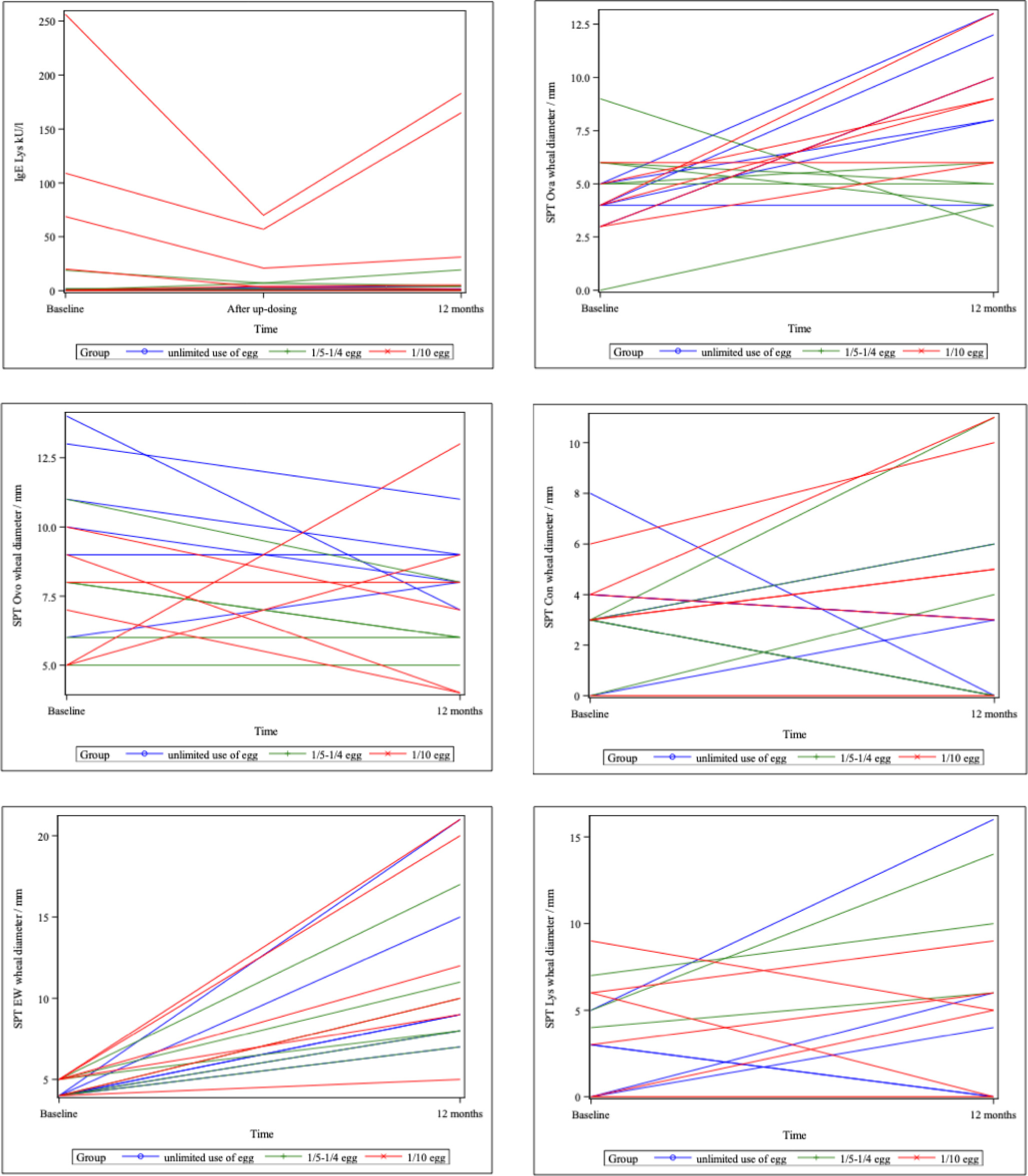
The treated children could be divided in three subgroups based on the use of egg at 12 months of treatment: use of 1/10th of egg (six patients), use of 1/5th–1/4th of egg (six patients), and unlimited use of egg (six patients). The egg white and component-specific SPT, IgE, IgG4, and IgA results are presented in Supplementary Figure 3.
Egg white and all component-specific IgE levels were more than ten-fold in children using only 1/1th of egg daily, compared to children with unlimited use of egg. While no difference was observed in baseline egg white--specific IgE between the groups, the component-specific IgE levels were elevated already at baseline. As well the egg white and component-specific IgG4 were higher in -children in the 1/10th of egg subgroup, compared to the children in the unlimited use subgroup at baseline and at 12 months, with clearly decreased levels after up-dosing. The increased levels in the 1/10th of egg subgroup were observed in IgA1 levels as well.
Discussion
In this study, we demonstrated that a lightened version of egg OIT in 6–16-year old children was equally effective and safer, compared to earlier studies.8,10,11,17,18 In addition, obtained results showed decreased egg component-induced wheal reactions in skin-prick tests and egg component--specific IgE levels in the actively treated OIT group. Furthermore, we found increased egg component-specific IgG4, IgA1, and IgA2 levels in the active OIT group. It was noteworthy that not only ovomucoid but all other components were involved as well, although egg was used as a part of daily diet during the maintenance phase.
Most previous egg OIT studies were performed using high doses (1–4 g) of dried egg white in both up-dosing and during maintenance.8–11 However, in a study of OIT in peanut--allergic preschool children, a maintenance dose of 300 mg was as effective as a 3000-mg dose.19 Our study used egg white powder during short up-dosing to 200 mg, a dose that prevented an average accidental exposure to egg--containing product (70–150 mg).20 Thereafter, the maintenance phase was carried out with egg-containing foods as a part of normal diet. The daily egg dose was increased from the starting dose of 1/10th of an egg in two-thirds of the children up to unlimited use of eggs in one-third of the treated children after 12 months of treatment. This study design was less heavy for the children and resulted in good adherence and fewer adverse events. There were no dropouts during OIT and follow-up period and the reported adverse reactions were mild, compared to previous studies.20 During up-dosing, we administered cetirizine to prevent adverse reactions. This is a routine practice in all Finnish allergen immunotherapy centers.21 Premedication with antihistamines could be a part of routine clinical practice in OIT, but the future comparative studies are required to assess clinical benefits.
Decrease in IgE and increase in IgG4, IgA1, and IgA2 in case of all four studied egg components were observed after 12 months of therapy. Our results with IgE, IgG, and IgA were in line with earlier studies showing decrease in component-specific IgE and increase in IgG4 and IgA.9,12,22 More importantly, we had a control group and studied IgA subclasses and showed the desensitization in vivo with SPT. Our results with skin test outcomes, IgE, IgG4, and IgA, were in accord with to the results of earlier studies that studied only egg white, ovalbumin and ovomucoid.11,12,22 We observed similar responses in addition to ovalbumin and ovomucoid to conalbumin and lysozyme. Conalbumin and lysozyme were included, in addition to ovalbumin and ovomucoid, in a study comprising 50 children and no control group.9 Contrary to that study, we found decrease in ovomucoid-, conalbumin-, and lysozyme-specific IgE and increase in conalbumin- and lysozyme-specific IgA. In addition, our study was the first to analyze IgA subclasses against all egg white components.
The amount of egg that the patients consumed daily at 12 months of treatment varied between 1/10th of egg and 1/5th–1/4th of egg to the unlimited use of egg. A subgroup analysis of the egg white and component-specific baseline levels was more than ten-fold higher in the 1/10th of egg subgroup, compared to the unlimited use subgroup. These high levels of IgE were likely to be the explanation for the unsuccessful attempts to increase the daily use of egg in diet.
In earlier studies, OIT was performed with egg white powder. We used egg white powder only during up-dosing and in the maintenance phase of the children using egg as a part of their normal daily diet. Despite of this, the skin test results and antibody responses for all the components were stable after the maintenance phase. The maintained responses for the heat labile components of ovalbumin, conalbumin, and lysozyme could be explained by different levels of denaturation depending on the length and temperature of cooking. The heat labile components may retain more of their antigenicity in omelets, fried or scrambled eggs or pancakes, compared to gratinated foods cooked for longer times at high temperatures in oven. Changes in IgE, IgG4, and IgA, compared to the heat labile ovalbumin, were also observed in a study in which both up-dosing and maintenance phase were performed with 20-min hardboiled egg.12 This finding was in agreement with our observations with conalbumin and lysozyme, in addition to ovalbumin. The denatured proteins may also be able to affect antibody levels. In an immunotherapy study with birch peptides IgA and IgG4 responses were discovered against Bet v 1, suggesting that linear peptides could activate memory B cells.23
In our study, we found significant elevation of IgA1 and IgA2 antibodies against egg components during OIT, which was associated with desensitization. These findings suggested that elevated levels of egg-specific IgA1 and IgA2 could be useful in determining clinical response to egg OIT. These elevated antibodies were likely to be functionally protective after OIT is completed. Both isoforms of serum IgA act similarly despite their reported distributional differences in the body.24 In a previous publication, Kulis et al. reported similar IgA increase in the saliva of subjects who responded favorably to peanut sublingual immunotherapy.25 Increase in antigen-specific IgA2 was also observed in the serum of subjects that had subcutaneous immunotherapy for grass pollen allergy.26 Wright et al. reported higher levels of IgA against egg allergens in subjects that developed sustained unresponsiveness.22
Our results showed that oral tolerance to egg was associated with increase of component-specific IgG4 antibodies. Elevated levels of egg-specific IgG4 could be useful in determining clinical response to egg OIT, and it could be functionally protective against allergic reactivity as well. In previous studies, it was postulated that development of either allergic hypersensitivity or immune tolerance were critically influenced by the balance between IgG4 and IgE production.27,28 The blocking role of IgG4 antibodies was suggested as an explanation for the absence of clinical reactivity in egg allergy and cow’s milk allergy.28,29 The induction of egg white-specific IgG4 reduced specific IgE levels in IgE tests by competition of IgG and IgE. This had a major concern in microarray assays, where the amount of allergen in immunomatrix was very low.30 This was also possible in our IgE assays, although less likely, as we used ImmunoCAP, where the amount of allergens in immunomatrix was high. In general, the presence of allergen-specific IgG4 indicates that anti-inflammatory and tolerance-inducing mechanisms are activated.
Patient visits in this study were carried out as a part of normal outpatient clinic of allergic children. This limited our resources to use an open OFC instead of double-blind challenges. Although this could be a limitation to our study, the age of our patients and their type of clinical reactivity allowed an objective assessment of clinical manifestations. Furthermore, the additive value of double-blind challenges was limited even in much younger children.31
Conclusion
We used a lightened egg OIT protocol with a short up-dosing with EW powder of just 200 mg and the maintenance phase thereafter with an egg as a part of normal daily diet. This approach afforded a good clinical response and an expected humoral immune response against all egg white components. The obtained desensitization and skin-prick and humoral responses to all components of egg could be maintained with egg in daily diet, mainly processed by cooking. Additional data are available in the Supplementary Tables and Figures after the reference list.
Acknowledgments
We thank Asta Simola and Taina Suominen, pediatric nurses performing OIT, and Leena Kavén-Honka for technical assistance.
Conflict of interest
Johannes Savolainen (ALK, Thermo Fisher Scientific Phadia); other authors had no conflict of interest to declare.
REFERENCES
1. Pyrhonen K, Nayha S, Kaila M, Hiltunen L, Laara E. Occurrence of parent-reported food hypersensitivities and food allergies among children aged 1–4 yr. Pediatr Allergy Immunol. 2009;20(4):328–38. 10.1111/j.1399-3038.2008.00792.x
2. Boyano-Martinez T, Garcia-Ara C, Diaz-Pena JM, Martin-Esteban M. Prediction of tolerance on the basis of quantification of egg white-specific IgE antibodies in children with egg allergy. J Allergy Clin Immunol. 2002;110(2):304–9. 10.1067/mai.2002.126081
3. Bollinger ME, Dahlquist LM, Mudd K, Sonntag C, Dillinger L, McKenna K. The impact of food allergy on the daily activities of children and their families. Ann Allergy Asthma Immunol. 2006;96(3):415–21. 10.1016/S1081-1206(10)60908-8
4. Makinen-Kiljunen S, Haahtela T. Eight years of severe allergic reactions in Finland: A register-based report. World Allergy Organ J. 2008;1(11):184–9. 10.1097/WOX.0b013e3181898224
5. Muraro A, Halken S, Arshad SH, Beyer K, Dubois AE, Du Toit G, et al. EAACI food allergy and anaphylaxis guidelines. Primary prevention of food allergy. Allergy. 2014;69(5):590–601. 10.1111/all.12398
6. Nwaru BI, Takkinen HM, Kaila M, Erkkola M, Ahonen S, Pekkanen J, et al. Food diversity in infancy and the risk of childhood asthma and allergies. J Allergy Clin Immunol. 2014;133(4):1084–91. 10.1016/j.jaci.2013.12.1069
7. Muraro A, Roberts G, Halken S, Agache I, Angier E, Fernandez-Rivas M, et al. EAACI guidelines on allergen immunotherapy: Executive statement. Allergy. 2018;73(4):739–43. 10.1111/all.13420
8. Burks AW, Jones SM, Wood RA, Fleischer DM, Sicherer SH, Lindblad RW, et al. Oral immunotherapy for treatment of egg allergy in children. N Engl J Med. 2012;367(3):233–43. 10.1056/NEJMoa1200435
9. Palosuo K, Karisola P, Savinko T, Fyhrquist N, Alenius H, Makela MJ. A randomized, open-label trial of hen’s egg oral immunotherapy: Efficacy and humoral immune responses in 50 children. J Allergy Clin Immunol Pract. 2021;9(5):1892–901.e1. 10.1016/j.jaip.2021.01.020
10. Caminiti L, Pajno GB, Crisafulli G, Chiera F, Collura M, Panasci G, et al. Oral Immunotherapy for egg allergy: A double--blind placebo-controlled study, with postdesensitization follow-up. J Allergy Clin Immunol Pract. 2015;3(4):532–9. 10.1016/j.jaip.2015.01.017
11. Perez-Rangel I, Rodriguez Del Rio P, Escudero C, Sanchez-Garcia S, Sanchez-Hernandez JJ, Ibanez MD. Efficacy and safety of high-dose rush oral immunotherapy in persistent egg allergic children: A randomized clinical trial. Ann Allergy Asthma Immunol. 2017;118(3):356–64.e3. 10.1016/j.anai.2016.11.023
12. Sugimoto M, Kamemura N, Nagao M, Irahara M, Kagami S, Fujisawa T, et al. Differential response in allergen--specific IgE, IgGs, and IgA levels for predicting outcome of oral immunotherapy. Pediatr Allergy Immunol. 2016;27(3):276–82. 10.1111/pai.12535
13. Sampson HA, Gerth van Wijk R, Bindslev-Jensen C, Sicherer S, Teuber SS, Burks AW, et al. Standardizing double-blind, placebo--controlled oral food challenges: American Academy of Allergy, Asthma & Immunology-European Academy of Allergy and Clinical Immunology PRACTALL consensus report. J Allergy Clin Immunol. 2012;130(6):1260–74. 10.1016/j.jaci.2012.10.017
14. Ansotegui IJ, Melioli G, Canonica GW, Caraballo L, Villa E, Ebisawa M, et al. IgE allergy diagnostics and other relevant tests in allergy, a World Allergy Organization position paper. World Allergy Organ J. 2020;13(2):100080. 10.1016/j.waojou.2019.100080
15. Heinzerling L, Mari A, Bergmann KC, Bresciani M, Burbach G, Darsow U, et al. The skin prick test—European standards. Clin Transl Allergy. 2013;3(1):3. 10.1186/2045-7022-3-3
16. Haahtela T, von Hertzen L, Makela M, Hannuksela M, Allergy Programme Working G. Finnish Allergy Programme 2008–2018—Time to act and change the course. Allergy. 2008;63(6):634–45. 10.1111/j.1398-9995.2008.01712.x
17. Giavi S, Vissers YM, Muraro A, Lauener R, Konstantinopoulos AP, Mercenier A, et al. Oral immunotherapy with low allergenic hydrolysed egg in egg allergic children. Allergy. 2016;71(11):1575–84. 10.1111/all.12905
18. Graham F, Tardio N, Paradis L, Des Roches A, Begin P. Update on oral immunotherapy for egg allergy. Hum Vaccin Immunother. 2017;13(10):2452–61. 10.1080/21645515.2017.1339844
19. Vickery BP, Berglund JP, Burk CM, Fine JP, Kim EH, Kim JI, et al. Early oral immunotherapy in peanut-allergic preschool children is safe and highly effective. J Allergy Clin Immunol. 2017;139(1):173–81.e8. 10.1016/j.jaci.2016.05.027
20. Buchanan AD, Green TD, Jones SM, Scurlock AM, Christie L, Althage KA, et al. Egg oral immunotherapy in nonanaphylactic children with egg allergy. J Allergy Clin Immunol. 2007;119(1):199–205. 10.1016/j.jaci.2006.09.016
21. Rodriguez Del Rio P, Alvarez-Perea A, Blumchen K, Caimmi D, Caubet JC, Konstantinopoulos AP, et al. Food immunotherapy practice: Nation differences across Europe, The FIND project. Allergy. 2021. 10.1111/all.15016
22. Wright BL, Kulis M, Orgel KA, Burks AW, Dawson P, Henning AK, et al. Component-resolved analysis of IgA, IgE, and IgG4 during egg OIT identifies markers associated with sustained unresponsiveness. Allergy. 2016;71(11):1552–60. 10.1111/all.12895
23. Spertini F, Della Corte G, Kettner A, de Blay F, Jacobsen L, Jutel M, et al. Efficacy of 2 months of allergen-specific immunotherapy with Bet v 1-derived contiguous overlapping peptides in patients with allergic rhinoconjunctivitis: Results of a phase IIb study. J Allergy Clin Immunol. 2016;138(1):162–8. 10.1016/j.jaci.2016.02.044
24. Pakkanen SH, Kantele JM, Moldoveanu Z, Hedges S, Hakkinen M, Mestecky J, et al. Expression of homing receptors on IgA1 and IgA2 plasmablasts in blood reflects differential distribution of IgA1 and IgA2 in various body fluids. Clin Vaccine Immunol. 2010;17(3):393–401. 10.1128/CVI.00475-09
25. Kulis M, Saba K, Kim EH, Bird JA, Kamilaris N, Vickery BP, et al. Increased peanut-specific IgA levels in saliva correlate with food challenge outcomes after peanut sublingual immunotherapy. J Allergy Clin Immunol. 2012;129(4):1159–62. 10.1016/j.jaci.2011.11.045
26. Pilette C, Nouri-Aria KT, Jacobson MR, Wilcock LK, Detry B, Walker SM, et al. Grass pollen immunotherapy induces an allergen-specific IgA2 antibody response associated with mucosal TGF-beta expression. J Immunol. 2007;178(7):4658–66. 10.4049/jimmunol.178.7.4658
27. Aalberse RC, Stapel SO, Schuurman J, Rispens T. Immunoglobulin G4: An odd antibody. Clin Exp Allergy. 2009;39(4):469–77. 10.1111/j.1365-2222.2009.03207.x
28. Caubet JC, Lin J, Ahrens B, Gimenez G, Bardina L, Niggemann B, et al. Natural tolerance development in cow’s milk allergic children: IgE and IgG4 epitope binding. Allergy. 2017;72(11):1677–85. 10.1111/all.13167
29. Strait RT, Morris SC, Finkelman FD. IgG-blocking antibodies inhibit IgE-mediated anaphylaxis in vivo through both antigen interception and Fc gamma RIIb cross-linking. J Clin Invest. 2006;116(3):833–41. 10.1172/JCI25575
30. Sereme Y, Casanovas N, Michel M, Martin-Blondel A, Mankouri F, Pinchemel S, et al. IgG removal significantly enhances detection of microarray allergen-specific IgE reactivity in patients’ serum. Allergy. 2021;76(1):395–8. 10.1111/all.14536
31. Isolauri E, Turjanmaa K. Combined skin prick and patch testing enhances identification of food allergy in infants with atopic dermatitis. J Allergy Clin Immunol. 1996;97(1, Pt 1): 9–15. 10.1016/S0091-6749(96)70277-4
Supplementary
Table S1 Modified open OFC and raw egg powder up-dosing protocol.
| Modified open OFC* | ||
|---|---|---|
| Dose No. | Raw egg powder, single dose (mg) | Raw egg powder, cumulative dose (mg) |
| 1. | 0.1 | 0.1 |
| 2. | 0.2 | 0.3 |
| 3. | 0.4 | 0.7 |
| 4. | 0.8 | 1.5 |
| 5. | 1.5 | 3 |
| 6. | 3 | 6 |
| 7. | 6 | 12 |
| 8. | 12 | 24 |
| 9. | 25 | 49 |
| 10. | 50 | 99 |
| 11. | 100 | 199 |
| 12. | 200 | 399 |
*Increasing doses were given at approximately every 30 min. If the subject did not tolerate a given dose and symptoms were mild, then that dose or the previously tolerated one dose was repeated, and the protocol proceeded as outlined. If the subject experienced significant symptoms, then the protocol was stopped, and the highest tolerated dose was used as the starting daily dose (Buchanan et al., 2007).20
Figure S1 Study flow diagram (n = 50) of the study protocol of OIT and control groups through the study. All patients who started OIT had reached maintenance dose (200-mg egg white) and passed OFC after 12 months from initiation of the study. Skin-prick tests with egg white, ovomucoid, ovalbumin, conalbumin, and lysozyme were established at commencement of the study (baseline) and after 12 months from initiation of the study. IgE, IgG4, IgA1, and IgA2 antibody levels against egg antigens were examined in the beginning, at the moment of maintenance dose (200-mg egg white) was reached, and after 12 months from initiation of the study
Figure S2 Egg component-specific IgA1 and IgA2 assay. To measure the egg component-specific IgA1 and IgA2 antibodies, Nunc MaxiSorp (Thermo Fisher Scientific Invitrogen) flat-bottomed 96-well ELISA plates were coated with ovalbumin, ovomucoid, conalbumin, or lysozyme diluted in 1 mg/mL phosphate buffered saline (PBS), 50 µL per well, and incubated overnight at 4°C. The plates were washed twice with PBS containing 0.05% Tween (PBS-Tween) and blocked with 1% gelatin in PBS 300 µL per well and incubated for 1 h at 37°C. The plates were washed thrice with PBS-Tween and the serum samples were diluted in the ratio of 1:10 in 1% gelatin in PBS-Tween and added to plates, 100 µL per well, incubated for 1 h at 37°C. The plates were washed thrice with PBS-Tween and the bound antibodies were detected with alkaline phosphatase (AP)-conjugated mouse anti-human IgA1 or IgA2 antibodies (GenWay, San Diego, CA, USA) diluted in the ratio of 1:500 in 1% gelatin in PBS-Tween added to plates, 100 µL per well, and incubated for 1 h at 37°C. The plates were washed thrice with PBS-Tween and the bound AP-conjugate was visualized with paranitrophenyl phosphate disodium substrate (Reagena, Siilinjärvi, Finland) diluted in 1 mg/mL diethanolamine magnesium chloride buffer (Reagena), 100 µL per well, and incubated at 37°C. The enzymatic reaction was stopped after 30 min by addition of 1 N NaOH, 100 µL per well. The absorbance was observed at 405 nm on a Multiscan FC (Thermo Scientific) plate reader and the results were displayed as optical density (OD). Samples from all three time points of each patient were analyzed in parallel on the same plate, allowing paired comparison of IgA levels at different time points of each patient, but IgA comparisons between individual patients were not exercised. Antibody levels in three OIT subgroups: Use of 1/10th of egg, use of 1/5th–1/4th of egg, and unlimited use of egg (six patients in each group)
Figure S3 Spaghetti plots for 18 patients, subgroup analysis.
Table S2 Comparison between OIT subgroups, skin-prick test results.
| OIT group 1 | OIT group 2 | OIT group 3 | P-valuea | P-valueb | P-valuec | |
|---|---|---|---|---|---|---|
| Skin-prick test (mean, mm) | ||||||
| EW, baseline | 4 | 4.5 | 4.7 | 0.01 | 0.05 | 0.6 |
| EW, 12 months | 11.5 | 10.2 | 12.8 | 0.7 | 0.63 | 0.39 |
| Ovom, baseline | 10.5 | 7.7 | 7.3 | 0.05 | 0.08 | 0.79 |
| Ovom, 12 months | 8.7 | 6.5 | 7.5 | 0.45 | 0.02 | 0.51 |
| Oval, baseline | 4.2 | 5.2 | 4.2 | 1 | 0.44 | 0.46 |
| Oval, 12 months | 9.2 | 4.5 | 8.8 | 0.85 | 0.01 | 0 |
| Cona, baseline | 3.7 | 2 | 3.3 | 0.81 | 0.2 | 0.22 |
| Cona, 12 months | 2.5 | 3.5 | 5.7 | 0.13 | 0.63 | 0.41 |
| Lyso, baseline | 1.8 | 2.7 | 4.0 | 0.24 | 0.6 | 0.51 |
| lyso 12 months | 4.3 | 5 | 4.2 | 0.96 | 0.85 | 0.78 |
EW: egg white; OIT group 1: unlimited use of egg; OIT group 2: using 1/5th–1/4th of egg daily; OIT group 3: using 1/10th of egg daily; aP values between OIT groups 1 and 3; bP values between OIT groups 1 and 2; cP values between OIT groups 2 and 3.
Table S3 Comparison between OIT subgroups, IgE values.
| OIT group 1 | OIT group 2 | OIT group 3 | P-valuea | P-valueb | P-valuec | |
|---|---|---|---|---|---|---|
| IgE value (kU/L) | ||||||
| EW, baseline | 4 | 1.8 | 2.5 | 0.56 | 0.35 | 0.75 |
| EW after up-dosing | 12.9 | 22.3 | 130.0 | 0.12 | 0.34 | 0.15 |
| EW, 12 months | 11.8 | 18.8 | 290.6 | 0.09 | 0.41 | 0.09 |
| Ovom, baseline | 11.2 | 6.8 | 154.4 | 0.11 | 0.21 | 0.14 |
| Ovom after up-dosing | 8.4 | 21 | 108.4 | 0.07 | 0.2 | 0.12 |
| Ovom, 12 months | 6.7 | 19.7 | 117.8 | 0.09 | 0.12 | 0.13 |
| Oval, baseline | 7 | 14.1 | 45.9 | 0.03 | 0.41 | 0.09 |
| Oval after up-dosing | 8 | 12 | 118.7 | 0.07 | 0.57 | 0.08 |
| Oval, 12 months | 4.6 | 8.9 | 89.3 | 0.15 | 0.48 | 0.17 |
| Cona, baseline | 5.4 | 7.5 | 59.7 | 0.07 | 0.72 | 0.09 |
| Cona after up-dosing | 2.2 | 2.7 | 91.1 | 0.09 | 0.75 | 0.09 |
| Cona, 12 months | 1.1 | 5.5 | 145.2 | 0.1 | 0.28 | 0.11 |
| Lyso, baseline | 0.7 | 3.8 | 75.8 | 0.09 | 0.33 | 0.1 |
| Lyso after up-dosing | 1.3 | 3 | 26.0 | 0.07 | 0.27 | 0.09 |
| Lyso, 12 months | 1.4 | 4.8 | 64.4 | 0.1 | 0.29 | 0.12 |
EW: egg white; OIT group 1: unlimited use of egg; OIT group 2: using 1/5th–1/4th of egg daily; OIT group 3: using 1/10th of egg daily; aP values between OIT groups 1 and 3; bP values between OIT groups 1 and 2; cP values between OIT groups 2 and 3.
Table S4 Comparison between OIT subgroups, IgG4 values.
| OIT group 1 | OIT group 2 | OIT group 3 | P-valuea | P-valueb | P-valuec | |
|---|---|---|---|---|---|---|
| IgG4 value (kU/L) | ||||||
| EW, baseline | 1.2 | 2.7 | 27.4 | 0.07 | 0.41 | 0.09 |
| EW after up-dosing | 0.4 | 3 | 1.7 | 0.15 | 0.29 | 0.6 |
| EW, 12 months | 24.2 | 58.7 | 57.4 | 0.36 | 0.45 | 0.98 |
| Ovom, baseline | 8.9 | 30.4 | 70.6 | 0.08 | 0.31 | 0.3 |
| Ovom after up-dosing | 0.1 | 3 | 1.2 | 0.1 | 0.27 | 0.52 |
| Ovom, 12 months | 13.3 | 29.5 | 51.6 | 0.2 | 0.46 | 0.48 |
| Oval, baseline | 3.5 | 27.6 | 57.7 | 0.07 | 0.3 | 0.4 |
| Oval after up-dosing | 0.4 | 2.3 | 1.5 | 0.23 | 0.3 | 0.67 |
| Oval, 12 months | 21.8 | 37.7 | 41.2 | 0.44 | 0.64 | 0.93 |
| Cona, baseline | 8.4 | 15.5 | 42.5 | 0.2 | 0.49 | 0.34 |
| Cona after up-dosing | 0.2 | 0.7 | 0.5 | 0.38 | 0.36 | 0.68 |
| Cona, 12 months | 5 | 5.5 | 5.5 | 0.87 | 0.92 | 0.99 |
| Lyso, baseline | 1.2 | 1.9 | 5.3 | 0.09 | 0.64 | 0.21 |
| Lyso after up-dosing | 0.1 | 0.2 | 0.4 | 0.12 | 0.65 | 0.27 |
| Lyso, 12 months | 0.8 | 1.5 | 4.5 | 0.11 | 0.53 | 0.24 |
EW: egg white; OIT group 1: unlimited use of egg; OIT group 2: using 1/5th–1/4th of egg daily; OIT group 3: using 1/10th of egg daily; aP values between OIT groups 1 and 3; bP values between OIT groups 1 and 2; cP values between OIT groups 2 and 3.
cP values between OIT groups 2 and 3.
Table S5 Comparison between OIT subgroups, IgA values.
| OIT group 1 | OIT group 2 | OIT group 3 | P-valuea | P-valueb | P-valuec | |
|---|---|---|---|---|---|---|
| IgA1 OD index | ||||||
| Ovom, baseline | 0.2 | 0.5 | 1.0 | 0.02 | 0.05 | 0.15 |
| Ovom after up-dosing | 0.2 | 1 | 1.7 | 0 | 0.11 | 0.17 |
| Ovom, 12 months | 0.2 | 0.6 | 1.1 | 0 | 0.05 | 0.06 |
| Oval, baseline | 0.1 | 0.5 | 1.0 | 0.02 | 0.04 | 0.16 |
| Oval after up-dosing | 0.4 | 1 | 1.7 | 0 | 0.09 | 0.09 |
| Oval, 12 months | 0.3 | 0.6 | 1.1 | 0 | 0.04 | 0.07 |
| Cona, baseline | 0.4 | 0.3 | 0.8 | 0.16 | 0.82 | 0.12 |
| Cona after up-dosing | 0.6 | 1.2 | 1.9 | 0.09 | 0.21 | 0.42 |
| Cona, 12 months | 0.5 | 0.6 | 1.4 | 0.08 | 0.73 | 0.09 |
| Lyso, baseline | 0.4 | 0.3 | 0.5 | 0.28 | 0.78 | 0.19 |
| Lyso after up-dosing | 0.4 | 0.6 | 1.0 | 0.01 | 0.19 | 0.08 |
| Lyso, 12 months | 0.5 | 0.4 | 0.7 | 0.07 | 0.68 | 0.02 |
| IgA2 OD index | ||||||
| Ovom, baseline | 0 | 0.1 | 0.1 | 0.02 | 0.04 | 0.92 |
| Ovom after up-dosing | 0.1 | 0.2 | 0.3 | 0.03 | 0.28 | 0.23 |
| Ovom, 12 months | 0.1 | 0.1 | 0.2 | 0.04 | 0.38 | 0.3 |
| Oval, baseline | 0.1 | 0.2 | 0.2 | 0.18 | 0.26 | 0.76 |
| Oval after up-dosing | 0.2 | 0.6 | 0.6 | 0.06 | 0.34 | 0.96 |
| Oval, 12 months | 0.2 | 0.4 | 0.5 | 0.04 | 0.33 | 0.66 |
| Cona, baseline | 0.3 | 0.1 | 0.1 | 0.5 | 0.39 | 0.72 |
| Cona after up-dosing | 0.2 | 0.3 | 0.8 | 0.25 | 0.7 | 0.28 |
| Cona, 12 months | 0.2 | 0.2 | 0.5 | 0.25 | 0.82 | 0.27 |
| Lyso, baseline | 0.1 | 0.1 | 0.1 | 0.55 | 0.97 | 0.61 |
| Lyso after up-dosing | 0.1 | 0.1 | 0.2 | 0.32 | 0.91 | 0.35 |
| Lyso, 12 months | 0.1 | 0.1 | 0.2 | 0.34 | 0.92 | 0.32 |
OIT group 1: unlimited use of egg; OIT group 2: using 1/5th–1/4th of egg daily; OIT group 3: using 1/10th of egg daily; aP values between OIT groups 1 and 3; bP values between OIT groups 1 and 2; cP values between OIT groups 2 and 3.