
Download
SHORT COMMUNICATION
Allergen-specific immunotherapy and COVID-19: What happened?
Fabiana Furcia,b*, Bianca Olivieric, Laura Bendad, Federica Robbid, Sofia Vallicellad, Sebastiano Gangemib, Gianenrico Sennaa,c, Marco Caminatic
aAsthma Centre and Allergy Unit, University of Verona and Verona University Hospital, Verona, Italy
bSchool and Operative Unit of Allergy and Clinical Immunology, Department of Clinical and Experimental Medicine, Policlinico G. Martino, University of Messina, Messina, Italy
cDepartment of Medicine, University of Verona and Verona University Hospital, Verona, Italy
dHospital Pharmacy, Verona University Hospital, Verona, Italy
Abstract
Background: The COVID-19 infection played a key role in the discontinuation of patient treatment, such as allergen-specific immunotherapy, in chronic diseases.
Objectives: We conducted a retrospective observational study at Verona University Hospital, Verona, Italy, to assess the level of adherence to sublingual immunotherapy (SLIT) in patients affected by allergic rhinitis and mild asthma.
Materials and Methods: We compared and analysed data related to first prescription and collection of 5-grass-pollen 300-index of reactivity (IR) SLIT and tablet lyophilisate, containing 75,000 standardized quality tablet units (SQ-T) allergen extract of grass-pollen from Phleum pratense L, for the five-year period 2017-2021.In particular we considered the group of naïve patients from 2017 who completed pre-COVID treatment (2017-2019) and the group of naïve patients from 2019 who completed treatment during the COVID period (2019-2021). The significance test used was Student’s t-test, and P ˂ 0.05 was considered as statistically significant.
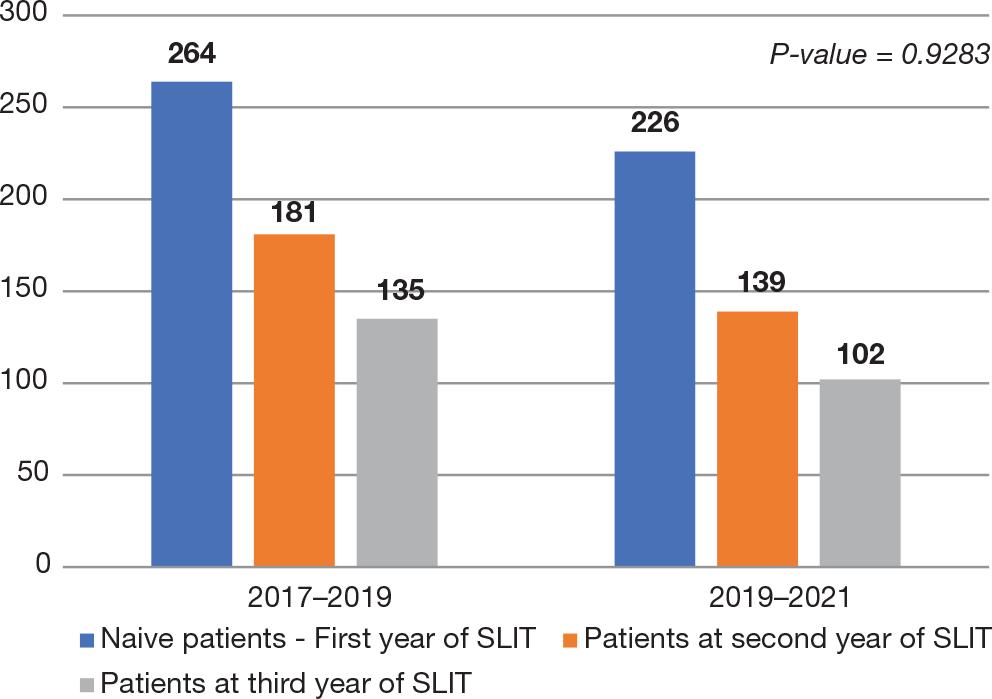
Results: In the three-year period 2017-2019, 264 naïve patients began treatment in 2017, of these 181 continued in 2018, 135 continued in 2019. Instead, for the period 2017–2019, there were 226 naïve patients in 2019; of these 139 continued in 2020, and 102 in 2021.
Conclusions: COVID-19 did not seem to influence adherence to SLIT, which declined independently even in during the pre-pandemic 3-year period.
Key words: adherence, allergen immunotherapy, allergic rhinitis, asthma, COVID-19
*Corresponding author: Fabiana Furci, Asthma Centre and Allergy Unit, University of Verona and Verona University Hospital, Verona, Italy. Email address: [email protected]
Received 12 November 2022; Accepted 5 January 2023; Available online 1 March 2023
Copyright: Furci F, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
The COVID-19 infection played a significant role in the discontinuation of patient treatment, such as allergen-specific immunotherapy (AIT), used in allergic diseases, such as allergic rhinitis and asthma. We conducted a retrospective observational study at Verona University Hospital, Verona, Italy, to assess the true level of adherence to sublingual immunotherapy (SLIT) in patients affected by allergic rhinitis and mild asthma; we prescribed 5-grass-pollen 300-index of reactivity (IR) SLIT and tablet lyophilisate for sublingual administration, containing 75,000 standardized quality tablet units (SQ-T) of allergen extract of grass--pollen from Phleum pratense L.1,2 AIT is a long-term treatment that not only acts on the symptoms of allergic rhinitis but also changes the course of the disease. However, to achieve efficacy, it is important that the treatment is taken continuously for 3 years.3 Real-life studies have shown that adherence to AIT is even lower than that reported in controlled clinical trials. Studies which directly compared the adherence rates between subcutaneous immunotherapy (SCIT) and SLIT demonstrated conflicting results.4,5 In a large retrospective analysis of a community pharmacy database from the Netherlands, only 18% of users reached the minimally required duration of treatment of 3 years (SCIT, 23%; SLIT, 7%) and the median duration for SCIT and SLIT users was 1.7 and 0.6 years, respectively.6
Subcutaneous immunotherapy requires patients to attend clinics on a weekly or monthly basis for injections whereas SLIT has the advantage of being self-administered at home, except for the first dose, which is usually administrated in the clinic to ensure appropriate management of early local clinical manifestations. In the context of the COVID-19 pandemic, SCIT represented a problem of management whereas SLIT allowed patients to start therapy under in-person supervision and/or continue therapy without having to access the healthcare facility. In the present paper, it was proposed to permanently or temporarily switch from a SCIT course to SLIT, thus preventing the consequences of discontinuation of therapy.
In particular, in the present study, in order to assess whether the pandemic had an effect on treatment support, we compared the adherence of patients with allergic rhinitis treated with grass-pollen SLIT during the 3-year period preceding the COVID-19 pandemic (2017–2019) to the data from the following 3-year period (2019–2021). In addition, we compared the cumulative number of treatment--naïve patients who started SLIT for the first time during the pre-pandemic 2-year period (2018–2019) to those who started treatment during the pandemic (2020–2021) to assess whether the COVID-19 pandemic influenced the number of treatment initiations with grass-pollen SLIT. The data were provided by the hospital pharmacy of the University Hospital of Verona (Italy) and comprised the patients who started grass-pollen SLIT Grazax® and Oralair® prescribed by the hospital’s allergy unit. The significance test used was Student’s t-test, and P ˂ 0.05 was considered as statistically significant.
The results demonstrated that 264 treatment-naïve patients with allergic rhinitis started grass-pollen SLIT in 2017. Of these, in 2018, 181 (69%) took the prescribed therapy from the hospital pharmacy, while only 135 (51%) continued in 2019, the third year of treatment. During the following 3-year period, in 2019, 226 naïve patients started SLIT, but in 2020, only 139 patients (62%) collected the prescribed therapy for the second year, and in 2021, only 102 (45%) collected the therapy for the third year from the hospital pharmacy (Figure 1). Comparing the data of the two 3-year periods, there was no statistically significant difference between the trends in loss of adherence to treatment, with P ˃ 0.05 (P = 0.9283).
Figure 1 Comparison of the trend on adherence to grass pollen SLIT for the 3-year period 2017–2019 and 2019–2021.
During the pre-pandemic 2-year period (2018 and 2019), 498 treatment-naïve patients collected grass-pollen SLIT from the hospital pharmacy for the first time, and during the following 2 years, during the pandemic (2020 and 2021), 354 patients collected grass-pollen SLIT for the first time. This represented a 29% drop in patients who started treatment with grass-pollen SLIT during the pandemic period.
Various factors, such as age of patients, cost, inconvenience, and adverse reactions, influenced adherence to therapy.1 However, in the present study, the problem of cost did not exist, as for this type of immunotherapy, there was no cost component for patients. No details were available as to why so many patients abandoned immunotherapy in the second or third year, but this was reflected in the effectiveness of the treatment, which must have been continued for 3 years to have long-term results.7 The negative effect that loss of adherence to therapy had on public health expenditures could not be ignored. Allergic rhinitis always has a great economic impact, and immunotherapy is an investment in patient care, but if it is not continued for 3 years, it is a waste of resources. The greatest concern was that the pandemic would have a negative effect on AIT adherence, particularly for SCIT, but to a lesser extent also for SLIT. In contrast, COVID-19 did not seem to affect adherence to SLIT, which declined on an individual basis even during the pre-pandemic 3-year period.
Author Contributions
All the authors were equally involved in the conception and designing of the work, analysis of the data, drafting of the work, and approval of the final version of the paper to be published.
REFERENCES
1. Musa F, Al-Ahmad M, Arifhodzic N, Al-Herz W. Compliance with allergen immunotherapy and factors affecting compliance among patients with respiratory allergies. Hum Vaccin Immunother. 2017;13:514–17. 10.1080/21645515.2016.1243632
2. Aytekin ES, Soyer O, Şekerel BE, Şahiner UM. Subcutaneous allergen immunotherapy in children: Real life compliance and effect of COVID-19 pandemic on compliance. Int Arch Allergy Immunol. 2021;182:631–6. 10.1159/000514587
3. Durham SR, Emminger W, Kapp A, de Monchy JG, Rak S, Scadding GK, et al. SQ-standardized sublingual grass immunotherapy: Confirmation of disease modification 2 years after 3 years of treatment in a randomized trial. J Allergy Clin Immunol. 2012;129:717–25.e5. 10.1016/j.jaci.2011.12.973
4. Senna G, Caminati M, Lockey RF. Allergen immunotherapy adherence in the real world: How bad is it and how can it be improved? Curr Treat Options Allergy. 2015;2:39–53. 10.1007/s40521-014-0037-6
5. Senna G, Caminati M, Canonica GW. Safety and tolerability of sublingual immunotherapy in clinical trials and real life. Curr Opin Allergy Clin Immunol. 2013;13:656–62. 10.1097/ACI.0000000000000007
6. Kiel MA, Röder E, Gerth van Wijk R, Al MJ, Hop WC, Rutten-van Mölken MP. Real-life compliance and persistence among users of subcutaneous and sublingual allergen immunotherapy. J Allergy Clin Immunol. 2013;132:353–60. 10.1016/j.jaci.2013.03.013
7. Penagos M, Eifan AO, Durham SR, Scadding GW. Duration of allergen immunotherapy for long-term efficacy in allergic rhinoconjunctivitis. Curr Treat Options Allergy. 2018;5:275–90. 10.1007/s40521-018-0176-2