
Download

CASE REPORT
Combined application of dupilumab and mite allergen-specific immunotherapy in children with moderate to severe atopic dermatitis
Bo Ding, Yin Lai, Yanming Lu*
Department of Pediatrics, Renji Hospital affiliated to ShangHai JiaoTong University School of Medicine, Shanghai, China
Abstract
Background: Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disease that manifests in skin dryness, severe itching, and eczema, and can significantly impact a patient’s quality of life. Current treatment regimens do not prevent the recurrence of the disease and are associated with adverse effects. Here, we report two cases of moderate-to-severe AD in children that were treated with dupilumab, a dual inhibitor of IL-4 and IL-13 signaling, in combination with mite allergen-specific immunotherapy.
Case summary: Both patients presented with the diagnosis of AD that was not adequately controlled by the conventional treatment regimen, including topical corticosteroids (TCS), topical calcineurin inhibitors, emollients, and the traditional Chinese medicine treatments. In both patients, AD-associated skin irritation impacted the quality of life, disturbed sleep patterns, and caused stress and anxiety.
Patients received treatment with dupilumab and mite allergen-specific immunotherapy in addition to the baseline treatment regimen of external glucocorticoids (TCS) and oral antihistamines. Nine months after beginning of treatment, clinical symptoms, signs, medication scores, and evaluation scale scores of both children significantly improved, and the treatment was associated with an overall good tolerance.
Conclusion: A combination of dupilumab and mite allergen-specific immunotherapy in addition to the standard anti-AD treatment improves clinical symptoms and is not associated with increased incidence of adverse effects.
Key words: Anti-AD Treatment, Atopic Dermatitis, Dupilumab, Mite Allergen-specific Immunotherapy, Immunotherapy
*Corresponding author: Yanming Lu, Department of Pediatrics, Renji Hospital (The Southern Division) Affiliated to Shanghai JiaoTong University School of Medicine, 2000 Jiangyue Road, Minhang, Shanghai, China. Email address: [email protected]
Received 18 September 2022; Accepted 5 January 2023; Available online 1 March 2023
Copyright: Ding B, et al.
This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disease characterized by dryness, severe itching, and eczema.1–4 AD can be acute (diffuse plaques, exudates, papules, erythema, and aggressive vesicles), subacute -(redness, dryness, scaly thickening, and exfoliating plaques), and chronic (exfoliation and lichenification).5 The prevalence of AD in children varies from country to country, ranging from 2.7 to 30%.1,2,4,6,7 Most of the AD cases (80%) manifest in infancy or childhood, with a certain natural remission rate. However, in 34% of patients, AD will persist into adulthood or even manifest as a life-long disease.3,4,6 Among children with AD, moderate-to-severe disease accounts for about one-third of the cases.8 About half of the patients with severe AD will develop asthma, and 75% will develop rhinitis.9 In addition, severe skin lesions and itching can lead to sleep and social disturbances, anxiety and depression, low self-esteem, and can seriously affect the quality of life of patients and their families, in addition to a significant -economic burden (1500 €/person/year).2,6,9
The goal of AD management is to develop a treatment plan that will allow to relieve symptoms, prevent disease progression, and at the same time, reduce the risks, associated with the treatment.5 Current FDA-recommended treatment regimens that include active maintenance therapy with topical glucocorticoids (TCS) or calcineurin inhibitors (TCI) are often limited or ineffective for cases of moderate-to-severe AD. Additionally, long-term use of TCS is associated with adverse effects, such as telangiectasia, hirsutism, skin atrophy and systemic resorption.4,8,11,12
The basic feature of AD is CD4+ T helper (Th2)-type inflammation that is initiated by the skin barrier dysfunction, which makes it easy for external environmental substances (such as microorganisms and allergens) to invade the epidermis.1,9,10 Therefore, systemic immunosuppressants, such as cyclosporin, are often used to control acute AD flares.1 However, in addition to the recurrence of disease after discontinuation of systemic therapy, long-term use of cyclospoin is associated with poor tolerance and adverse events, such as nephrotoxicity, hypertension, gingival hyperplasia.8,11,12 IL-4 and IL-13 are key mediators of the Th2 pathway,4 and are closely related to the spread of skin inflammation, epidermal barrier dysfunction, and pruritus.8,13 Dupilumab, a monoclonal antibody blocking interleukin (IL) 4 and IL-13 pathways, is considered a first-line treatment for patients with moderate-to-severe AD that cannot be adequately controlled by local therapy or cannot tolerate systemic therapy. It is approved by the EU and the US FDA for patients over 6 years old with good safety.4,6,10 However, there are only few reports on the clinical applications of dupilumab in children and adolescents.
In 80% of AD patients, the condition is exogenous and is caused by sensitization to different air and food allergens, manifested as elevated levels of total IgE and allergen-specific IgE, and positive skin prick and specific patch tests.14 In exogenous AD, mites play an important role in inducing or aggravating allergic skin lesions and have become the most prevalent allergen (63.3%) in AD children in China.12,14 While mite allergen-specific immunotherapy was initially used to treat allergic rhinitis or asthma, recent studies show the efficiency of allergen-specific immunotherapy in AD patients.15
Recently, several trials showed the efficiency of adding mite allergen-specific immunotherapy to pharmacotherapy with dupilumab in patients with uncontrolled asthma and allergic rhinitis.16,17 However, research in this area is still scarce.
This article reports two cases of moderate-to-severe AD in children controlled by dupilumab combined with mite allergen-specific immunotherapy. To the best of our knowledge, this is the first report of combined dupilumab and mite allergen-specific immunotherapy treatment for AD in children.
Case 1 patient, female, 13 years (Chinese, ethnic Han) old presented with the facial erythema, papules, pruritus, dry skin, and scaling that appeared 6 months after birth. She was diagnosed with “eczema” and was treated with topical corticosteroids and moisturizing cream. The symptoms of the dry skin were relieved by the treatment but recurred after stopping the medication. From the age of 3, the rash began to spread, gradually involving the neck, trunk, and extremities. The patient was prescribed the following medications: (1) TCS: Youzhuoer (0.1% Hydrocortisone Butyrate Cream) applied to the affected area in appropriate doses twice a day and Eloson (mometasone furoate cream 0.1%), applied to the affected area in appropriate doses once a day; (2) TCI: Tacrolimus ointment (calcium-regulated neurophosphatase inhibitor 0.03%), applied dermally to the affected area and rubbed in well, twice a day. However, the condition was not permanently relieved. In recent years, the patient’s condition has continued to worsen (frequent flares in spring and autumn and after swimming), with obvious itching, and sometimes skin ulceration with exudation or bleeding. The patient also complained about the difficulty falling asleep, poor sleep quality, restricted growth, and development.
Physical examination revealed dry skin on the whole body, multiple erythema, maculopapular rash on buttocks, trunk and limbs, scattered scratches, scabs, desquamation, skin pigmentation, and hyperplasia of fine hair.
The patient was diagnosed with severe AD. The patient had a history of allergic reactions: egg yolk allergy at 6 months of age and mango allergy at 3 years of age presenting as a perioral rash. Both allergies resolved with age. Mite allergen sensitization tests were performed with the following results: total IgE: 765, house dust mite (D1) sIGE: 52, dust mite (D2) sIGE: 57, and clawless mite: 1.89.
Case 2 patient was 11 years old (Chinese, ethnic Han) and presented with infantile eczema in infancy, with milk protein allergy (perioral and eyelid edema). Eczema resolved after the topical steroid ointment treatment. In June 2021, a small amount of eczema appeared on the elbows and the back of the knees for no obvious reason, spreading to the limbs, neck, and behind the ears. The rash manifested as erythema, papules, with itching, dry skin, and scaling. The patient was diagnosed with AD in hospital, and repeatedly treated with topical glucocorticoids and emollients. The patient was also administered oral cetirizine, and the condition was monitored during regular follow-ups. After the treatment, the rash subsided, and the dry skin was relieved. However, the condition recurred when the patient stopped the medications, and was manifested by scratching, and sometimes accompanied by skin ulceration and bleeding. Dermatitis was aggravated by water, stress, sun exposure, and rainy weather. After the onset of the disease, the patient’s rashes recurred frequently, the itching was obvious, and sleep was affected, resulting in anxiety and stress.
The diagnosis was severe AD. The patient had intermittent episodes of mild allergic rhinitis. Mite allergen sensitization tests were performed with the following results: total IgE: 1565, streptavidin m6 sIgE: 90, house dust mixed h × 2: ˃100.
Treatment and Outcomes
Considering the long course of the disease, the poor efficacy of traditional treatment, and the efficacy and safety of the drug, after full communication with the patients and their parents, dupilumab and mite allergen--specific immunotherapy were added to the baseline treatment regimen of external glucocorticoids (TCS) and oral antihistamines.
Both children were given a combined dupilumab and subcutaneous immunotherapy (SCIT) treatment. The rationale behind adding dupilumab was to control acute skin inflammation before introducing desensitization therapy, because both children had moderate-to-severe AD. Starting SCIT treatment in such patients may potentially aggravate the symptoms of AD, resulting in treatment failure and recurrence of the disease and loss of parental confidence in the treatment. Treatment regimens for Cases 1 and 2 are summarized in Table 1.
Table 1 Case 1 and Case 2.
| Time/Dupilumab dose | Combination therapy | NRS (a/b) | SCORAD | EASI | IGA | DLQI | POEM | Side effect | |
|---|---|---|---|---|---|---|---|---|---|
| Case 1, female, 12 years old | |||||||||
| Initial/600 mg | Halometasone, Ebastine, Emollients | 8/8 | 63 | 20.4 | 4 | 20 | 20 | Dizziness, oral herpes | |
| Week 3/300 mg | Halometasone, Emollient | 5/5 | 26 | 2.2 | 2 | 17 | 17 | ||
| Week 6/300 mg | Dexamethasone acetate ointment, emollient | 2/2 | 13 | 0.5 | 1 | 13 | 7 | ||
| Week 9/300 mg | – | 2/2 | 13 | 0.8 | 2 | 16 | 8 | Headache | |
| Week 12/300 mg | SCIT (No. 1, Week 14), Emollient | 2/2 | 15.3 | 0.9 | 1 | 13 | 3 | ||
| Week 16/300 mg | SCIT | 2/2 | 13.8 | 0.6 | 1 | 4 | 7 | ||
| Week 20/300 mg | SCIT | 2/2 | 8.1 | 0.3 | 1 | 2 | 3 | Liptis | |
| Week 24/300 mg | SCIT, Claritin | 3/3 | 13.6 | 0.5 | 1 | 1 | 9 | Cheilitis worsens after SCIT, edema of lips and eyelids | |
| Week 28/300 mg | SCIT (No. 4), Claritin, Emollient | 2/2 | 10.2 | 0.4 | 1 | 2 | 7 | Itchy skin | |
| Week 32/300 mg | SCIT, Claritin | 2/2 | 17.1 | 0.6 | 2 | 1 | 11 | ||
| Week 36/300 mg | SCIT | Dry armpit skin | |||||||
| Case 2, Male, 11 years old | |||||||||
| Initial/300 mg | Cetirizine, TCS, Traditional Chinese Medicine | 8/8 | 62.2 | 24.5 | 3 | 15 | 15 | Itching at night, exacerbation of existing dermatitis | |
| Week 2/300 mg | SCIT (No. 1, 5 weeks) cetirizine, TCS, Chinese medicine | 6/8 | 39.2 | 12.4 | 3 | 13 | 14 | Same as initial | |
| Week 6/300 mg | SCIT | 2/3 | 20.8 | 1.5 | 2 | 6 | 7 | Same as initial | |
| Week 10/300 mg | SCIT, TCS (occasional), Imestine Fumarate, Emollients | 4/3 | 22.2 | 2 | 2 | 6 | 4 | Same as initial + conjunctivitis | |
| Week 14/300 mg | SCIT, TCS (occasional), emollients | 5/4 | 23 | 2.4 | 2 | 3 | 12 | Same as initial | |
| Week 18/300 mg | SCIT (No. 4), Emollient | 4/2 | 13.3 | 1.1 | 2 | 2 | 8 | Same as initial | |
| Week 22/300 mg | SCIT, cetirizine, emollient | 2/2 | 23.1 | 4.8 | 2 | 4 | 4 | Same as initial | |
| Week 26/300 mg | SCIT, TCS, Emollients | 2/2 | 14.9 | 1.5 | 2 | 4 | 4 | Same as initial | |
| Week 33/300 mg | SCIT, TCS (occasional), emollients | 2/2 | 17.2 | 0.8 | 1 | 2 | 3 | Same as initial | |
The time marked is the time since the initial Dupilumab treatment.
a/b: Degree of pruritus or severity affecting sleep; DLQI: Dermatology Life Quality Index; EASI: Eczema Area and Severity Index; IGA: Investigator Global Assessment scale for atopic dermatitis; NRS: Pruritus Numerical Rating Scale; POEM: Patient-oriented Eczema Measure; SCIT: subcutaneous immunotherapy; SCORD: Atopic dermatitis severity index; TCS: topical corticosteroids
The immunotherapy preparation used in both patients was Alutard SQ (Alk-Abello Ltd., house dust mite allergen preparation). The instructions for dosing schedule were as follows:
Weeks 1–3: Vial 1: 0.2 ml, 0.4 ml, 0.8 ml;
Weeks 4–6: Vial 2: 0.2 ml, 0.4 ml, 0.8 ml;
Weeks 7–9: Vial 3: 0.2 ml, 0.4 ml, 0.8 ml;
Weeks 10–15: Vial 4: 0.1 ml, 0.2 ml, 0.4 ml, 0.6 ml, 0.8 ml, 1.0 ml.
Week 16: No treatment.
Week 17: Vial 4: 1.0 ml.
Week 21: Vial 4: 1.0 ml.
One injection per month was given thereafter. The concentrations of Vials 1, 2, 3, and 4 were 100; 1000; 10,000; 100,000 SQ-U/ml, respectively.
The condition of both patients was assessed using the following tools: pruritus Numerical Rating Scale (NRS), Scoring atopic dermatitis (SCORAD; Eczema Area and Severity Index (EASI); Investigator Global Assessment scale for Atopic Dermatitis (IGA); Dermatology Life Quality Index (DLQI); Patient Oriented Eczema Measure (POEM).18
Medications and condition assessment of both patients in the beginning of the treatment and at follow-up visits are summarized in Table 1 Case 1 and Figures 1–3 (Case 1), and Table 1 Case 2 and Figures 4 and 5 (Case 2).
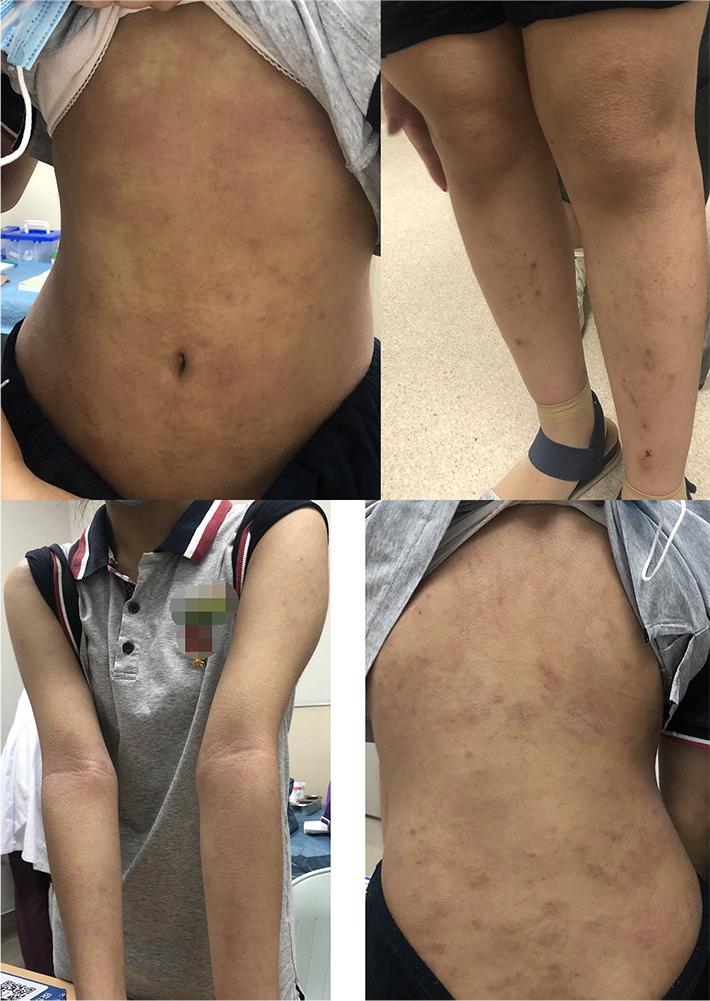
Figure 1 Children before dupilumab (in remission from dermatitis after combined treatment with oral intake of Halometasone and Ebastine): generalized dry skin, multiple erythema, and macular papules on buttocks, trunk and extremities, scattered scratching, crusting and flaking, skin pigmentation.
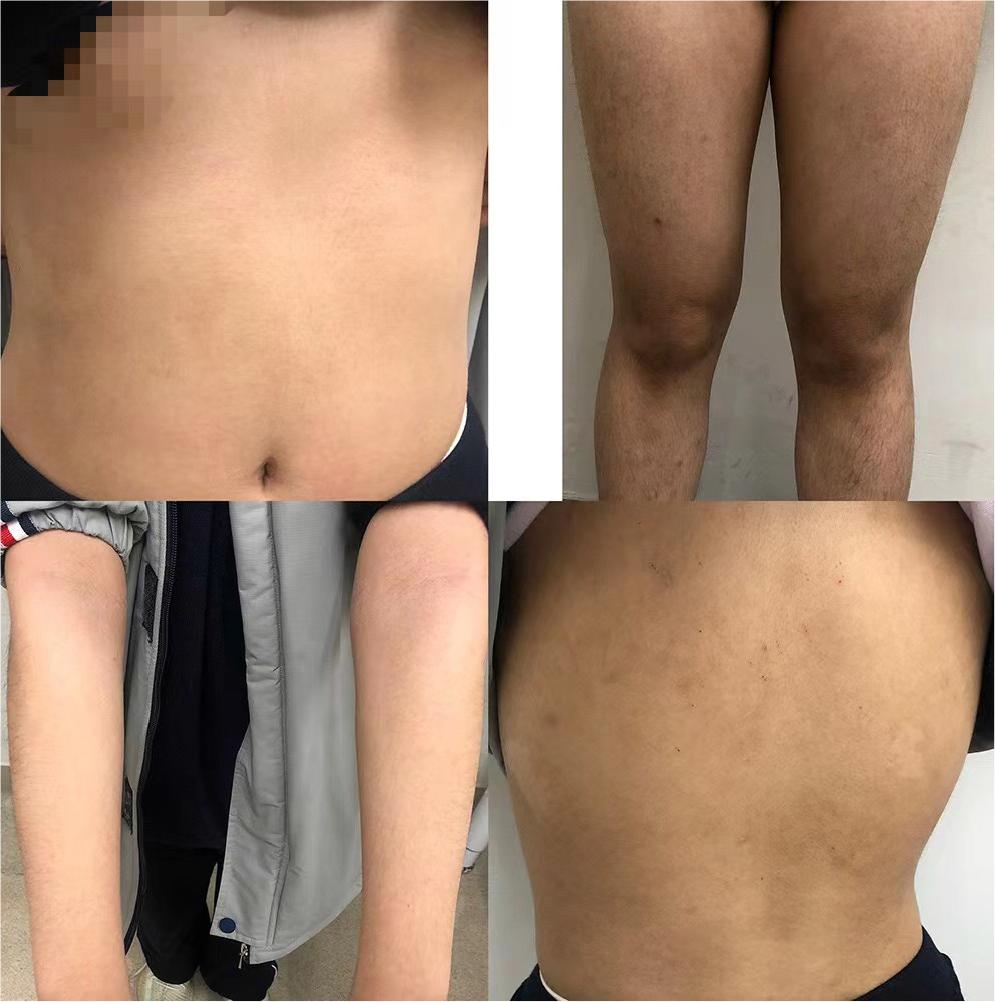
Figure 2 Minor localized erythema, scratching and desquamation after 12 weeks of dupilumab treatment.
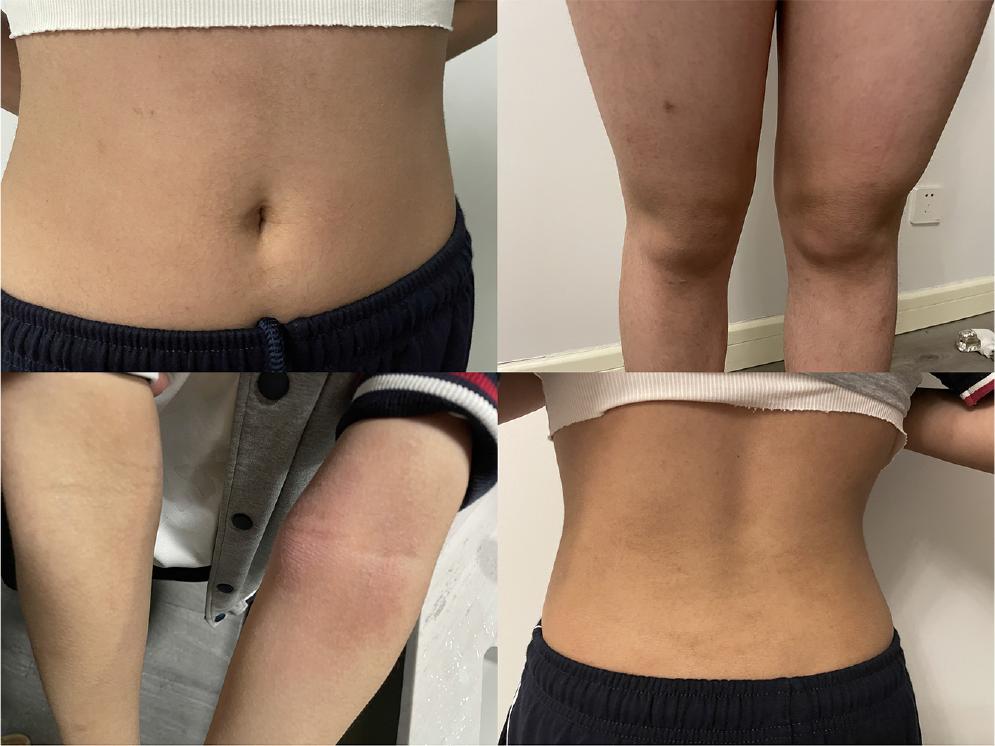
Figure 3 Dupilumab for 36 weeks + SCIT Vial #4 (maintenance phase): with flushed, papulopustular skin visible on the inside of both elbows and dry skin in the axilla.
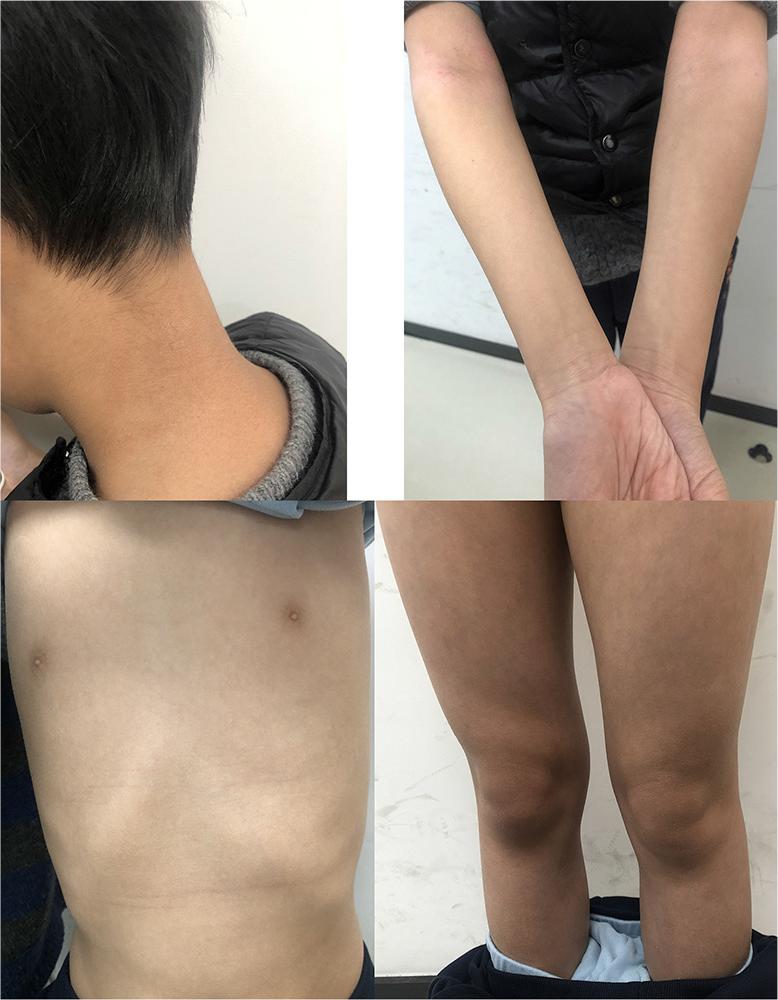
Figure 4 Erythema and papules with hyperpigmentation, with scratching, dryness, and scaling visible behind the ears, neck, trunk, and extremities before dupilumab administration.
Figure 5 Small number of papules, erythema, and localized dry, flaky skin after 30 weeks of dupilumab use.
Results
Considering the weight of the patient in Case 1 (55 kg), the initial dose of dupilumab should have been 400 mg, followed by 200 mg per 2 weeks. However, considering the dosage form and economic issues, the does was converted to an initial dose of 600mg, followed by 300 mg/3 weeks. After the initial treatment, the child had transient dizziness and oral herpes, which did not reappear after clinical observation, but the child’s clinical symptoms, signs, medication scores, and evaluation scale scores were significantly improved. The child developed headache after the injection of dupilumab in the 9th week, and the headache worsened after the injection in the 12th week, which was initially considered to be related to the treatment. The child was administered Saridon, a tablet containing 250 mg acetaminophen, 150 mg isoproterenol, and 50 mg caffeine anhydrous for mild-to-moderate pain, for symptomatic treatment, and the dose of dupilumab was adjusted to 300 mg per 4 weeks. However, the headache was still not relieved. After careful questioning, it became evident that the headache was associated with a state of mental stress (mathematics class) and did not appear during the holidays. The conclusion was made that the headache is not completely related to the treatment. Mite allergen-specific immunotherapy was introduced on Week 14. With the gradual increase in the concentration of SCIT treatment medication, the children’s elbow and axillary dermatitis recurred slightly, but compared with the beginning of treatment, the disease control improved substantially, and the tolerance was good.
Combined with the weight of the child in Case 2 (40 kg), the initial dose of the dupilumab should have been 400 mg, followed by 200 mg every 2 weeks. However, considering the body weight, drug formulation, and economic issues, the dose conversion was adjusted to 300 mg as the -initial dose, and the dose was readministered after 2 weeks, followed by 300 mg per 4 weeks for the duration of the treatment. On the day of each injection of dupilumab, the child developed obvious pruritus and aggravated dermatitis at the original lesion site that improved spontaneously within 2–3 days without special treatment. Allergic conjunctivitis occurred during the treatment and was relieved after symptomatic treatment with Emetin (Emedastine fumarate) eye drops (S.A. Alcon Couvreur N.V., Belgium).
Discussion
Our study demonstrated that the combination of dupilumab and mite allergen-specific immunotherapy in addition to the standard anti-AD treatment improves clinical symptoms and is not associated with increased incidence of adverse effects in children with AD. To the best of our knowledge, this is the first study demonstrating efficiency and safety of the combined dupilumab and SCIT on children with AD.
Previous randomized trial by Corren et al.17 showed that in patients with allergic rhinitis, with 16 weeks of SCIT + dupilumab treatment, improved SCIT tolerability but were not significantly affected by post-allergen challenge nasal symptoms compared with SCIT alone. Recent study by Hoshino et al. showed that mite SCIT combined with standard pharmacotherapy plus dupilumab was clearly beneficial in treating uncontrolled asthma with rhinitis.16 Because ours was a case study of only two patients, we could not perform a comparative evaluation of different therapy strategies. However, our results demonstrate a significant improvement in clinical symptoms and signs, medication scores, and evaluation scale scores in both patients that were not associated with significant adverse effects.
Dupilumab is a fully humanized monoclonal antibody that dually blocks IL-4 and IL-13 downstream signaling by binding to the IL-4 Rα subunit of the IL-4 receptor, thus reducing inflammation. The aggregation of cells in turn alleviates the immune response of Th2 cells.19–21 In a randomized, double-blind, placebo-controlled Phase III clinical study in children and adolescents with AD, dupilumab was shown to significantly improve the symptoms, signs, and quality of life of patients.22,23 Sustained improvement in disease severity was achieved and was well tolerated even when patients continued the use of the drug up to 52 weeks.24 There were only mild to moderate rate of adverse reactions associated with dupilumab treatment, similar to that of the placebo treatment (81 and 77%, respectively).25 Common adverse reactions included injection site reactions (edema, pain, and itching), conjunctivitis, blepharitis, oral herpes, keratitis, itching of eyes, other herpes virus infections, dry eye, and headache, with no increased risk of infection in patients.13,21,22,26,27 In addition, erythema of the head, face, neck, and extremities, related to the application of dupilumab, has also been reported in recent years, and the mechanism may be hypersensitivity reactions related to dupilumab treatment.28 In our study, one patient reported pruritus and aggravated dermatitis at the original lesion site after the dupilumab injection, and the symptoms improved spontaneously within 2–3 days without any special treatment.
A study retrospectively analyzed AD patients who received mite allergen-specific immunotherapy for at least 3 years, and finally 63.5% of patients achieved near or complete clinical remission, and those patients who were younger than 12 years old with moderate-to--severe AD,4 and only sensitized to house dust mite (HDM), had better treatment response. Less than 1% of patients reported side effects, including urticaria, transient worsening of AD lesions, and asthma recurrence. However, the side effects are mild and resolve spontaneously with antihistamines.3 In our study, a patient exhibited symptoms of allergic conjunctivitis during the treatment that was successfully relieved after symptomatic treatment.
Conclusions
This case study reports two patients with moderate-- to-severe AD who had been treated with various topical corticosteroids and other drugs for many years, but the disease was not controlled. Combined dupilumab and mite allergen-specific improved clinical symptoms and signs, medication scores, and evaluation scale scores in both patients with AD and was not associated with significant adverse effects. In both cases, combined treatment improved the patients’ quality of life.
Further studies with large sample sizes are needed to evaluate the effect of the combined treatment in children with AD.
Declarations
Ethics statement
The Ethics Committee of Renji Hospital affiliated to Shanghai Jiaotong University approved this study on July 21, 2021 (Approval no. 2021-037).
Informed consent
The informed consent from each patient was obtained.
Conflict of interest
The authors declare that they have no competing interests.
Funding
Not applicable.
Authors’ contributions
BD analyzed the data and was the major contributor in writing the manuscript. BD and YL contributed to data analysis. Y. Lu was responsible for reviewing and editing the manuscript. All authors read and approved the final manuscript.
REFERENCES
1. Atopic Dermatitis Working Group, Immunology Group, Chinese Society of Dermatology. Guideline for diagnosis and treatment of atopic dermatitis in China. Chin J Dermatol. 2020;53(2): 81–8. 10.35541/cjd.20191000
2. Giavina-Bianchi MH, Giavina-Bianchi P, Rizzo LV. Dupilumab in the treatment of severe atopic dermatitis refractory to systemic immunosuppression: Case report. Einstein Sao Paulo Braz. 2019;17(4):eRC4599. 10.31744/einstein_journal/2019RC4599
3. Lee J, Lee H, Noh S, Bae BG, Shin JU, Park CO, et al. Retrospective analysis on the effects of house dust mite specific immunotherapy for more than 3 years in atopicd. Yonsei Med J. 2016;57(2):393–8. 10.3349/ymj.2016.57.2.393
4. Deleanu D, Nedelea I. Biological therapies for atopic dermatitis: An update. Exp Ther Med. 2019;17(2):1061–7. 10.3892/etm.2018.6989
5. Kulthanan K, Tuchinda P, Nitiyarom R, Chunharas A, Chantaphakul H, Aunhachoke K, et al. Clinical practice guidelines for the diagnosis and management of atopic dermatitis. Asian Pac J Allergy Immunol. 2021;39(3):145–55.
6. Bieber T. Atopic dermatitis: An expanding therapeutic pipeline for a complex disease. Nat Rev Drug Discov. 2022;21(1): 21–40. 10.1038/s41573-021-00266-6
7. Tam H, Calderon MA, Manikam L, Nankervis H, García Núñez I, Williams HC, et al. Specific allergen immunotherapy for the treatment of atopic eczema. Cochrane Database Syst Rev. 2016;2(2):CD008774. 10.1002/14651858.CD008774.pub2
8. Moyle M, Cevikbas F, Harden JL, Guttman-Yassky E. Understanding the immune landscape in atopic dermatitis: The era of biologics and emerging therapeutic approaches. Exp Dermatol. 2019;28(7):756–68. 10.1111/exd.13911
9. Weller K, Soost S, Worm M, Maurer M, Zuberbier T. Atopic dermatitis and allergic rhinitis—Do co-effects in therapy exist? J Dtsch Dermatol Ges J Ger Soc Dermatol JDDG. 2012;10(4): 221–36; quiz 238–9. 10.1111/j.1610-0387.2011.07885.x
10. Giavina-Bianchi M, Giavina-Bianchi P. Efficacy and safety of dupilumab in two adolescents with severe atopic dermatitis. Einstein Sao Paulo Braz. 2021;19:eRC6064. 10.31744/einstein_journal/2021RC6064
11. Davari DR, Nieman EL, McShane DB, Morrell DS. Current Perspectives on the Systemic Management of Atopic Dermatitis. J Asthma Allergy. 2021;14:595–607. 10.2147/JAA.S287638
12. Chan TC, Wu NL, Wong LS, Cho YT, Yang CY, Yu Y, et al. Taiwanese Dermatological Association consensus for the management of atopic dermatitis: A 2020 update. J Formos Med Assoc Taiwan Yi Zhi. 2021;120(1 Pt 2):429–42. 10.1016/j.jfma.2020.06.008
13. Wei D, Ying G a. O. Research advances in the treatment of moderate-to-severe atopic dermatitis in children with dupilumab. Chin J Pract Pediatr. 2021;36(9):660.
14. Dong W lan, An J, Yu M, Yin P, Xu T ling, Liu B, et al. The prevalence and year lived with disability of atopic dermatitis in China: Findings from the global burden of disease study 2019. World Allergy Organ J. 2021;14(11):100604. 10.1016/j.waojou.2021.100604
15. Bae JM, Choi YY, Park CO, Chung KY, Lee KH. Efficacy of allergen-specific immunotherapy for atopic dermatitis: A-systematic review and meta-analysis of randomized controlled trials. J Allergy Clin Immunol. 2013;132(1):110–7. 10.1016/j.jaci.2013.02.044
16. Hoshino M, Akitsu K, Kubota K, Ohtawa J. Efficacy of a house dust mite sublingual immunotherapy tablet as add-on dupilumab in asthma with rhinitis. Allergol Int Off J Jpn Soc Allergol. 2022;71(4):490–7. 10.1016/j.alit.2022.05.010
17. Corren J, Saini SS, Gagnon R, Moss MH, Sussman G, Jacobs J, et al. Short-term subcutaneous allergy immunotherapy and dupilumab are well tolerated in allergic rhinitis: A randomized trial. J Asthma Allergy. 2021;14:1045–63. 10.2147/JAA.S318892
18. Gooderham MJ, Bissonnette R, Grewal P, Lansang P, Papp KA, Hong CH. Approach to the assessment and management of adult patients with atopic dermatitis: A consensus document. Section II: Tools for assessing the severity of atopic dermatitis. J Cutan Med Surg. 2018;22(1_suppl):10S–16S. 10.1177/1203475418803628
19. Zhai LL, Savage KT, Qiu CC, Jin A, Valdes-Rodriguez R, Mollanazar NK. Chronic pruritus responding to dupilumab—-A case series. Med Basel Switz. 2019;6(3):72. 10.3390/medicines6030072
20. Sastre J, Dávila I. Dupilumab: A new paradigm for the treatment of allergic diseases. J Investig Allergol Clin Immunol. 2018;28(3):139–50. 10.18176/jiaci.0254
21. Castagnoli R, De Filippo M, Votto M, Marseglia A, Montagna L, Marseglia GL, et al. An update on biological therapies for pediatric allergic diseases. Minerva Pediatr. 2020;72(5): 364–71. 10.23736/S0026-4946.20.05993-9
22. Simpson EL, Paller AS, Siegfried EC, Boguniewicz M, Sher L, Gooderham MJ, et al. Efficacy and safety of dupilumab in adolescents with uncontrolled moderate to severe atopic dermatitis: A phase 3 randomized clinical trial. JAMA Dermatol. 2020;156(1):44–56. 10.1001/jamadermatol.2019.3336
23. Regeneron Pharmaceuticals. A randomized, double-blind, placebo-controlled study to investigate the efficacy and safety of dupilumab administered concomitantly with topical corticosteroids in patients, ≥6 years to ˂12 years of age, with severe atopic dermatitis [Internet]. clinicaltrials.gov; 2020 Jul [cited 2022 Dec 29]. Report No.: NCT03345914. Available from: https://clinicaltrials.gov/ct2/show/NCT03345914
24. Cork MJ, Thaçi D, Eichenfield LF, Arkwright PD, Hultsch T, Davis JD, et al. Dupilumab in adolescents with uncontrolled moderate-to-severe atopic dermatitis: Results from a phase IIa open-label trial and subsequent phase III open-label extension. Br J Dermatol. 2020;182(1):85–96. 10.1111/bjd.18476
25. Guo Y, Cai Y. Immune mechanism and clinical research progress in the treatment of atopic dermatitis with dupilumab. China J Lepr Skin Dis. 2018;34(2):125–8.
26. dupixent_fpi.pdf [Internet]. [cited 2022 Dec 30]. Available from: https://www.regeneron.com/downloads/dupixent_fpi.pdf
27. Johnson BB, Franco AI, Beck LA, Prezzano JC. Treatment-resistant atopic dermatitis: Challenges and solutions. Clin Cosmet Investig Dermatol. 2019;12:181–92. 10.2147/CCID.S163814
28. Kim YJ, Lee MY, Won CH. Acral erythema arising in patients with atopic dermatitis after dupilumab therapy: A case report of 3 patients. Asia Pac Allergy. 2022;12(1):e1. 10.5415/apallergy.2022.12.e1