
Download
ORIGINAL ARTICLE
The importance of aeroallergen sensitivity in children with cystic fibrosis
Özge Ataya*, Suna Asilsoyb, Seda Şirin Kösec, Gizem Atakulb, Serdar Alb, Özge Kangallı Boyacioğlub, Nevin Uzunerb, Özkan Karamanb
aDepartment of Pediatric Immunology and Allergy, Izmır Dr. Behcet Uz Children’s Hospital, İzmir, Turkey
bDepartment of Pediatric Immunology and Allergy, Faculty of Medicine, Dokuz Eylül University, İzmir, Turkey
cDeptartment of Pediatric Immunology and Allergy, Dr. Sami Ulus Child Disease Training and Research Hospital, Ankara, Turkey
Abstract
Background Cystic fibrosis (CF) is an inherited autosomal recessive disorder that causes chronic airway disease. In addition to genetic factors, environmental factors may affect the clinical phenotype of CF. In this study, the presence of aeroallergen sensitivity in our patients with CF and its effects on clinical findings are evaluated.
Methods In this study, patients included were diagnosed with CF and followed in the Pediatric Respiratory and Allergy Clinic of the Faculty of Medicine, Dokuz Eylul University, Izmir, Turkey. Demographic characteristics, clinical and laboratory findings, skin prick test (SPT) results, and modified Shwachman–Kulczycki (MSK) scores of the patients were evaluated.
Results We evaluated 51 patients with CF with a median age of 10 (6–18) years. The mean MSK score of the patients was 72.54±11.50, and the mean predictive value of forced expiratory volume (FEV1) in the initial (1st) second was 80.43±19.50. According to SPT, aeroallergen sensitivity was detected in 17 (33.3%) patients. The prevalence of bacterial colonization and bronchiectasis was higher, and MSK scores were lower in Aspergillus fumigatus (AF)-sensitive patients (P ≤ 0.01). However, no similar difference was found in other allergen sensitivities. MSK scores (P = 0.001) and predictive FEV1 values (P = 0.005) of 25 (49%) patients with bacterial colonization were significantly lower than those without colonization.
Conclusion Aeroallergen sensitivity was detected in approximately one-third of CF patients. Although it has been emphasized in studies that environmental factors may have an impact on lung functions and clinical conditions in CF, the effect of allergens other than AF sensitivity may be less important compared to other environmental factors, such as the presence of bacterial colonization.
Key words: Aspergillus fumigatus, asthma, atopy, children, cystic fibrosis
*Corresponding author: Özge Atay, MD, Department of Pediatric Immunology and Allergy, Izmır Dr. Behcet Uz Children’s Hospital, İzmir, Turkey. Email address: [email protected]
Received 25 August 2022; Accepted 1 November 2022; Available online 22 November 2022
Copyright: Atay Ö, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Cystic fibrosis (CF) is an autosomal recessive inherited disease that may damage the lungs caused by a mutation in the cystic fibrosis transmembrane conductance regulator (CFTR) gene.1 Another prevalent chronic childhood lung disease is asthma.2 The fact that clinical manifestations in patients with asthma and CF are similar, this may be associated with difficulties in differential diagnosis and treatment.3–5 It was reported for both the diseases that genetic factors and environmental factors, including infections and allergens, affected the lung functioning of the patients.3,6 Relevant studies suggested that in CF, allergens may invade the respiratory epithelium as a result of inflammation because of infections, allergic inflammation may cause the patients predisposed to colonization of pathogens, and CFTR gene mutations may turn individuals susceptible to atopy.3,7 The most commonly reported allergen susceptibility among CF patients was associated with mold, and especially Aspergillus fumigatus (AF). AF may induce an allergic reaction, including allergic bronchopulmonary aspergillosis (ABPA).8 Owing to difficulties in differential diagnosis concerning asthma and/or special conditions, including comorbid ABPA, the asthma-specific treatments, such as corticosteroids, can be used in patients with CF.3–5
Allergen susceptibility and the prevalence of allergic diseases are increasing across the world.9 Nevertheless, there are only a limited number of studies that have investigated allergen susceptibility in patients with CF. Furthermore, the previous studies provided inconsistent reports regarding relationships between atopy and lung functioning.6,10 Accordingly, this study aimed to investigate the prevalence of aeroallergen susceptibility in patients with a CF diagnosis followed up in our clinic, and to investigate the relationship between atopy and CF by examining clinical and laboratory findings in susceptible patients.
Methods
A retrospective chart review was performed of the patients who met the diagnostic criteria for CF and followed up in the Pediatric Respiratory and Allergy Department of Dokuz Eylül University Hospital, Turkey between June 2019 and July 2020.11 Patients aged between 6 and 18 years, who attended to the control examinations for at least four times annually, are diagnosed with CF, and underwent a skin prick test (SPT), were included in the study.
The above SPT included pollens (grasses, Artemisia vulgaris, Alnus glutinosa, Populus alba, betula [birch], Fagus silvatica, Parietaria officinalis, and Olea europaea); house dust mites (Dermatophagoides pteronysinus, and Dermatophagoides farinae); animal epithelium (Felis domesticus, Canis familiaris, and Blatella germanica); fungi (Alternaria alternata, Cladosporium herbarum, and Aspergillus fumigatus), and commercial extracts ALK-Abello® (Hørsholm, Denmark). An induration diameter of 3 mm or above was considered positive for the purpose of SPT.
The demographic characteristics, CFTR gene mutations, medications in use, total immunoglobulin E (IgE), and blood eosinophil levels were retrieved from the file records of the patients. An eosinophil level of ≥470/µL was considered eosinophilia whereas a total IgE of ≥77.7 IU/mL was considered high.12,13
The modified Shwachman–Kulczycki (MSK) score was used to rate the general activity, physical examination, nutritional status, and radiological findings of the patients based on a 0–25-point scale for each of the subdomains.14,15 Accordingly, based on the disease severity group, the patients were classified as excellent (86–100), good (71–85), average (56–70), poor (41–55), and severe (<40). The patients were divided into two groups, including those with an MSK score of >70 and those with an MSK score of ≤70, both of which were simultaneously rated with SPT.
The spirometry analysis results of the patients, including the forced expiratory volume in 1 s (FEV1) predicted values, forced vital capacity (FVC) values, and FEV1:FVC ratio during their latest presentation, were recorded. Spirometry reference values were based on the Third National Health and Nutrition Examination Survey (NHANES III), and results of Hankinson et al. and Wang et al.16,17 We performed spirometry pre- and post-bronchodilator tests to examine reversibility.
Oropharyngeal swab and sputum culture samples collected from the patients were examined. Chronic infection was investigated for the most common microorganisms, such as Pseudomonas aeruginosa (PA), Staphylococcus aureus (SA), Burkholderia cepacia complex (BCC), Atypical mycobacteria (Amb), Aspergillus fumigatus, Stenotrophomonas maltophilia (SM), Escherichia coli (EC), Haemophilus influenzae (HI), and Klebsiella pneumoniae (KP). If the same microorganism was detected in two or more samples in at least four samplings conducted during the last year, this was considered a chronic infection of the microorganism.18
Patients were divided into classes based on the estimated mutation effect on CFTR functioning.19 The “minimal” function was defined as the existence of class I, II, or III mutations, while the “residual” function was defined as the existence of at least one mutation from class IV or V. In case of at least one unknown mutation in patients, these were classified as unclassified genotypes.
Diagnosis for ABPA was made pursuant to the criteria established by Agarwall et al.20
Allergic rhinitis (AR) was clinically diagnosed based on the presence of symptoms, including rhinorrhea, nasal congestion, nasal itching, and sneezing pursuant to the Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines.21
The patients were classified according to their body mass index (BMI) during their most recent presentation, as severely underweight (BMI < 16.5), underweight (BMI < 18.5), normal weight (BMI = 18.5–24.9) overweight (BM I≥ 25), and obese (BMI ≥ 30).22 Patients were divided into two groups, including patients with a BMI of <18.5 and ≥18.5 according to their respective BMI values.
Ethics Committee
The required ethics committee approval for this study was obtained from the Local Ethics Committee of the School of Medicine, Dokuz Eylül University (approval No.: 2020/21-28).
Statistical Analyses
The normality hypothesis was tested by Kolmogorov–Smirnov test to decide the statistical methods to be used. The nonparametric test methods were used in case any of the groups did not meet the assumption of normality. Accordingly, the Mann–Whitney U test or Student’s t-test was used for comparison of the variables obtained upon measurement in two independent groups whereas the Chi-square and Fisher exact tests were used for the analysis of the relationships between categorical variables or intergroup differences. Pearson correlation test analysis was used to investigate possible relationships between MSK scores, FEV1 predictive value, and age, and total IgE level, absolute eosinophil count (AEC), and BMI. Statistical analyses of the study were conducted using the IBM Statistical Package for the Social Sciences (SPSS) for Windows, version 25, and P ≤ 0.05 was considered statistically significant.
Results
Of the 51 patients, 27 (52.9%) included in this study were males with a median age of 10 years (min–max: 6–18 years) whereas the median age of CF diagnosis was 4 months (min–max: 1–55 months). Minimal function and residual function CFTR gene mutations were detected in 15 (29.4%) and 16 (31.4%) patients, respectively. Identified in 10 patients (19.6%), the Delta F508 mutation was the most prevalent gene mutation, and 25 (49%) patients had bacterial colonization. Spirometry analysis could not be performed in 10 patients because of compliance difficulties, respiratory distress, and reluctance. The FEV1 predicted value was ≥80% in 19 (46.34%), 60–80% in 16 (39.02%), and <60% in 6 (14.63%) patients out of 41 patients. Only 5 (12.19%) patients had early reversibility upon spirometry analysis. The MSK score regarding the severity of the disease was excellent in 7 (13.7%), good in 18 (35.3%), average in 20 (39.2%), and severe in 6 patients (11.8%). Regarding BMI, 20 (39.2%) patients were severely underweight, 16 (31.4%) were underweight, 12 (23.5%) were normal, and 3 (5.9%) were overweight. The first-degree relatives of 6 patients (11.8%) had a remarkable history of an atopic disease. Elevated total IgE and eosinophilia were discovered in 19 (37.3%) and 15 (29.4%) patients, respectively (Table 1).
Table 1 General characteristics of children with cystic fibrosis.
| Gender | P | Total | ||
|---|---|---|---|---|
| Female | Male | |||
| Age (years) Median (min–max) | 13 (6–18) | 14 (6–18) | 0.223 | 10 (6–18) |
| CFTR genotype classifications N (%) | 0.809 | |||
| Minimal function | 6 (11.76) | 9 (17.64) | 15 (29.41) | |
| Residual function | 8 (15.68) | 8 (15.68) | 16 (31.37) | |
| Unclassified | 10 (19.60) | 10 (19.60) | 20 (39.21) | |
| Bacterial colonization N (%) | 0.518 | |||
| Yes | 12 (23.52) | 13 (25.49) | 25 (49.01) | |
| No | 12 (23.52) | 14 (27.45) | 26 (50.98) | |
| Spirometry* Mean±SS | ||||
| FEV1 | 79.83±20.18 | 80.91±19.39 | 0.937 | 80.43±19.50 |
| FEV1/FVC | 100.22±11.30 | 96.60±7.84 | 0.453 | 98.19±9.56 |
| AEC Median (min–max) | 100 (100–800) | 350 (100–800) | 0.090 | 200 (100–800) |
| Total IgE Median (min–max) | 29.95 (2.11–1027) | 139 (8.10–1143) | 0.008 | 36.3 (2.11–1143) |
| Modified Shwachman–Kulczycki score Mean±SS | 67.50±10.46 | 74.78±10.60 | 0.376 | 72.54±11.50 |
| BMI Mean±SS | 17.18±2.97 | 18.34±3.41 | 0.136 | 17.47±3.09 |
*41 Patients were evaluated.
AEC: absolute eosinophil count; BMI: body mass index; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; CFTR: cystic fibrosis transmembrane conductance regulator genotype.
According to SPT results, 17 (33.3%) patients had allergen susceptibility. The most prevalent susceptibilities were identified against fungi 10 (19.6%), pollen 8 (15.7%), animals 5 (9.8%), and house dust mites 4 (7.8%). AF was the most prevalent allergen with a rate of 17.6% (N = 9). Three (5.9%) patients had ABPA.
Patients with allergen susceptibility, based on SPT results, had higher total IgE levels and higher prevalence of eosinophilia (P < 0.001 and 0.011, respectively). These patients more frequently used inhaled corticosteroids (ICs) and short-acting beta agonists (SABA) (P < 0.01). No difference was discovered between allergen susceptibility and CFTR genotype classifications, familial history of atopy, bacterial colonization, spirometry results, MSK scores, BMI, and bronchiectasis (P > 0.05). The patients susceptible to AF had higher total IgE levels and more prevalent eosinophilia (P = 0.001 and 0.030, respectively). The prevalence of bacterial colonization and bronchiectasis was higher, and MSK scores were lower (P = 0.010, 0.001, and 0.007, respectively). Similar differences were not identified in patients with pollen, house dust mite, and animal epithelial susceptibility (P < 0.05; Table 2).
Table 2 Demographic, clinical, and laboratory data of patients according to skin prick test (SPT) positivity and Aspergillus fumigatus (AF) sensitivity.
| SPT | AF | |||||
|---|---|---|---|---|---|---|
| Positive | Negative | P | Positive | Negative | P | |
| Age (years) Median (min–max) | 14 (8–18) | 13 (6–18) | 0.105 | 13 (6–16) | 9.5 (6–18) | 0.100 |
| Gender N (%) | ||||||
| Females | 5 (9.80) | 19 (37.25) | 0.074 | 3 (5.88) | 21 (41.17) | 0.473 |
| Males | 12 (23.52) | 15 (29.41) | 6 (11.76) | 21 (41.17) | ||
| CFTR genotype classifications N (%) | ||||||
| Minimal function | 6 (11.76) | 9 (17.64) | 3 (5.88) | 12 (23.52) | 0.920 | |
| residual function | 5 (9.80) | 11 (21.56) | 0.806 | 3 (5.88) | 13 (25.49) | |
| unclassified | 6 (11.76) | 14 (27.45) | 3 (5.88) | 17 (33.33) | ||
| Presence of bacterial colonization N (%) | 11 (21.56) | 14 (27.45) | 0.314 | 8 (15.68) | 17 (33.33) | 0.010 |
| Spirometry* Mean±SS | ||||||
| FEV1 | 80.80±22.17 | 80.23±18.25 | 0.930 | 83.25±22.51 | 79.75±19.02 | 0.655 |
| FEV1/FVC | 95.53±6.56 | 99.73±10.74 | 0.179 | 96.25±3.45 | 98.66±10.51 | 0.528 |
| AEC Median (min–max) |
500 (100–800) | 200 (100–800) | 0.011 | 400 (200–800) | 200 (100–800) | 0.030 |
| Total IgE Median (min–max) |
252 (21.10–1143) | 23.75 (2.11–316) | <0.001 | 445 (21.10–1143) | 27.4 (2.11–1030) | 0.001 |
| Presence of allergic rhinitis N (%) | 4 (7.84) | 6 (11.76) | 0.618 | 2 (3.92) | 8 (15.68) | 0.830 |
| Presence of bronchiectasis N (%) |
9 (17.64) | 11 (21.56) | 0.156 | 8 (15.68) | 12 (23.52) | 0.001 |
| IC treatment use N (%) | 12 (23.52) | 8 (15.68) | 0.001 | 7 (13.72) | 13 (25.49) | 0.013 |
| SABA treatment use N (%) |
16 (31.37) | 19 (37.25) | 0.006 | 9 (17.64) | 26 (50.98) | 0.023 |
| Modified Shwachman–Kulczycki score Mean±SS | 69.11±12.14 | 74.26±10.94 | 0.133 | 63.33±10.00 | 74.52±10.92 | 0.007 |
| BMI Mean±SS | 18.34±3.65 | 17.54±3.01 | 0.289 | 16.91±2.51 | 17.60±3.22 | 0.814 |
*41 Patients were evaluated.
AEC: absolute eosinophil count; CFTR: cystic fibrosis transmembrane conductance regulator genotype; BMI: body mass index; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; IC: inhaled corticosteroids; SABA: short acting beta agonist.
Ten (19.60%) patients had allergic rhinitis. No difference was discovered between the patients with and without allergic rhinitis by age (P = 0.526), gender (P = 0.835), CFTR genotype classifications (P = 0.364), MSK score (P = 0.298), FEV1 predicted value (P = 0.270), total IgE level (P = 0.286), and AEC (P = 0.116).
The most prevalent bacterial colonization cases include Pseudomonas aeruginosa in 17 (33.3%) patients and Staphylococcus aureus in 11 (21.6%) patients. These patients had significantly higher rate of bronchiectasis compared to noncolonized patients (P = 0.043 and 0.001, respectively). Patients colonized with PA had higher rates of positive SPT and AF susceptibility compared to the noncolonized patients (P = 0.036 and 0.004, respectively). However, there was no similar difference with Sa colonization (P = 1,000 and 0.385, respectively).
Moreover, no difference was established between the patients’ FEV1 predicted values, CFTR genotype classification, and positive SPT results (P > 0.05). Nevertheless, the FEV1 predicted value was lower in patients with bacterial colonization and comorbid bronchiectasis, without elevated total IgE, and with lower BMI (P < 0.05; Table 3).
Table 3 Differences in predictive values of FEV1 between groups.
| FEV1 (%)* | P | |
|---|---|---|
| Gender | ||
| Females | 79.83±20.18 | 0.863 |
| Males | 80.91±19.39 | |
| CFTR genotype classifications | 0.767 | |
| Minimal function | 77.73±20.85 | |
| Residual function | 80.33±13.72 | |
| Unclassified | 82.88±21.51 | |
| Bacterial colonization | ||
| Yes | 72.77±16.63 | 0.005 |
| No | 89.31±19.16 | |
| SPT | ||
| Positive | 80.80±22.17 | 0.930 |
| Negative | 80.23±18.25 | |
| Eosinophilia | ||
| Yes | 81.21±16.61 | 0.857 |
| No | 80.03±21.13 | |
| Total IgE | ||
| High | 89.00±18.85 | 0.023 |
| Normal | 74.96±18.20 | |
| Allergic rhinitis | ||
| Yes | 73.62±14.93 | 0.276 |
| No | 82.09±20.30 | |
| Presence of bronchiectasis | ||
| Yes | 73.61±19.99 | 0.046 |
| No | 85.78±17.73 | |
| IC treatment | ||
| Yes | 74.88±23.95 | 0.126 |
| No | 84.37±14.93 | |
| SABA treatment | ||
| Yes | 75.20±19.04 | 0.006 |
| No | 93.08±14.59 | |
| Modified Shwachman–Kulczycki score | ||
| ≤70 points | 72.27±18.41 | 0.003 |
| >70 points | 89.89±16.54 | |
| BMI | ||
| <18.5 | 73.34±17.52 | 0.007 |
| ≥18.5 | 89.50±18.50 | |
*41 Patients were evaluated.
AEC: absolute eosinophil count; CFTR: cystic fibrosis transmembrane conductance regulator genotype; BMI: body mass index; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; IC: inhaled corticosteroids; SABA: short-acting beta agonist; SPT, skin prick test.
No relationship was established between the patients’ CFTR genotype classifications and MSK scores, bacterial colonization, bronchiectasis, total IgE levels, AEC, and BMI values (P = 0.142, 0.259, 0.121, 0.424, 0.344, and 0.780, respectively). Bronchiectasis was more prevalent in patients with Delta F508 mutation (P = 0.026).
No correlation was determined between the MSK scores and positive SPT results (P = 0.133). Nevertheless, the MSK scores were lower in patients susceptible to AF compared to nonsusceptible patients (P = 0.007; Table 3). In addition, the MSK scores were significantly lower in patients with fungal susceptibility (P = 0.030). No similar differences were determined with susceptibility to pollen, house dust mite, and animal epithelium (P = 0.376, 0.682, and 0.793, respectively). The MSK scores were lower in patients with minimally function mutations, bronchiectasis, bacterial colonization, SABA use, and BMI of ≤18.5 (P < 0.05; Table 4).
Table 4 Differences in modified Shwachman–Kulczycki (MSK) scores between groups.
| MSK score | P | |
|---|---|---|
| Gender | ||
| Females | 71.45±12.28 | 0.529 |
| Males | 73.51±10.90 | |
| CFTR genotype classifications | 0.044 | |
| Minimal function | 77.73±20.85 | |
| Residual function | 80.33±13.72 | |
| Unclassified | 82.88±21.51 | |
| Bacterial colonization | ||
| Yes | 64.80±8.83 | <0.001 |
| No | 80.00±8.48 | |
| Eosinophilia | ||
| Yes | 72.00±10.65 | 0.828 |
| No | 72.77±11.97 | |
| Total IgE | ||
| High | 71.57±11.18 | 0.647 |
| Normal | 73.12±11.82 | |
| Allergic rhinitis | ||
| Yes | 76.00±12.64 | 0.295 |
| No | 71.70±11.21 | |
| Presence of bronchiectasis | ||
| Yes | 62.50±6.38 | <0.001 |
| No | 79.03 ± 9.16 | |
| IC treatment | ||
| Yes | 70.00±12.03 | 0.126 |
| No | 74.19±11.03 | |
| SABA treatment | ||
| Yes | 69.14±10.67 | 0.001 |
| No | 80.00±9.83 | |
| BMI | ||
| <18.5 | 69.84±11.94 | 0.028 |
| ≥18.5 | 77.10±9.32 |
BMI: body mass index; IC: inhaled corticosteroids; SABA: short-acting beta agonist; CFTR: cystic fibrosis transmembrane conductance regulator genotype.
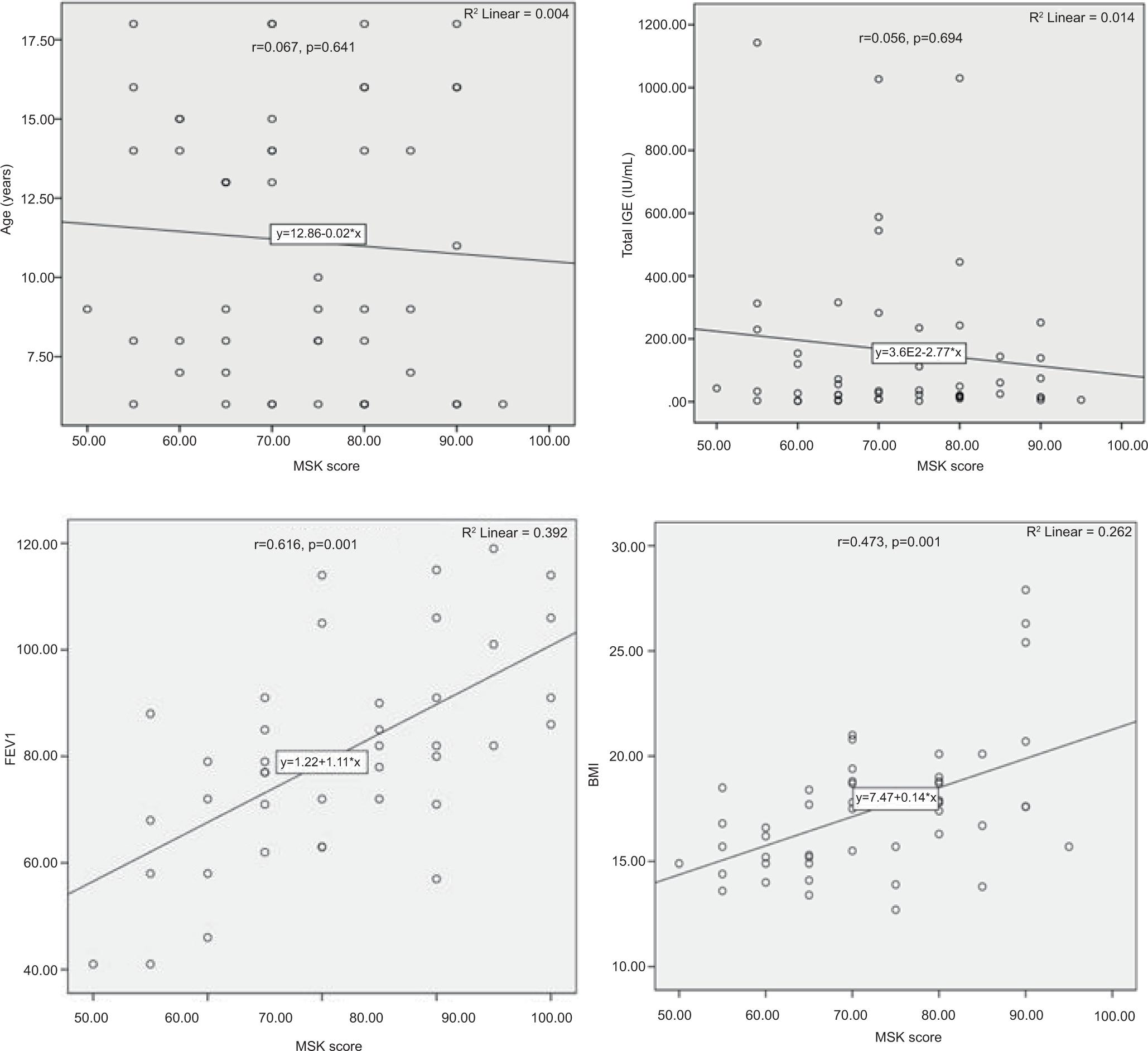
The MSK scores of patients were correlated moderately with the FEV1 predicted value and weakly with BMI values (r = 0.616 and P < 0.001; and r = 0.473 and P < 0.001, respectively). However, patients’ MSK scores were not correlated with age and total IgE levels (P > 0.05; Figure 1). The FEV1 predicted values were moderately correlated with BMI values (r = 0.528 and P < 0.001).
Figure 1 Scatter plots to evaluate correlation between patients’ MSK scores and FEV1 predictive value, BMI. MSK: Modified Shwachman–Kulczycki score; FEV1: forced expiratory volume in 1 s; BMI: body mass index; r: correlation coefficient; R2: determination coefficient.
All patients received Dornase alfa therapy, pancreatic enzyme replacement therapy, and supportive vitamin treatment. Furthermore, 35 (68.62%) patients were treated with SABA and 20 (39.21%) with ICs.
No difference was established between patients who had received and did not receive IC treatment (P = 0.150) by MSK score (P = 0.239), FEV1 predicted value (P = 0.161), and BMI (P = 0.740). Nevertheless, the total IgE level was higher (149 [min–max: 2.40–1143] vs. 21.1 [min–max: 2.11–1030], P = 0.002).
Positive SPT results were more prevalent in patients having IC treatment compared to those who did not have IC therapy (60% vs. 25%, P = 0.001). No difference was discovered between patients having IC treatment, with and without allergen susceptibility, regarding MSK score and FEV1 predicted value (P = 0.583 and 0.539, respectively).
Discussion
Only a limited number of studies focusing on environmental allergens were discovered, although the relevant literature has reported the importance of environmental factors on variability in lung functioning of the patients with CF.6,23 Previous studies suggested that the prevalence of atopy in patients with CF was similar to that in the general population.24,25 According to the phase-II study of the International Study of Asthma and Allergies in Childhood (ISAAC) conducted in Turkey, the prevalence of susceptibility to at least one aeroallergen was 8.8% in 2112 school-age children based on SPT results.26 In the present study, atopy was found out in 33.3% of our patients with CF. This is indicative of the fact that the allergen susceptibility in children with CF was higher compared to healthy children in the Turkish society. Furthermore, it was suggested that environmental factors were more important regarding the prevalence of atopy, compared to genetic differences.6 In the present study, no difference was marked between the presence of atopy and CFTR gene mutations.
The patients susceptible to allergens had higher total IgE levels, higher rate of eosinophilia, and higher rates of IC and SABA treatments. No difference was established for bacterial colonization, FEV1 predicted value, bronchiectasis, BMI, and MSK scores between SPT positive and negative groups. Nevertheless, the prevalence of bronchiectasis was higher and MSK scores were lower in patients susceptible to AF. Patients with PA colonization had a higher rate of positive SPT results, compared to noncolonized patients, with manifest AF susceptibility. Nevertheless, no difference was found by SA colonization. This could suggest that certain infectious agents were associated with atopy.
A study, which investigated 55 patients with CF in the adult population, associated the presence of atopy in CF with rhinitis symptoms.27 However, the present study did not identify any correlation between presence of atopy and allergic rhinitis. Based on the results of the study, we suggest that the effect of allergic rhinitis on CF clinical findings is not remarkable.
Susceptibility was determined to fungi (19.6%), followed by pollen (15.7%), while the most prevalent was the AF susceptibility. It was reported that 35% of children with CF had susceptibility to AF, 25% to grass pollen, and 13% to house dust mites.8 Relevant studies suggested an association between susceptibility to AF and severe lung diseases.1,3,6,28 ABPA is defined as a clinical picture that may result in chronic lung diseases because of a sudden hypersensitivity reaction to AF.20 It was reported that 31–59% of the patients with CF were susceptible to AF and approximately 1–10% of those patients had ABPA.1,3 In the present study, clinical findings suggested ABPA in three patients susceptible to AF. Susceptibility to fungi was discovered in one case and that to pollen in another case. Although we had a small number of patients, we considered that additional allergen susceptibility could affect the occurrence of ABPA. Relevant literature reported that atopy was an important risk factor for the occurrence of ABPA, and ABPA was more prevalent in SPT positive individuals with CF, who were susceptible to at least one aeroallergen other than AF.1,3
It was also reported that all pulmonary function parameters, including forced expiratory volume in 1 s (FEV1), were lower in patients with ABPA, infected with PA, and in atopic individuals with CF.5 Certain studies suggested that the effect of atopy on respiratory function was insignificant.25 In the present study, no significant difference was discovered between FEV1 predicted value and positive SPT results, eosinophilia, and IC treatment. Whereas, the FEV1 predictive value was significantly lower in patients with bacterial colonization, bronchiectasis, and lower BMI. Therefore, we considered that atopy had little effect on respiratory function in patients with CF. Nevertheless, the prevalence of bacterial colonization and bronchiectasis was higher and MSK scores were lower in our patients susceptible to AF. Therefore, we suggest that AF could be considered in patients with CF with severe clinical prognosis.
It is difficult to prove comorbid asthma in patients with CF. However, the term “CF asthma” was introduced for the patients with CF with airway obstruction attacks responsive to bronchodilators, personal atopy evidence, and eosinophilia. It was even suggested that the above definition represented a different phenotype.29,30 While certain studies argued that higher total IgE levels and eosinophilia might support the CF and asthma combination, other studies disagreed with this.3,25,31 The total IgE and eosinophil levels were higher in our atopic CF patients. Nevertheless, we were able to detect early reversibility in a very few patients by means of spirometry.
Relevant studies in the literature reported that 88.2% of the patients with CF used some sort of inhaled bronchodilator.29 The rate of ICs prescription was reported as 10% in France, 12% in Germany, and 36% in the United Kingdom.32 Although use of ICs is frequent in patients with CF, relevant studies found inconsistent results regarding the effects of IC treatment on FEV1.33–35 Although ICs have a potential to reduce inflammatory lung injury and have positive effects on symptomatic wheezing, data on the usefulness of ICs in CF are inconclusive. Some authors have considered it safe to withdraw IC therapy.36 The rate of use of ICs was 39.2% in our patients. The prevalence of positive SPT results was significantly higher in patients using ICs, compared to those who did not use ICs, and the total IgE levels were significantly higher as well. However, no difference was established by the FEV1 predicted value and MSK score. Similarly, no significant difference was discovered by FEV1 predicted value and MSK score between atopic and non-atopic groups using ICs. These data suggested that the presence of aeroallergen sensitivity does not constitute a sufficient indication for the use of ICs. Obviously, we believe that extensive studies are required to assess the effectiveness of and requirement for IC treatment in CF patients.
A Turkish study, which investigated 54 patients with CF, reported that the mean MSK scores of the patients aged between 6 and 22 years was 71±18.7 whereas the mean BMI was 17.8±3.57. Furthermore, it was demonstrated that a strong positive correlation existed between FEV1 value and MSK score (r = 0.778 and P < 0.01).15 Another study reported a weak correlation between the pulmonary function and BMI in children with CF (r = 0.52 and P < 0.001).37
The mean MSK score of our patients was 72.54±11.50 whereas the mean BMI was 17.47±3.09. The patients’ MSK scores were moderately correlated with FEV1 predicted values and weakly correlated with BMI values. Furthermore, the FEV1 predicted values were moderately correlated with BMI values.
Our study was based on the data collected from our clinic; the number of patients was limited and did not represent the total population of CF patients. In addition, the fact that some patients were on bronchodilator therapy was another limiting factor.
Conclusion
The importance of aeroallergens, which constitute an important risk factor for asthma and account for a different phenotype, is unclear as regards CF. Although the same may cause a new phenotype of CF, their effect on prognosis seems unremarkable, except for mold allergens. Nevertheless, the relationship between CF and atopy should be closely observed for the fact that atopy in patients with CF may mediate the occurrence of ABPA. Furthermore, individuals susceptible to AF should be closely monitored for bacterial colonization, bronchiectasis, ABPA, and poor clinical outcomes, regardless of other aeroallergens. Identification of the population in which the IC treatment is aimed to prevent pulmonary exacerbation in CF may prove to be effective, and may prevent unnecessary drug use. Extensive studies to investigate this topic would be useful.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to research, authorship, and/or publication of this article.
REFERENCES
1. Rosario NA, Riedi CA. Cystic fibrosis and atopy. Allergol Immunopathol. 2013;41(2):1379. 10.1016/j.aller.2012.07.007
2. Stern J, Pier J, Litonjua AA. Asthma epidemiology and risk factors. Semin Immunopathol. 2020;42(1):5–15. 10.1007/s00281-020-00785-1
3. Antunes J, Fernandes A, Miguel Borrego L, Leiria-Pinto P, Cavaco J. Cystic fibrosis, atopy, asthma and ABPA. Allergol Immunopathol. 2010;38:278–84. 10.1016/j.aller.2010.06.002
4. Brand PLP. Bronchodilators in cystic fibrosis. J Soc Med. 2000;93(38):37–9.
5. Janahi IA, Rehman A, Al-Naimi AR. Allergic bronchopulmonary aspergillosis in patients with cystic fibrosis. Ann Thorac Med. 2017;12(2):74–82. 10.4103/atm.ATM_231_16
6. Collaco JM, Morrow CB, Green DM, Cutting GR, Mogayzel PJ Jr. Environmental allergies and respiratory morbidities in cystic fibrosis. Pediatr Pulmonol. 2013;48(9):857–64. 10.1002/ppul.22700
7. Warner JO, Kilburn SA. Cystic fibrosis and allergy. Pediatr Allergy Immunol. 1996;7(9):67–9. 10.1111/j.1399-3038.1996.tb00399.x
8. Silverman M, Hobbs FD, Gordon IR, Carswell F. Cystic fibrosis, atopy, and airways lability. Arch Dis Child. 1978;53(11):873–7. 10.1136/adc.53.11.873
9. Moustaki M, Loukou I, Tsabouri S, Douros K. The role of sensitization to allergen in asthma prediction and prevention. Front Pediatr. 2017;5:166. 10.3389/fped.2017.00166
10. Pitcher-Wilmott RW, Levinsky RJ, Gordon I, Turner MW, Matthew DJ. Pseudomonas infection, allergy, and cystic fibrosis. Arch Dis Child. 1982;57(8):582–6. 10.1136/adc.57.8.582
11. Farrell PM, Rosenstein BJ, White TB, Accurso FJ, Castellani C, Cutting GR, et al. Cystic fibrosis foundation. Guidelines for diagnosis of cystic fibrosis in newborns through older adults: Cystic Fibrosis Foundation consensus report. J Pediatr. 2008;153(2):4–14. 10.1016/j.jpeds.2008.05.005
12. Just J, Deslandes-Boutmy E, Amat F, Desseaux K, Nemni A, Bourrat E, et al. Natural history of allergic sensitization in infants with early-onset atopic dermatitis: Results from ORCA Study. Pediatr Allergy Immunol. 2014;25(7):668–73. 10.1111/pai.12287
13. Tu YL, Chang SW, Tsai HJ, Chen LC, Lee WI, Hua MC, et al. PATCH study group. Total serum IgE in a population-based study of Asian children in Taiwan: Reference value and significance in the diagnosis of allergy. PLoS One. 2013;8(11):80996. 10.1371/journal.pone.0080996
14. Doershuk C, Mathews L, Tucker A. A five-year clinical evaluation for a therapeutic program for patients with cystic fibrosis. J Pediatr. 1964;65:677–93. 10.1016/S0022-3476(64)80152-9
15. Alishbayli G, Kilinc AA, Cokugras H. Evaluation of the health-related quality of life in Turkish cystic fibrosis patients. Pediatr Int. 2021;63(8):965–70. 10.1111/ped.14553
16. Wang X, Dockery DW, Wypij D, Gold DR, Speizer FE, Ware JH, et al. Pulmonary function growth velocity in children 6 to 18 years of age. Am Rev Respir Dis. 1993;148:1502–8. 10.1164/ajrccm/148.6_Pt_1.1502
17. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general US population. Am J Respir Crit Care Med. 1999;159:179–87. 10.1164/ajrccm.159.1.9712108
18. Royal Brompton and Harefield Hospitals Paediatric CF Team. Clinical guidelines: Care of children with cystic fibrosis. 8th ed., 2020. Available from: www.rbht.nhs.uk/childrencf.
19. Green DM, McDougal KE, Blackman SM, Sosnay PR, Henderson LB, Naughton KM, et al. Mutations that permit residual CFTR function delay acquisition of multiple respiratory pathogens in CF patients. Respir Res. 2010;11(1):140. 10.1186/1465-9921-11-140
20. Agarwal R, Sehgal IS, Dhooria S, Aggarwal AN. Developments in the diagnosis and treatment of allergic bronchopulmonary aspergillosis. Expert Rev Respir Med. 2016;10(12):1317–34. 10.1080/17476348.2016.1249853
21. Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. World Health Organization; GA(2)LEN; allergen. Allergic rhinitis and its impact on asthma (ARIA) 2008 update. Allergy. 2008;63(86):8–160. 10.1111/j.1398-9995.2007.01620.x
22. Weir CB, Jan A. BMI classification percentile and cut off points. 2021, May 9. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing, 2021.
23. Collaco JM, Blackman SM, McGready J, Naughton KM, Cutting GR. Quantification of the relative contribution of environmental and genetic factors to variation in cystic fibrosis lung function. J Pediatr. 2010;157(5):802–7. 10.1016/j.jpeds.2010.05.018
24. Wilmott RW. The relationship between atopy and cystic fibrosis. Clin Rev Allergy. 1991;9(1–2):29–46. 10.1007/BF02914533
25. Balfour-Lynn IM, Elborn JS. “CF asthma”: What is it and what do we do about it? Thorax. 2002;57(8):742–8. 10.1136/thorax.57.8.742
26. Karaman O, Turgut CS, Uzuner N, Olmez D, Babayigit A, Kose S, et al. The determination of asthma, rhinitis, eczema, and atopy prevalence in 9-to 11-year-old children in the city of Izmir. Allergy Asthma Proc. 2006;27(4):319–24. 10.2500/aap.2006.27.2877
27. Hallstrand TS, Calenoff E, Becker JW, Henderson WR Jr, Aitken ML. The role of allergy in manifestations of respiratory disease in adult cystic fibrosis. Ann Allergy Asthma Immunol. 2004;92:228–33. 10.1016/S1081-1206(10)61552-9
28. Nikolaizik WH, Moser M, Crameri R, Little S, Warner JO, Blaser K, et al. Identification of allergic bronchopulmonary aspergillosis incystic fibrosis patients by recombinant Aspergillus fumigatus I/a-specific serology. Am J Respir Crit Care Med. 1995;152: 634–9. 10.1164/ajrccm.152.2.7633719
29. Kent BD, Lane SJ, van Beek EJ, Dodd JD, Costello RW, Tiddens HA. Asthma and cystic fibrosis: A tangled web. Pediatr Pulmonol. 2014;49(3):205–13. 10.1002/ppul.22934
30. Pabary R. Severe pulmonary exacerbation in cystic fibrosis caused by cat allergy. Paediatr Respir Rev. 2014;15(1):29–31. 10.1016/j.prrv.2014.04.010
31. Sanchez I, Powell RE, Pasterkamp H. Wheezing and air flow obstruction during methacholine challenge in children with cystic fibrosis and in normal children. Am Rev Respir Dis. 1993;147:705–9. 10.1164/ajrccm/147.3.705
32. Koch C, McKenzie SG, Kaplowitz H, Hodson ME, Harms HK, Navarro J, et al. International practice patterns by age and severity of lung disease in cystic fibrosis: Data from the Epidemiologic Registry of Cystic Fibrosis (ERCF). Pediatr Pulmonol. 1997;24:147–54. 10.1002/(SICI)1099-0496(199708)24:2<147::AID-PPUL15>3.0.CO;2-2
33. Ren CL, Pasta DJ, Rasouliyan L, Wagener JS, Konstan MW, Morgan WJ, et al. Relationship between inhaled corticosteroid therapy and rate of lung function decline in children with cystic fibrosis. J Pediatr. 2008;153(6):746–51. 10.1016/j.jpeds.2008.07.010
34. Nikolaizik WH, Schoni MH. Effect of inhaled corticosteroids on lung function of cystic fibrosis patients—a prospective study. Eur Respir J. 1994;7:430S.
35. Levine H, Cohen-Cymberknoh M, Klein N, Hoshen M, Mussaffi H, Stafler P, et al. Reversible airway obstruction in cystic fibrosis: Common, but not associated with characteristics of asthma. J Cyst Fibros. 2016;15(5):652–9. 10.1016/j.jcf.2016.01.003
36. Balfour-Lynn IM, Welch K. Inhaled corticosteroids for cystic fibrosis. Cochrane Database Syst Rev. 2012;14(11):CD001915. 10.1002/14651858.CD001915.pub3
37. Calella P, Valerio G, Thomas M, McCabe H, Taylor J, Brodlie M, et al. Association between body composition and pulmonary function in children and young people with cystic fibrosis. Nutrition. 2018;48:73–6. 10.1016/j.nut.2017.10.026