
Download
ORIGINAL ARTICLE
Functional constipation related to cow’s milk allergy in children: A management proposal.
Mariannita Gelsomino, Ester Del Vescovo, Giulia Bersani, Stefano Miceli Sopo*
Pediatric Allergy Unit, Pediatrics Area, Department of Life Sciences and Public Health, Policlinico Gemelli Universitary Foundation IRCCS, Catholic University of Sacred Heart, Rome, Italy
Abstract
Functional constipation (FC) is one of the most common disorders in childhood and has a negative impact on the quality of life of children. Scientific evidence regarding a causal relationship between FC and cow’s milk allergy is controversial, as it is also reported by the latest European Society for Paediatric Gastroenterology, Hepatology and Nutrition-North American Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN–NASPGHAN) recommendations. In the case of FC, routine allergometric tests are not recommended and the cows’ milk-free diet is only proposed in the case of laxative-resistant constipation and only following the advice of an expert. Instead, after a careful review of the literature and in view of the many clinical cases encountered in our clinical practice, we believe that it is useful to propose cows’ milk-free diet as first line for the treatment of FC at least in pre-school children and in children with a personal or family history of atopy or with a previous diagnosis of cow’s milk protein allergy.
Key words: Atopy, children, cow’s milk allergy, elimination diet, functional constipation
*Corresponding author: Stefano Miceli Sopo. Allergy Unit, Pediatrics Area, Department of Woman and Child Health, Policlinico Gemelli Universitary Foundation IRCCS, Catholic University of Sacred Heart, Rome, Italy. Email address: [email protected], [email protected]
Received 11 November 2020; Accepted 11 December 2020 Available online 1 May 2021
Copyright: Gelsomino M, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
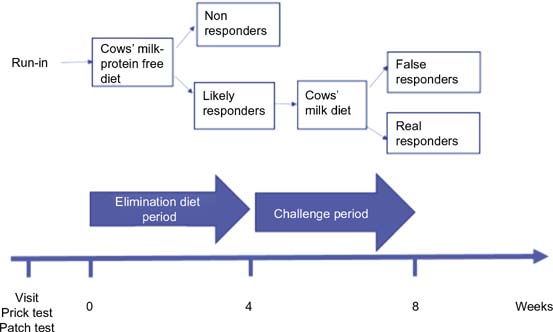
Functional constipation (FC) is a common problem in children, with a prevalence ranging from 0.5% to 32.2%, with a pooled prevalence of 9.5%.1,2 The ESPGHAN–NASPGHAN recommendations on FC3 report that the causal relationship between cow’s milk allergy (CMA) and FC is controversial. The authors do not recommend allergy tests for CMA in children with FC and suggest a 2–4 week attempt of cow’s milk (CM)-free diet only in unresponsive cases and following expert advice. However, our review of literature4 reports that, at least in childhood, the abovementioned causal relationship is fairly frequent, affecting 28%–78% of children with FC. With the help of three emblematic clinical cases, we propose here a simple protocol for the diagnosis of FC caused by CMA (Figure 1). The protocol is applicable to pediatric patients who meet the Rome IV criteria5,6 for the diagnosis of FC. In addition, patients undergo an anamnestic questionnaire to obtain information on current and previous personal atopic diseases, family history of atopy, and fecal appearance in the 4 weeks prior to the visit according to Bristol Stool Chart (BSC).7 At the first visit, skin prick test (SPT), for raw CM, casein, betalactoglobulin and lactalbumin commercial extracts, and atopy patch test (APT) for raw CM8 are performed. Patients started a CM-free diet lasting 4 weeks, with the exclusion of CM and its derivatives, without changing other food habits and lifestyle. At the end of this period, patients with persistent constipation, who still meet the Rome IV criteria,5,6 will be defined as “non responders” and they would go back to their normal diet. Meanwhile, patients who achieve normal bowel habits, who no longer meet the Rome IV criteria,5, 6 will be considered “likely responders.” The latter resume a free diet with daily intake of CM proteins up to a maximum period of 4 weeks (challenge period)9: telephone follow-up will be carried out and the challenge period will be interrupted as soon as the patient meets the Rome IV criteria again. Those who have maintained normalized stool habits after 4 weeks of free diet will be considered “false responders” (the patient doesn’t meet the Rome IV criteria after challenge period). While those who have showed the reappearance of constipation within 4 weeks of free diet will be defined as “real responders” (the patient meets the Rome IV criteria after challenge period) and will resume the CM-free diet for 1 year, at the end of which the possible acquisition of tolerance will be evaluated.
Figure 1 Protocol for diagnosis of FC related to CMA.
Case reports
In the first case report, A., a 9-year-old female child, came to our attention for FC, which arose from the age of 5. She had a history of asthma, urticaria, and allergic rhinoconjunctivitis well controlled with pharmacological therapy. When she was 1-year-old, she was diagnosed with CMA for the onset of skin rash after the introduction of CM, which regressed around the age of 2. In the last 8 weeks before the visit, the girl had evacuated <2 times per week with BSC type 3 stools,8 presenting painful defecation and numerous episodes of fecal incontinence, meeting Rome IV criteria6 for the diagnosis of FC. She had never taken laxative therapy before. Both SPT and APT were negative and a CM-free diet has been proposed. After 4 weeks, a normalization of stool habits was reported, with a bowel frequency of three evacuations per week (BSC type 3–4)7 and a less painful defecation. A. was therefore defined as a “likely responder,” and CM was reintroduced into her diet. At the end of a 4-week period, a worsening was reported, with <1 evacuation per week (BSC type 2).7 A. was considered a “real responder,” and continued the CM-free diet for 1 year, receiving soy milk as a substitute. At the end of this period, CM was attempted for 2 weeks, but the appearance of constipation was observed again, therefore A. resumed the diet of elimination with benefit. After a further 2 months, baked CM was introduced into her diet, without any change in her bowel habits (3–4 evacuations per week, BSC 4).7 After another 7 months, parmesan cheese and then pasteurized CM were introduced into her diet, and constipation no longer occurred. This “prudent” reintroduction of CM proteins into the diet was implemented by choice of the parents.
In the second case report, E., a 3-year-old male child was affected by constipation from the age of 5 months. He had got a history of atopic dermatitis well controlled with pharmacological therapy. In the last 2 months before our first visit, the child had evacuated stools corresponding to BSC type 17 and he met criteria 3 and 4 of Rome IV6 (i.e., retentive posture and hard and/or painful defecations), despite the regular use of polyethylene glycol with appropriate dosage and good compliance. SPT and APT were performed according to our protocol, with negative results. A CM-free diet has been proposed for 4 weeks. No clinical benefit was observed (<2 evacuations per week, retentive posture and hard and/or painful defecation with BSC type 1–2 stools),7 and it was necessary to resort to polyethylene glycol and to interrupt the diet at the end of the third week. E. is a case of a patient “non responder” to a CM-free diet.
In the third case report, D., a 9-year-old male child came to our attention for abdominal pain and constipation. He had a history of allergic rhinoconjunctivitis well controlled with pharmacological therapy. In the 2 months preceding our visit, the child had presented hard and/or painful defecations and large diameter stools at least once a week, meeting the definition of FC according to Rome IV criteria.5 In addition, the child evacuated BSC type 1–2 stools.7 SPT and APT were performed according to our protocol, with negative results. A CM-free diet has been proposed for 4 weeks. At the end of the period, an improvement of bowel habits was reported, with daily and painless evacuations of BSC type 3 stools.7 D. was considered a “likely responder” and therefore CM proteins were reintroduced into his diet. After 4 more weeks no reappearance of constipation was observed, D. continued to present daily evacuations of BSC type 3 stools.7 Therefore, the child was considered a “false responder.”
Discussion
The DRACMA guidelines on CMA10 report the CMA as a possible cause of constipation in childhood. In particular, the prevalence of constipation in children with CMA is 4.6%.11 The prevalence of CMA is higher among children with CF, ranging from 28% to 78%;4 the first 3 years of life seem to be the most affected age group.12 We believe that a CM protein-free diet can be proposed as first line of therapy at least to children with FC and atopy markers or personal/family history of atopic disease, especially if in preschool age, and not only to those with unresponsive constipation. The limitation of this therapeutic choice to children with atopy markers could be suggested by the results of the methodologically more robust study still available today on the association between CMA and FC. In fact, Iacono et al.13 reported that responders to the CM protein-free diet were significantly more likely to have serum CM-specific IgE positivity, and eosinophilic infiltration at the rectal biopsy. Other studies, however, have not found specific features between responders and non responders; and the children with a positive skin prick test were very few.14 In addition, Simeone et al.15 reported the prevalence of atopy in the constipated patients was not significantly different from control pediatric population (17.3% versus 18.8%). Therefore, the presence of atopy markers for the purposes of applying our protocol is not strictly prejudicial.
Potential conflict of interests related to the manuscript content
The authors declare no conflicts of interest.
Funding
There is no declaration of any sources of funding for the research reported in the manuscript. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors’ contributions
Stefano Miceli Sopo conceived the design of the study. Mariannita Gelsomino drafted the article. Giulia Bersani and Ester Del Vescovo acquired the data and researched the scientific literature. Mariannita Gelsomino and Stefano Miceli Sopo analyzed and commented on it. All authors revised the article, and gave a final approval of the version to be published.
Declaration
The authors declare that the work described has not been published previously, that it is not under consideration for publication elsewhere, that its publication is approved by all authors and tacitly by the responsible authorities where the work was carried out; if accepted, it will not be published or e-published elsewhere in the same form, in English or in any other language, without the written consent of the copyright holder. Written and oral consents from the patients and their parents were obtained, and the study was approved by the local ethical committee.
REFERENCES
1. Koppen IJ, Vriesman MH, Saps M. Prevalence of functional defecation disorders in children: A systematic review and meta-analysis. J Pediatr. 2018;198:121–30.e6 10.1016/j.jpeds.2018.02.029
2. Kovacic K, Sood MR, Mugie S. A multicenter study on childhood constipation and fecal incontinence: Effects on quality of life. J Pediatr. 2015;166:1482–7. 10.1016/j.jpeds.2015.03.016
3. Tabbers MM, Di Lorenzo C, Berger M. E 169 European Society for Pediatric Gastroenterology, Hepatology, and Nutrition; North American Society for Pediatric Gastroenterology. Evaluation and treatment of functional constipation in infants and children: Evidence-based recommendations from ESPGHAN and NASPGHAN. J Pediatr Gastroenterol Nutr. 2014;58:258–74. 10.1097/mpg.0000000000000266
4. Miceli Sopo S, Arena R, Greco M. Constipation and cow’s milk allergy: A review of the literature. Int Arch Allergy Immunol. 2014;164(1):40–5. 10.1159/000362365
5. Hyams JS, Di Lorenzo C, Saps M. Functional disorders: Children and adolescents. Gastroenterology. 2016;150:1456–68. 10.1053/j.gastro.2016.02.015
6. Hyams JS, Milla PG, Benninga M. Childhood functional gastrointestinal disorders: Neonate/toddler. Gastroenterology. 2006;130:1519–26. 10.1053/j.gastro.2005.11.065
7. National Collaborating Centre for Women’s and Children’s Health (UK). Constipation in Children and Young People. Diagnosis and Management of Idiopathic Childhood Constipation in Primary and Secondary Care. NICE Clinical Guidelines, No. 99. London: RCOG Press; 2010. https://www.nice.org.uk/guidance/cg99.
8. Luo Y, Zhang GQ, Li ZY. The diagnostic value of APT for food allergy in children: A systematic review and meta-analysis. Pediatr Allergy Immunol. 2019;30:451–61. 10.1111/pai.13031
9. Irastorza I, Ibañez B , Delgado-Sanzonetti L. Cow’s-milk-free diet as a therapeutic option in childhood chronic constipation. Pediatr Gastroenterol Nutr. 2010 Aug;51(2):171–6. 10.1097/mpg.0b013e3181cd2653
10. Fiocchi A, Brozek J, Schünemann H. World Allergy Organization (WAO) special committee on food allergy. World Allergy Organ Diagn Immunol. 2010 Jul;21(Suppl 21):1–125. 10.1111/j.1399-3038.2010.01068.x
11. Yang QH, Zheng BS, Zhou SM. Clinical features of cow’s milk protein allergy in infants presenting mainly with gastrointestinal symptoms: An analysis of 280 cases. Zhongguo Dang Dai Er Ke Za Zhi. 2019;21:271–6. 10.7499/j.issn.1008-8830.2019.03.016
12. Kamer B, Dólka E, Pyziak K. Food allergy as a cause of constipation in children in the first three years of life–own observations. Med Wieku Rozwoj. 2011;15(2):157–61. 10.1097/00042737-200602000-00002
13. Iacono G, Cavataio F, Montalto G. Intolerance of cow’s milk and chronic constipation in children. N Engl J Med. 1998;339:1100–4. 10.1056/nejm199810153391602
14. Dehghani SM, Ahmadpour B, Haghighat M. The role of cow’s milk allergy in pediatric chronic constipation: A randomized clinical trial. Iran J Pediatr. 2012;22:468–74.
15. Simeone D, Miele E, Boccia G. Prevalence of atopy in children with chronic constipation. Arch Dis Child. 2008;93:1044–7. 10.1136/adc.2007.133512