
Download
ORIGINAL ARTICLE
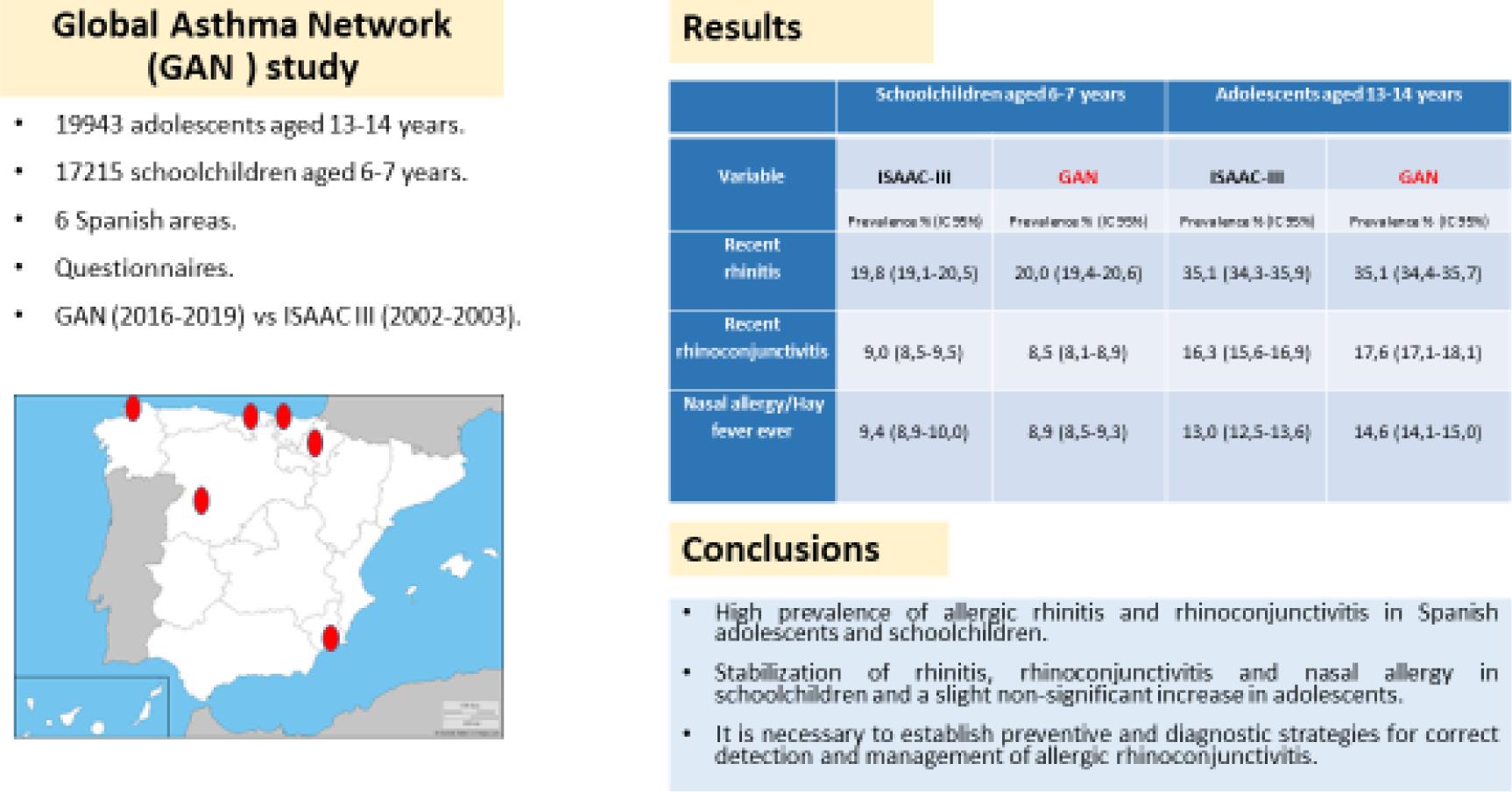
Prevalence and time trends of symptoms of allergic rhinitis and rhinoconjunctivitis in Spanish children: Global Asthma Network (GAN) study
Alberto Bercedo-Sanza*, Antonela Martínez-Torresb, Angel López-Silvarrey Varelac, Francisco Javier Pellegrini Belinchónd, Ines Aguinaga-Ontosoe,f, Carlos González Díazg, Luis García-Marcosh, Grupo GAN Spain#
aCentro de Salud Los Castros. Santander, Servicio Cántabro de Salud, Instituto de Investigación Sanitaria Valdecilla, IDIVAL, Cantabria, Spain
bUnidad de Neumología y Alergia Pediátrica y Grupo de Investigación en Enfermería, Hospital Infantil Universitario Virgen de la Arrixaca, Instituto Murciano de Investigación Biosanitaria IMIB, Murcia, Spain
cFundación María José Jove, Servicio Galego de Saúde (SERGAS), La Coruña, Spain
dCentro de Salud Pizarrales, Salamanca, Departamento de Ciencias Biomédicas y del Diagnóstico, Universidad de Salamanca, Salamanca, Spain
eDepartamento de Ciencias de la Salud, Universidad Pública de Navarra (UPNA), Pamplona, Spain
fIdiSNA, Instituto de Investigación Sanitaria de Navarra, Navarra, Spain.
gUnidad de Alergia Infantil, Hospital Universitario Basurto, Bilbao, Vizcaya, Spain
hUnidad de Neumología y Alergia Pediátrica Hospital Infantil Universitario Virgen de la Arrixaca, Universidad de Murcia e Instituto Murciano de Investigación Biosanitaria IMIB, Murcia, Spain
#List of members at the end of this article.
Abstract
Introduction: The time trends of the prevalence of rhinitis, rhinoconjunctivitis and nasal allergy previously described in the ISAAC (International Study of Asthma and Allergies in Childhood) in 2002 are unknown; or if the geographical or age differences in Spain persist.
Objective: To describe the prevalence of rhinitis, rhinoconjunctivitis and nasal allergy in different Spanish geographical areas and compare them with those of the ISAAC.
Methods: Cross-sectional study of the prevalence of rhinitis, rhinoconjunctivitis and nasal allergy, carried out in 2016-2019 on 19943 adolescents aged 13-14 years and 17215 schoolchildren aged 6-7 years from six Spanish areas (Cartagena, Bilbao, Cantabria, La Coruña, Pamplona, and Salamanca), through a questionnaire based on the Global Asthma Network (GAN) protocol.
Results: The prevalences of recent rhinitis and rhinoconjunctivitis (last 12 months), and nasal allergy/hay fever were 35.1%, 17.6%, and 14.6% in the adolescents and 20%, 8.5%, and 8.9% in the schoolchildren, respectively, with rhinoconjunctivitis in adolescents varying from 20.9% in Bilbao to 13.4% in Cartagena; and in schoolchildren, from 9.8% in La Coruña to 6.4% in Pamplona. These prevalences of rhinoconjunctivitis and nasal allergy in adolescents were higher than those described in the ISAAC (16.3% and 13%) and similar in schoolchildren to the ISAAC (9% and 9.4%).
Conclusions: There has been a stabilisation of rhinitis, rhinoconjunctivitis and nasal allergy in schoolchildren that slows the previous upward trend of ISAAC; and a slight non-significant increase in rhinoconjunctivitis and nasal allergy in adolescents. The variability found in adolescents would require local research to be better understood.
Key words: Rhinitis, Rhinoconjunctivitis, Adolescent, Schoolchild, Prevalence, Cross-sectional Studies, Global Asthma Network
*Corresponding author: Alberto Bercedo-Sanz, Centro de Salud Los Castros, Servicio Cántabro de Salud, Instituto de Investigación Sanitaria Valdecilla, IDIVAL, Avenida de Los Castros 145, 39012 Santander, Cantabria, Spain. Email address: [email protected]
Received 23 June 2022; Accepted 3 October 2022; Available online 1 September 2023
Copyright: Bercedo-Sanz A, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Allergic diseases in children and adolescents are a global public health problem, which involve considerable morbidity and geographical variations, as has been shown in the data published by the “International Study of Asthma and Allergies in Childhood” (ISAAC) (1992–2012).1–4 Whilst the prevalence of asthma, allergic rhinitis and atopic dermatitis symptoms increased at a worrying level in some centres, in other centres with already high prevalence they remained stable. The ISAAC study has offered a huge amount of epidemiological data, including the prevalence of rhinitis and allergic rhinoconjunctivitis and their risk and protective factors, from a large number of centres and countries worldwide and has demonstrated the importance of climate variations,5,6 environmental pollution,7 Mediterranean diet8–10 and obesity in allergic diseases.11 In recent years, the “Global Asthma Network” (GAN) has been set up with the aim of updating the prevalence of allergic diseases and their associated factors,12–14 with its first global estimation of asthma having already been published. These show the presence of wheezing in one of every 10 adolescents and schoolchildren,15 as well as the Spanish asthma data which confirm an increase in adolescents (15.3%) and a stabilisation in Spanish schoolchildren (10.4%) with respect to ISAAC-III 2002–2003 (10.6% and 9.9%, respectively).16–18
Despite rhinitis and allergic conjunctivitis being among the conditions that most frequently affect the paediatric population and which have a major clinical, economic and quality-of-life impact, epidemiological research about them is scant. The first data from the GAN network suggest that the worldwide prevalence of allergic rhinoconjunctivitis symptoms has stabilised with a slight decrease in the upward trend previously shown in the ISAAC study.19 In Spain, the latest prevalence data available in adolescents and schoolchildren correspond to ISAAC-III and are 31.2% and 17.1% for allergic rhinitis symptoms and 16.7% and 8.3% for allergic rhinoconjunctivitis in the past year, respectively.1,20,21 At present, the evolution of rhinitis and allergic rhinoconjunctivitis symptoms is not known. Also, not known is whether, as with bronchial asthma, a stabilisation of their prevalence in schoolchildren and an increase among adolescents has occurred, or if geographical differences exist within our country.
The GAN study in Spain consists of six centres: Murcia, Bilbao, Cantabria, La Coruña, Pamplona and Salamanca. The aim of the present study is to describe the prevalence of rhinitis and allergic rhinoconjunctivitis symptoms in those Spanish centres and compare the prevalence of those centres that took part in phase III of ISAAC (2002–2003) with those of the GAN study (2016–2019).
Material and Methods
This is a cross-sectional study that follows the methodology detailed in the specific manual for all GAN centres.12 This study is based on gathering information through standardised questionnaires that have been previously validated from a general sample that is estimated at 3000 participants in each age group (13–14 years and 6–7 years), which would enable to distinguish the prevalence of asthma that differ by 3% or more with a power of 90% and a 99% confidence level.13,14
The field work was carried out during the 2016–2019 school years, depending on the participating centres. Each principal researcher contacted the corresponding regional Education Department to obtain authorisation for the study in the primary and secondary schools selected and subsequently contacted the school heads, teachers and parents to explain the nature of the study. Pupils who were in second and third years of secondary school education (13–14 years) or in first and second years of primary school education (6–7 years) were selected from both public and private schools. A calendar of visits to the primary and secondary schools was charted out to supervise and advise on the handing out and collection of the written self-administered questionnaires for adolescents and the questionnaires for primary schoolchildren aged 6–7 years, which were filled in by their parents.
The fundamental instrument was the validated questionnaire, which included sections referring to allergic rhinitis symptoms, the seriousness of those symptoms and risk and/or protective factors. The questionnaire was translated from English to Spanish and back-translated from Spanish to English, as per the ISAAC method, to ensure that the sense of the items was not lost.22,23 Each participating centre followed the recommendations of the GAN study operating manual in relation to the selection of participating schools, the inclusion criteria, the specific variables and their coding. Sample sizes of at least 1000 and preferably 3000 were sought for each age group.12
The presence of recent allergic rhinitis in the past year was defined as a positive answer to the question: “In the past 12 months, have you (has this child) had a problem with sneezing, or a runny, or blocked nose when you (he/she) did not have a cold or the flu?” For recent rhinoconjunctivitis, the presence of recent allergic rhinitis was established by a positive answer to “In the past 12 months, has your (this child’s) nose problem been accompanied by itchy--watery eyes?” The variable of serious -rhinoconjunctivitis had to comply with the presence of recent rhinoconjunctivitis and a positive answer of “a lot” to the question “In the past 12 months, how much did your (this child’s) nose problem interfere with your (his/her) daily activities?” In the case of the presence of hay fever or nasal allergy, it was necessary to answer yes to the question “Have you (Has this child) ever had nasal allergy, including hay fever or rhinitis?”
The questionnaires were anonymised and read in the coordinating centre of Cartagena (Murcia) using a scanner (Fujitsu fi-7700) with OMR Remark Office© V10 mark recognition software (Gravic Inc. Malvern, PA, USA). A descriptive analysis of the variables was performed and subsequently a comparison was made using the chi-square test to calculate the possible differences found by sex among the participating centres. The prevalence was calculated with their 95% confidence intervals (95%CI) and were compared for each age group with those described in the centres that participated in the ISAAC study using the chi-square test. The statistical significance threshold was set at p ≤ 0.05. The STATA version 17 (College Station, TX, USA) software package was used for the said analysis.
The GAN study was approved in the national coordinating centre by the Ethics Committee for Clinical Research of the University Clinical Hospital “Virgen de la Arrixaca” in Murcia and subsequently validated and approved in each participating centre. Prior informed consent was obtained from the parents in the case of adolescents.
Results
The GAN study was carried out in six Spanish centres with a total sample size of 19,943 adolescents aged 13–14 years and 17,215 schoolchildren aged 6–7 years. One hundred and eighty-four secondary schools with adolescents and 323 primary schools with schoolchildren aged 6–7 years participated (Table 1). The participation rate was higher in adolescents, 81.3% (58.8%–95%), than in schoolchildren, 62.6% (55.2%–73.7%). This finding was similar to the rest of the GAN centres from other countries because the questionnaires of schoolchildren were completed by their parents at their homes.
Table 1 Characteristics of the participating GAN centres.
| GAN Centre | Population type | Participating schools n | Study population n | Sample size n | Participation (% pupils) |
|---|---|---|---|---|---|
| Bilbao | |||||
| 6–7 years | Urban | 52 | 4902 | 2707 | 55.2 |
| 13–14 years | 33 | 3711 | 3379 | 91.1 | |
| Cantabria | |||||
| 6–7 years | Urban | 75 | 5052 | 2841 | 56.2 |
| 13–14 years | 47 | 5664 | 4382 | 77.3 | |
| Cartagena | |||||
| 6–7 years | Urban | 61 | 5342 | 3509 | 65.7 |
| 13–14 years | 26 | 4657 | 3437 | 73.8 | |
| La Coruña | |||||
| 6–7 years | Urban | 48 | 4796 | 3407 | 71 |
| 13–14 years | 26 | 3760 | 3462 | 92.1 | |
| Pamplona | |||||
| 6–7 years | Urban | 36 | 4163 | 2363 | 56.8 |
| 13–14 years | 21 | 3056 | 1798 | 58.8 | |
| Salamanca | |||||
| 6–7 years | Mixed | 51 | 3242 | 2388 | 73.7 |
| 13–14 years | 31 | 3668 | 3485 | 95.0 | |
| Total | |||||
| 6–7 years | 323 | 27,497 | 17,215 | 62.6 | |
| 13–14 years | 184 | 24,516 | 19,943 | 81.3 |
Prevalence results
The prevalence obtained by means of the written questionnaire is given in Tables 2 and 3. The total prevalence of recent rhinitis and allergic rhinoconjunctivitis symptoms were 35.1% and 17.6% in adolescents, and 20% and 8.5% in the schoolchildren. For adolescents, the range was from 42.2% for recent rhinitis in La Coruña and 20.9% for recent rhinoconjunctivitis in Bilbao, to 25% and 13.4% in Cartagena, respectively. With respect to schoolchildren, there was less variation, with La Coruña having 23.8% for rhinitis and 9.8% for recent rhinoconjunctivitis in the upper limit, and Cartagena with 17% for recent rhinitis and Pamplona with 6.4% for recent rhinoconjunctivitis in the lower limit. In this age group, only Cartagena and Pamplona had recent rhinitis prevalence below 20%. On the other hand, the prevalence of nasal allergy (including hay fever or rhinitis) on occasions was relatively high, with 14.6% in adolescents and 8.9% in schoolchildren.
Table 2 Prevalence (%) of rhinitis symptoms in children.
| Centre | Sample size | Rhinitis ever | Recent rhinitis | Recent rhinitis and itching | Recent rhinocon-junctivitis | Recent rhinoconjunctivitis and daily activity limited | Nasal allergy/Hay fever ever | Physician-diagnosed nasal allergy/Hay fever | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Never | On occasions | Quite often | Very often | NA | ||||||||
| Bilbao | 2707 | 682 (25.2) |
556 (20.5) |
321 (11.9) |
239 (8.8) |
79 (33.1) |
113 (47.3) |
24 (10.0) |
15 (6.3) |
8 (3.4) |
239 (8.8) |
181 (6.7) |
| Cantabria | 2841 | 760 (26.8) |
574 (20.2) |
326 (11.5) |
243 (8.6) |
101 (41.6) |
100 (41.2) |
26 (10.7) |
12 (4.9) |
4 (1.7) |
246 (8.7) |
190 (6.7) |
| Cartagena | 3509 | 758 (21.6) |
595 (17.0) |
351 (10.0) |
268 (7.6) |
77 (28.7) |
132 (49.3) |
38 (14.2) |
13 (4.9) |
8 (3.0) |
233 (6.6) |
145 (4.1) |
| La Coruña | 3407 | 1000 (29.4) |
810 (23.8) |
443 (13.0) |
334 (9.8) |
106 (31.7) |
161 (48.2) |
50 (15.0) |
12 (3.6) |
5 (1.5) |
391 (11.5) |
310 (9.1) |
| Pamplona | 2363 | 513 (21.7) |
414 (17.5) |
218 (9.2) |
152 (6.4) |
38 (25.0) |
83 (54.6) |
25 (16.5) |
4 (2.6) |
2 (1.3) |
163 (6.9) |
119 (5.0) |
| Salamanca | 2388 | 609 (25.5) |
492 (20.6) |
257 (10.8) |
224 (9.4) |
82 (36.6) |
107 (47.8) |
25 (11.2) |
6 (2.7) |
4 (1.8) |
261 (10.9) |
198 (8.3) |
| Total | 17,215 | 4322 (25.1) |
3441 (20.0) |
1916 (11.1) |
1460 (8.5) |
483 (33.1) |
696 (47.7) |
188 (12.9) |
62 (4.3) |
31 (2.1) |
1533 (8.9) |
1143 (6.6) |
Written GAN questionnaire in schoolchildren aged 6–7 years.
*Prevalence expressed in absolute numbers and percentage in brackets. NA: no data available; GAN: Global Asthma Network.
Table 3 Prevalence (%) of rhinitis symptoms in adolescents.
| Centre | Sample size | Rhinitis ever | Recent rhinitis | Recent rhinitis and itching | Recent rhinocon-junctivitis | Recent rhinoconjunctivitis and daily activity limited | Nasal allergy/Hay fever ever | Physician-diagnosed nasal allergy/Hay fever | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Never | On occasions | Quite often | Very often | NA | ||||||||
| Bilbao | 3379 | 1628 (48.2) |
1303 (38.6) |
688 (20.4) |
705 (20.9) |
301 (42.7) |
265 (37.6) |
95 (13.5) |
39 (5.5) |
5 (0.7) |
526 (15.6) |
378 (11.2) |
| Cantabria | 4382 | 1861 (42.5) |
1436 (32.8) |
689 (15.7) |
697 (15.9) |
283 (40.6) |
282 (40.5) |
93 (13.3) |
34 (4.9) |
5 (0.7) |
586 (13.4) |
424 (9.7) |
| Cartagena | 3437 | 1191 (34.7) |
860 (25.0) |
443 (12.9) |
460 (13.4) |
193 (42.0) |
200 (43.5) |
47 (10.2) |
14 (3.0) |
6 (1.3) |
322 (9.4) |
227 (6.6) |
| La Coruña | 3462 | 1791 (51.7) |
1462 (42.2) |
664 (19.2) |
689 (19.9) |
301 (43.7) |
286 (41.5) |
68 (9.9) |
30 (4.4) |
4 (0.6) |
540 (15.6) |
408 (11.8) |
| Pamplona | 1798 | 821 (45.7) |
644 (35.8) |
327 (18.2) |
313 (17.4) |
129 (41.2) |
140 (44.7) |
31 (9.9) |
12 (3.8) |
1 (0.3) |
210 (11.7) |
149 (8.3) |
| Salamanca | 3485 | 1539 (44.2) |
1291 (37.0) |
675 (19.4) |
643 (18.5) |
251 (39.0) |
271 (42.2) |
75 (11.7) |
38 (5.9) |
8 (1.2) |
718 (20.6) |
489 (14.0) |
| Total | 19,943 | 8831 (44.3) |
6996 (35.1) |
3486 (17.5) |
3507 (17.6) |
1458 (41.6) |
1444 (41.2) |
409 (11.7) |
167 (4.8) |
29 (0.8) |
2902 (14.6) |
2075 (10.4) |
Written GAN questionnaire in adolescents aged 13–14 years.
*Prevalence expressed in absolute numbers and percentage in brackets. NA: no data available; GAN: Global Asthma Network.
Regarding the seriousness of allergic rhinoconjunctivitis, 4.8% of adolescents were afflicted (0.8% of the studied population) and 4.3% of schoolchildren (0.3% of the studied population) indicated that the rhinoconjunctivitis symptoms interfered in their daily activities to a great extent.
Comparison of the prevalence between ISAAC-III and GAN
A comparison of the prevalence of rhinitis symptoms in the past year from the ISAAC-III (2002–2003) and GAN (2016–2019) studies is presented in Table 4. A stabilisation of the total prevalence of recent rhinitis was observed in adolescents (35.1% ISAAC-III versus 35.1% GAN) and schoolchildren (19.8% ISAAC-III versus 20% GAN). However, in adolescents there was variability among the participating centres: whilst Bilbao and La Coruña presented a statistically significant increase, Cantabria, Cartagena and Pamplona showed lower prevalence. For schoolchildren, similar prevalence was shown for recent rhinitis in all the centres that participated in both studies.
Table 4 Comparison of the prevalence of allergic rhinitis symptoms in schoolchildren aged 6–7 years and adolescents aged 13–14 years in the ISAAC-III study versus the GAN study. *Written questionnaire.
| Variable | Centre | Schoolchildren aged 6–7 years | Adolescents aged 13–14 years | ||||
|---|---|---|---|---|---|---|---|
| ISAAC-III | GAN | Comparison p | ISAAC-III | GAN | Comparison p | ||
| Prevalence % (95%CI) n | Prevalence % (95%CI) n | Prevalence % (95%CI) n | Prevalence % (95%CI) n | ||||
| Recent rhinitis | Bilbao | 20.1 (18.7–21.6) 613 | 20.5 (19.0–22.1) 556 | 0.865 | 26.9 (25.3–28.6) 775 | 38.6 (36.9–40.2) 1303 | <0.001 |
| Cantabria | NA | 20.2 (18.7–21.7) 574 | NA | 44.0 (41.8–46.4) 799 | 32.8 (31.4–34.2) 1436 | <0.001 | |
| Cartagena | 17.1 (15.7–18.6) 467 | 17.0 (15.7–18.2) 595 | 0.966 | 31.4 (29.7–33.2) 898 | 25.0 (23.6–26.5) 860 | 0.003 | |
| La Coruña | 24.7 (23.2–26.3) 745 | 23.8 (22.4–25.2) 810 | 0.679 | 37.0 (35.2–38.7) 1102 | 42.2 (40.6–43.9) 1462 | 0.008 | |
| Pamplona | 17.1 (15.8–18.5) 544 | 17.5 (16.0–19.1) 414 | 0.871 | 39.4 (37.7–41.2) 1156 | 35.8 (33.6–38.1) 644 | 0.132 | |
| Salamanca | NA | 20.6 (19.0–22.3) 492 | NA | NA | 37.0 (35.4–38.7) 1291 | NA | |
| Total | 19.8 (19.1–20.5) 2369 | 20.0 (19.4–20.6) 3441 | 0.851 | 35.1 (34.3–35.9) 4730 | 35.1 (34.4–35.7) 6996 | 1.0 | |
| Recent rhinocon-junctivitis | Bilbao | 9.1 (8.1–10.2) 278 | 8.8 (7.8–10.0) 239 | 0.905 | 14.3 (13.0–15.6) 412 | 20.9 (19.5–22.3) 705 | 0.006 |
| Cantabria | NA | 8.6 (7.6–9.6) 243 | NA | 11.9 (10.4–13.4) 215 | 15.9 (14.8–17.0) 697 | 0.150 | |
| Cartagena | 8.8 (7.8–9.9) 240 | 7.6 (6.8–8.6) 268 | 0.622 | 16.8 (15.4–18.2) 480 | 13.4 (12.3–14.6) 460 | 0.146 | |
| La Coruña | 11.0 (9.9–12.2) 333 | 9.8 (8.8–10.9) 334 | 0.612 | 19.9 (18.5–21.4) 593 | 19.9 (18.6–21.3) 689 | 1.0 | |
| Pamplona | 7.0 (6.1–7.9) 222 | 6.4 (5.5–7.5) 152 | 0.820 | 16.7 (15.3–18.1) 489 | 17.4 (15.7–19.2) 313 | 0.797 | |
| Salamanca | NA | 9.4 (8.2–10.6) 224 | NA | NA | 18.5 (17.2–19.8) 643 | NA | |
| Total | 9.0 (8.5–9.5) 1073 | 8.5 (8.1–8.9) 1460 | 0.659 | 16.3 (15.6–16.9) 2189 | 17.6 (17.1–18.1) 3507 | 0.205 | |
| Nasal allergy/Hay fever ever | Bilbao | 8.9 (7.9–9.9) 270 | 8.8 (7.8–10.0) 239 | 0.968 | 15.7 (14.4–17.1) 453 | 15.6 (14.4–16.8) 526 | 0.966 |
| Cantabria | NA | 8.7 (7.7–9.8) 246 | NA | 16.5 (14.9–18.3) 300 | 13.4 (12.4–14.4) 586 | 0.061 | |
| Cartagena | 7.9 (6.9–9.0) 216 | 6.6 (5.8–7.5) 233 | 0.595 | 11.3 (10.1–12.5) 322 | 9.4 (8.4–10.4) 322 | 0.429 | |
| La Coruña | 12.6 (11.5–13.9) 381 | 11.5 (10.4–12.6) 391 | 0.639 | 15.4 (14.2–16.8) 460 | 15.6 (14.4–16.8) 540 | 0.931 | |
| Pamplona | 8.2 (7.3–9.2) 261 | 6.9 (5.9–8.0) 163 | 0.625 | 7.4 (6.5–8.4) 218 | 11.7 (10.2–13.3) 210 | 0.130 | |
| Salamanca | NA | 10.9 (9.7–12.3) 261 | NA | NA | 20.6 (19.3–22.0) 718 | NA | |
| Total | 9.4 (8.9–10.0) 1128 | 8.9 (8.5–9.3) 1533 | 0.658 | 13.0 (12.5–13.6) 1753 | 14.6 (14.1–15.0) 2902 | 0.127 | |
*Prevalence expressed in percentage, confidence interval 95% CI in brackets and absolute number. NA: no data available; GAN: Global Asthma Network; ISAAC: International Study of Asthma and Allergies in Childhood.
For recent rhinoconjunctivitis, a slight increase, albeit non-significant, in the total prevalence in adolescents (16.3% ISAAC-III versus 17.6% GAN) and a stabilisation in schoolchildren (9% ISAAC-III versus 8.5% GAN) was observed. Major variability was also detected in adolescents, with centres such as Bilbao and Cantabria having increased rhinoconjunctivitis prevalence, Cartagena with a lower prevalence and La Coruña and Pamplona showing no significant changes. In the case of schoolchildren, changes in the prevalence of rhinoconjunctivitis were not found in each centre between the two studies.
When the presence of nasal allergy (including hay fever or rhinitis) ever was compared between the two studies, a non-significant increase in its prevalence was observed in adolescents (13% ISAAC-III versus 14.6% GAN) and a stabilisation in schoolchildren (9.4% ISAAC-III versus 8.9% GAN). There was also variability between centres in adolescents: Cantabria presented a lower prevalence of nasal allergy in the GAN study, an increase in Pamplona and no change in Bilbao, Cartagena and La Coruña. Salamanca, the only centre that had not participated in ISAAC-III, contributed the highest prevalence of nasal allergy (20.6%).
Comparison of prevalence between sexes
With regard to the differences according to sex (Table 5), it was observed that the prevalence of recent rhinitis and rhinoconjunctivitis was higher in female adolescents in five of the GAN centres, whilst in schoolchildren the opposite was true, with the males having a higher prevalence of rhinoconjunctivitis in all the centres. This difference was greater in some of the GAN centres in comparison with the ISAAC-III study in the case of the prevalence of recent rhinoconjunctivitis.
Table 5 Comparison of the prevalence of rhinitis symptoms by sex in schoolchildren aged 6–7 years and in adolescents aged 13–14 years in the ISAAC-III study versus the GAN* study. Written questionnaire.
| Centre | Recent rhinitis | Recent rhinoconjunctivitis | Nasal allergy/Hay fever ever | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ISAAC-III | GAN | ISAAC-III | GAN | ISAAC III | GAN | |||||||
| Female | Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | Male | |
| Bilbao | ||||||||||||
| 6–7 years | 17.7 (15.8–19.7) |
22.7 (20.5–24.9) |
19.5 (17.4–21.7) |
21.5 (19.4–23.8) |
7.5 (6.2–8.9) |
10.9 (9.3–12.6) |
7.5 (6.1–9.0) |
10.2 (8.7–12.0) |
7.5 (6.2–8.9) |
10.4 (8.9–12.1) |
7.3 (6.0–8.9) |
10.4 (8.8–12.1) |
| 13–14 years | 28.8 (26.6–31.2) |
24.7 (22.4–27.0) |
41.7 (39.3–44.2) |
36.0 (33.6–38.4) |
15.9 (14.0–17.8) |
12.6 (10.9–14.5) |
24.2 (22.1–26.4) |
17.6 (15.8–19.5) |
15.2 (13.4–17.1) |
16.3 (14.3–18.3) |
16.2 (14.4–18.1) |
15.4 (13.7–17.3) |
| Cantabria | ||||||||||||
| 6–7 years | NA | NA | 18.5 (16.5–20.7) |
21.9 (19.8–24.2) |
NA | NA | 7.0 (5.7–8.5) |
10.1 (8.6–11.8) |
NA | NA | 7.1 (5.8–8.5) |
10.4 (8.8–12.1) |
| 13–14 years | 48.7 (45.4–52.0) |
39.2 (36.0–42.5) |
38.1 (36.1–40.2) |
26.8 (24.9–28.8) |
13.0 (10.9–15.4) |
10.6 (8.7–12.8) |
19.5 (17.8–21.2) |
12.1 (10.7–13.5) |
17.2 (14.9–19.8) |
15.8 (13.5–18.4) |
14.0 (12.6–15.6) |
12.8 (11.4–14.3) |
| Cartagena | ||||||||||||
| 6–7 years | 15.5 (13.7–17.6) |
18.8 (16.8–21.0) |
14.8 (13.2–16.6) |
19.1 (17.2–21.0) |
8.4 (7.0–10.0) |
9.3 (7.8–10.9) |
7.1 (5.9–8.4) |
8.2 (6.9–9.5) |
7.6 (6.2–9.1) |
8.3 (6.9–9.9) |
5.7 (4.6–6.8) |
7.6 (6.4–8.9) |
| 13–14 years | 36.0 (33.5–38.5) |
26.9 (24.6–29.3) |
27.8 (25.8–30.0) |
22.2 (20.2–24.3) |
19.0 (17.0–21.1) |
14.6 (12.8–16.5) |
15.8 (14.2–17.6) |
10.9 (9.4–12.5) |
11.3 (9.7–13.0) |
11.3 (9.7–13.1) |
10.2 (8.8–11.7) |
8.5 (7.2–9.9) |
| La Coruña | ||||||||||||
| 6–7 years | 21.0 (19.0–23.2) |
28.5 (26.2–30.9) |
21.4 (19.5–23.5) |
26.1 (24.1–28.3) |
9.5 (8.1–11.1) |
12.6 (11.0–14.4) |
9.4 (8.0–10.9) |
10.2 (8.8–11.8) |
11.8 (10.2–13.5) |
13.5 (11.8–15.4) |
10.1 (8.7–11.6) |
12.7 (11.2–14.4) |
| 13–14 years | 39.5 (36.9–42.1) |
34.6 (32.3–37.1) |
45.4 (43.0–47.8) |
39.1 (36.8–41.5) |
22.0 (19.8–24.2) |
18.0 (16.1–20.0) |
22.3 (20.3–24.3) |
17.5 (15.8–19.4) |
15.6 (13.7–17.5) |
15.3 (13.5–17.2) |
15.2 (13.5–17.0) |
16.2 (14.5–18.0) |
| Pamplona | ||||||||||||
| 6–7 years | 15.5 (13.7–17.4) |
18.8 (16.9–20.8) |
17.5 (15.4–19.8) |
17.5 (15.4–19.8) |
6.5 (5.4–7.9) |
7.4 (6.2–8.8) |
6.1 (4.8–7.7) |
6.7 (5.4–8.3) |
7.3 (6.1–8.7) |
9.1 (7.8–10.7) |
6.8 (5.4–8.5) |
7.0 (5.6–8.5) |
| 13–14 years | 42.2 (39.5–44.8) |
37.0 (34.6–39.5) |
34.8 (31.8–37.9) |
37.0 (33.7–40.4) |
19.2 (17.1–21.4) |
14.5 (12.8–16.3) |
16.5 (14.2–19.0) |
18.4 (15.9–21.2) |
7.1 (5.8–8.6) |
7.8 (6.5–9.2) |
12.3 (10.3–14.5) |
11.0 (8.9–13.3) |
| Salamanca | ||||||||||||
| 6–7 years | NA | NA | 18.9 (16.7–21.3) |
22.4 (20.0–24.9) |
NA | NA | 8.3 (6.8–10.0) |
10.5 (8.8–12.4) |
NA | NA | 9.5 (7.9–11.3) |
12.4 (10.6–14.4) |
| 13–14 years | NA | NA | 41.1 (38.7–43.4) |
32.7 (30.5–35.0) |
NA | NA | 22.6 (20.7–24.6) |
14.0 (12.4–15.7) |
NA | NA | 21.9 (20.0–23.9) |
19.5 (17.6–21.5) |
*Prevalence expressed in percentage and confidence interval 95%CI in brackets. NA: no data available; GAN: Global Asthma Network; ISAAC: International Study of Asthma and Allergies in Childhood.
Discussion
The results described and the comparisons between ISAAC-III and GAN show a stabilisation in the total prevalence of recent rhinitis and allergic rhinoconjunctivitis in schoolchildren, as well as a stabilisation of recent allergic rhinitis and a slight non-significant increase in rhinoconjunctivitis in adolescents. The increasing trend of rhinoconjunctivitis in both age groups previously shown in the ISAAC study throughout its different phases carried out from 1993 to 2003 in Spain20,21,24 is not globally confirmed in our study, suggesting a stabilisation in schoolchildren (8.5%) and a slight increase in adolescents (17.6%). The same data were observed when the presence of nasal allergy was analysed (hay fever or allergy rhinitis) ever, with a stabilisation in schoolchildren and a slight non-significant increase in adolescents.
On the other hand, great variability was observed for rhinitis and rhinoconjunctivitis in adolescents in each GAN centre and some differences among the prevalence of recent allergic rhinitis and nasal allergy (hay fever) in both age groups (35.1% versus 14.6% in adolescents and 20% versus 8.9% in schoolchildren, respectively), which were already seen in all phases of the ISAAC study. These data, together with the presence of physician-diagnosed nasal allergy (10.4% in adolescents and 6.6% in schoolchildren), require greater local research to be understood and for preventive health strategies to be established. It is possible that, among the factors responsible for this, apart from the geographical and climatic factors, there are also differences in the access to diagnostic tests in the primary care setting or in referral to specialised hospital services. This could contribute to an underdiagnosis of allergic rhinitis, as the data shown would seem to suggest.
Our study provides information on the local evolution of rhinitis, rhinoconjunctivitis and nasal allergy in Spain, with a trend similar to that of the evolution of asthma in the recently published Spanish GAN study.16 The Spanish study also confirmed an increase in asthma in adolescents and a stabilisation in schoolchildren. In the data referring to recent rhinitis and rhinoconjunctivitis and the presence of nasal allergy in each centre, there were no appreciable geographical variations between adolescents in coastal areas and inland areas, although there was a lower prevalence in Cartagena (25%, 13.4% and 9.4%, respectively) compared to the rest of the participating GAN centres (35.1%, 17.6% and 14.6%, respectively) and lower than in the ISAAC-III study.20 These differences can be explained by the fact that it is the only Mediterranean representative in the study and that it was related to the climate difference and the hours of exposure to the sun as protective factors.6 In schoolchildren, the centres of Cartagena and Pamplona stand out with lower prevalence than the rest of the GAN centres along the northern coast (Bilbao, Cantabria and La Coruña) and inland such as Salamanca. The GAN study on the evolution of asthma did not show clearly appreciable geographical variations either, although those areas that presented high prevalence in ISAAC continued to have high figures for asthma in the GAN study in adolescents, whilst in schoolchildren a geographical coast–inland pattern was observed.16
The first data from 25 countries in the GAN study (which includes only three Spanish centres that participated in both the ISAAC and GAN studies) refer to the prevalence of rhinoconjunctivitis, severe symptoms and hay fever in adolescents (13.3%, 0.8% and 15.2%, respectively) and in schoolchildren (7.7%, 0.6% and 11.1%, respectively), with a slight decrease in rhinoconjunctivitis, albeit not significant, in the 15 years separating ISAAC-III and GAN both in adolescents (−1.32% each 10 years) as well as in schoolchildren (−0.44% each 10 years). However, large variations existed in the trends observed among countries and among centres within each country so it is difficult to draw conclusions, although it is suggested that rhinoconjunctivitis may not increase further in schoolchildren, as is the case of the most complete data shown from six centres in Spain.19,25,26 With regard to the severity of the rhinoconjunctivitis, the results of our study are within the mean of the rest of the GAN centres in the world: approximately 5% of adolescents suffering from it had sufficiently serious symptoms so as to significantly interfere in their daily activities.
Comparison with other studies
In other studies performed in youngsters in Finland, it was shown that since 2000 there has been a deceleration in allergic rhinitis (10.7% in 2017), which could stabilise from 2020.27 In Poland, after monitoring 7- to 10-year-old children from 1993 to 2014, an increase in the prevalence of allergic rhinitis was observed until 2007 (15.9%) and stabilisation with a slight decrease in 2014 (13.9%).28 In the United States, the data from the National Health Survey detected a decrease in hay fever and respiratory allergy in the period 1997–2018 from 17.5% to 14.7% in people under the age of 18 years, with a prevalence of only hay fever described in 2018 at 7.2% reaching a peak of 10.5% in adolescents.29 Other countries, such as Turkey, showed an increased prevalence of physician-diagnosed allergic rhinitis in schoolchildren aged 6–14 years from 1994 to 2014.30 It is likely that the stabilisation of rhinitis and rhinoconjunctivitis in many geographical areas and countries, including the data from our study, could indicate that the maximum potential has been reached with regard to all those persons predisposed already suffering it, and this would explain the upward trends in other countries in which certain protective factors have also stopped acting and that other risk factors prevail more.
Comparison of prevalence of rhinoconjunctivitis between sexes
Our results also confirm the sex differences in the prevalence of rhinitis and allergic rhinoconjunctivitis: schoolboys and female adolescents are the most affected, as was the case in ISAAC-III, and in accordance with the asthma symptoms.16 This finding also agrees with other GAN centres where the trend in the prevalence of rhinitis and rhinoconjunctivitis change from primary school age to adolescence, when it is prevalent in females; whilst males are the most affected at primary school age.25,26 These sex differences are not clear enough, but it is postulated that oestrogens and progesterone would increase the inflammation of the airways mediated by TH2 and would interact with the allergy.31,32
Limitations and strengths of the study
Despite the broad representability of the paediatric population studied to avoid selection bias, the fact that some ISAAC centres did not participate in GAN may limit the time trend data. Other limitations are those inherent in a cross-sectional study, that is, it does not enable a cause–effect relationship to be established and the use of questionnaires may cause memory bias in parents, although by limiting the questions to the past year, this bias is minimised. With regard to the diagnosis of rhinitis and allergic rhinoconjunctivitis by means of questionnaires of compatible symptoms (and not by physician diagnosis), massive epidemiological studies cannot implement any better system to compare cities and countries, although this limitation must be taken into consideration.
Conclusions
In short, the Spanish GAN study confirms the stabilisation of rhinitis, allergic rhinoconjunctivitis and nasal allergy in schoolchildren that slows the upward trend shown in ISAAC with a slight non-significant increase in rhinoconjunctivitis and nasal allergy in adolescents, similar to those found for asthma. The variability found in adolescents in each GAN centre warrants further study to improve understanding. The results of the present study indicate the need to establish similar preventive and diagnostic strategies throughout the country to correctly detect and manage allergic rhino conjunctivitis (Figure 1).
Figure 1 Prevalence and time trends of symptoms of allergic rhinitis and rhinoconjunctivitis in Spanish children.Table 4 (Continued)
Acknowledgements
We would like to thank the regional education and health departments of the autonomous communities of the participating Spanish centres as well as the teaching staff in the primary and secondary schools and the parents and pupils without whose consent this study would not have been possible.
Funding sources
This study has been funded by Ayudas de investigación del Instituto de Investigación Sanitaria Valdecilla (IDIVAL) de Cantabria, PRIMVAL 17/01 y 18/01 (Cantabria centre); Ministerio de Economía y Competitividad, Instituto de Salud Carlos III: Proyectos de investigación en Salud PI17/00179 (Cartagena centre), PI17/00756 (Bilbao centre), PI17/00694 (Pamplona centre); Fundación María José Jove (La Coruña centre); Gerencia Regional de Salud de la Junta de Castilla y León (GRS 1239/b/16) and Sociedad Española de Inmunología Clínica, Alergología y Asma Pediátrica SEICAP (Salamanca centre).
Components of the Spanish GAN centres
GAN Centre Cartagena (national coordinator centre): L. García-Marcos, M. Sánchez-Solís, Unidad de Neumología y Alergia Pediátrica, Hospital Infantil Universitario Virgen de la Arrixaca, Universidad de Murcia. Instituto Murciano de Investigación Biosanitaria IMIB, Murcia, Spain. A. Martínez-Torres, Unidad de Neumología y Alergia Pediátrica y Grupo de Investigación en Enfermería, Hospital Infantil Universitario Virgen de la Arrixaca. Instituto Murciano de Investigación Biosanitaria IMIB, Murcia, Spain. V. Pérez-Fernández, E. Morales Bartolomé, Universidad de Murcia. Instituto Murciano de Investigación Biosanitaria IMIB, Murcia, Spain. J.J. Guillén-Pérez, J.F. Amoraga Bernal, J. Llamas Fernández y A. García Coy. Servicio de Salud Pública de Cartagena. Consejería de Salud de Murcia, Spain. GAN Centre Bilbao: C. González Díaz, A. González Hermosa, J. Rementeria Radigales. Servicio de Pediatría. Hospital Universitario Basurto, Bilbao. Vizcaya, Spain. GAN Centre Cantabria: A. Bercedo-Sanz, L. Lastra Martínez, R. Pardo Crespo. S. Peñil Sánchez. Servicio Cántabro de Salud. Instituto de Investigación Sanitaria Valdecilla. IDIVAL. Cantabria, Spain. GAN Centre La Coruña: A. López-Silvarrey Varela, Fundación María José Jove; Servicio Galego de Saúde (SERGAS), La Coruña, Spain. T.R. Pérez Castro, Grupo de Investigación Cardiovascular (GRINCAR); Epidemiología Cardiovascular, Atención Primaria y Enfermería (INIBIC); Facultad de Enfermería y Podología, Universidad de La Coruña, Spain. A. Otero Rodríguez, A. Garea Otero, A. Torrado Nogueira, J. Iglesias López, F.J. González Barcala. Servicio Galego de Saúde (SERGAS), La Coruña, Spain. R. Montero López, St. Josef Braunau Hospital, Braunau, Austria. GAN Centre Pamplona: I. Aguinaga-Ontoso, F. Guillén-Grima, E. Rayón-Valpuesta, J. Coque-Rubio, O. Alvarez-Flames, S. Sola-Cía, R. Saenz-Mendia, R. de la Rosa-Eduardo, R. García-Orellan, X. Elizalde Departamento de Ciencias de la Salud, Universidad Pública de Navarra (UPNA). Pamplona. Spain. IdiSNA. Instituto de Investigación Sanitaria de Navarra. S. Monje-Ortega, Hospital Santa Marina-Osakidetza. Bilbao, Vizcaya. GAN Centre Salamanca: J. Pellegrini Belinchón, Centro de Salud Pizarrales, Salamanca, Spain. Departamento de Ciencias Biomédicas y del Diagnóstico, Universidad de Salamanca, Spain. F. Lorente toledano. Departamento de Ciencias Biomédicas y del Diagnóstico, Universidad de Salamanca, Spain. S. Arriba-Méndez, Servicio de Pediatría, Hospital Universitario Salamanca e Instituto de Investigación Biomédica de Salamanca IBSAL, Spain. A. Marín-Cassinello, Departamento de Neumología y Alergología Pediátrica, Hospital General Universitario Santa Lucía, Cartagena, Murcia, Spain. M. Domínguez, Centro de Salud San Juan, Salamanca, Spain. MC. Sánchez–Jiménez, Centro de Salud Tejares, Salamanca y Universidad de Salamanca, Spain. M. M. López-González, Centro de Salud Pizarrales, Salamanca, Spain. M.C. Vega-Hernández, Departamento de Estadística, Universidad de Salamanca, Spain. M. Polo-De Dios. Centro de Salud Zamora Sur. Zamora, Spain.
REFERENCES
1. Asher MI, Montefort S, Björkstén B, Lai CKW, Strachan DP, Weiland SK, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross--sectional surveys. Lancet. 2006;368:733–743. 10.1016/S0140-6736(06)69283-0
2. Strachan D, Sibbald B, Weiland S, Aït-Khaled N, Anabwani G, Anderson HR, et al. Worldwide variations in prevalence of symptoms of allergic rhinoconjunctivitis in children: the International Study of asthma and Allergies in Childhood (ISAAC). Pediatr Allergy Immunol. 1997;8:161–176. 10.1111/j.1399-3038.1997.tb00156.x
3. Odhiambo JA, Williams HC, Clayton T, Robertson CF, Asher MI, and the ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124:1251–1258. 10.1016/j.jaci.2009.10.009
4. Mallol J, Crane J, von Mutius E, Odhiambo J, Keil U, Stewart A, et al. The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three: a global synthesis. Allergol Immunopathol (Madr). 2013;41:73–85. 10.1016/j.aller.2012.03.001
5. García-Marcos L, Batlles-Garrido J, Blanco-Quiros A, García Hernández G, Guillén-Grima F, González Díaz C, et al. Influence of two different geo-climatic zones on the prevalence and time trends of asthma symptoms among Spanish adolescents and schoolchildren. Int J Biometeorol. 2009;53:53–60. 10.1007/s00484-008-0190-3
6. Arnedo-Pena A, García-Marcos L, Bercedo-Sanz A, Aguinaga-Ontoso I, González-Díaz C, García-Merino A, et al. Prevalence of asthma symptoms in schoolchildren, and climate in west European countries: an ecologic study. Int J Biometeorol. 2013;57:775–784. 10.1007/s00484-012-0606-y
7. Arnedo-Pena A, García-Marcos L, Carvajal Urueña I, Busquets Monge R, Morales Suarez-Varela M, Miner Canflanca I, et al. [Air pollution and recent symptoms of asthma, allergic rhinitis, and atopic eczema in schoolchildren aged between 6 and 7 years]. Arch Bronconeumol. 2009;45:224–229. 10.1016/j.arbres.2008.10.004
8. García-Marcos L, Miner Canflanca I, Batllés Garrido JB, López-Silvarrey Varela A, García-Hernádez G, Guillén Grima F, et al. Relationship of asthma and rhinoconjunctivitis with obesity, exercise and Mediterranean diet in Spanish schoolchildren. Thorax. 2007;62:503–508. 10.1136/thx.2006.060020
9. Nagel G, Weinmayr G, Kleiner A, García-Marcos L, Strachan DP. Effect of diet on asthma and allergic sensitisation in the International Study on Allergies and Asthma in Childhood (ISAAC) Phase Two. Thorax. 2010;65:516–522. 10.1136/thx.2009.128256
10. Garcia-Marcos L, Castro-Rodriguez JA, Weinmayr G, Panagiotakos DB, Priftis KN, Nagel G. Influence of Mediterranean diet on asthma in children: a systematic review and meta-analysis. Pediatr Allergy Immunol. 2013;24:330–338. 10.1111/pai.12071
11. Mitchell EA, Beasley R, Bjorksten B, Crane J, García-Marcos L, Keil U, et al. The association between BMI, vigorous physical activity and television viewing and the risk of symptoms of asthma, rhinoconjunctivitis and eczema in children and adolescents: ISAAC Phase Three. Clin Exp Allergy. 2013;43: 73–84. 10.1111/cea.12024
12. The Global Asthma Network manual for global surveillance: prevalence, severity, management and risk factors. Available from: http://globalasthmanetwork.org/surveillance/manual/manual.php [cited 19 June 2022].
13. Ellwood P, Asher MI, Billo NE, Bissell K, Chiang CY, Ellwood EM, et al. The Global Asthma Network rationale and methods for Phase I global surveillance: prevalence, severity, management and risk factors. Eur Respir J. 2017;49:1601–1605. 10.1183/13993003.01605-2016
14. Ellwood P, Ellwood E, Rutter C, Perez-Fernandez V, Morales E, García-Marcos L, et al. Global Asthma Network Phase I surveillance: geographical coverage and response rates. J Clin Med. 2020;9:3688. 10.3390/jcm9113688
15. Asher MI, Rutter CE, Bissell K, Chiang CY, El Sony A, Ellwood E, et al. Worldwide trends in the burden of asthma symptoms in school-aged children: Global Asthma Network Phase I cross--sectional study. Lancet. 2021;398:1569–1580. 10.1016/S0140-6736(21)01450-1
16. Bercedo Sanz A, Martínez-Torres A, González Díaz C, López-Silvarrey Varela A, Pellegrini Belinchón FJ, Aguinaga-Ontoso I, et al. Prevalencia y evolución temporal de síntomas de asma en España. Estudio Global Asthma Network (GAN). An Pediatr (Bar). 2022;97(3):161–171. 10.1016/j.anpedi.2021.10.007
17. García-Marcos L, Blanco Quirós A, García Hernández G, Guillén-Grima F, González Díaz C, Carvajal Urueña I, et al. Stabilization of asthma prevalence among adolescents and increase among schoolchildren (ISAAC phases I and III) in Spain. Allergy. 2004;59:1301–1307. 10.1111/j.1398-9995.2004.00562.x
18. Carvajal-Urueña I, García-Marcos L, Busquets-Monge R, Morales Suarez-Varela M, García de Andoni N, Batles-Garrido J, et al. Geographic variation in the prevalence of symptoms in Spanish children and adolescents. International Study of Asthma and Allergies in Childhood (ISAAC) Phase 3, Spain. Arch Bronconeumol. 2005;41:659–666. 10.1016/S0300-2896(05)70721-3
19. Strachan DP, Rutter CE, Asher MI, Bissell K, Chiang CY, El Sony A, et al. Worldwide time trends in prevalence of symptoms of rhinoconjunctivitis in children: Global Asthma Network Phase I. Pediatr Allergy Immunol. 2022;33:e13656.
20. Arnedo-Pena A, García-Marcos L, Blanco-Quiros A, Martínez Gimeno A, Aguinaga Ontoso I, González Díaz C, et al. Evolución temporal de la prevalencia de síntomas de rinitis alérgica en escolares de 13.14 años de 8 áreas españolas entre 1993–1994 y 2001–2002 según el Estudio internacional sobre asma y Alergia en lainfancia (ISAAC). Med Clin (Barc). 2004;123(13):490–495. 10.1016/S0025-7753(04)74569-8
21. Arnedo-Pena A, García-Marcos L, García-Hernández G, Aguinaga Ontoso I, González Díaz C, Morales Suarez-Varela M, et al. Tendencia temporal y variaciones geográficas de la prevalencia de síntomas de rinitis alérgica en escolares de 6–7 años de ocho áreas españolas, según el ISAAC. An Pediatr (Barc). 2005;62(3):229–236. 10.1157/13071837
22. Ellwood P, Williams H, Ait-Khaled N, Bjorksten B, Robertson C, ISAAC Phase III Study Group. Translation of questions: the International Study of Asthma and Allergies in Childhood (ISAAC) experience. Int J Tuberc Lung Dis. 2009;13:1174–1182.
23. Instituto Murciano de Investigación Biosanitaria (IMIB). Investigación en Pediatría. Global Asthma Network. Available from: http://pediatria.imib.es/portal/instituto/pediatria_gan.jsf [cited 19 June 2022].
24. ISAAC Phase III Study Group Español. Prevalencia de síntomas sugestivos de rinitis alérgica y de dermatitis atópica en adolescentes (Estudio ISAAC España). An Esp Pediatr. 1999;51:369–376.
25. García-Marcos L, Innes Asher M, Pearce N, Ellwood E, Bissell K, Chiang CY, et al. The burden of asthma, hay fever and eczema in children in 25 countries: GAN Phase I study. Eur Respir J. 2022;60(3):2102866. 10.1183/13993003.02866-2021
26. García-Almaraz R, Reyes-Noriega N, Del-Río-Navarro BE, Berber A, Navarrete-Rodríguez EM, Ellwood P, et al. Prevalence and risk factors associated with allergic rhinitis in Mexican school children: Global Asthma Network Phase I. World Allergy Organ J. 2021;14(1):100492. 10.1016/j.waojou.2020.100492
27. Reijula J, Latvala J, Mäkelä M, Siitonen S, Saario M, Haahtela T. Long-term trends of asthma, allergic rhinitis and atopic eczema in young Finnish men: a retrospective analysis, 1926–2017. Eur Respir J. 2020;56:1902144. 10.1183/13993003.02144-2019
28. Brozek G, Lawson J, Szumilas D, Zejda J. Increasing prevalence of asthma, respiratory symptoms, and allergic diseases: four repeated surveys from 1993–2014. Respirar Med. 2015;109(8):982–990. 10.1016/j.rmed.2015.05.010
29. Centers for Disease Control and Prevention. Most recent national asthma data. Available from: https://www.cdc.gov/nchs/hus/contents2019.htm#Table-012 [cited 19 June 2022].
30. Doğruel D, Bingöl G, Altıntaş DU, Seydaoğlu G, Erkan A, Yılmaz M. The trend of change of allergic diseases over the years: three repeated surveys from 1994 to 2014. Int Arch Allergy Immunol. 2017;173(3):178–182. 10.1159/000477726
31. Fuseini H, Newcomb DC. Mechanisms driving gender differences in asthma. Curr Allergy Asthma Rep. 2017;17(3):19. 10.1007/s11882-017-0686-1
32. Wei JX, Ggerlich J, Genuneit J, Nowak D, Vogelberg C, von Mutius E, et al. Hormonal factors and incident asthma and allergic rhinitis during puberty in girls. Ann Allergy Asthma Immunol. 2015;115:21–27.e22. 10.1016/j.anai.2015.04.019