
Download
ORIGINAL ARTICLE
Mometasone furoate nasal spray in Italian children with seasonal allergic rhinitis: a comprehensive assessment
Cristiana Indolfia, Giulio Dinardoa, Giuseppina Rosaria Umanoa, Angela Klaina, Marcella Contieria, Alberto Decimoa, Fabio Decimoa, Giorgio Ciprandib*, Michele Miraglia Del Giudicea
aDepartment of Woman, Child and General and Specialized Surgery, University of Campania “Luigi Vanvitelli,” Naples, Italy
bAllergy Clinic, Casa di Cura Villa Montallegro, Genoa, Italy
Abstract
Objective: Seasonal allergic rhinitis (SAR) is a common disease of childhood and is characterized by type 2 inflammation, bothersome symptoms, and impaired quality of life (QoL). Intranasal corticosteroids are effective medications in managing SAR. In addition, mometasone furoate nasal spray (MFNS) is a well-known therapeutic option. However, the literature provided no data about the effects of MFNS in European children with SAR. Thus, this study addressed this unmet requirement.
Methods: MFNS was compared to isotonic saline. Both treatments were prescribed: one drop of spray per nostril, twice a day, for 3 weeks. Nasal cytology, total symptom score (TSS), visual analogic scale concerning the parental perception of severity of symptoms, and the Pediatric Rhinoconjunctivitis Quality of Life Questionnaire (PRQLQ) were assessed at baseline, after 7 and 21 days, and 1 month after discontinuation.
Results: MFNS significantly reduced eosinophil and mast cell counts, improved QoL, and relieved symptoms, as assessed by doctors and perceived by parents. These effects persisted over time, even after discontinuation. Both treatments were safe and well-tolerated.
Conclusions: The present study documented that a 3-week MFNS treatment was able to significantly dampen type 2 inflammation, improve QoL, and reduce severity of symptoms in Italian children with SAR, and was safe.
Key words: mometasone furoate nasal spray, nasal cytology, quality of life, seasonal allergic rhinitis, symptoms, type 2 inflammation
*Corresponding author: Giorgio Ciprandi, Allergy Clinic, Casa di Cura Villa Montallegro, Genoa, Italy. Email address: [email protected]
Received 4 April 2022; Accepted 9 May 2022; Available online 1 September 2022
Copyright: Ciprandi G, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Allergic rhinitis (AR) is a prevalent medical condition of childhood, as it may affect up to 30% of children worldwide.1 AR entails a type 2-driven inflammation, including eosinophilic and mast cell infiltration of the nasal mucosa.2 Type 2 inflammation sustains the appearance of symptoms; typical AR symptoms are itching, sneezing, watery rhinorrhoea, lacrimation, and congestion.3 Therefore, inflammation represents the target of therapeutical intervention.3 Moreover, children usually experience annoying symptoms so that their quality of life (QoL) is significantly altered.4
Conventionally, two main AR phenotypes exist, seasonal AR (SAR) and perennial AR (PAR), based on duration of symptoms and causal allergen. SAR recognizes pollen exposure as causal agent. SAR notably impairs nasal function and has bulky comorbidity.5,6
The management of SAR essentially includes intranasal corticosteroids and oral antihistamines.1 However, intranasal corticosteroids are more effective than antihistamines in controlling inflammatory events.7
In this regard, mometasone furoate nasal spray (MFNS) is currently one of the most used intranasal corticosteroids for patients with allergic rhinitis.8,9 There is considerable evidence that MFNS is effective and safe in managing patients with SAR.10,11 In addition, MFNS significantly reduces allergic inflammation consequent to allergen exposure.12 As a result, MFNS represents a valuable option for treating children with SAR.13 However, main clinical studies were performed in SAR children living in the United States. Thus, the clinical characteristics of these patients are different from that of the local ones. Therefore, the current study was designed to comprehensively evaluate impact of MFNS on nasal inflammation, symptoms, and QoL in a group of Italian children with SAR.
Materials and Methods
The present study recruited children suffering from SAR during the pollen season. They had a poor control of SAR despite antihistaminic treatment (cetirizine 2.5 mg, twice a day (bid), in preschoolers, or 5 mg, bid, in schoolers). Diagnosis of SAR was performed according to the validated criteria.14 Allergy was defined if history of nasal symptoms was consistent with documented sensitization.
Inclusion criteria were: age range 4–12 years, SAR diagnosis, total symptoms score (TSS) ≥ 6, and written informed consent of parents or legal guardians. Exclusion criteria were: perennial AR, rhinitis because of other reasons, concomitant acute or chronic rhinosinusitis, nasal polyps, asthma comorbidity, current use of topical or systemic corticosteroids, antihistamines, antileukotrienes, inadequate washout of them, nasal anatomic defect, respiratory infections in preceding 2 weeks, participation in other clinical studies in the previous month, documented hypersensitivity to the study product or its excipients, and trip planned outside the study area.
The study was conducted at a third-level pediatrics department located in Southern Italy. The study procedure was approved by the local Ethics Committee (Prt No. 408, 20/06/2019). The study was registered at clinicaltrials.gov (NCT05301647).
Children were randomly (ratio 1:1) subdivided into two groups: the active group was treated with MFNS (mometasone group) and the control group was treated with iso-tonic saline. For both groups, the schedule was instilling one drop of spray into each nostril (MFNS 50 mcg/spray), bid, for 21 days.
The participants were evaluated at baseline (T0), after 7 (T1) and 21 (T2) days, and at 30 days (T3) after discontinuation of treatment.
During the study, systemic or intranasal antihistamines, other corticosteroids, leukotriene antagonists, and sodium cromoglicate were prohibited.
The primary endpoint of this study was the change in eosinophilic infiltrate, assessed by nasal cytology, after the treatment. The secondary objectives were the nasal mast cell and neutrophil count, severity of symptoms, and changes in QoL during the study.
Nasal cytology is a well-defined methodology.15 The procedure included sampling, processing, and microscope reading. Sampling required collecting cells from the surface of the middle portion of the inferior turbinate by a sterile disposable curette. The procedure was performed under anterior rhinoscopy, with an appropriate light source, and it was painless. The sample obtained was immediately smeared on a glass slide, air-dried, and stained with MayGrünwald-Giemsa (MGG) for 30 min. Next, the stained sample was read under optical microscopy, with a 1000× objective with oil immersion. Slide reading was conducted blindly by an experienced cytologist, thus ensuring methodological correctness. The count of eosinophils, neutrophils, and mast cells was expressed as a mean value of 10 microscopic fields.
The validated Pediatric Rhinoconjunctivitis Quality of Life Questionnaire (PRQLQ) had 23 questions in five domains (nasal symptoms, ocular symptoms, practical issues, limitation of activities, and other symptoms) that were answered on a 7-point (0–6) scale, where 0 represents the absence of problems, and 6 the greatest symptom of distress.16 Children will complete the questionnaire together with a parent at baseline and during the study. A total score was calculated as a mean of five domains.
Total symptom score was the sum of the following three domains: (i) nasal symptoms (TNSS), included itching, sneezing, rhinorrhea, nasal congestion; (ii) ocular symptoms (TOSS): itching, hyperemia of the conjunctiva, tearing; and (iii) throat symptoms (TTSS): itching, coughing.17 With the help of their parents, patients scored severity of symptoms on a 4-point scale: 0 = absent or irrelevant, 1 = mild, 2 = moderate, and 3 = severe. Total symptom score was assessed at 12 h (TTS 12h) and 2 weeks (TTS 2W) before the visits. TSS represents the doctor’s point of view of severity of symptoms.
A visual analogic scale (VAS) measured the parental perception of severity of symptoms (0 = no symptom; 10 = very severe symptoms).
Safety was assessed as the incidence of adverse events for each treatment and physical examination.
Compliance was measured by counting the amount of sprays performed, as reported in a clinical diary.
Statistical analysis included different tests. Shapiro–Wilk test was performed to investigate distribution of continuous variables. Differences between active and control groups were tested with Mann–Whitney U test for independent samples. Longitudinal changes for continuous variables were investigated by the Wilcoxon signed-rank test for paired samples. Delta changes in questionnaire scores were calculated for each group as T1–T0 scores for the control group, and T2–T0 scores and T3–T0 scores for the mometasone group. Differences in delta changes between groups were investigated by Mann–Whitney U test. Chi-square test and Fisher’s exact test were performed for differences in categorical variables. P ≤ 0.05 was considered statistically significant. Data were expressed as median (interquartile range) or percentage, as appropriate. All analyses were performed with SAS® on Demand for Academics (SAS Institute Inc., Cary, NC)
Results
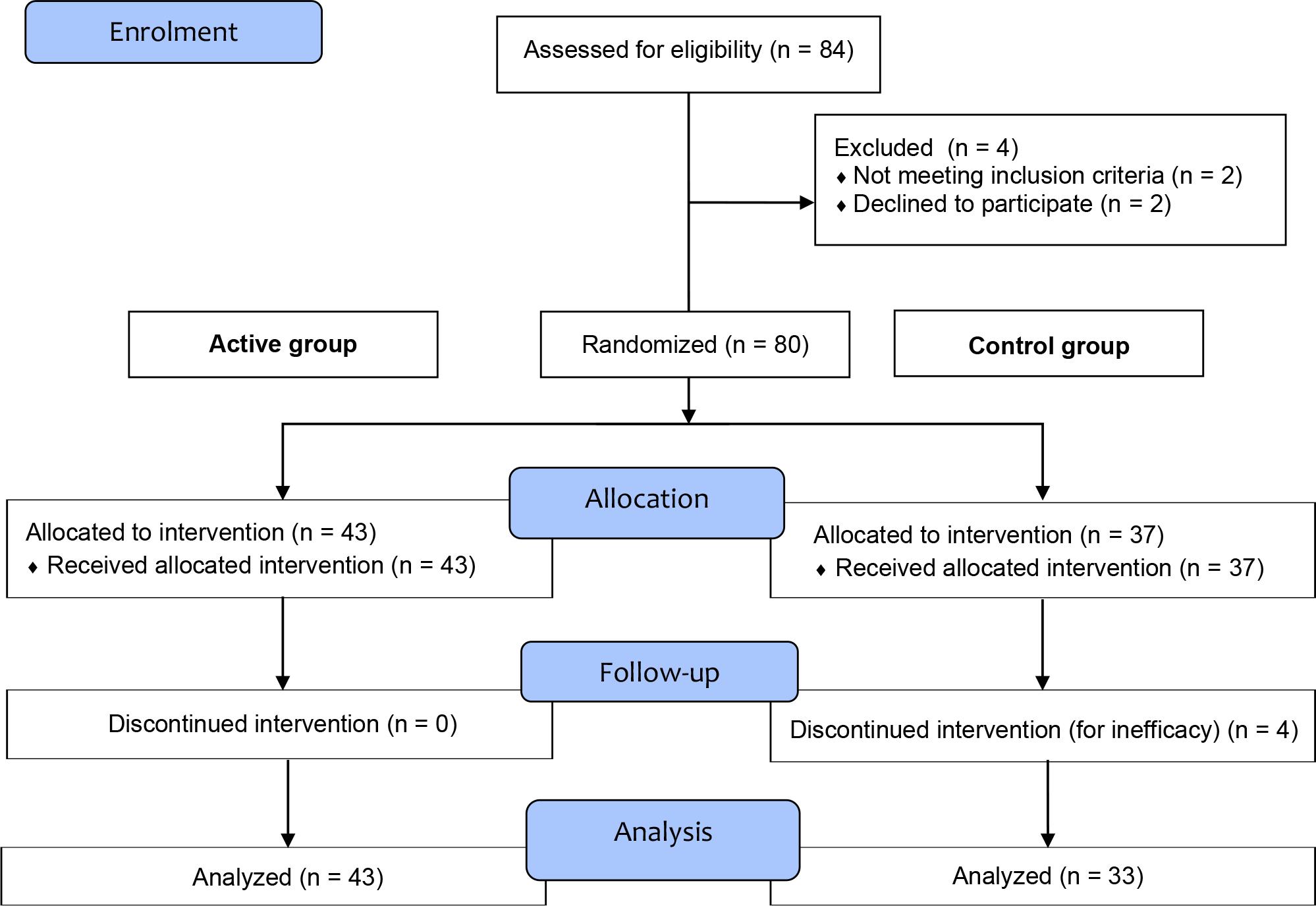
In all, 84 children were assessed for eligibility, 80 were randomized, but 76 (40 boys and 36 girls, mean age 11.4 ± 3.3 years) completed the study, and were analyzed. Four children in the control group were excluded as they discontinued the treatment because they were unsatisfied with the treatment. Therefore, the active group included 43 children and the control group had 33 children (Figure 1). The analysis was performed on the per-protocol population.
Figure 1 CONSORT 2010 flow diagram.
The compliance was good, as the proportion was 85%.
The cellular patterns, QoL scores, and severity of symptoms were superimposable in the two groups at baseline (Table 1).
Table 1 Demographics and clinical characteristics at baseline.
| Control group N = 33 | Active group N = 43 | P | |
|---|---|---|---|
| Age (years) | 11.2 ± 3.1 | 11.6 ± 3.5 | 0.81 |
| Gender Male Female |
18 15 |
22 21 |
0.89 |
| QoL score | 13.0 (10.0–15.0) | 15.0 (13.0–19.0) | 0.09 |
| Total VAS | 4.0 (2.5–5.0) | 4.0 (4.0–5.0) | 0.07 |
| Eosinophils (n) | 3 (0–10) | 0 (0–7) | 0.10 |
| Neutrophils (n) | 0 (0–10) | 5 (0–0) | 0.27 |
| Mast cells (n) | 0 (0–2) | 0 (0–0) | 0.53 |
QoL: quality of life; VAS: visual analogic scale.
Intergroup analysis
Nasal cytology
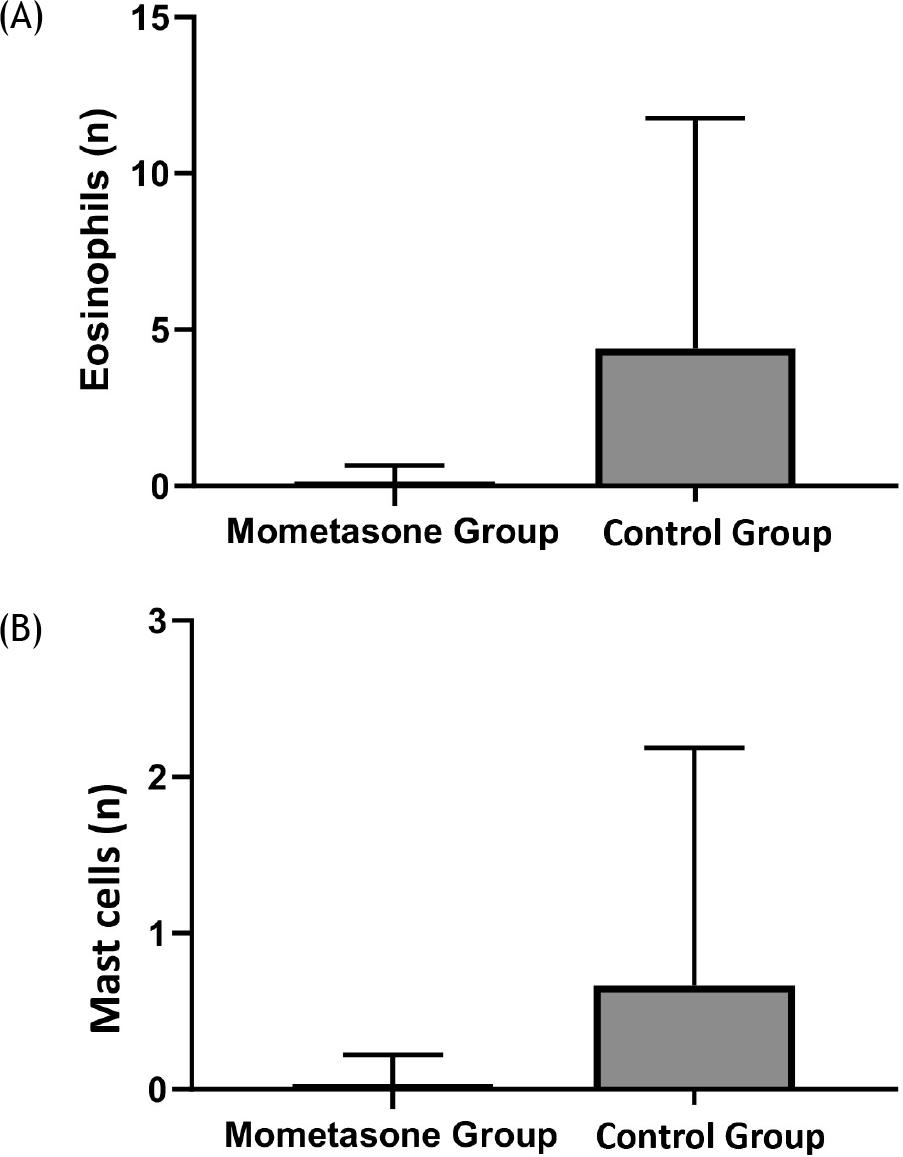
In the active group, eosinophils significantly diminished at T2 (P < 0.0001) compared to the control group, as shown in Figure 2A. However, the difference was not significant at T3. Consistently, mast cells significantly diminished at T2 (P = 0.03) in the active group compared to the control group, as shown in Figure 2B. However, the neutrophil count did not change during the treatment (P = 0.4).
Figure 2 (A) Eosinophil count at T1 in mometasone and placebo groups. (B) Mast cell count at T1 in mometasone and placebo groups.
Quality of life
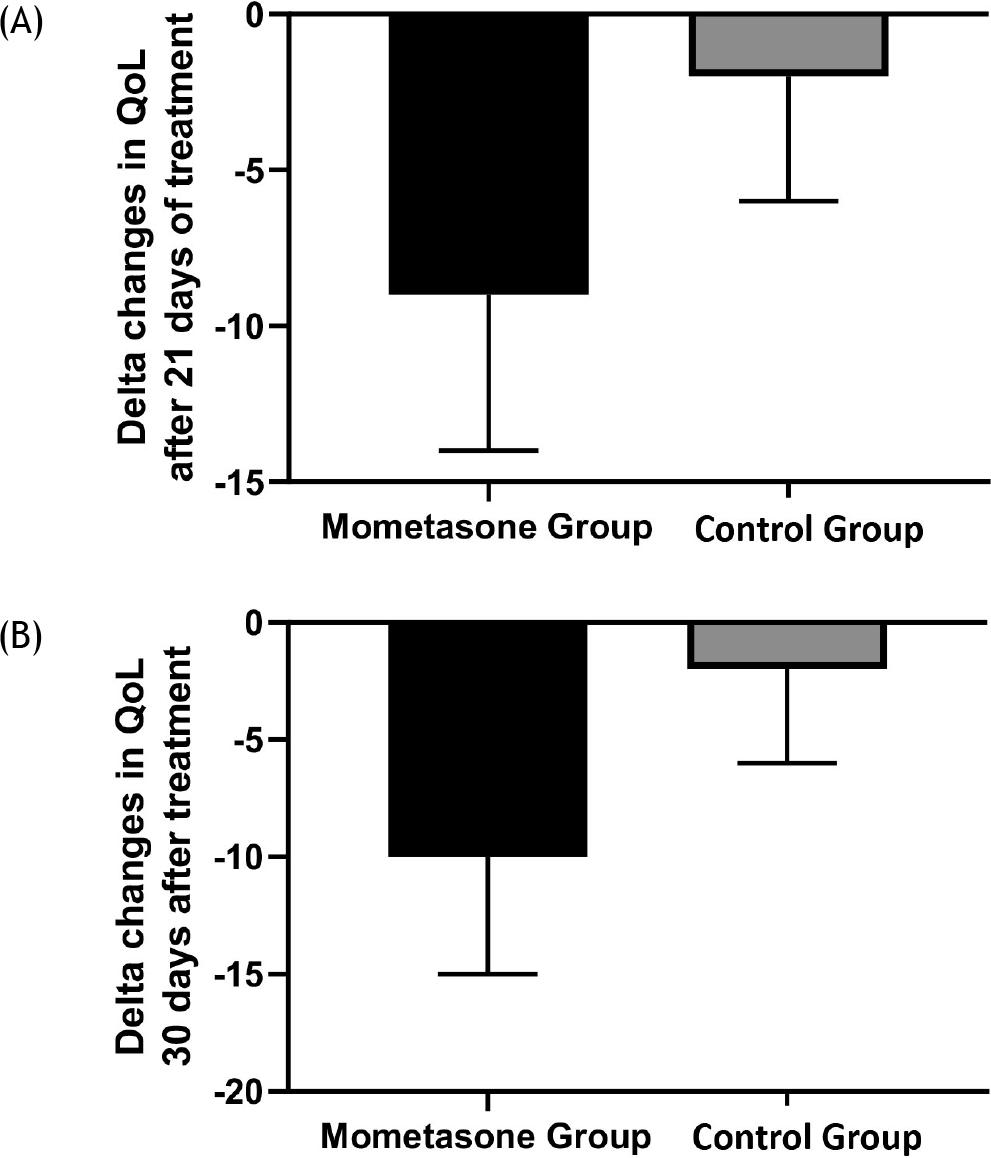
The QoL score significantly changed in the active group compared to the control group at T2 and T3 (P < 0.0001 for both), as shown in Figures 3A and B.
Figure 3 (A) Delta changes in QoL scores after 21 days of treatment in mometasone and placebo groups. (B) Delta changes in QoL scores 30 days after treatment in mometasone and placebo groups.
Severity of symptoms
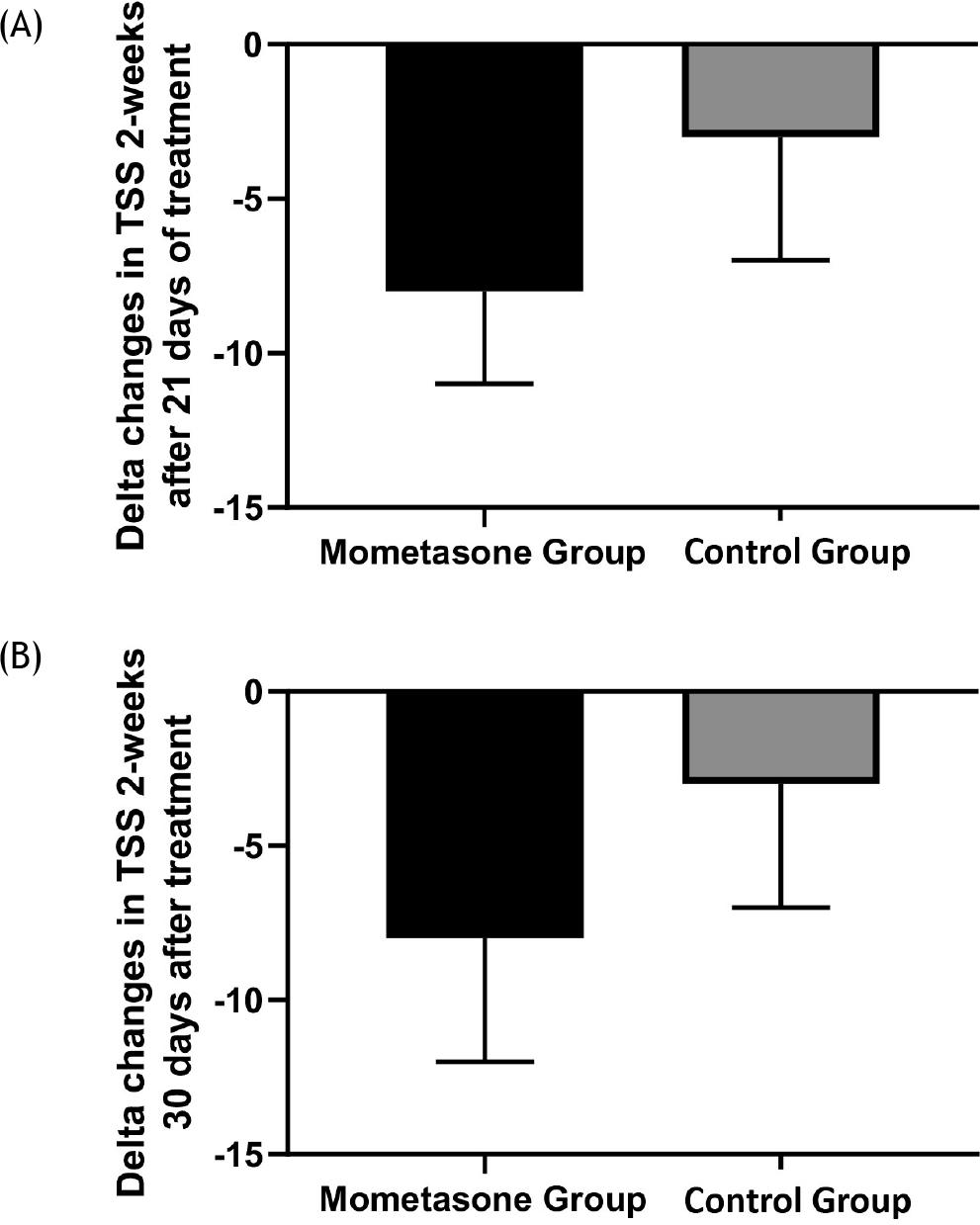
Severity of symptoms, measured by TSS, concerning the previous 2 weeks (TSS 2W) significantly diminished in the active group compared to the control group at T2 and T3 (P = 0.02 and 0.03, respectively), as shown in Figures 4A and B.
Figure 4 (A) Delta changes in TSS 2W after 21 days of treatment in mometasone and placebo groups. (B) Delta changes in TSS 2W 30 days after treatment in mometasone and placebo groups.
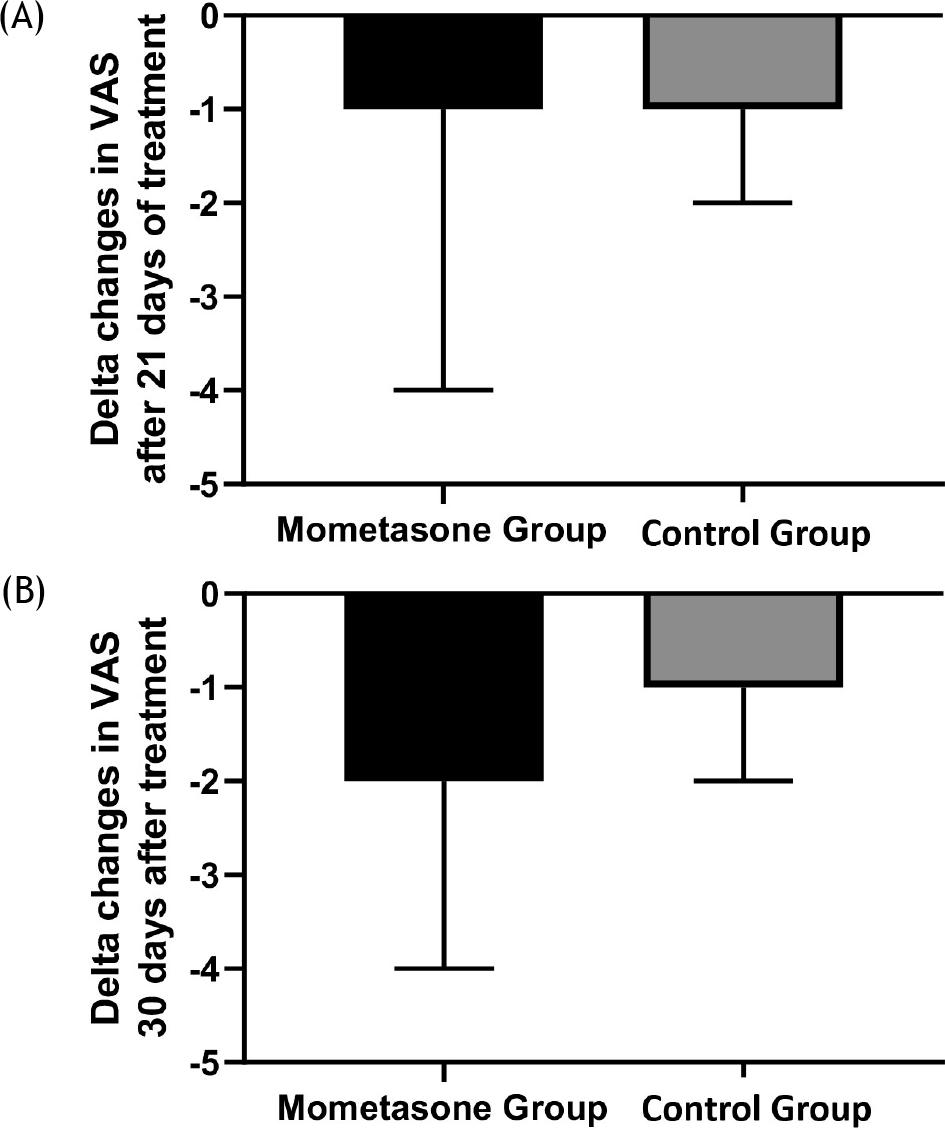
Consistently, the parental perception of severity of symptoms, measured by VAS, significantly diminished in the active group compared to the control group at T2 and T3 (P = 0.02 and 0.008, respectively), as shown in Figures 5A and B. However, there was no difference between groups for TSS 12h.
Figure 5 (A) Delta changes in VAS after 21 days of treatment in mometasone and placebo groups. (B) Delta changes in VAS 30 days after treatment in mometasone and placebo groups.
Intra-group analysis in the active group
Nasal cytology
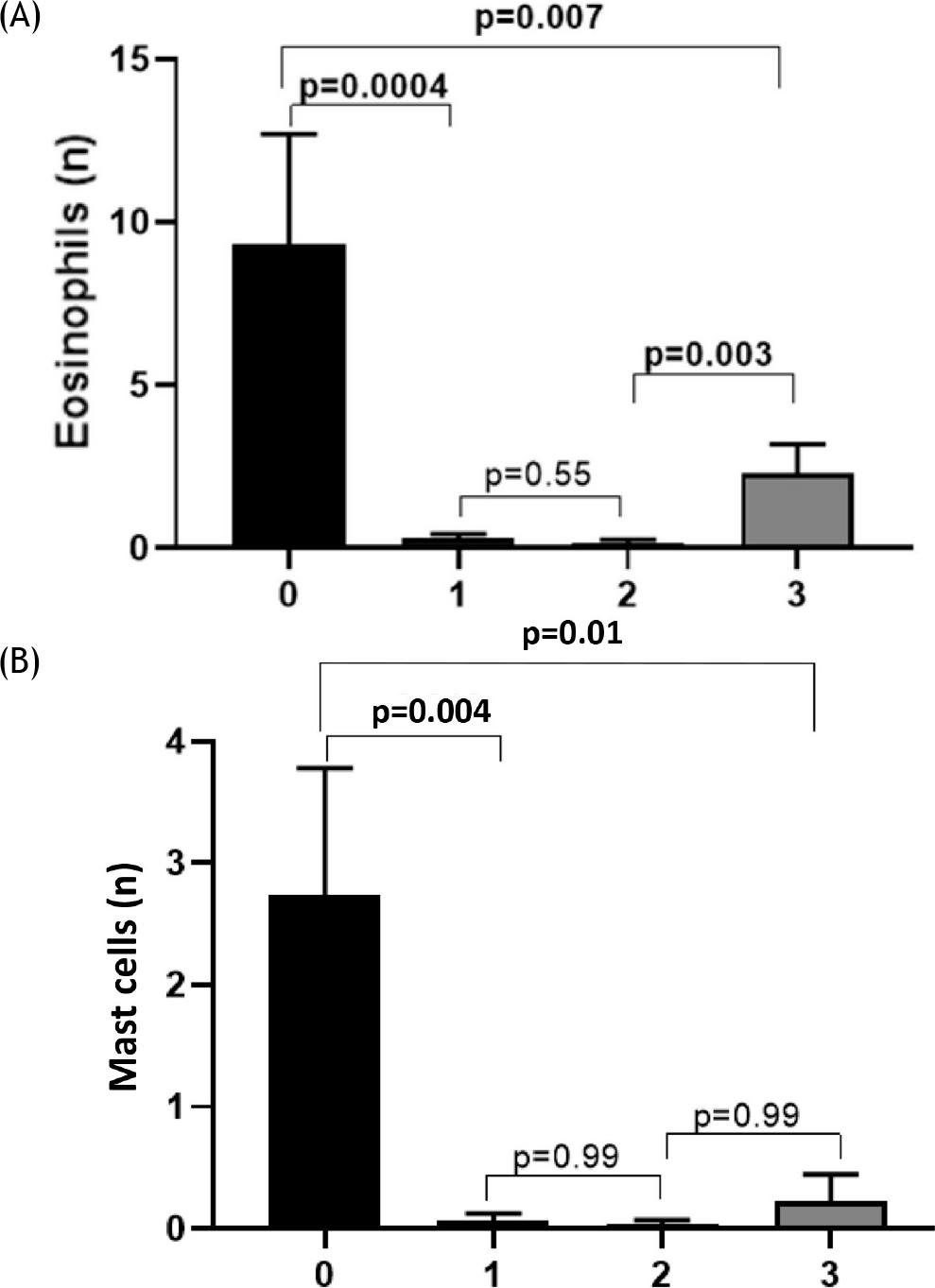
The longitudinal analysis demonstrated that there was a significant reduction of eosinophils between T0 and T1 (P = 0.0004); this reduction persisted between T1 and T2 (P = 0.55), but eosinophil count increased at T3 in comparison with T2 (P = 0.003); the eosinophil count at T3, however, remained lower than T0 (P = 0.007), as reported in Figure 6A. Consistently, mast cells count provided similar outcomes: they significantly diminished at T1 (P = 0.004), then there were no more changes at the subsequent visits, but the difference between T0 and T3 remained significant (P = 0.01), as shown in Figure 6B.
Figure 6 (A) Eosinophil count over time in the mometasone group. (B) Mast cell count over time in the mometasone group.
Quality of life
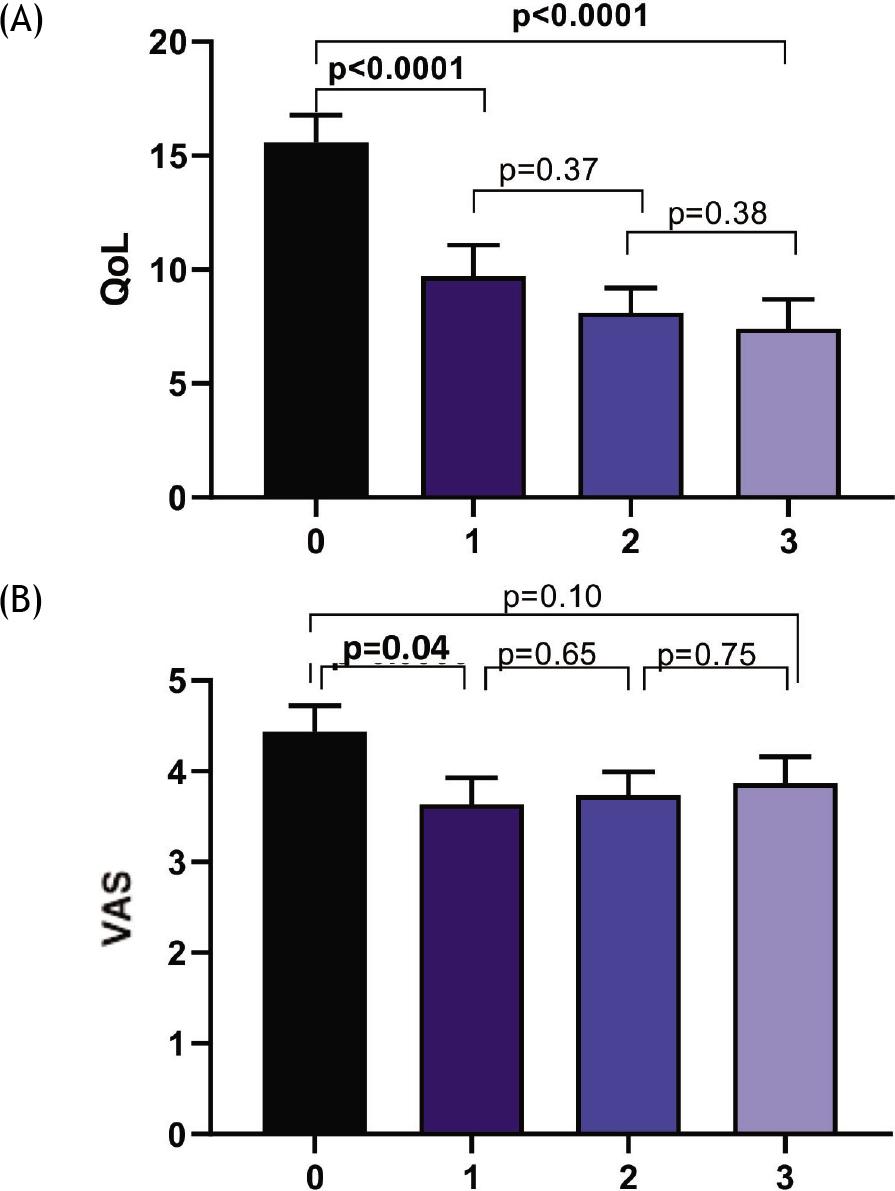
The QoL score significantly diminished at T1 (P < 0.0001), then there was no difference over time, but reduction in QoL score was significant at T3 compared to T0, as shown in Figure 7A.
Figure 7 (A) QoL scores over time in the mometasone group. (B) VAS scores over time in the mometasone group.
Severity of symptoms
The parental perception of severity of symptoms assessed by VAS significantly diminished at T1 (P = 0.04), but there was no difference on other visits, as shown in Figure 7B.
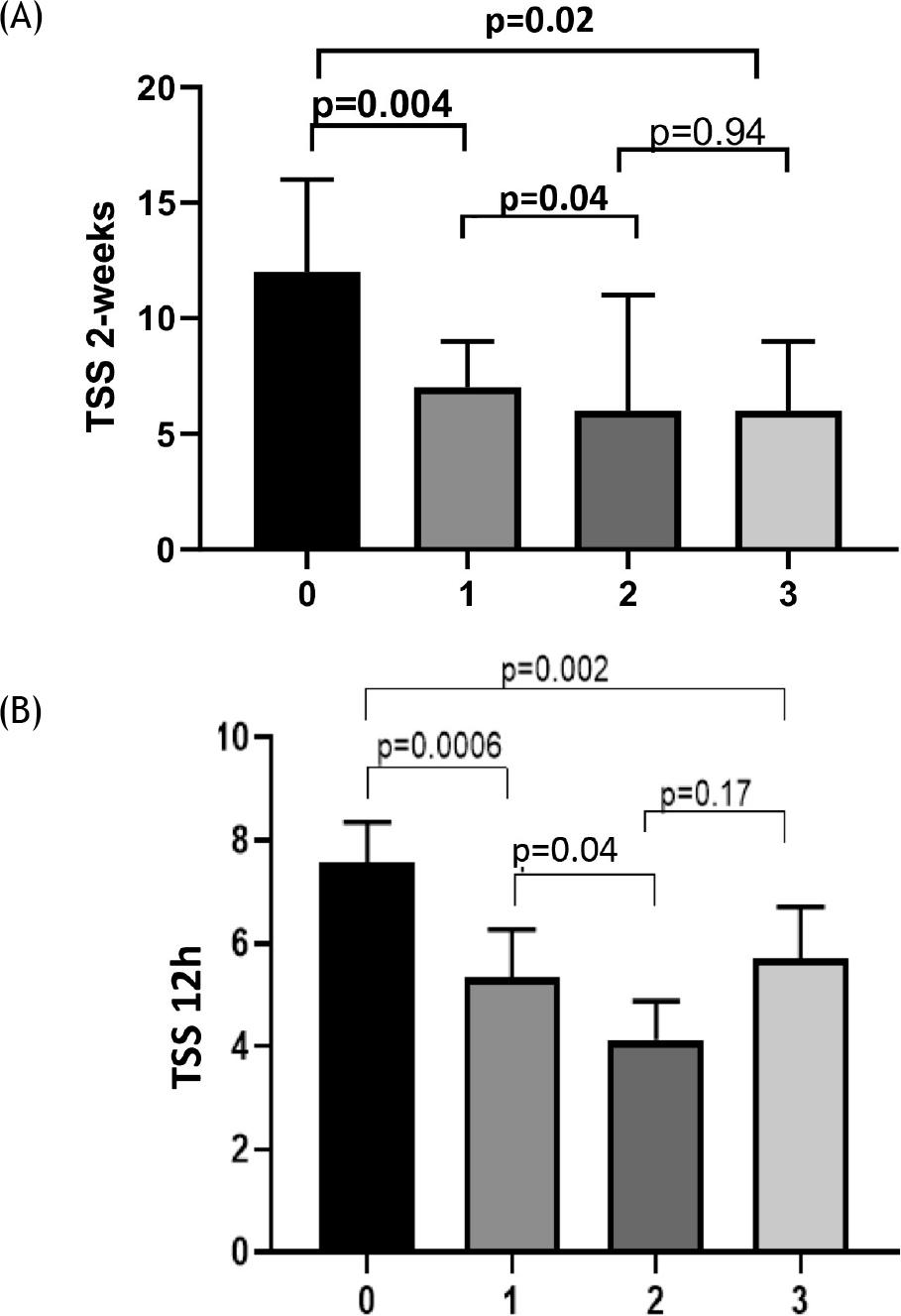
Total symptom score in the previous 2 weeks (TTS 2W) significantly diminished at T1 (P = 0.004) and T2 in comparison to T1 (P = 0.04), and between T0 and T3 (P < 0.02), as shown in Figure 8A. Consistently, TTS 12h significantly diminished at T1 (P = 0.0006), and between T2 and T1 (P=00.04); there was no difference between T2 and T3, but there was a significant difference between T3 and T0 (P = 0.002), as shown in Figure 8B.
Figure 8 (A) TSS 2W over time in the mometasone group. (B) TSS 12h over time in the mometasone group.
Both treatments were well-tolerated, and no clinically relevant adverse event was reported.
Discussion
Seasonal allergic rhinitis has clinical relevance as the symptoms are usually severe; SAR also has a negative impact on QoL, and type 2 inflammation is intense during pollen exposure.
The present study demonstrated that a 3-week course of MFNS significantly dampened type 2 inflammation, improved QoL, and relieved symptoms. Notably, there was consistency between the doctor’s and parents’ assessment of severity of symptoms. This finding underscores the reliability of parental perception of children’s clinical features. More interestingly, improvement in the primary outcome, such as eosinophilic inflammation, and secondary outcomes, including mast cells, severity of symptoms, and QoL, persisted even after discontinuation. This finding is clinically relevant as it confirms the prolonged activity of MFNS as observed in previous studies.10,11 In addition, this study was consistent with an earlier study that underlined the better effectiveness provided by intranasal corticosteroids in comparison to saline lavage.18
The present study adds novelty as it was been conducted in Europe. In particular, the center was located in southern Italy, a geographical area characterized by high pollen exposure and prolonged pollen season. In addition, the present study investigated cytological parameters, such as eosino-phil count. The vast majority of studies essentially consider clinical parameters. In contrast, having cytological parameters also allows for more complete information about the mechanism of action of corticosteroids. In fact, intranasal corticosteroids act eminently on the inflammatory component of allergic reaction. In particular, they significantly reduce eosinophilic infiltrate. This aspect represents the peculiarity of this study. Moreover, the European population, in particular the one evaluated in this study, that is, population of the Mediterranean basin, presents clinical and patho-physiological differences. In fact, it is known that every single pollen presents biological specificities compared to others, which result in a different clinical, functional, and cytological picture.19 The distribution of various pollen families in fact varies considerably according to geographical, meteorological, and climatic characteristics.20 Therefore, the results obtained allow to expand knowledge on the efficacy of the corticosteroid molecule tested. It would also be interesting to further this area of research by comparing other corticosteroid molecules with regard to anti-inflamma-tory activity on cytological pattern.
The present study has limitations, including the single-center and open design study, the restricted number of enrolled children, and the lack of sample size calculation and mediators’ assessment. On the other hand, this study simultaneously assessed nasal inflammation, QoL, and severity of symptoms, as measured by doctors and parents.
Conclusion
The present study documented that a 3-week MFNS treatment could significantly diminish type 2 inflammation, improve QoL, and reduce severity of symptoms in Italian children with SAR, and was safe.
Author contributions
Cristiana Indolfi, Giulio Dinardo, Angela Klain, Marcella Contieri, and Alberto Decimo collected the data and performed the research. Giuseppina Rosaria Umano analyzed the data, Fabio Decimo coordinated the research, Giorgio Ciprandi wrote the paper, and Michele Miraglia Del Giudice designed the study. All authors read and approved the final manuscript.
Financial disclosure
The authors stated that there was no conflict of interest to declare. There was no sponsorship. Valeas Farmaceutici SpA, Milan, Italy, provided an unrestricted grant to cover publication costs.
Data Availability
Data are available upon request to corresponding author.
REFERENCES
1. Wise SK, Lin SY, Toskala E, Orlandi RR, Akdis CA, Alt JA et al. International consensus statement on allergy and rhinology: Allergic rhinitis. Int Forum Allergy Rhinol. 2018;8: 108–352. 10.1002/alr.22073_c
2. Wen T, Rothenberg ME. Cell-by-cell deciphering of T cells in allergic inflammation. J Allergy Clin Immunol. 2019;144:1143–8. 10.1016/j.jaci.2019.10.001
3. Han X, Krempski JW, Nadeau K. Advances and novel developments in mechanisms of allergic inflammation. Allergy. 2020;75(12):3100–11. 10.1111/all.14632
4. Ciprandi, G, Klersy C, Cirillo I, Marseglia GL. Quality of life in allergic rhinitis: Relationship with clinical, immunological, and functional aspects. Clin Exp Allergy. 2007;37:1528–35. 10.1111/j.1365-2222.2007.02809.x
5. Ciprandi G, Cirillo I, Vizzaccaro A, Milanese M, Tosca MA. Nasal obstruction in patients with seasonal allergic rhinitis: Relationships between allergic inflammation and nasal airflow. Intern Arch Allergy Immunol. 2004;134:34–40. 10.1159/000077531
6. Cirillo I, Marseglia GL, Klersy C, Ciprandi G. Allergic patients have more numerous and prolonged respiratory infections than nonallergic subjects. Allergy. 2007;62:1087–90. 10.1111/j.1398-9995.2007.01401.x
7. Juel-Berg N, Darling P, Bolvig J, Foss-Skiftesvik MH, Halken S, Winther L, et al. Intranasal corticosteroids compared with oral antihistamines in allergic rhinitis: A systematic review and meta-analysis. Am J Rhinol Allergy. 2017;31(1):19–28. 10.2500/ajra.2016.30.4397
8. Baldwin CM, Scott LJ. Mometasone furoate: A review of its intranasal use in allergic rhinitis. Drugs. 2008;68(12):1723–39. 10.2165/00003495-200868120-00009
9. Ciprandi G, Varricchio A. The relevance of the mometasone furoate nasal spray in clinical practice. J Biol Regul Homeost Agents. 2018;32(4):1051–4.
10. Meltzer EO, Baena-Cagnani CE, Gates D, Teper A. Relieving nasal congestion in children with seasonal and perennial allergic rhinitis: Efficacy and safety studies of mometasone furoate nasal spray. World Allergy Organ J. 2013;6(1):5. 10.1186/1939-4551-6-5
11. Meltzer EO, Shekar T, Teper AA. Mometasone furoate nasal spray for moderate-to-severe nasal congestion in subjects with seasonal allergic rhinitis. Allergy Asthma Proc. 2011;32(2): 159–67. 10.2500/aap.2011.32.3424
12. Ciprandi G, Tosca MA, Passalacqua G, Canonica GW. Intranasal mometasone furoate reduces late-phase inflammation after allergen challenge. Ann Allergy Asthma Immunol. 2001; 86(4):433–8. 10.1016/S1081-1206(10)62491-X
13. Hoyte FCL, Nelson HS. Recent advances in allergic rhinitis. F1000 Res. 2018;7:F1000 Faculty Rev-1333. 10.12688/f1000research.15367.1
14. Karatzas K, Katsifarakis N, Riga M, Werchan B, Werchan M, Berger U, et al. New European Academy of Allergy and Clinical Immunology definition on pollen season mirrors symptom load for grass and birch pollen-induced allergic rhinitis. Allergy. 2018;73:1851–9. 10.1111/all.13487
15. Gelardi M, Fiorella ML, Russo C, Fiorella R, Ciprandi G. Role of nasal cytology. Int J Immunopathol Pharmacol. 2010;23 (Suppl 1):45–49.
16. Juniper EF, Guyatt GH, Feeny DH, Ferrie PJ, Griffith LE, Townsend M. Measuring quality of life in children with asthma. Qual Life Res. 1996;4:35–46. 10.1007/BF00435967
17. Benazzo M, Leonardi S, Corsico A, Licari A, Miraglia Del Giudice M, Peroni D, et al. Cetirizine modifies quality of life and symptoms in children with seasonal allergic rhinitis: A pilot study. Acta Biomed. 2020;92(1):e2021003.
18. Madison S, Brown EA, Franklin R, Wickersham EA, McCarthy LH. Clinical question: Nasal saline or intranasal corticosteroids to treat allergic rhinitis in children. J Okla State Med Assoc. 2016;109(4–5):152–3.
19. Gelardi M, Maselli del Giudice A, Candreva T, Fiorella ML, Allen M, Klersy K, et al. Nasal resistance and allergic inflammation depend on allergen type. Int Arch Allergy Immunol. 2006;141:384–9. 10.1159/000095465
20. D’Amato G, Holgate ST, Pawankar R, Ledford DK, Cecchi L, Al-Ahmad M, et al. Meteorological conditions, climate change, new emerging factors, and asthma and related allergic disorders. A statement of the World Allergy Organization. World Allergy Organ J. 2015;8(1):25. 10.1186/s40413-015-0073-0