
Download


ORIGINAL RESEARCH
Momordica charantia polysaccharides alleviate diarrhea-predominant irritable bowel syndrome by regulating intestinal inflammation and barrier via NF-κB pathway
Shanyun Ji, Qing Zhang*
Department of Digestive Internal Medicine, Lianyungang Hospital of Traditional Chinese Medicine, Lianyungang, Jiangsu, China
Abstract
Background: Momordica charantia exerts anti-inflammatory effect against ulcerative colitis. Momordica charantia polysaccharides (MCPs) attenuate gastritis through inhibition of ethanol-induced inflammatory response.
Objective: The role of MCPs in diarrhea-predominant irritable bowel syndrome (IBS-D) is investigated.
Materials and Methods: Chemical stimulation followed by acute and chronic pressure stimulation was used to establish rats model with IBS-D. The model rats were then administrated with MCPs. Defecation frequency, fecal water content and abdominal withdrawal reflex (AWR) score were then recorded. Pathologic changes in the colonic tissues were evaluated by hematoxylin and eosin staining. Inflammation was detected by ELISA and qRT-PCR, and immunohistochemistry was used to assess intestinal mucosal permeability.
Results: First, IBS-D of mice wasIBS-D ratsmice exhibited many abnormal clinical manifestations, including increased frequency of defecation, fecal water content, and abdominal withdrawal reflex (AWR) score. Second, the mice were administrated with MCPs, which reduced frequency of defecation, fecal water content, and AWR score, and 100-mg/kg MCPs indicated therapeutic effect on IBS-D mice equivalent to rifaximin. Moreover, MCPs also ameliorated pathologic changes in the colonic tissues of IBS-D mice. Third, inflammatory response in IBS-D mice was also suppressed by MCPs through up-regulation of Interleukin (IL)-10, and down-regulation of tumor necrosis factor-α (TNF-α), Interleukin(IL)-1β, and IL-6. MCPs enhanced levels of occludin (OCLN) and zona occludens protein-1 (ZO-1) in IBS-D mice to improve intestinal mucosal permeability. Finally, phosphorylation of p65 in IBS-D mice was reduced by MCP treatment.
Conclusion: MCPs ameliorated intestinal permeability and repressed intestinal inflammation to attenuate IBS-D by inactivating nuclear factor kappa B (NF-κB) signaling.
Key words: momordica charantia polysaccharides, diarrhea-predominant irritable bowel syndrome, intestinal permeability, intestinal inflammation, NF-κB
*Corresponding author: Qing Zhang, Department of Digestive Internal Medicine, Lianyungang Hospital of Traditional Chinese Medicine, No. 160, Chaoyang Middle Road, Haizhou District, Lianyungang, Jiangsu 222000, China. Email address: [email protected]
Received 14 January 2022; Accepted 22 February 2022; Available online: 1 May 2022
Ji S, Zhang Q
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Irritable bowel syndrome (IBS), a common clinical functional gastrointestinal disease, is characterized by abdominal pain and disturbance in bowel movement.1 The Occurrence of IBS is closely associated with intestinal flora imbalance, inflammation, and physical and mental stress in early life.2,3 In recent years, incidents of IBS have increased gradually, ranging from 9% to 22% in Western countries and from 7% to 12% in China.4 Alterations in intestinal microbiota, environmental factors, visceral hypersensitivity, alterations in gastrointestinal motility, and other factors are considered involved in the pathogenesis of IBS.5 IBS contains four different subtypes, which include unclassified, mixed bowel habits, constipation-predominant IBS (IBS-C), and diarrhea-predominant IBS (IBS-D). IBS-D is the primary type encountered in China.5 Medications, such as Xifaxan (rifaximin) and Viberzi (eluxadoline), that reduce abdominal pain and episodes of diarrhea, have been approved for treating IBS-D.6 However, rifaximin might develop antimicrobial resistance.7 Therefore, other strategies are urgently required for prevention of IBS-D.
Alteration in host-gut microbial system, such as Actinobacteria, Firmicutes, Bacteroidetes, and Proteobacteria, reduces microbial richness and beneficial bacterial groups but enhances the detrimental ones, thus contributing to the development of IBS-D.5 Low-fermentable oligosaccharide, disaccharide, monosaccharide, and polyols diet induces intestinal microbiota, and changes and reduces abdominal pain and stool consistency in patients with IBS-D.5 Therefore, strategies to alter gut microbiota might be promising for preventing IBS-D.8
Momordica charantia (bitter melon) is a popular vegetable used widely as a traditional Chinese medicine for treating inflammatory diseases.9 Momordica charantia also exerts pharmacological properties, including anthelmintic, immunomodulatory, antihyperlipidemic, antioxidant, antimicrobial, anticancer, anti-obesity, and antidiabetic, in distinct diseases.10 Momordica charantia polysaccharides (MCPs), its primary active components, have demonstrated beneficial antioxidant and anti-inflammatory effects to relieve depressive behavior in mice.11 MCPs have also been depicted to regulate changes in the gut microbiota in obese mice, and attenuate metabolic disorders.12 Therefore, MCPs might be beneficial for treating IBS-D as well.
In this study, the authors investigated effects of MCPs on intestinal inflammation and barrier of mice with IBS-D. The underlying mechanism might provide a novel strategy for treating IBS-D.
Materials and methods
Preparation of MCPs
A total of 100-g dried Momordica charantia powder was dissolved in 90% ethanol, the supernatant was removed and the residue was incubated with water at 100°C for 4 h. The extract was filtered, concentrated at 60°C, and de-proteinated. The extract was incubated overnight with ethanol with a weight ratio of 4:1 at 4°C, and nMCPs were precipitated through centrifugation and lyophilization.
Animal models
Specific pathogen-free, 6–8-week old mice, with a weight fromweighing 200g to –220 g (N = 50), were purchased from Hunan Silaike Jingda Laboratory Animal Co. Ltd. (Changsha, China) and housed in cages with food and water ad libitum. Ethical approval for the study was obtained from the Ethics Committee of Lianyungang Hospital of Traditional Chinese Medicine (Approval No. 2020 (KY)-04) (Approval No.2020- (KY)-04). Mice were divided into the following five groups: control (N = 10), IBS-D (N = 10), IBS-D + rifaximin (N = 10), IBS-D + 50-mg/kg MCPs (N = 10), and IBS-D + 100-mg/kg MCPs (N = 10). In IBS-D groups, mice were anesthetized with 2% pentobarbital injected intraperitonealy Intracolonic administration of 4% acetic acid (1 mL) at the position 8 cm proximal to the anus was made in all animals. The colon was diluted with byphosphate-buffered saline solution (PBS; 1 mL). Mice in the control group were instilled PBS without acetic acid, and those in the IBS-D groups were subjected to unpredictable chronic stress for 3 weeks, after 7 days post acetic acid-induced colitis. Mice were also subjected to acute restraint stress for 1 h after 7 days post chronic stress exposure. Animals in the IBS-D, IBS-D + rifaximin, IBS-D + 50-mg/kg MCPs, and IBS-D + 100-mg/kg MCPs groups were fed with normal saline, 50-mg/kg rifaximin, 50-mg/kg MCPs, and 100-mg/kg MCPs once a day. All the animals were subjected to behavioral evaluation 7 days later, and the distal colons were isolated from the mice for subsequent experiments.
Detection of defecation frequency and fecal water content
Mice were placed in cages with food and water ad libitum for 24 h. The number of fecal pellets in 1 h was counted and regarded as defecation frequency. The fecal water content was calculated as follows: weight of stool - weight of dried stool/weight of stool.
Detection of abdominal withdrawal reflex (AWR) scores
Mice were placed in a small cubicle and inserted with a vaseline-coated balloon dilator (2 mm in diameter) at 8 cm proximal to the anus into the descending colon. The dilator was attached to a pressure gauge T-connector. Desired pressure (20, 40, 60, or 80 mmHg) was produced in balloon to induce colorectal distension. The AWR score was assigned by blinded observers based on the following criteria: Point 0 for no behavioral response, point 1 for simple head movement, point 2 for abdominal muscle contraction, point 3 for abdominal rise, and point 4 for back arch and pelvis ascending. Experiments were repeated at least in triplicate.
Pathologic analysis
The distal colons were fixed in 10% formalin, dehydrated with 4% paraformaldehyde, and then embedded into paraffin. Tissues were sliced into 5-μm thick sections with a thickness of , which were stained with hematoxylin and eosin (H&E; Sigma-Aldrich, St. Louis, MO, USA). The slides were observed under microscope (Olympus BX53, Olympus, Tokyo, Japan). The pathological injury score was calculated by blinded observers as points of mucosa damage plus points of inflammatory damage based on the following criteria: Point 0 for less than 1% mucosa damage or no inflammation; point 1 for slight mucosa damage (less than 1/3) or sparse inflammatory infiltrate (less than 25% damage extent); point 2 for mild mucosa damage (less than 2/3) or mild inflammatory infiltrate (25–50% damage extent); point 3 for mucosa and gland damage (large area damaged) or inflammatory infiltrate (50–75% damage extent); and point 4 for severe mucosa damage (completely damaged) or severe inflammatory infiltrate (75–100% damage extent). All experiments were repeated at least in triplicate.
Real-time quantitative polymerase chain reaction (RT-qPCR)
The distal colons were lysed with TRIzol kit (Invitrogen, Carlsbad, CA, USA), and isolated RNAs were synthesized into complementary DNAs (cDNA). PreTaq II kit (Takara, Dalian, Liaoning, China) was used to determine messenger RNA (mRNA) expression of tumor necrosis factor-α (TNF-α), Interleukin 1β (IL-1β), IL-6, and IL-10. The relative expression was calculated using the delta-delta Ct (control) (2-ΔΔCt) method through normalization to glyceraldehyde 3-phosphate dehydrogenase (GAPDH). Primers are shown in Table 1.
Table 1 Primers.
| Genes | Forward | Reverse |
|---|---|---|
| GAPDH | 5’-TCAACGACCACTTTGTCAAGCAGAGT-3’ | 5’-GCTGGTGGTCCAGGGGTCTTACT-3’ |
| IL-6 | 5’-AGACAGCCACTCACCTCTTCAG-3’ | 5’-TTCTGCCAGTGCCTCTTTGCTG-3’ |
| IL-10 | 5’-GCCTAACATGCTTCGAGATC-3’ | 5’-TGATGTCTGGGTCTTGGTTC-3’ |
| IL-1β | 5’-CCAGCTTCAAATCTCACAGCAG-3’ | 5’-CTTCTTTGGGTATTGCTTGGGATC-3’ |
| TNF-α | 5’-CCGAGTGACAAGCCTGTAGC-3’ | 5’-AGGAGGTTGACCTTGGTCTG-3’ |
Enzyme-linked immunosorbent serologic assay (ELISA)
Colonic tissues were digested in radioimmunoprecipitation assay (RIPA) buffer (Beyotime, Beijing, China), and centrifuged at 12,000 g to collect supernatants. Levels of TNF-α, IL-1β, IL-6, and IL-10 were detected by ELISA kits (Pharmingen, San Diego, CA, USA).
Immunofluorescence
The colonic sections were incubated with target retrieval solution (Agilent Technologies, Santa Clara, CA, USA) and blocked in 4% hydrogen peroxide. Followed by treatment with 4% goat serum, the sections were incubated with rabbit anti-rat occludin (OCLN) and zona occludens protein-1 (ZO-1) antibodies (1:100; Abcam, Cambridge, MA, USA). The slides were incubated with horseradish peroxidase-conjugated goat anti-rabbit secondary antibody, and then stained with diaminobenzidine (DAB). The slides were counterstained with DAPI (4',6-diamidino-2-phenylindole) fluorescent stain before observing observation under microscope.
Western blot analysis
Proteins were isolated from colonic tissues and separated by 10% sodium dodecyl sulfate–polyacrylamide gel electrophoresis (SDS-PAGE). Proteins were transferred on nitrocellulose membranes, and the membranes were blocked with 5% bovine serum albumin. The membranes were probed with specific antibodies: anti-p-p65 and anti-p65 (1:3,000), anti-p-IκBα and anti-IκBα (1:4,000), and anti-GAPDH (1:5,000). The membranes were washed and incubated with horseradish peroxidase (HRP)-conjugated secondary antibody (1:5,000). Immunoreactivities were visualized using enhanced chemiluminescence (Sigma-Aldrich). All the antibodies were purchased from Abcam.
Statistical analysis
All the data with at least triple replicates were expressed as mean ± standard deviation (SD). Comparisons between groups were conducted wereby Student’s t-test. Multiple comparisons within groups were carried outconducted using one-way analysis of variance (ANOVA) using the SPSS software. P < 0.05 was considered as statistically significant.
Results
MCPs alleviated clinical manifestations in mice with IBS-D
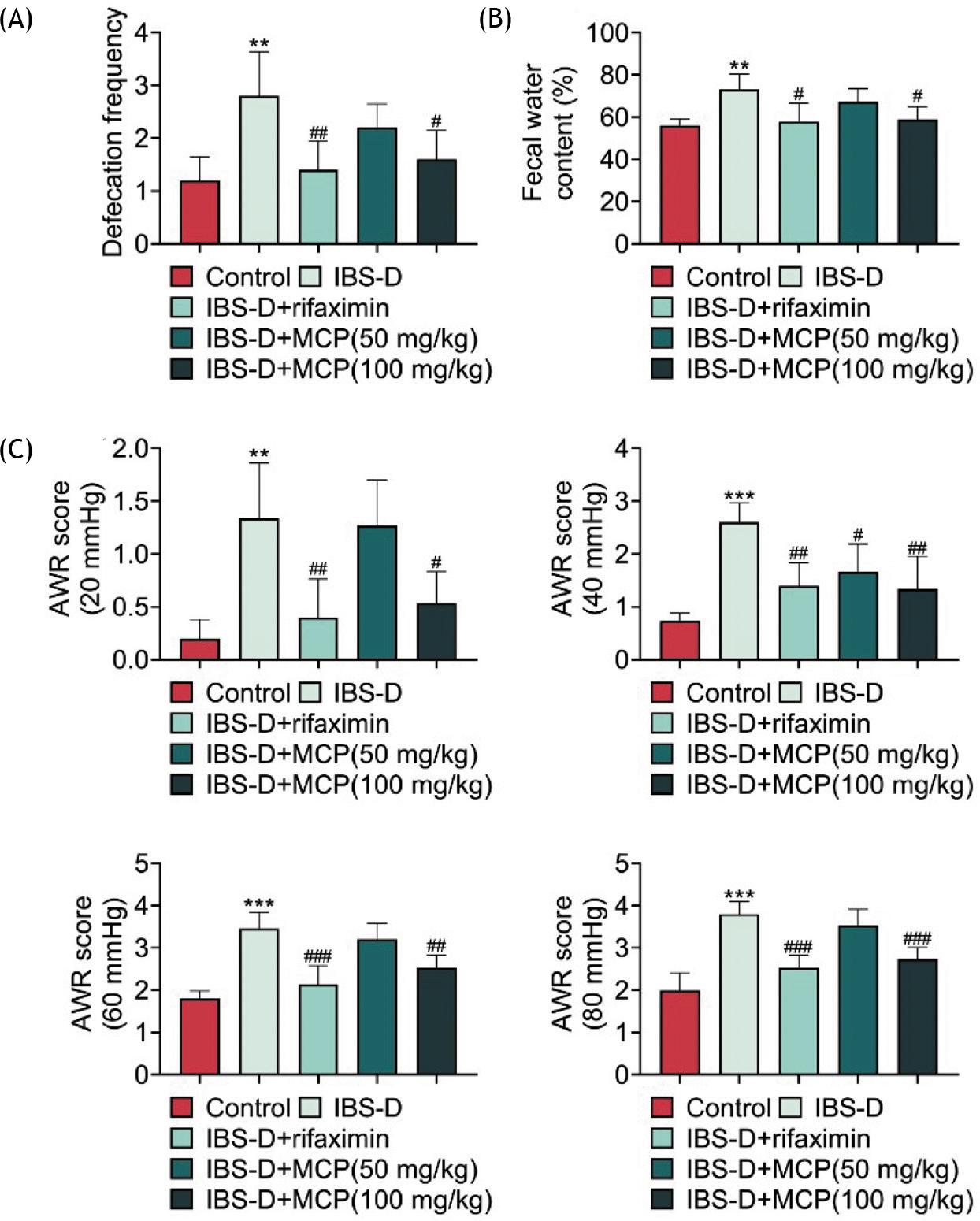
In order to induce IBS-D, mice were subjected to chemical stimulation followed by acute and chronic pressure stimulation. The defecation frequency (Figure 1A) and fecal water content (Figure 1B) were increased in mice with IBS-D. Rifaximin reduced the levels of both defecation frequency (Figure 1A) and fecal water content (Figure 1B) in IBS-D mice. Administration of MCPs decreased defecation frequency (Figure 1A) and fecal water content (Figure 1B) of IBS-D animals in a dose-dependent manner, and 100 mg/kg MCP demonstrated equivalent effects to rifaximin on frequency of defecation (Figure 1A) and fecal water content (Figure 1B). Moreover, AWR scores were increased with the increase ing of pressure (20, 40, 60, or 80 mmHg) in IBS-D mice (Figure 1C). However, MCPs decreased the scores and the effect was equivalent to rifaximin (Figure 1C), suggesting that MCPs alleviated clinical manifestations in mice with IBS-D.
Figure 1 MCPs alleviated clinical manifestations of mice with IBS-D. (A) Defecation frequency was increased in mice with IBS-D, while administration with rifaximin and MCPs reduced frequency of defecation. (B) Fecal water content was increased in mice with IBS-D, while administration of rifaximin and MCPs reduced the level of fecal water content. (C) AWR score was enhanced in mice with IBS-D, while administration of rifaximin and MCPs reduced the level of AWR score. Control vs. *P < 0.05, **P < 0.01, ***P < 0.001. IBS-D vs. #P < 0.05, ##P < 0.01.
MCPs alleviated colon pathological edema in mice with IBS-D
Histological analysis demonstrated that the colonic epithelial cells in the control group were intact, and the intestinal mucosal barrier depicted integrity (Figure 2). However, the colonic epithelial cells in IBS-D mice had exhibited significant edema, impaired integrity of the intestinal mucosa, and increased inflammatory infiltration (Figure 2). Administration of MCPs reduced the pathological injury score through amelioration of edema, integrity of the intestinal mucosa, and the increased inflammatory infiltration (Figure 2). The protective effect of 100-mg/kg MCPs against colon pathological edema in mice with IBS-D was equivalent to that of rifaximin (Figure 2).
Figure 2 MCPs alleviated colon pathological edema in mice with IBS-D. Histological analysis demonstrated that the colonic epithelial cells in IBS-D mice had significant edema, impaired integrity of intestinal mucosa, and increased inflammatory infiltration compared to the control group. Administration of rifaximin and MCPs reduced pathological injury score through amelioration of edema, integrity of the intestinal mucosa, and inflammatory infiltration. Control vs. ***P < 0.001. IBS-D vs. ##P < 0.01, ###P < 0.001.
MCPs alleviated colonic inflammation in mice with IBS-D
Levels of pro-inflammatory factors, including TNF-α, IL-1β, and IL-6, were enhanced in IBS-D mice (Figures 3A and B). Administration with rifaximin and MCPs increased expression of IL-10 and decreased levels of TNF-α, IL-1β, and IL-6 in IBS-D mice (Figures 3A and B), demonstrating the anti-inflammatory effect of MCPs against IBS-D.
Figure 3 MCPs alleviated colonic inflammation in mice with IBS-D. (A) mRNA expressions of TNF-α, IL-1β, and IL-6 were up-regulated in mice with IBS-D, and administration of rifaximin and MCPs enhanced the mRNA expression of IL-10 to reduce TNF-α, IL-1β, and IL-6 levels. (B) Protein expressions of TNF-α, IL-1β, and IL-6 were up-regulated in mice with IBS-D, and administration of rifaximin and MCPs enhanced the protein expression of IL-10 to reduce TNF-α, IL-1β, and IL-6 levels. Control vs. *P < 0.05 and ***P < 0.001. IBS-D vs. #P < 0.05, ##P < 0.01, and ###P < 0.001.
MCPs improved intestinal mucosal permeability in mice with IBS-D
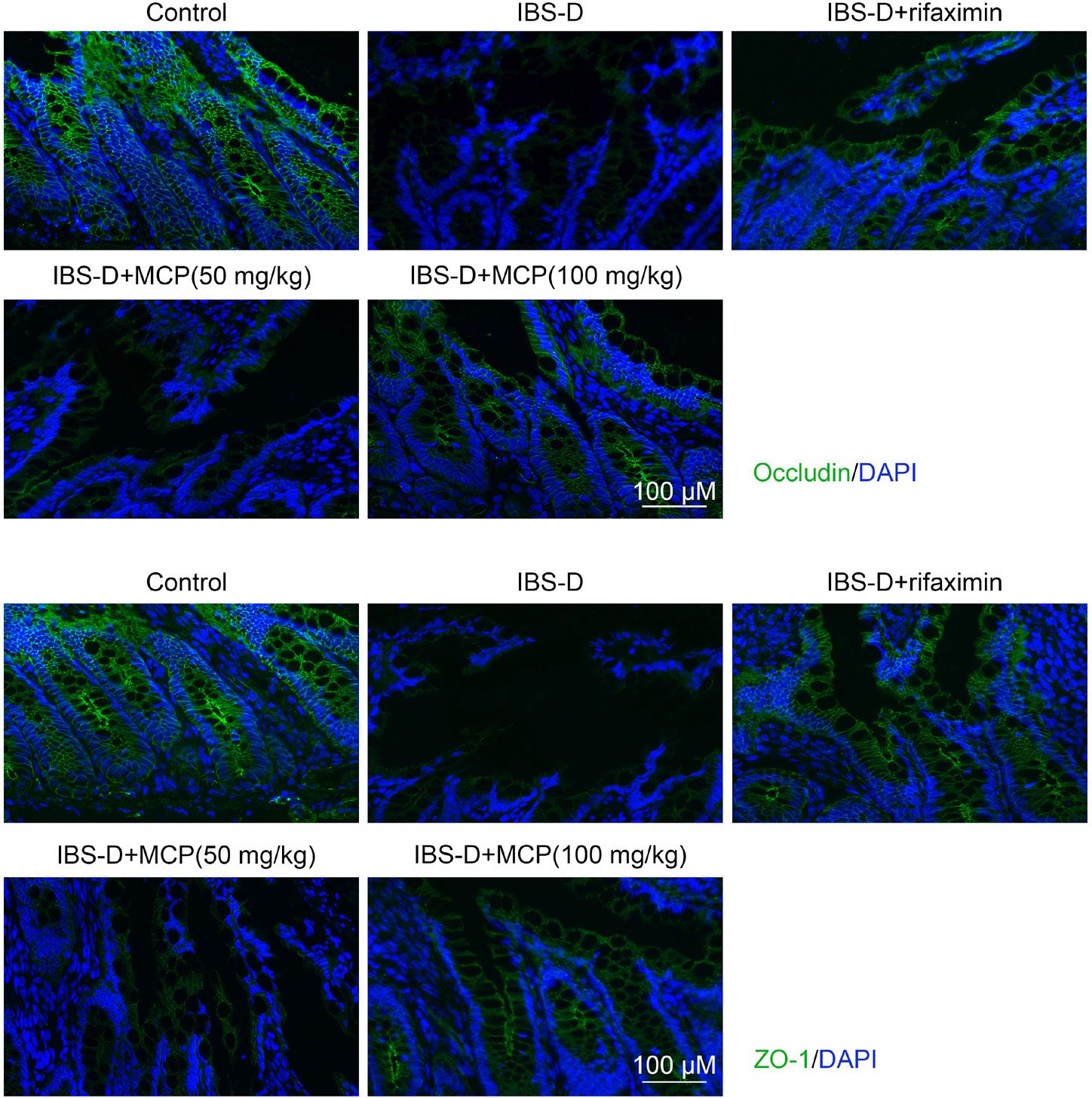
Immunofluorescence analysis demonstrated that proteins involved in tight junctions, OCLN, and ZO-1 were decreased in IBS-D mice (Figure 4). However, MCPs increased the levels of OCLN and ZO-1 in IBS-D mice (Figure 4) to attenuate the impaired integrity of the intestinal mucosa. MCPs (100 mg/kg) demonstrated equivalent effect to that of rifaximin on improving the intestinal mucosal permeability in mice with IBS-D (Figure 4).
Figure 4 MCPs improved intestinal mucosal permeability in mice with IBS-D. Occludin and ZO-1 were decreased whereas rifaximin and MCPs increased OCLN and ZO-1 in IBS-D mice.
MCPs regulated nuclear factor kappa B (NF-κB) signaling in mice with IBS-D
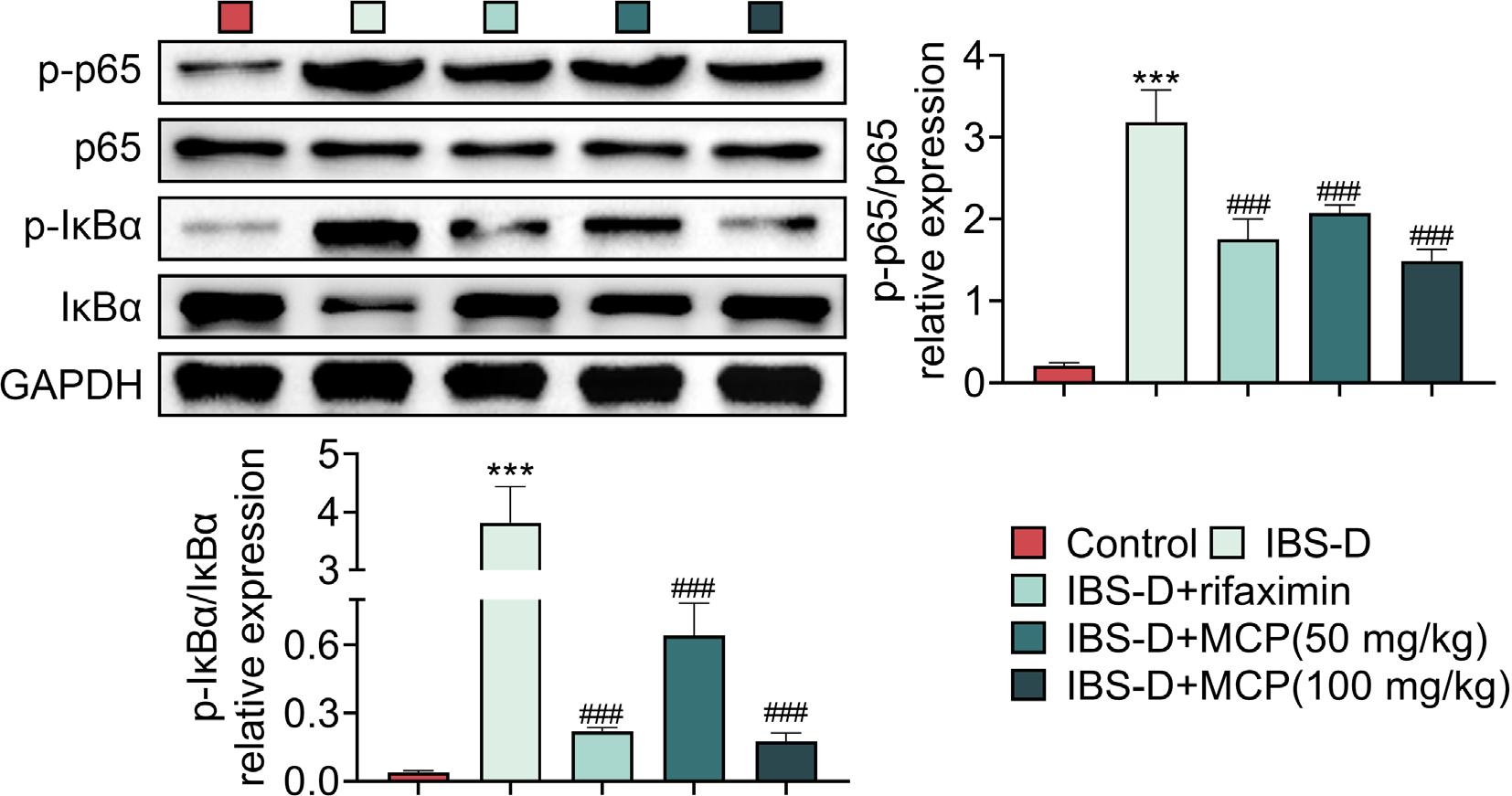
Protein expression of NF-κB, IκBα, was down-regulated in IBS-D mice (Figure 5), while p-p65 and p-IκBα were up-regulated in the IBS-D animals (Figure 5). However, rifaximin and MCPs enhanced the expression of IκBα to reduce p-p65 and p-IκBα expressions in IBS-D animals (Figure 5), indicating that MCPs repressed the activation of NF-κB signaling in IBS-D mice.
Figure 5 MCPs regulated NF-κB signaling in IBS-D mice. IκBα was down-regulated, and p-p65 and p-IκBα were up-regulated in IBS-D mice. Rifaximin and MCPs enhanced expression of IκBα to reduce p-p65 and p-IκBα in IBS-D mice. Control vs. ***P < 0.001. IBS-D vs. ###P < 0.001.
Discussion
Momordica charantia, a traditional Chinese herb, is widely used in the treatment of trinitrobenzene sulfonic acid-induced instigated ulcerative colitis through suppression of inflammatory response.13 MCPs are indicated to decrease levels of harmful bacteria, Helicobacter and Proteobacteria but enhanced the levels of beneficial bacteria, Bifidobacterium, Lactobacillus, Coprococcus, Anaerostipes, Actinobacteria, and Firmicutes, to ameliorate metabolic disorders in obese mice.12 This study found that MCPs alleviated IBS-D through promotion of intestinal mucosal permeability and suppression of intestinal inflammation.
A prior study demonstrated that chemical stimulation accompanied with stimulation of acute and chronic pressure induced pathological edema and intestinal hypersensitivity in mice, and was widely used in the establishment of IBS-D model.14 Our results also demonstrated that defecation frequency and fecal water content were increased in IBS-D mice. Moreover, the colorectal distension was also enhanced in IBS-D animals. However, MCPs ameliorated colonic motility and sensibility in IBS-D mice by decreasing defecation frequency and fecal water content. MCPs also attenuated colorectal distension in IBS-D animals. Additionally, MCPs also reduced infiltration of inflammatory cells and alleviated intestinal mucosal barrier integrity of the mucosal layers in IBS-D mice. MCPs had equivalent effect to that of an Food and Drug Administration (FDA) approved antibiotic agent (rifaximin) on IBS-D. Therefore, MCPs alleviated clinical manifestations and colon pathological edema in mice with IBS-D. Moreover, levels of OCLN and ZO-1, essential for permeability of tight junctions in the colonic tissues, were reduced in IBS-D mice.15 MCPs enhanced OCLN and ZO-1 to improve intestinal mucosal permeability in mice with IBS-D.
Infective gastroenteritis induces alteration in microbiome diversity, and aggravates the systemic inflammation during the development of IBS-D.16 Levels of proinflammatory factors (TNF-α, IL-6, and inducible nitric oxide synthase [iNOS[) were increased in IBS-D mice.14 IL-10, an anti-inflammatory factor, was lower in patients with IBS-D than that in healthy controls.17 Anti-inflammatory therapies depicted promising clinical perspectives in IBS-D.18 MCPs reduced levels of TNF-α and IL-1β to protect against Parkinson’s disease.19 Results in this study revealed that MCPs increased IL-10 expression to down-regulate the levels of TNF-α, IL-1β, and IL-6 in IBS-D mice, thereby exerting anti-inflammatory effect against IBS-D. Compared with healthy controls, patients with IBS-D demonstrated higher level of malondialdehyde and lower level of total antioxidant capacity.17 Therefore, oxidative stress was also implicated in the pathogenesis of IBS-D.20 Considering the antioxidant effect of MCPs in myocardial infarction,21 these polysaccharides might also reduce oxidative stress in IBS-D mice.
NF-κB, a nuclear transcription factor of inflammation, is involved in various inflammatory diseases such as IBS-D.22 Abnormal activation of the mucosal NF-κB signaling reduced the expression of IL-10 and promoted the expression of pro-inflammatory cytokines, such as IL-1β, IL-6, and TNF-α, in IBS-D.22 The secretion of pro-inflammatory cytokines and recruitment of neutrophils induced a series of pathological changes, such as intestinal epithelial cell injury, crypt abscess, and microvasculitis, and lead to increased intestinal permeability during the development of IBS-D.23 MCPs inhibited ethanol-induced activation of NF-κB signaling in the mucosa, and suppressed inflammatory response.24 Here, our results indicated that MCPs enhanced the expression of IκBα to reduce p-p65 and p-IκBα expressions in IBS-D mice, indicating that MCPs inhibited the activation of NF-κB signaling in IBS-D mice.
Conclusion
Momordica charantia polysaccharides alleviated clinical manifestations and colon pathological edema in IBS-D mice, improved intestinal barrier, and inhibited intestinal inflammation through inactivation of NF-κB signaling pathway. MCP might be regarded as a potential strategy for preventing IBS-D.24 However, the protective function of MCPs in the intestinal mucosal barrier of IBS-D should be investigated in the future research. Additionally, previousprevious prior study has highlighted the link between IBS and non-alcoholic fatty liver disease (NAFLD).25 Momordica charantiaMC extract inhibited lipid accumulation, suppressed adipose tissue volume, improvedincreased glucose tolerance and insulin resistance, and reduced gene expression thatinvolved in synthesis of fatty acid synthesis,26 which is likely to cause NAFLD. The data indicated that MCPs might function in NAFLD. Therefore, it is also interesting to further explore the effect of MCPs on NAFLD.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
Competing interests
The authors state that there were no conflicts of interest to disclose.
Contribution of authors
Shanyun Ji designed the study and supervised data collection. Qing Zhang analyzed and interpreted the data. Both authors prepared and reviewed draft of the manuscript. Both authors read and approved the final manuscript.
REFERENCES
1. Weaver KR, Melkus GD, Henderson WA. Irritable Bowel syndrome. Am J Nurs. 2017;117(6):48–55. 10.1097/01.NAJ.0000520253.57459.01
2. Greenwood-Van Meerveld B, Johnson AC. Stress-induced chronic visceral pain of gastrointestinal origin. Front Syst Neurosci. 2017;11:86. 10.3389/fnsys.2017.00086
3. Chen YJ, Wu H, Wu SD, Lu N, Wang YT, Liu HN, et al. Parasutterella, in association with irritable bowel syndrome and intestinal chronic inflammation. J Gastroenterol Hepatol. 2018;33(11):1844–52. 10.1111/jgh.14281
4. Canavan C, West J, Card T. The epidemiology of irritable bowel syndrome. Clin Epidemiol. 2014;6:71–80. 10.2147/CLEP.S40245.
5. Altomare A, Di Rosa C, Imperia E, Emerenziani S, Cicala M, Guarino MPL. Diarrhea predominant-irritable bowel syndrome (IBS-D): Effects of different nutritional patterns on intestinal dysbiosis and symptoms. Nutrients. 2021;13(5):1506. 10.3390/nu13051506.
6. Weber HC. New treatment options for irritable bowel syndrome with predominant diarrhea. Curr Opinion Endocrinol Diabetes Obesity. 2017;24(1):25-30. 10.1097/MED.0000000000000302
7. Farrell DJ. Rifaximin in the treatment of irritable bowel syndrome: Is there a high risk for development of antimicrobial resistance? J Clin Gastroenterol. 2013;47(3):205-211. 10.1097/MCG.0b013e31827559a3
8. Mei L, Zhou J, Su Y, Mao K, Wu J, Zhu C, et al. Gut microbiota composition and functional prediction in diarrhea-predominant irritable bowel syndrome. BMC Gastroenterol. 2021;21(1):105–. 10.1186/s12876-021-01693-w
9. Bortolotti M, Mercatelli D, Polito L. Momordica charantia, a nutraceutical approach for inflammatory related diseases. Front Pharmacol. 2019;10:486. 10.3389/fphar.2019.00486
10. Li Z, Xia A, Li S, Yang G, Jin W, Zhang M, et al. The pharmacological properties and therapeutic use of bitter melon (Momordica charantia L.). Curr Pharmacol Rep. 2020;6(3): 103–9. 10.1007/s40495-020-00219-4
11. Deng Z, Yuan C, Yang J, Peng Y, Wang W, Wang Y, et al. Behavioral defects induced by chronic social defeat stress are protected by Momordica charantia polysaccharides via attenuation of JNK3/PI3K/AKT neuroinflammatory pathway. Ann Transl Med. 2019;7(1):6–. 10.21037/atm.2018.12.08
12. Wen J-J, Li M-Z, Gao H, Hu J-L, Nie Q-X, Chen H-H, et al. Polysaccharides from fermented Momordica charantia L. with Lactobacillus plantarum NCU116 ameliorate metabolic disorders and gut microbiota change in obese rats. Food Funct. 2021;12(6):2617–30. 10.1039/D0FO02600J
13. Semiz A, Ozgun Acar O, Cetin H, Semiz G, Sen A. Suppression of inflammatory cytokines expression with bitter melon (Momordica Charantia) in TNBS-instigated ulcerative colitis. J Transl Inter Med. 2020;8(3):177–87. 10.2478/jtim-2020-0027
14. Zhang C, Huang Y, Li P, Chen X, Liu F, Hou Q. Ginger relieves intestinal hypersensitivity of diarrhea predominant irritable bowel syndrome by inhibiting proinflammatory reaction. BMC Compl Med Ther. 2020;20(1):279. 10.1186/s12906-020-03059-3
15. Hou Q, Huang Y, Zhu Z, Liao L, Chen X, Han Q, et al. Tong-Xie-Yao-Fang improves intestinal permeability in diarrhoea-predominant irritable bowel syndrome rats by inhibiting the NF-κB and notch signalling pathways. BMC Complement Altern Med. 2019;19(1):337. 10.1186/s12906-019-2749-4
16. Ng QX, Soh AYS, Loke W, Lim DY, Yeo W-S. The role of inflammation in irritable bowel syndrome (IBS). J Inflamm Res. 2018;11:345–9. 10.2147/JIR.S174982
17. Choghakhori R, Abbasnezhad A, Hasanvand A, Amani R. Inflammatory cytokines and oxidative stress biomarkers in irritable bowel syndrome: Association with digestive symptoms and quality of life. Cytokine. 2017;93:34–43. 10.1016/j.cyto.2017.05.005
18. Kumar S, Singh P, Kumar A. Targeted therapy of irritable bowel syndrome with anti-inflammatory cytokines. Clin J Gastroenterol. 2022; 15(1):1-10. 10.1007/s12328-021-01555-8
19. Guo D, Zhou J, Zhang M, Taximaimaiti R, Wang X, Wang H. Momordica Charantia polysaccharides attenuates MPP+-induced injury in Parkinson’s disease mice and cell models by regulating TLR4/MyD88/NF-κB patway. Int J Polym Sci. 2021;2021:5575636. 10.1155/2021/5575636
20. Cojocariu RO, Balmus IM, Lefter R, Ababei DC, Ciobica A, Hritcu L, et al. Behavioral and oxidative stress changes in mice subjected to combinations of multiple stressors relevant to irritable bowel syndrome. Brain Sci. 2020;10(11):865. 10.3390/brainsci10110865
21. Raish M. Momordica charantia polysaccharides ameliorate oxidative stress, hyperlipidemia, inflammation, and apoptosis during myocardial infarction by inhibiting the NF-κB signaling pathway. Int J Biol Macromol. 2017;97:544–51. 10.1016/j.ijbiomac.2017.01.074
22. He X, Cui L-H, Wang X-H, Yan Z-H, Li C, Gong S-D, et al. Modulation of inflammation by toll-like receptor 4/nuclear factor-kappa B in diarrhea-predominant irritable bowel syndrome. Oncotarget. 2017;8(69):113957–65. 10.18632/oncotarget.23045
23. Coëffier M, Déchelotte P, Ducrotté P. Intestinal permeability in patients with diarrhea-predominant irritable bowel syndrome: Is there a place for glutamine supplementation? Gastroenterology. 2015;148(5):1079–80. 10.1053/j.gastro.2015.02.057
24. Raish M, Ahmad A, Ansari MA, Alkharfy KM, Aljenoobi FI, Jan BL, et al. Momordica charantia polysaccharides ameliorate oxidative stress, inflammation, and apoptosis in ethanol-induced gastritis in mucosa through NF-kB signaling pathway inhibition. Int J Biol Macromol. 2018;111:193–9. 10.1016/j.ijbiomac.2018.01.008
25. Scalera A, Di Minno MN, Tarantino G. What does irritable bowel syndrome share with non-alcoholic fatty liver disease? World J Gastroenterol. 2013;19(33):5402–20. 10.3748/wjg.v19.i33.5402
26. Fan M, Lee JI, Ryu YB, Choi YJ, Tang Y, Oh M, et al. Comparative analysis of metabolite profiling of momordica charantia leaf and the anti-obesity effect through regulating lipid metabolism. Int J Environ Res Public Health. 2021;18(11):5584. 10.3390/ijerph18115584