
Download
REVIEW ARTICLE
Easy approach to detect cell immunity to COVID vaccines in common variable immunodeficiency patients
Yvelise Barriosa, Andrés Francoa, Cristina Alava-Cruzb, Ricardo Cuesta-Martinc, Carmen Camarac, Victor Matheub*
aDepartment of Immunology, Hospital Universitario de Canarias, San Cristóbal de La Laguna, Spain
bDepartment of Allergy, Hospital Universitario de Canarias, San Cristóbal de La Laguna, Spain
cDepartment of Immunology, Hospital Universitario La Paz, Madrid, Spain
Abstract
Background Patients with primary antibody deficiencies, such as Common Variable Immunodeficiency (CVID), have some problems to assess immune response after coronavirus disease (COVID) vaccination. Cutaneous delayed-type hypersensitivity (DTH) has the potential to be used as a useful, simple, and cheaper tool to assess T-cell (T lymphocyte) function.
Methods Seventeen patients with CVID, a rare disease, received two doses of the mRNA-based Pfizer-BioNTech COVID-19 vaccine. Humoral Immune Response (HIR) was determined by measuring specific immunoglobulin G (IgG) antibodies, and Cellular Immune Response (CIR) was evaluated using an ex vivo interferon-gamma release assay (IGRA) and in vivo by DTH skin test.
Results Two weeks after the second dose of the vaccine, 12 out of 17 CVID patients have high optical density (OD) ratios of specific anti-spike protein (S) IgG whereas five patients were negative or low. Ex vivo CIR was considered positive in 14 out of 17 S1-stimulated patients. Unspecific stimulation was positive in all 17 patients showing no T-cell defect. A positive DTH skin test was observed in 16 CVID patients. The only patient with negative DTH also had negative ex vivo CIR.
Conclusions The use of DTH to evaluate CIR was validated with an optimal correlation with the ex vivo CIR. The CIR after vaccination in patients with antibody deficiencies seems to have high precision and more sensitivity to antibodies-based methods in CVID.
Clinical Implications There is a remarkable correlation between cutaneous DTH and ex vivo IGRA after COVID vaccination. A COVID-specific skin DTH test could be implemented in large populations.
Capsule Summary Cutaneous delayed-type hypersensitivity has the potential to be used as a useful, simple, and cheaper tool to assess T-cell functioning.
Key words: Common Variable Immunodeficiency (CVID), rare disease, T-cell response, COVID vaccination, DTH, skin test, SARS-CoV-2, antibody deficiency
*Corresponding author: Victor Matheu, Department of Allergy, Hospital Universitario de Canarias, San Cristóbal de La Laguna, Spain. Email address: [email protected]
Received 13 January 2022; Accepted 9 March 2022; Available online 1 May 2022
Copyright: Matheu V, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Induction of cellular immunity after Severe Acute Respiratory Syndrome–CoronaVirus-2 (SARS-CoV-2) mRNA vaccines requires to be confirmed in patients with antibody deficiency.1 Ex vivo/in vitro cell-immune studies are troublesome and often not possible in low- to middle-size laboratories. For this reason, few studies have been published to answer this question in immunocompromised patients.2 Delayed-Type Hypersensitivity (DTH) responses are a component of type-IV hypersensitivity reaction category of cell-mediated immunity. Unlike type I–III, which involve various forms of antibody-mediated activities, only effector T cells and activated macrophages participate in DTH responses. These responses are often associated with host response to intracellular pathogens. In the search for T-cell (T lymphocyte) response targets, spike (S) protein is an exciting molecule to study in vivo response by DTH after natural infection3 and in vaccinated individuals.4 In this report, we present for the first time the results of this new application of DTH method to assess cellular immune responses in Common Variable Immunodeficiency (CVID) patients. Humoral and ex vivo cellular immune responses were also investigated in parallel to underline the biological significance of the obtained results.
The National COVID-19 Immunization Plan, organized by Health Public Plan, included primary immunodeficiency (PID) patients among the priority groups for administration of vaccine. CVID patients from this group who received two doses of the mRNA-based Pfizer-BioNTech COVID-19 vaccine 3 weeks apart were included. All of them were previously described as poor antibody responders in conventional vaccine diagnostic protocols. A positive control group with immunocompetent vaccinated individuals was included in the analysis.
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Hospital Universitario de Canarias. The study was approved by the Ethical Committee with code CHUC_2021_04. All included subjects received full information about procedures. Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from patient(s) to publish this paper.
In vivo cellular immune response
Delayed-type hypersensitivity skin test using receptor-binding domain (RBD) antigen was investigated in all participants 2 weeks after administration of the second dose of the vaccine. After signing informed consent, a trained professional administered 25-μL SARS-CoV-2 recombinant protein of RBD through intradermal testing (IDT) puncture in the volar part of the arm as described before.4 The patients were instructed to take photograph of the part of the arm at the agreed times for the late reading at 12, 24, and 48 h.
Humoral immune response
Serum samples were taken before administration of the first dose of the vaccine (day 0), before administration of the second dose (day 20), and 2 weeks after the second dose (day 35). Presence of specific immunoglobulin G (IgG) anti-S1 SARS-CoV-2 protein was detected using a commercially available method (Euroimmun, Lübeck, Germany) in all serum samples. optical density (OD) ratios above 0.8 were considered positive.
Ex vivo cellular immune response
An interferon-gamma release assay (IGRA) investigated the spike protein-specific T-cell responses 2 weeks after the second dose of the vaccine (day 35).5 The assay was performed using fresh whole blood collected and stimulated (37ºC, 24 h) either with the spike protein or unspecific mitogen, causing interferon (IFN)-gamma (γ) secretion from T cells. After this, an IFN-gamma ELISA (Euroimmun) was performed using supernatants. The range of positive levels was 0.4–31.86 international units (IU)/mL.
Statistics
The data were collected from Jamovi software and analyzed by the authors. Differences between the distributions of continuous variables were evaluated using 2-tailed Mann–Whitney U test. Differences at P ˂ 0.5 were considered as statistically significant.
Results
Demographic data of patients diagnosed with Common Variable Immunodeficiency (CVID) are shown in Table 1. There were 13 females (76%) and 4 males (24%) (mean age: 43.9 years; SD: 17) with a mean CD3 cell count of 1430 cells/μL (SD: 670 cells/μL) and a mean CD19 positive cells of 161 cells/μL (SD: 146 cells/μL). There were nine CVID patients (52%) with a CD19 positive cell count of less than 100 cells/μL.
Table 1 Demographic description of patients with CVID (#1–17).
| Patient | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 70 | 62 | 68 | 34 | 32 | 50 | 40 | 57 | 47 | 79 | 18 | 22 | 26 | 31 | 38 | 39 | 34 | |
| Gender | W | W | W | M | M | M | W | W | W | W | W | W | M | W | W | W | M | |
| total CD3 | 923 | 2477 | 3097 | 512 | 1374 | 1493 | 792 | 1450 | 1192 | 1273 | 2100 | 2200 | 1050 | 1084 | 1189 | 1345 | 760 | |
| total CD19 | 50 | 260 | 99 | 40 | 219 | 188 | 99 | 196 | 57 | 85 | 582 | 345 | 127 | 28 | 288 | 24 | 61 | |
| IGR A | Spike | 15 | 31,86 | 0,5 | 0 | 2,9 | 31,86 | 0,5 | 6,26 | 11,95 | 0,43 | 1,34 | 13,22 | 0,5 | 0,25 | 0,25 | 5,8 | 19 |
| Unspecific | 31,86 | 31,86 | 31,86 | 31,86 | 4,7 | 31,86 | 12 | 31,86 | 31,86 | 31,74 | 31,86 | 31,86 | 9,02 | 31,67 | 31,67 | 31,86 | 31,67 | |
| DTH | 24 h | 10 | 20 | 21 | 0 | 14 | 14 | 3 | 22 | 26 | 6 | 21 | 21 | 22 | 24 | 10 | 12 | 24 |
| 48 h | 14 | 20 | 26 | 0 | 17 | 14 | 6 | 18 | 18 | 0 | 24 | 22 | 24 | 26 | 6 | 19 | 20 | |
| IgG Spike | 5.1 | 5.8 | 5.8 | 1.4 | 5 | 3 | 5.7 | 3 | 5.9 | 0.4 | 5.1 | 6 | 0.6 | 0.5 | 6 | 0.5 | 6.1 | |
| Controls | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | |
| Age | 68 | 60 | 66 | 35 | 31 | 50 | 40 | 56 | 47 | 75 | 20 | 23 | 27 | 30 | 36 | 38 | 36 | |
| Gender | W | W | W | M | M | M | W | W | W | W | W | W | M | W | W | W | M | |
| DTH | 24 h | 24 | 10 | 22 | 8 | 26 | 22 | 19 | 16 | 20 | 19 | 27 | 14 | 14 | 22 | 22 | 15 | 24 |
| 48 h | 29 | 12 | 20 | 16 | 10 | 16 | 34 | 16 | 14 | 14 | 16 | 12 | 12 | 6 | 14 | 14 | 20 | |
| IgG Spike | 6.2 | 7.8 | 7.9 | 6.4 | 7.5 | 7.6 | 7.9 | 6 | 7.5 | 7.6 | 6,2 | 7 | 6,2 | 6,5 | 6,2 | 5,7 | 7.6 | |
Notes: DTH response diameter values are in millimeter at 24 and 48 h after IDT puncture.
In vitro response (IFN-gamma levels) after stimulation with spike protein of SARS-CoV-2 and to a nonspecific mitogen.
Total CD3 and CD19 counts and specific IgG antibody levels to spike protein (OD ratio) in 17 CVID patients.
Shaded cells demonstrate description of 17 immunocompetent matched controls with results of DTH (brown color) and specific level of IgG antibodies to spike protein.
In vivo cellular immune response
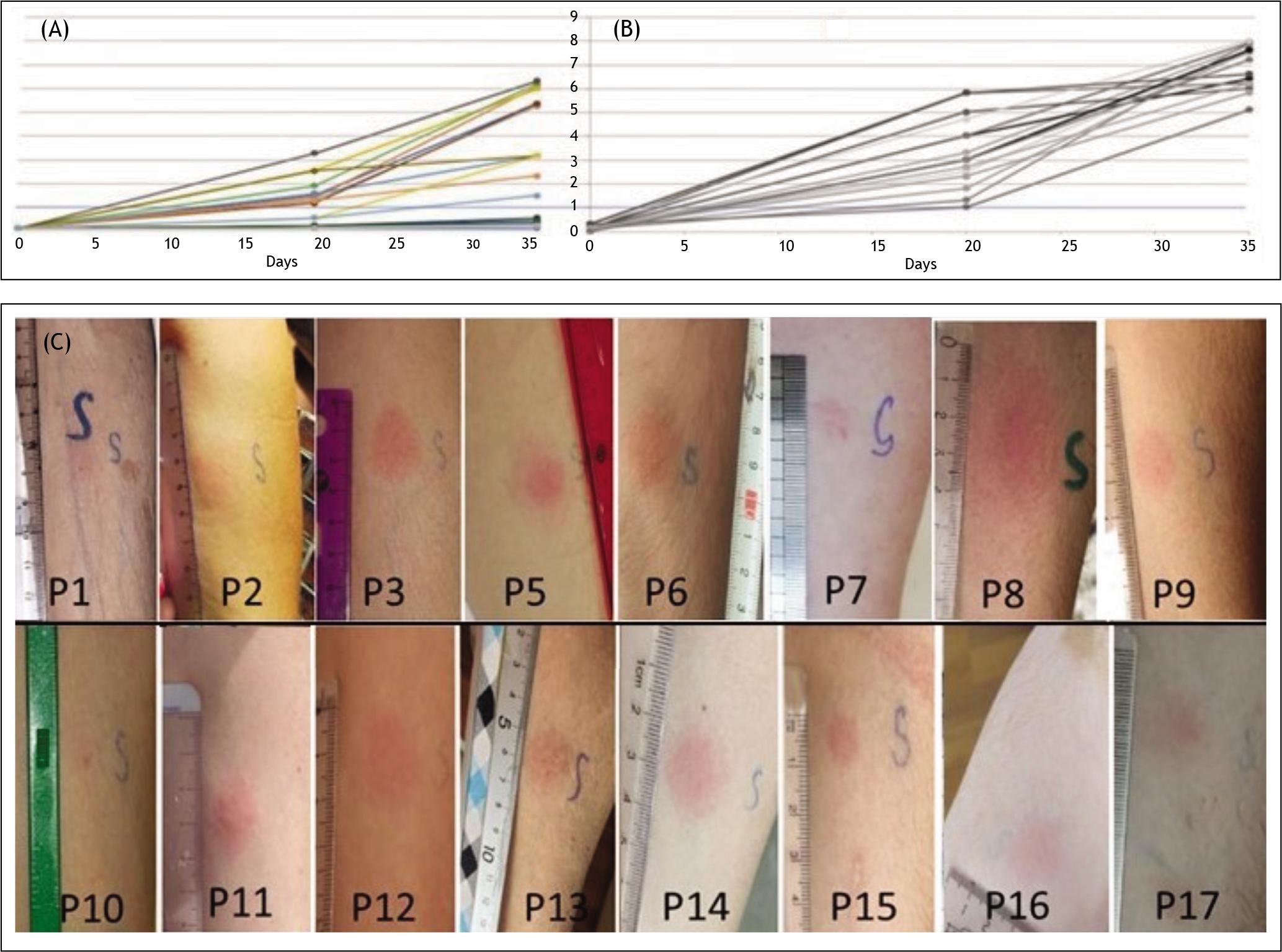
A positive DTH skin test was observed in 16 CVID patients (Figure 1). Only one patient had negative DTH and ex vivo IGRA (patient #4). Two other patients (patient #14 and 15) with negative IGRA demonstrated a positive DTH skin test (Figure 1), and one of them also had high specific anti-S1 IgG (patient #15). Patient with a positive but weak DTH response corresponded to the patient who had a less intense IFN-gamma secretion after S1-stimulation (patient #10). The control group of vaccinated and immunocompetent individuals had both potent humoral and cellular responses (Figure 1B).3
Figure 1 (A) Levels of specifi c IgG anti-S1 SARS-CoV-2 in 17 patients with CVID on day 0 (day of 1st dose of vaccine), day 20 (day before 2nd dose of vaccine), and day 35 (14 days after 2nd dose of vaccine). (B) Levels of specifi c IgG anti-S1 SARS-CoV-2 in 17 immunocompetent patients. There was a statistically signifi cant difference in the fi nal points between both groups (P ˂ 0.001). (C) Images of the photographs taken and sent by the patients showing results after 48 h of IDT puncture in 16 CVID positive patients.
Humoral immune response
Two weeks after the second dose of the vaccine, 12 out of 17 CVID patients (71%) had high specific anti-S protein IgG whereas 5 patients (29%) were negative (n = 4) or low positive (n = 1). Results of specific IgG anti-S1 antibodies in 17 immunocompetent patients matched in age (mean: 43 years, SD: 16.5) and gender (4:13—male:female ratio) and were signifi cantly higher on day 35 (P ˂ 0.001) than CVID patients (Figure 1 and Table 1). No patient had suffered from SARS-CoV-2 infection with negative IgG anti-N antibodies before or during the study process.
Ex vivo cellular immune response
Ex vivo IGRA was found positive ( ˃ 0.4 IU/mL) in 14 out of 17 S1-stimulated patients (Table 1). Three patients were considered negative for IGRA after S1-stimulation (patient #4, 14, and 15) but positive after mitogen-unspecifi c stimulation, establishing a good cellular function in these patients. IGRA after unspecifi c stimulation was positive in all 17 patients (Table 1).
Discussion
Massive vaccination to combat SARS-CoV-2 has proven extremely successful, potentially controlling the COVID-19 pandemic, limiting the viral spread, and preventing severe illness. In order to demonstrate the effi cacy of the vaccine, it is vital to answer questions regarding humoral and cellular responses generated in vaccinated individuals. Data regarding the effectiveness of anti-SARS-CoV-2 vaccine is especially required in immuno-compromised populations because antibody production defects are the more frequently observed, precluding any antibody-based method to assess humoral responses to the vaccine. 6 In fact, 5 out of 17 CVID patients in this study did not produce any specifi c anti-S protein IgG or low levels whereas 14 of the 17 patients were considered positive for ex vivo cellular immune responses, and 16 of the 17 patients demonstrated a positive in vivo DTH skin test, indicating the relevance of cellular assays to fi ll this gap in immunological information. This is the fi rst study evaluating in vivo cellular immune response in vaccinated immunodefi cient patients. These in vivo results were compared with ex vivo cell immune responses to identify correlation between these two approaches to assess the cellular immune status of this CVID population, where it was speculated to have the worst humoral immune response to the vaccine.7 However, there were several limitations to this study. The main limitation was the small sample size; CVID is a rare disease, and our reference population comprised less than 1 million inhabitants. In addition, some patients not included in the studies followed different vaccination guidelines. Hence, it would have been desirable to expand to other types of primary immunodeficiencies
We had a remarkable correlation between these two methods that could overcome the inconvenience of an ex vivo/in vitro assessment, thus making more accessible these basic studies to understand the immunological response in a large group of patients. In the future, a COVID-specific DTH test could be implemented in large populations to make individualized recommendations about requirement to boost immune responses in specific groups of patients
Patent
Yvelise Barrios and Victor Matheu had filed provisional (79241/P8547) Utility Model application related to DTH tests for cellular immunity against SARS-CoV-2.
Author Contributions
Conceptualization: Victor Matheu and Yvelise Barrios. Methodology: Andrés Franco and Cristina Alava-Cruz. Validation: Andrés Franco and Cristina Alava-Cruz. Formal analysis: Andrés Franco. Investigations: Cristina Alava-Cruz and Carmen Camara. Resources: Victor Matheu. Writing— original draft preparation: Yvelise Barrios and Victor Matheu. Writing—review and editing: Yvelise Barrios and Victor Matheu. Visualization: Yvelise Barrios and Victor Matheu. Project administration: Yvelise Barrios. Funding acquisition: Victor Matheu. All authors read and agreed to the final published version of the manuscript.
Funding
This research was partially self-funded and partially funded by Spanish Society of Allergy and Clinical Immunology (SEAIC 2021 Beca20A4).
Conflict of Interest
Yvelise Barrios has been subsequently to the elaboration of this work, scientific advisor of BioVaxys. Rest of authors declared that they had no competing interests. Pfizer had no role in designing of the study; in collection, analyses, or interpretation of data; in writing of the manuscript; or in decision to publish the results.
Acknowledgments
The authors thank patients and immunology laboratory technicians (Tamara MJ Placer, Gloria Camacho, María Romera, Montserrat Padilla).
REFERENCES
1. Sandbrink JB, Shattock RJ. RNA vaccines: A suitable platform for tackling emerging pandemics? Front Immunol. 2020 Dec 22;11:608460. 10.3389/fimmu.2020.608460. PMid: 33414790; PMCID: PMC7783390.
2. Hagin D, Freund T, Navon M, Halperin T, Adir D, Marom R, et al. Immunogenicity of Pfizer-BioNTech COVID-19 vaccine in patients with inborn errors of immunity. J Allergy Clin Immunol. 2021 Jun 1:S0091-6749(21)00887-3. Epub ahead of print. 10.1016/j.jaci.2021.05.029. PMid: 34087242; PMCID: PMC8168345.
3. Barrios Y, Franco A, Sanchez-Machin I, Poza-Guedes P, Gonzalez-Perez R, Matheu V. A novel application of delayed-type hipersensitivity reaction to measure cellular immune response in SARS-CoV-2 exposed individuals. Clin Immunol. 2021 May;226:108730. Epub 2021 Apr 16. 10.1016/j.clim.2021.108730. PMid: 33865990; PMCID: PMC8049849.
4. Barrios Y, Franco A, Sánchez-Machín I, Poza-Guedes P, González-Pérez R, Matheu V. The beauty of simplicity: Delayed-type hypersensitivity reaction to measure cellular immune responses in RNA-SARS-Cov-2 vaccinated individuals. Vaccines. 2021;9:575. 10.3390/vaccines9060575.
5. Murugesan K, Jagannathan P, Pham TD, Pandey S, Bonilla HF, Jacobson K, et al. Interferon-gamma release assay for accurate detection of SARS-CoV-2 T cell response. Clin Infect Dis. 2020 Oct 9:ciaa1537. Epub ahead of print. 10.1093/cid/ciaa1537. PMid: 33035306; PMCID: PMC7665338.
6. Hellerstein M. What are the roles of antibodies versus a durable, high quality T-cell response in protective immunity against SARS-CoV-2? Vaccine X. 2020 Dec 11;6:100076. Epub 2020 Aug 28. 10.1016/j.jvacx.2020.100076. PMid: 32875286; PMCID: PMC7452821.
7. Sauer K, Harris T. An effective COVID-19 vaccine needs to engage T cells. Front Immunol. 2020 Sep 28;11:581807. 10.3389/fimmu.2020.581807. PMid: 33117391; PMCID: PMC7549399