
Download


ORIGINAL ARTICLE
Survey of immunopharmacological effects of botulinum toxin in cell signaling of bronchial smooth muscle cells in allergic asthma
Chao Chenga, Entezar Mehrabi Nasabb, Seyyed Shamsadin Atharic*
aDepartment of Pediatrics, Suzhou Science and Technology Town Hospital, Suzhou, Jiangsu China
bDepartment of Cardiology, School of Medicine, Tehran Heart Center, Tehran University of Medical Sciences, Tehran, Iran
cDepartment of Immunology, School of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran
Abstract
Background Asthma is a lung disease that has influenced more than 350 million people worldwide. Airway smooth muscle (ASM) spasm leads to airway hyperresponsiveness (AHR) and bronchial obstruction, which are clinical manifestations of an asthma attack. Botulinum toxin (BTX) is a bacteria toxin that acts as muscle relaxant and may have therapeutic effects on AHR and asthma.
Objective In this study, the effect of BTX on AHR and related gene expressions was evaluated.
Material and Methods An asthma mice model was developed which was treated with BTX in two ways: intranasally (IN) and via nebulization (N) (0.01, 0.1, and 1 U/mL and 10 U/mL, respectively) on days 25, 27 and 29. AHR was evaluated on days 24, 26, 28, and 30, and gene expressions were evaluated for TrkA, TrkB, M1–M5, α7nAChR, TNF-α, and extracellular signal-regulated kinase 2 (ERK2) proteins. For histopathology of the lungs, perivascular and peribronchial inflammation, production of mucus, and goblet cell hyperplasia were studied.
Results On day 24, treatment with BTX (for all doses) had no significant effect on AHR, but on days 26 and 28, AHR was decreased and this continued up to day 30 for all treated groups. Treatment with BTX had no significant effect on the gene expressions of TrkA, TrkB, M1–M5, α7nAChR, TNF-α, and ERK2 proteins, perivascular inflammation, peribronchial inflammation, hyperplasia of the goblet cell and production of mucus. Besides, mice administered with 10 mg/mL BTX perished. The BTX therapy controlled asthma attacks by decreasing AHR and relaxation of ASMs.
Conclusion However, BTX had no significant effect on airway inflammation and production of mucus. While using BTX, it is necessary to prescribe safe doses in order to prevent adverse reactions.
Key words: muscle, paralysis, toxin, therapy, signal
*Corresponding author: Seyyed Shamsadin Athari, Department of Immunology, School of Medicine, Zanjan University of Medical Sciences, Zanjan, Iran. Email address: [email protected]
Received 25 November 2021; Accepted 27 January 2022; Available online 1 May 2022
Copyright: Shamsadin Athari S, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Significance of this study
What is already known about this subject?
-
BTX had effect on airway obstruction and spasm.
-
BTX had no effect on hyperplasia of the goblet cell and mucus production.
-
BTX with 10 mg/mL dose had toxicity for the evaluated mice.
What are the new findings?
-
BTX had effect on AHR on days 26 and 28.
-
BTX decreased AHR.
-
Treatment with BTX had no effect on inflammation.
How can it impact clinical practice in the foreseeable future?
-
BTX therapy controlled asthma attacks via decreasing AHR and relaxation in ASMs.
Introduction
Asthma is one of the main lung diseases that has affected more than 350 million people worldwide and results in maximum deaths, especially in developed countries. Spasm of smooth muscle cells and airway inflammation are the main teasers in asthma. Main clinical manifestations of asthma include wheezing, shortness of breath, cough, and chest tightness. Airway inflammation leads to remodeling of the bronchi in the long period, but airway smooth muscle (ASM) spasm results in airway hyperresponsiveness (AHR) and bronchial obstruction, which are acute manifestations of an asthma attack. Asthma is controllable and new therapies are more effective than previous treatments in preventing or averting clinical manifestations. There are two groups of anti-asthma drugs, which include short- acting and long-acting medicates. While short-acting drugs have quick effect and mainly inhibit ASM spasm and airway obstruction, long-acting drugs have continuous effect and mainly inhibit eosinophilic airway inflammation and obstruction.1–3
Airway hyperresponsiveness is a characteristic feature of asthma, and with contraction of ASM it leads to excessive narrowing of airway in response to stimulators and asthma manifestations (cough, wheezing, and breathlessness). However, acute asthma is difficult to control and requires a novel therapeutic approach, which includes AHR inhibition.4,5 AHR is important to recognize the severity of asthma, as seasonal exposure to allergens can alter severity of AHR. However, anti-asthma therapy intensely improves AHR. The exaggerated airway narrowing in asthma highlights the role of ASM in AHR manifestations. Bronchoconstriction, in part, is due to constriction of ASM surrounding the airway. Hence, increased contractility of ASM has been stated as a principal cause of AHR.6,7
Botulinum toxin (BTX) as a bacteria exotoxin is produced by Clostridium botulinum. It is a valuable therapeutic tool for treating overactivity and hypersecretory of smooth muscles. BTX contains heavy and light chains linked by a disulphide bond. After accessing the target tissue, heavy chain binds to glycoprotein structures on cholinergic nerve terminals and then internalized. Light chain binds to soluble N-ethylmaleimide-sensitive factor attachment protein receptor (SNARE) complex with high specificity, after which it proteolytically cleaves specific target proteins, prevents acetylcholine vesicle docking on inner surface of the presynaptic membrane, paresis skeletal, or smooth muscles.8 Therefore, new generation of treatments are necessary. There are some bio-toxins such as BTX which can be used as muscle paralyzing and relaxant agents and may have a therapeutic value in problems such as asthma. Therefore, in this study, the effect of BTX on AHR and relaxation of ASM, as well as related gene expression, was evaluated.
Material and methods
Modeling and Treatment schedule
Male BALB/c mice (n = 100) were acclimatized in standard laboratory conditions and were allocated in 10 groups. In 9 groups, allergic asthma was induced by ovalbumin (OVA) as shown in Figure 1. Briefly, for sensitization, mice were injected OVA with alum intraperitoneally, and for a challenge, the animals were nebulized with OVA aerosols for 30 min/day. The 10th group (negative control group) was sensitized and challenged with phosphate buffer solution (PBS). Eight of the nine OVA-received groups were treated with BTX.
Figure 1 Animal asthma model of BALB/c mice was sensitized by intraperitoneal injection of OVA with alum and then challenged by inhalation of OVA aerosols for 30 min/day. Mice were treated with BTX intranasally and via nebulization on days 25, 27, and 29. AHR was measured on days 24, 26, 28, and 30, and sampling was done on day 31.
It was administered in two ways: (1) diluted in normal saline and administered intranasally, and (2) aero solized as a nebulized solution (0.01, 0.1, 1, and 10 U/mL intra-nasally and via nebulization) on days 25, 27, and 29. The ninth OVA-challenged group received no treatment (positive control group). On days 24, 26, 28, and 30, AHR measurements were made and on day 31, lung tissue sampling was exercised.
Methacholine (MCh) challenge test for AHR measurement
In order to determining AHR, MCh challenge test was used by determining enhanced pause (Penh value). After anesthetizing, the mice were tracheotomized, and then exposed to aerosolized MCh with a series of doubling concentrations (0, 1, 2, 4, 8, 16, and 32 mg/mL).
Real-time polymerase chain reaction (RT-PCR)
In lung cells, total RNA was extracted and reverse- transcribed to complementary DNA (cDNA). Quantitative RT-PCR was performed for expression of target genes. Glyceraldehyde 3-phosphate dehydrogenase (GAPDH) was used as an internal control gene. The used primer sequences were (5’-3’); GAPDH, F: TGTTCCTACCCCCAATGTGT, R: GGTCCTCAGTGTAGCCCAAG; TrkA, F: TCCTTCTCGCCAGTG GACGGTAA, R: AGTGCCTTGACAGCCACGAGCAT; TrkB, F: TGA CGCAGTCGCAGATGCTG, R: TTTCCTGTACATGATGCTCTCTGG; M1, F: TCCCTCACATCCTCCGAAGGTG, R: CTTTCTTGGTGGG CCTCTTGACTG; M2, F: CTGGAGCACAACAAGATCCAGAAT, R: CC CCCTGAACGCAGTTTTCAGT;M3, F: GCAAGACCTCTGACACCAA CT, R: AGCAAACCTCTTAGCCAGCG; M4, F: CGGCTACTGGCT CTGCTACGTCAA, R: CTGTGCCGATGTTCCGATACTGG; M5, F: TA GCATGGCTGGTCTCCTTCA, R: CGCTTCCCGACCAAGTACTG; α7nAChR, F: GTCGTGTGTGGTCGTTTG3', R: ATCACCTCACT CTCATCCTG; TNF-α, F: GCCTCTTCTCATTCCTGCTTG, R: CTGA TGAGAGGGAGGCCATT; ERK2, F: GGAGCAGTATTATGACCCA AGTGA, R: TCGTCCACTCCATGTCAAACT.
Histopathology
Lung tissues (on day 31) were isolated, and after producing slide sections, were stained with hematoxylin and eosin (H&E), periodic acid shiff (PAS), and alcian blue-periodic acid shiff (AB-PAS). Slides were evaluated for perivascular and peribronchial eosinophilic inflammation, mucus production, and goblet cell hyperplasia.
Statistical analysis
The results were shown as mean values ± SD. The SPSS (version 20) software was used for analysis. Paired t-test was used to analyze differences between treated and untreated groups, and P ˂ 0.05 was taken as significant. The graphs were performed by GraphPad Prism (version 6).
Result
Survival
Mice of two asthma groups that were administrated the first dose of BTX, 10 mg/mL, intranasally and thru nebulization perished. On day 25, animals of IN1 group (that received 1 mg/mL intranasally) and on day 29, animals of N1 group (that received 1 mg/mL via nebulization) perished.
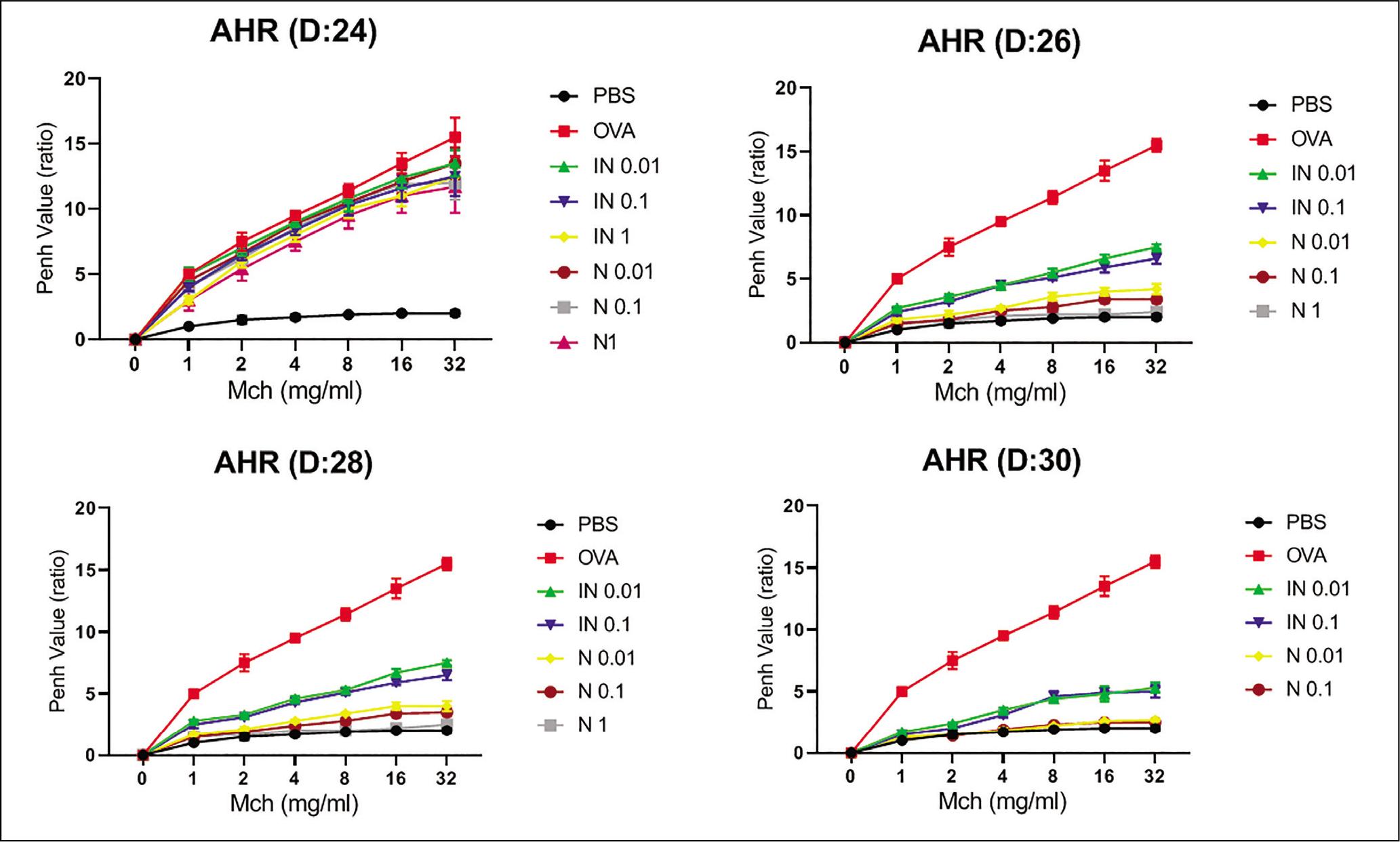
Airway Hyperresponsiveness
The Penh value was significantly (P ˂ 0.05) increased in the untreated asthma group compared to the PBS-challenged group for all concentrations of MCh. Increased AHR in asthmatic mice had no significant changes (P ˃ 0.05) on day 24 for all concentrations of MCh (given 32 mg/mL of MCh on day 24; OVA: 15.5 ± 1.5, intranasal 0.01: 13.5 ± 1, IN 0.1: 12.5 ± 1.3, IN 1: 12.5 ± 1.5; via nebulization 0.01: 13.5 ± 1.2, 0.1: 12 ± 1.3, N 1: 11.7 ± 2) (Figure 2). All treated groups demonstrated significant (P ˂ 0.05) decreasing of AHR for the same concentrations of MCh on days 26 and 28 (Figure 2). Decrease in AHR continued up to day 30 for all treated groups and demonstrated significant (P ˂ 0.05) decrease compared to the untreated OVA group for all concentrations of MCh (given 32 mg/mL of MCh on day 30, OVA: 15.5 ± 0.5, intranasal 0.01: 5.3 ± 0.4, IN 0.1: 5 ± 0.5, nebulization 0.01: 2.7 ± 0.1, N 0.1: 2.5 ± 0.2) (Figure 2).
Figure 2 To determine AHR, MCh challenge test was performed by determining Penh value on days 24, 26, 28, and 30. The mice were tracheotomized and exposed to MCh with a series of doubling concentrations (0, 1, 2, 4, 8, 16, and 32 mg/mL).
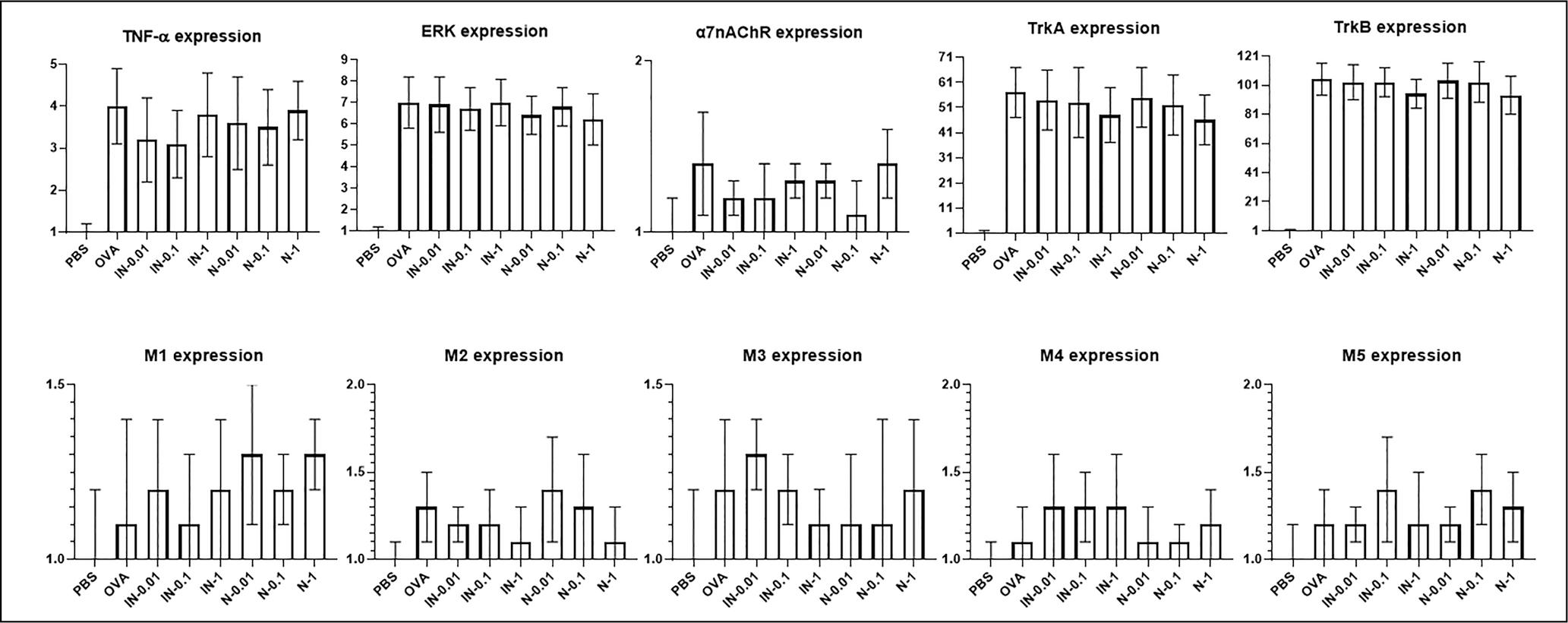
RT-PCR
The gene expressions of TrkA, TrkB, M1–M5, α7nAChR, TNF-α, and ERK2 proteins were significantly (P ˂ 0.05) increased in asthma groups compared to the PBS-challenged group. Treatment with various doses of BTX intranasally and via nebulization had no significant effect (P ˃ 0.05) on the expressions of these genes compared to the untreated asthma group (Figure 3).
Figure 3 To determine gene expression after extraction of total RNA, the cDNA was synthesized and quantitative RT-PCR was performed for the gene expressions of TrkA, TrkB, M1–M5, α7nAChR, TNF-α, and ERK2 proteins.
Histopathology
In the untreated asthma group, eosinophilic inflammation in and around vascular (3.2 ± 0.4) and bronchial (3.7 ± 0.2) smooth muscles, production of mucus (3.3 ± 0.3), and the goblet cell hyperplasia (3.4 ± 0.5) were significantly (P ˂ 0.05) increased compared to the respective elements of PBS-challenged group (0.5 ± 0.2, 0.5 ± 0.1, 0.6 ± 0.1, and 0.5 ± 0.2, respectively). Treatment with 0.01, 0.1, and 1mg/mL BTX intranasally and via nebulization had no significant (P ˃ 0.05) effect on the perivascular and peribronchial eosinophilic inflammation, hyperplasia of the goblet cell, and production of mucus compared to untreated asthma group (Figure 4).
Figure 4 Lung tissues were isolated and slide sections were produced. These were stained with H&E, PAS, and AB-PAS and evaluated for perivascular and peribronchial eosinophilic inflammation, mucus production, and goblet cell hyperplasia.
Discussion
Asthma attack is developed by two essential factors, inflammation and bronchoconstriction, and is mediated by ASM contraction. Airway inflammation starts slowly, but quick attack is initiated by contraction of ASM. Inhibition of bronchoconstriction controls asthma attack and decreases aftermath morbidity and mortality. Initiated bronchoconstriction because of ASM contraction in asthma reduces air flow and decreasing responsiveness of the ASM in airways will attenuate the bronchoconstrictor response in asthma and can be achieved effective pharmacotherapy.3,8
In asthma, ASMs, key to bronchoconstriction, have muscarinic receptors whereas nicotinic acetylcholine receptors (nAChRs) are found only on airway neurons. It has been shown that α7 subunit of nAChR is expressed in ASM cells can be modulated by exposure to pro-inflammatory cytokines such as TNFα and IL-13. Classically, nicotine acts via nAChRs, and in ASMs, contractility involves muscarinic receptors. Allergy in asthma increases ASMs Ca2+ and response to bronchoconstrictor agonists such as acetylcholine (ACh). Effect of ACh on ASM is usually associated with muscarinic receptors, while nAChR is generally considered to acts as Ca2+ channels on pre-ganglionic neurons.9–11 On the other hand, TNF-α and IL-13 are attributed to increased CD38-mediated calcium release.12 Also, TNF-α induces muscarinic receptor density, increases its activity as well as the amount of G-proteins in ASM, and may also modulate β2-adrenergic function.13 On day 24, without BTX treatment via intranasal and nebulization, no significant change on AHR was observed, but on days 26 and 28, BTX could significantly decrease AHR for all concentrations of MCh. Decrease in AHR continued up to day 30 for all treated groups, and significant decreasing trend was observed compared to untreated asthma group for all concentrations of MCh. In addition, decrease in AHR on day 30 had a significant difference compared to BTX-treated groups on days 26 and 28. This demonstrated that treatment with BTX in asthma could control airway obstruction and AHR, and may stop breathlessness in asthma mice. Asthma induction period in this study had two stages, that is, sensitization and challenging, and challenging had several stages that include OVA solution nebulization on days 24, 26, 28, and 30. BTX was not used before day 24, and therefore AHR was not controlled, but 24 h before days 26, 28, and 30 (i.e. on days 25, 27, and 29), asthmatic mice were treated with BTX, and next day, AHR was controlled and reduced significantly compared to day 24. This demonstrated that BTX could control AHR. BTX could control AHR in same day (that was used; for example in day 25, 27 or 29), it is unclear.
In normal airways, ASMs regulate the airway caliber, bronchomotor tone, and assist in mucus motility and airways contraction. β2-adrenoceptor agonists or muscarinic antagonists modulates the contractile function of ASMs.13
AHR, as an airways predisposition to excessive narrowness in response to stimuli, is considered an asthma cardinal feature. Presence of AHR is associated with decline in lung functioning, thereby increasing risk of asthma development and persistence to wheeze. However, increased contractility of ASM is the principal cause of AHR, which is also influenced by β2-adrenergic receptor genotype. On the other hand, in asthma, ASM contraction is altered by actin– myosin cross-bridges and activity of myosin light chain kinase (MLCK) and myosin light chain phosphatase (MLCP). Hypertrophy of constructed ASM and changes in extracellular matrix composition lead to airway remodeling, and therefore AHR has a correlation with bronchoconstriction and airways wall thickening.7,14,15 Prevention of bronchoconstriction potentially reduces severity of asthma, and BTX allows chemical denervation transient of ASM. BTX acts to weaken muscles by preventing acetylcholine vesicle docking of the presynaptic membrane (on the inner surface), which causes chemical denervation and paresis of smooth or skeletal muscles. Duration of BTX effect on skeletal muscles was estimated as 3–5 months. Hence, use of BTX to treat asthma is worth exploring. BTX can be administrated in the following three ways: (1) intranasally, trans- tracheally, or intratracheally via bronchoscopy, (2) injecting smooth muscles, and (3) aerosolized as a nebulized solution.8 The first dose of BTX decreased AHR (on day 26), but since 1 day passed in measuring the time, BTX had weak effect on ASMs. However, on day 30, most of the BTX doses had affected ASMs. Hence, the best effect of BTX on AHR was observed on day 30, and it demonstrated a significant difference in comparison to effect on AHR on day 26. In all treated groups, if BTX doses were increased, AHR was decreased more than the lower dose. Although duration of effect of BTX on skeletal muscles has been estimated as 3–5 months, no data exist about BTX effect on respiratory smooth muscles, and we also could not determine this duration.
Vocal Cord Dysfunction (VCD) is a respiratory problem in which the vocal cord restricts airflow by being blocked during inspiration, leading to coughing, shortness of breath, wheezing, and tightness of the chest. This problem is often misdiagnosed as asthma and treated accordingly. It has been observed that steroids used in asthma therapy are not beneficial in treating VCD. However, it is suggested that BTX relaxes the thyroarytenoid muscles surrounding the vocal cords, resulting in improved airflow.16,17 BTX is a neurotoxin comprising heavy and light chains. The heavy chain binds to specific neuronal ecto-acceptor, and the light chain cleaves synaptosomal-associated protein having a molecular weight of 25 kD (SNAP-25), inhibits synaptic exocytosis, disables neural transmission, and blocks release of acetylcholine.18 BTX has therapeutic effects on allergic rhinitis, particularly in patients whose clinical manifestations are not controlled with standard treatment. BTX has demonstrated maximum effect in rhinorrhea compared to other manifestations, and its effect on the nasal cavity occurs by inhibition of acetylcholine release from the cholinergic nerve in the nasal mucosa and the preganglionic cholinergic nerve in the sphenopalatine ganglion, and induction of apoptosis in the nasal gland. BTX acts by cleaving SNAP-25 and altering SNAP-5 to regulate exocytosis.19,20 We administrated BTX via intranasal and nebulizing routes. It was observed that the same concentration of BTX had varying effects if administered via different routes. If the same concentration and dose of BTX was used as a nebulizer, it had a strong effect to control AHR compared to intra-nasal route of administration.
Mild dose of purified BTX attenuates chronic pneumonia, dyspnea, cough, acute respiratory failure, and neurological deficits that are recognized as the clinical manifestations of COVID-19. Therapeutic BTX improves oxygen supply, thereby improving the survival rate, which can also be considered as a potent treatment for COVID-19 patients.21 In our study, asthmatic mice died after they were given the first dose of BTX (10 mg/mL) via intranasal and nebulization, and some groups the animals died even after receiving 1 mg/mL of BTX. It could be due to BTX affecting the respiratory system and breathing-related muscles that lead to paralysis and muscle relaxation. Therefore, BTX must be used with care for treating asthma and controlling AHR, and a safe dose of BTX must be determined beforehand. It is a strong treatment to control AHR and asthma, but can lead to respiratory paresis and death in asthmatic patients. Besides, we could not determine the safe dose of BTX to control AHR and airway obstruction.
nAChRs are of muscle and neuronal types,22,23 and extracellular signal-regulated kinase (ERK), as effector kinase, is involved in signaling pathways of multiple essential cell processes such as survival, proliferation, and differentiation.24,25 TrkA is a receptor tyrosine kinase and activated by nerve growth factor (NGF) and auto-phosphorylation. Since TrkA receptor is expressed on ASMs, it may have an important function in asthma. However, NGF expression is increased in various allergic manifestations, and activation of TrkA receptor by NGF causes its internalization mediated by clathrin-dependent pathways, followed by lysosomal degradation. Activation of TrkA in ASMs increases TrkA expression and increased pathophysiological consequences. Therefore, TrkA receptor is an interesting target in the development of new therapeutic approaches for allergic asthma.26 Treatment with BTX intranasally and nebulization in asthma mice had no significant effect on the gene expressions of TrkA, TrkB, M1–M5, α7nAChR, and TNF-α proteins, perivascular inflammation, peribronchial inflammation, hyperplasia of the goblet cell, and production of mucus compared to the untreated asthma group mice.
Allergo-immune responses are main reasons of allergic asthma pathophysiology, and these responses can be initiated in local lymph nodes of the respiratory system. Sometimes, environmental factors lead to dysregulation of lymph nodes strictures and immune responses. These responses and related bio-factors can have direct and indirect effect on airway, and therefore harnessing of these responses is necessary.1,27,28 Allergic asthma pathophysiology is airway eosinophilic inflammation, airway hyper- reactivity, and bronchial obstruction. In our study, BTX had no effect on the eosinophilic inflammation of airway, and also it could not control peribronchial and perivascular eosinophilic inflammation. Therefore, it could not control chronic pathology of asthma and may have no effect on control or prevention of airway remodeling.
Botulinum toxin therapy controls asthma by decreasing AHR and induction of ASM relaxation. It could be used via nebulization to have local effect and relaxation of ASMs, but it has no significant effect on inflammation and mucus production. In addition, in using of BTX, safe dose and prevention of adverse reactions are necessary. At the least, long-term use of BTX may produce anti-BTX antibodies and clinical resistance, which must be noted. In addition, we could not study the effect of BTX on chronic asthma and airway remodeling. The pharmacokinetics and pharmaco-dynamics of BTX on respiratory epithelium required more clarity.
Ethical Approval
All methods and protocols of this study were approved by the ethics committee of animal house of ix.med.vet.dep, 2021 (No. IX.MED.VET.DEP.REC.2021.3200002.2).
Conflict of Interest
There were no conflicts of interest to declare.
Author Contributions
Chao Cheng and Seyyed Shamsadin Athari supervised the study. Chao Cheng, Entezar Mehrabi Nasab, and Seyyed Shamsadin Athari participated in the design, evaluation, and result analysis of this study. All authors approved the final submitted version of manuscript.
Acknowledgements
The authors are thankful to Drs. Sum and Kalania.
REFERENCES
1. Atharia SS, Athari SM. The importance of eosinophil, platelet and dendritic cell in asthma. Asian Pac J Trop Dis. 2014;4(1):S41–7. 10.1016/S2222-1808(14)60413-8
2. Jiang J, Nasab EM, Athari SM, Athari SS. Effects of vitamin E and selenium on allergic rhinitis and asthma pathophysiology. Respir Physiol Neurobiol. 2021;286:103614. 10.1016/j.resp.2020.103614
3. Athari SM, Nasab EM, Athari SS. Study effect of Ocimum basilicum seeds on mucus production and cytokine gene expression in allergic asthma mice model. Revue Française d’Allergologie 2018; 58(7):489–93. 10.1016/j.reval.2018.08.003
4. Huang S-J, Lin L-L, Chen L-C, Ou L-S, Yao T-C, Tsao K-C, et al. Prevalence of airway hyperresponsiveness and its seasonal variation in children with asthma. Pediatr Neonatol. 2018;59:561–6. 10.1016/j.pedneo.2018.01.005
5. Wang Z, Liu B, Zhu J, Wang D, Wang Y. Nicotine-mediated autophagy of vascular smooth muscle cell accelerates atheros clerosis via nAChRs/ROS/NF-κB signaling pathway. Atherosclerosis. 2019;284:1–10. 10.1016/j.atherosclerosis.2019.02.008
6. Matsuda M, Doi K, Tsutsumi T, Inaba M, Hamaguchi J, Terada T, et al. Adoptive transfer of type 1 regulatory T cells suppressed the development of airway hyperresponsiveness in ovalbumin-induced airway inflammation model mice. J Pharmacol Sci. 2019;141:139–45. 10.1016/j.jphs.2019.10.004
7. Chapman DG, Irvin CG. Mechanisms of airway hyperresponsiveness in asthma: The past, present and yet to come. Clin Exp Allergy. 2015;45(4):706–19. 10.1111/cea.12506
8. Lim ECH, Ong BKC, Oh VMS, Seet RCS. Botulinum toxin: A novel therapeutic option for bronchial asthma? Med Hypotheses 2006;66:915–9. 10.1016/j.mehy.2005.12.015
9. Borkar NA, Roos B, Prakash YS, Sathish V, Pabelick CM. Nicotinic α7 acetylcholine receptor (α7nAChR) in human airway smooth muscle. Arch Biochem Biophys. 2021;706:108897. 10.1016/j.abb.2021.10889
10. Liu Y, Hao S, Yang B, Fan Y, Qin X, Chen Y, et al. Wnt/ b-catenin signaling plays an essential role in a7 nicotinic receptor-mediated neuroprotection of dopaminergic neurons in a mouse Parkinson’s disease model. Biochem Pharmacol. 2017;140:115–23. 10.1016/j.bcp.2017.05.017
11. Ma K-G, Lv J, Yang W-N, Chang K-W, Hu X-D, Shi L-L, et al. The p38 mitogen activated protein kinase regulates β-amyloid protein internalization through the α7 nicotinic acetylcho-line receptor in mouse brain. Brain Res Bull. 2018;137:41–52. 10.1016/j.brainresbull.2017.11.006
12. Chong L, Zhang W, Yu G, Zhang H, Zhu L, Li H, et al. High-fat diet induces airway hyperresponsiveness partly through activating CD38 signaling pathway. Int Immunopharmacol. 2018;56:197–204. 10.1016/j.intimp.2018.01.033
13. Black JL, Panettieri RA Jr, Banerjee A, Berger P. Airway smooth muscle in asthma just a target for bronchodilation? Clin Chest Med. 2012;33:543–58. 10.1016/j.ccm.2012.05.002
14. Cao X, Wang M, Li J, Luo Y, Li R, Yan X, et al. Fine particulate matter increases airway hyperresponsiveness through kallikrein-bradykinin pathway. Ecotoxicol Environ Saf. 2020; 195:110491. 10.1016/j.ecoenv.2020.110491
15. Zhao Y, Zhang H, Yang X, Zhang Y, Feng S, Yan X. Fine particulate matter (PM2.5) enhances airway hyperresponsiveness (AHR) by inducing necroptosis in BALB/c mice.Environ Toxicol Pharmacol. 2019;68:155–63. 10.1016/j.etap.2019.03.013
16. Bisdorff B, Kenn K, Nowak D, Schlichtiger J, Bäuml J, Orban E, et al. Asthma and vocal cord dysfunction related symptoms in the general population—a pilot study. Ann Allergy Asthma Immunol. 2014;113(5):576–7. 10.1016/j.anai.2014.08.009
17. Fajt ML, Birnie KM, Bittar HET, Petrov AA. Co-existence of vocal cord dysfunction with pulmonary conditions other than asthma: A case series. Respir Med Case Rep. 2018;25:104–8. 10.1016/j.rmcr.2018.08.001
18. Wheeler A, Smith HS. Botulinum toxins: Mechanisms of action, antinociception and clinical applications. Toxicology. 2013;306:124–46. 10.1016/j.tox.2013.02.006
19. Yang TY, Jung YG, Kim YH, Jang TY. A comparison of the effects of botulinum toxin A and steroid injection on nasal allergy. Otolaryngol Head Neck Surg. 2008;139:367–71. 10.1016/j.otohns.2008.06.031
20. Horowitz BZ. Botulinum toxin. Crit Care Clin. 2005;21:825–39. 10.1016/j.ccc.2005.06.008
21. Kandasamy M. Perspectives for the use of therapeutic botulinum toxin as a multifaceted candidate drug to attenuate COVID-19. Med Drug Discov. 2020;6:100042. 10.1016/j.medidd.2020.100042
22. Li S, Zhao T, Xin H, Ye L-H, Zhang X, Tanaka H, et al. Nicotinic acetylcholine receptor 7 subunit mediates migration of vascular smooth muscle cells toward nicotine. J Pharmacol Sci. 2004;94:334-8. 10.1254/jphs.94.334
23. Gu Z, Fonseca V, Hai C-M. Nicotinic acetylcholine receptor mediates nicotine-induced actin cytoskeletal remodeling and extracellular matrix degradation by vascular smooth muscle cells. Vasc Pharmacol. 2013;58:87–97. 10.1016/j.vph.2012.08.003
24. Buscà R, Christen R, Lovern M, Clifford AM, Yue J-X, Goss GG, et al. ERK1 and ERK2 present functional redundancy in tetrapods despite higher evolution rate of ERK1. BMC Evol Biol. 2015;15:179. 10.1186/s12862-015-0450-x
25. Du Q, Meng W, Athari SS, Wang R. The effect of Co-Q10 on allergic rhinitis and allergic asthma. Allergy Asthma Clin Immunol. 2021;17:32. 10.1186/s13223-021-00534-5
26. Freund-Michel V, Frossard N. Overexpression of functional TrkA receptors after internalization in human airway smooth muscle cells. Biochimica et Biophys Acta 2008;1783:1964–71. 10.1016/j.bbamcr.2008.05.014
27. Hami M, Naddaf SR, Mobedi I, Zare-Bidaki M, Athari SS, Hajimohammadi B 5, et al. Prevalence of linguatula serrata infection in domestic bovids slaughtered in Tabriz Abattoir, Iran. Ir J Parasitol. 2009;4(3):25–31.
28. Haddadzadeh HR, Athari SS, Abedini R, Khazraii Nia S, Khazraii Nia P, Nabian S, et al. One-humped camel (Camelus drome-darius) infestation with linguatula serrata in Tabriz, Iran. Ir J Arthropod Borne Dis. 2010;4(1):54–9.