
Download



ORIGINAL ARTICLE
Allergic contact dermatitis to chlorhexidine in children
Luis Morala*, Alicia Moralb, Laura Murciac, Nuria Marcod
aDoctor Balmis General University Hospital, Alicante Institute for Health and Biomedical Research (ISABIAL), Alicante, Spain
bFaculty of Medicine, Miguel Hernández University, Sant Joan d’Alacant, Spain
cVinalopó Hospital, Elche, Spain
dVega Baja Hospital, Orihuela, Spain
Abstract
Background: Hypersensitivity to chlorhexidine is rare in children. The usefulness of different diagnostic tests for allergic contact dermatitis (ACD) is unknown.
Objective: We aim to describe a case series of children with hypersensitivity to chlorhexidine and to compare the results of different diagnostic tests.
Patients: Nine children with hypersensitivity to chlorhexidine were included. Only six of these children and their parents consented to a comprehensive allergy assessment, which included the prick test, intradermal test, patch test, and repeated open application test (ROAT).
Results: Seven children (78%) presented symptoms of chlorhexidine hypersensitivity within the first 5 years of life; two of them before the age of 1 year. In four children, the dermatitis lesions were suggestive of wound superinfection. All six children who participated in the comprehensive diagnostic evaluation had negative results on the prick test. The immediate-reading intradermal test was positive in one case and uncertain in two cases. The patch test was positive in five cases, and the ROAT was positive in all six cases when using 2% chlorhexidine alcohol solution.
Conclusion: ACD to chlorhexidine in children appears to be rare and can be difficult to detect. Clinicians should consider this diagnosis when wounds worsen with chlorhexidine. Although the patch test is the most standardized method for detecting ACD, the ROAT with 2% chlorhexidine alcohol solution was the most sensitive test in our patients.
Key words: children, chlorhexidine, contact dermatitis, hypersensitivity, patch test, repeated open application test
*Corresponding author: Luis Moral, Doctor Balmis General University Hospital. Avda. Pintor Baeza, 12. 03010 Alicante, Spain. Email address: [email protected]
Received 11 June 2024; Accepted 12 August 2024; Available online 1 November 2024
Copyright: Moral L, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Chlorhexidine is a highly effective antiseptic widely used on the skin and mucous membranes, and it is also found in many common healthcare and cosmetic products.1–3 There have been reports of allergic contact dermatitis (ACD) to chlorhexidine since the 1960s.4,5 However, fewer than 3% of people with ACD show sensitization to chlorhexidine despite its widespread use, indicating that it appears to be a weak allergen.6–9 There are few reported cases of ACD to chlorhexidine in children.10–18 Chlorhexidine can also cause immediate allergic reactions and anaphylaxis in both children and adults.19,20 The diagnosis of chlorhexidine allergy is based on suggestive symptoms following exposure, combined with positive diagnostic tests (mainly in vivo): prick test and intradermal test for immediate reactions,1 or patch test and repeated open application test (ROAT) for ACD.21 Few studies have used ROAT to diagnose ACD to chlorhexidine.11,22
This study had two objectives: first, to describe a series of children with hypersensitivity to chlorhexidine, and second, to compare the results of different tests for diagnosing ACD to chlorhexidine.
Materials and Methods
Our series comprised children under 15 years old who had been evaluated for suspected chlorhexidine allergy between 2014 and 2023 at the pediatric allergy units of three hospitals. We contacted the parents to request their consent to participate in the study. To address our first objective, we collected relevant data retrospectively from hospital and medical records and conducted clinical interviews with each patient and their parents at the time of study inclusion. The variables assessed included age at symptom onset, age at first allergy assessment, current age, sex, allergic or atopic diseases in the patient and their first-degree relatives, reason for using the antiseptic prior to the initial or main reaction, initial location and characteristics of the lesions, treatment received, and time to resolution. We also inquired about previous use of chlorhexidine and the number of reactions associated with its use. For children who had undergone prior allergy testing, we reviewed the results.
For the second study objective, we designed a comprehensive comparative diagnostic evaluation for the children who agreed to participate in this part of the study. The evaluation included the following skin tests.
-
Prick test with immediate reading (15 min)
-
Chlorhexidine (5 mg/mL)
-
Povidone-iodine (100 mg/mL)
-
Positive control (histamine) and negative control (saline)
-
-
Intradermal test with chlorhexidine (0.002 mg/mL), with immediate reading (15 min) and delayed readings (48 and 96 h).
-
Patch test with a 0.5% chlorhexidine digluconate aqueous solution applied to the upper back using an 8-mm Finn Chamber®. The area was occluded for 48 h, with readings performed on days 2, 4, 7, and 10. We classified the reactions as negative (−), uncertain (+/−), mild (+), moderate (++), and severe (+++).21 We performed the patch test on each patient with the following two products.
-
0.5% chlorhexidine digluconate aqueous solution (Chemotechnique MB Diagnostics AD, Vellinge, Sweden), stored in a cold environment.
-
0.5% chlorhexidine digluconate aqueous solution (Bohmclorh®, Laboratorios Bohm, S.A., Madrid, Spain), commonly used as an antiseptic, stored at room temperature.
-
-
Repeated open application test (ROAT). We explained the procedure to parents and patients, and provided written instructions. They had to apply each product to an encircled area on the volar surface of the forearm twice daily (every 12 h) for up to 10 days. Patients were required to return to the clinic for readings and recording of results on days 2, 4, 7, and 10 after the start of the test. On day 14, we contacted the patients to check for any late reactions. A result was considered positive if there were papules (often with a follicular appearance) or vesicles, along with an erythematous base, at the site of application. A result was deemed uncertain (+/−) if the reaction was inconclusive. Positive reactions were classified as mild (+) if they caused no or minimal subjective discomfort, moderate (++) if they caused pruritus or other local discomfort, and severe (+++) if they caused considerable discomfort. The ROAT was continued for 10 days or until a positive reaction (+, ++, or +++) was observed. At that point, the patient (or parent) stopped applying the product that caused the reaction and could apply topical corticosteroids to the site of the positive result. The ROAT was performed with the following five products.
-
Commercial chlorhexidine for topical use (Bohmclorh®, Laboratorios Bohm, S.A., Madrid, Spain), stored at room temperature, with the following four preparations
-
0.5% chlorhexidine digluconate aqueous solution.
-
2% chlorhexidine digluconate aqueous solution.
-
0.5% chlorhexidine digluconate alcohol solution.
-
2% chlorhexidine digluconate alcohol solution.
-
-
Povidone-iodine (Betadine®, Viatris, Merignac, France), stored at room temperature.
We conducted a descriptive analysis of the results, summarizing both the characteristics of the population and the outcomes of the diagnostic tests.
The Drug Research Ethics Committee of Dr. Balmis General University Hospital approved the study. Before including children in the study, we obtained written informed consent from their parents and, when possible, from the children themselves.
Results
We identified nine children (all boys) with confirmed or suspected chlorhexidine allergy. Table 1 presents the main characteristics of these patients.
Table 1 Patient characteristics.
| Patient | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| Age at symptom onset | 4 years | 2 months | 11 years | 8 months | 3-4-years | 3 years | 18 months | 9 years | 18 months |
| Age at first allergy assessment | 5 years | 9 months | 12 years | 2 years | 7 years | 5 years | 3 years | 12 years | 8 years |
| Current age | 5 years | 5 years | 15 years | 6 years | 7 years | 11 years | 5 years | 12 years | 9 years |
| Sex | Male | Male | Male | Male | Male | Male | Male | Male | Male |
| Allergic/atopic diseases | No | No | Asthma, AR | Asthma, AR, AD, food allergy | No | Possible mild AR | Asthma, AR | Asthma, AD in remission | Asthma, AR |
| Prick test with allergen extracts | Positive to several aeroallergens | Not performed | Positive to several aeroallergens | Positive to several foods | Not performed | Not performed | Positive to olive pollen | Not performed | Positive to Alternaria |
| Family history of allergy/atopy | Yes | Yes | Yes | Yes | Yes | No | No | Yes | Yes |
| Reason for using antiseptic | Surgical removal of temporal cyst | Contact with healthy skin or skin erosions | Scratch on the face | Not specified | Superficial wound on forearm | Skin erosions on leg on 2 occasions | Wound on forehead and leg | Skin wounds on 4-5 occasions | 3 episodes of skin wounds |
| Location of initial reaction | Ear, face, neck, scalp | Ankle, face/neck | Face | Not specified | Volar surface of the forearm | Calf | Forehead and leg | Area of contact (various reactions) | Forehead, chin,side |
| Clinical manifestations of the reaction | Extensive crusted vesicular eczema similar to impetigo | Mild local eczematous reaction | Erythema, pruritus, papules, and honey-colored plaque similar to impetigo | Dermatitis and pruritus | Immediate erythema and edema | Eczema with vesicles | Very erythematous and pruritic micropapular rash similar to impetigo | Generalized and contact urticaria. Rhinitis and dry cough in some episodes | Micropapular erythematous rash |
| Treatment of reaction | OAH, TAB, TCS, OCS. Resolved in 1 week | No improvement without treatment for 3 weeks. Resolved in 1 week with TCS. | OAH, TCS, TAB | Not specified | Washed with water. Resolved in under 1 h | TAB and TCS. Resolved in 1 week | Parent does not remember treatment. Resolved after 1 week | OAH. Resolved in under 24 h | OAH. Resolved in 1 week |
| Initial diagnostic testing | ROAT with CLX aqueous and alcohol solutions, positive in 2-3 days | Patch test with 0.5% CLX, positive on day 4. ROAT with 1% CLX aqueous solution, positive | ROAT with 1% CLX aqueous solution, positive after 48 h | No previous diagnostic testing | No previous diagnostic testing | Patch test with film, 0.5% CLX aqueous solution, positive on day 3 | Patch test with 2% CLX alcohol solution, positive on day 2 | No previous diagnostic testing | Patch test with 0.5% CLX aqueous solution, positiveat 48 h. ROAT with 2% CLX alcohol solution, positive from day 4 |
AD: atopic dermatitis; AR: allergic rhinitis; CLX: chlorhexidine; OAH: oral antihistamine; OCS: oral corticosteroid; TAB: topical antibiotic; TCS: topical corticosteroid.
Seven boys (78%) experienced symptoms within the first 5 years of life, including two boys who had symptoms before the age of 1 year. The time from symptom onset to allergy evaluation ranged from 7 months to 7 years. Six boys had other atopic conditions or were sensitized to foods or airborne allergens, in addition to one boy with unconfirmed mild allergic rhinitis. Seven boys had first-degree relatives with allergic or atopic diseases. Only one patient developed dermatitis due to chlorhexidine use after surgery (Figure 1). In the remaining patients, reactions occurred following the cleaning of superficial skin wounds. Patient 2 also reacted when his pediatrician used chlorhexidine for hand disinfection before a medical examination on healthy skin. All patients exhibited mild or moderate localized lesions at the site of antiseptic contact or application. In four patients, clinicians suspected a superinfection of the lesions. Two patients (5 and 8) reported immediate local or systemic reactions. Six patients experienced two or more reactions (patients 2, 4, 6, 7, 8, and 9). The time to resolution of symptoms ranged from less than 1 h to 1 week, except for patient 2, who received no treatment for 3 weeks and then improved within 1 week with topical corticosteroids. Possible sources of sensitization were identified in three patients: the mother of patient 2 used chlorhexidine during the postpartum period while breastfeeding, and chlorhexidine was used to clean the umbilical cord in patients 5 and 7. As shown in Table 1, the previous diagnostic studies varied and were non-standardized.
Figure 1 Initial reaction in patient 1.
Six patients (1, 2, 3, 5, 6, and 8) agreed to participate in the comparative diagnostic evaluation designed for this study. The prick tests with chlorhexidine and povidone-iodine were negative in all six patients. The immediate-reading intradermal test with chlorhexidine showed a positive reaction in patient 6 (10-mm wheal), an uncertain reaction in patient 2 (7-mm wheal without erythema), and an uncertain reaction in patient 5 (20-mm erythema without wheal), while all other patients showed no reaction. Figure 2 displays the results of the patch test and ROAT. Five of the six patients (83%) had a positive patch test for chlorhexidine, typically observed by day 4. The reaction was more intense with the chlorhexidine produced by Chemotechnique Diagnostics compared to Bohmclorh® (see Figures 2 and 3). All six patients showed two or more positive ROAT results for chlorhexidine (see Figures 2 and 4). Although the ROAT results varied among the four chlorhexidine preparations, all patients exhibited a positive reaction to the 2% chlorhexidine alcohol solution by day 7. There were no late responses (day 14) to the patch test or ROAT. The ROAT with povidone-iodine was negative in all cases. No patients experienced serious reactions to any of the skin tests.
Figure 2 Results of skin tests recorded at every visit until reaction considered positive. Results: no reaction (−; green), uncertain reaction (+/−; yellow), mild reaction (+; orange: papules or vesicles, with an erythematous base at the site of application, but no or minimal discomfort), moderate reaction (++; red: pruritus or other discomfort), and severe reaction (+++: considerable discomfort). The ROAT was stopped after positive reaction (+, ++, +++). Bohm.: Bohmclorh®, produced by Laboratorios Bohm, S.A., Madrid, Spain); Chemot.: produced by Chemotechnique MB Diagnostics AD, Vellinge, Sweden; CLX: chlorhexidine, Pat.: patient; ROAT: repeated open application test.
Figure 3 Patch test reading in patient 1 on day 4. Reaction to Chemotechnique Diagnostics chlorhexidine is shown on the left and reaction to Bohmclorh® on the right.
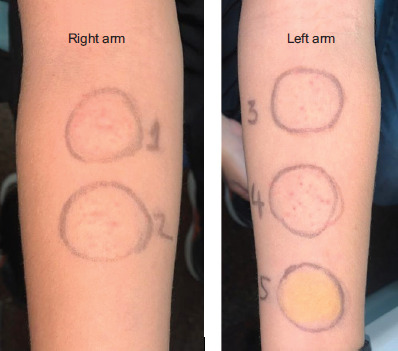
Figure 4 Repeated open application test (ROAT) reading for patient 8 on day 4. Right arm-1: 0.5% chlorhexidine aqueous solution; 2: 0.5% chlorhexidine alcohol solution. Left arm-3: 2 % chlorhexidine aqueous solution; 4: 2 % chlorhexidine alcohol solution; 5: povidone-iodine.
Discussion
There are very few cases of ACD to chlorhexidine in children compared to adults. Mailhol and colleagues performed patch testing on 641 children with atopic dermatitis and found that 17 (2.7%) were sensitized to chlorhexidine.23 In another study, Beaumont and colleagues identified 17 children sensitized to chlorhexidine among those who were sensitized to a commonly used antiseptic solution in France.22 Additionally, a pediatric series that included 14 children with ACD to antiseptics found seven with positive patch test reactions to chlorhexidine.24 None of these studies provided detailed information about their patients. Other case series have reported between one and eight patients each, totaling 24 children with allergic contact dermatitis (ACD) to chlorhexidine.10-18 Our study represents the largest series of individualized cases of ACD in children published to date. Although all patients in our study were boys, this appears to be coincidental, as only 14 of the 24 patients (58%) in previous studies were boys. One notable aspect of our study is the young age of our patients, including two boys who first exhibited symptoms at 2 and 8 months of age. No other studies have documented chlorhexidine reactions at such an early age. The lesions are typically mild and are triggered by chlorhexidine used in superficial or surgical wounds, or even on healthy skin, and they respond well to treatment. Diagnostic delay for this allergic reaction is common.10,16,17,22 In our study, the time to allergy assessment ranged from seven months to seven years after symptom onset, often with repeated reactions. This delay may result from the interval between exposure and symptom development, as well as the similarity of ACD to other skin conditions such as atopic dermatitis, irritant contact dermatitis, and, particularly, cellulitis and impetigo.10,11,24 Diagnostic delays may be longer in children compared to adults.22 Atopic diseases are common in the pediatric population, and atopic dermatitis may be a risk factor for sensitization to chlorhexidine.23 One possible source of early sensitization mentioned in several studies is the use of chlorhexidine for cleaning the umbilical cord.14,17,20,22,24 In our study, this exposure was reported in only two patients, but similar early exposures in other patients may have gone unnoticed or been forgotten. Additionally, the mother of one of our patients used chlorhexidine for postpartum care while breastfeeding, suggesting that breastmilk could be a potential source of sensitization. Other possible sources of sensitization identified in previous studies but not observed in our population include surgical interventions at an early age.11,12,15
Although two or our patients reported an immediate reaction to chlorhexidine, both had negative prick tests, and the intradermal test was uncertain in one of them. Conversely, the intradermal test was positive in a patient who had not experienced an immediate reaction. Delayed reading of the intradermal test yielded a negative result in all cases, indicating its low sensitivity in children with ACD to chlorhexidine. The patch test with chlorhexidine was positive in five of the six patients. Interestingly, the boy with the positive intradermal test (patient 6), who had an 8-year interval from symptom onset, had a negative patch test. The relationship between immediate and non-immediate allergic reactions to chlorhexidine is unknown, but the two types of allergy can coexist.18 In the patch test, Chemotechnique Diagnostics chlorhexidine produced more intense reactions than Bohmclorh®, despite the identical composition and concentration of the two products. A possible explanation is that Chemotechnique Diagnostics chlorhexidine is stored cold, which may decrease its degradation or volatilization. The ROAT with 2% chlorhexidine alcohol solution showed earlier and more intense results. It was the only test that produced a positive reaction in all cases. All patients had positive results to one or more tests, including patients who had experienced their initial reaction several years before, suggesting that the allergy persists over time. No tests produced a severe reaction.
The main limitations of our study were the small number of cases and the retrospective nature of data collection, which may be affected by memory bias. Additionally, it can be difficult to differentiate allergic reactions from irritant reactions in the ROAT, although chlorhexidine, ethanol and chlorhexidine in ethanol have been shown to be nonirritating in healthy volunteers.25
Conclusion
Chlorhexidine can cause ACD in children from the first year of life. It can be difficult to detect, leading to delayed diagnosis or even lack of diagnosis. When wounds treated with chlorhexidine worsen or do not heal, clinicians should consider ACD to chlorhexidine in their differential diagnosis, along with wound infection. Although the patch test is the most standardized test for diagnosing ACD, the ROAT with 2% chlorhexidine alcohol solution showed the highest diagnostic sensitivity in our study without causing serious reactions. There is a need for larger studies to investigate the prevalence and risk factors of ACD to chlorhexidine in children, to assess the effectiveness of different diagnostic tests, and examine the relationship with immediate chlorhexidine allergy.
Conflicts of Interest
The authors declare no conflict of interest.
REFERENCES
1 Chiewchalermsri C, Sompornrattanaphan M, Wongsa C, Thongngarm T. Chlorhexidine allergy: current challenges and future prospects. J Asthma Allergy. 2020;13:127–33. 10.2147/JAA.S207980
2 Opstrup MS, Johansen JD, Bossi R, Lundov MD, Garvey LH. Chlorhexidine in cosmetic products–a market survey. Contact Dermatitis. 2015;72(1):55–8. 10.1111/cod.12645
3 Opstrup MS, Johansen JD, Garvey LH. Chlorhexidine allergy: sources of exposure in the health-care setting. Br J Anaesth. 2015;114(4):704–5. 10.1093/bja/aev050
4 Calnan CD. Contact dermatitis from drugs. J R Soc Med. 1962;55(1):39–42. 10.1177/003591576205500111
5 Birdwood G. Reaction to chlorhexidine and cetrimide. Lancet. 1965;1(7386):651–652. 10.1016/S0140-6736(65)91742-3
6 Scheman A, Patel KR, Roszko K, Severson D, Brod B, Jacob SE, et al. Relative prevalence of contact allergens in North America in 2018. Dermatitis. 2020;31(2):112–21. 10.1097/DER.0000000000000521
7 Opstrup MS, Johansen JD, Zachariae C, Garvey LH. Contact allergy to chlorhexidine in a tertiary dermatology clinic in Denmark. Contact Dermatitis. 2016;74(1):29–36. 10.1111/cod.12487
8 Calado R, Calvão da Silva J, Gomes T, Gonçalo M. Is there a place for chlorhexidine in the European baseline series? Contact Dermatitis. 2021;85(3):372–3. 10.1111/cod.13861
9 Warshaw EM, Han J, Kullberg SA, DeKoven JG, Adler BL, Silverberg JI, et al. Patch testing to chlorhexidine digluconate, 1% aqueous: North American Contact Dermatitis Group experience, 2015-2020. Dermatitis. 2023;34(6):501–8. 10.1089/derm.2023.0077
10 Villa-Gonzalez JM, Gonzalez-Hermosa MR, Gardeazabal García J, Aramburu González A, Orbea Sopeña A, Pascual Ares M, et al. When the cure becomes worse than the disease: a case series of children with allergic contact dermatitis from chlorhexidine. J Eur Acad Dermatology Venereol. 2023;37(7):e936–8. 10.1111/jdv.19034
11 Magdaleno-Tapial J, Martínez-Doménech A, Valenzuela-Oñate C, Ferrer-Guillén B, Esteve-Martínez A, Zaragoza-Ninet V. Allergic contact dermatitis to chlorhexidine in pediatric patients. Pediatr Dermatol. 2019;36(4):540–1. 10.1111/pde.13808
12 Evangelista V, Vincenzi C, Bruni F, Piraccini BM, Neri I. Contact dermatitis apparently triggered by meningococcal and polyvalent vaccines: a case of allergic contact dermatitis due to chlorhexidine. Contact Dermatitis. 2021;85(3):354–5. 10.1111/cod.13846
13 Galadari A, Darrigade AS, Boralevi F, Milpied B. A child polysensitized to all constituents of Biseptine. Contact Dermatitis. 2020;82(1):65–6. 10.1111/cod.13393
14 Le Corre Y, Barbarot S, Frot AS, Milpied B. Allergic contact dermatitis to chlorhexidine in a very young child. Pediatr Dermatol. 2010;27(5):485–7. 10.1111/j.1525-1470.2010.01257.x
15 De Waard-Van Der Spek FB, Oranje AP. Allergic contact dermatitis to chlorhexidine and para-amino compounds in a 4-year-old boy: A very rare observation. Contact Dermatitis. 2008;58(4):239–41. 10.1111/j.1600-0536.2007.01256.x
16 Córdoba S, Sanz-Sánchez T, Mohedano-Vicente E, Borbujo J. Allergic contact dermatitis due to chlorhexidine in 2 pediatric patient. Actas Dermo-Sifiliográficas. 2019;110(1):76–7. 10.1016/j.ad.2017.10.018
17 Kefala K, Ponvert C. Allergic contact dermatitis to chlorhexidine-containing antiseptics and their excipients in children: a series of six cases. Pediatr Dermatol. 2023;40(1):151–3. 10.1111/pde.15127
18 Labrandero Hoyos C, Grau Echevarría A, Peñuelas Leal R, Spröhnle JL, Imbernon DB, Finello M, et al. Immediate and delayed hypersensitivity to chlorhexidine coexisting in the same patient. Contact Dermatitis. 2024;90(3):320–2. 10.1111/cod.14480
19 Opstrup MS, Jemec GBE, Garvey LH. Chlorhexidine allergy: on the rise and often overlooked. Curr Allergy Asthma Rep. 2019;19(5):23. 10.1007/s11882-019-0858-2
20 Wanin S, Baron M, Carra S, Saf S, Bourgoin-Heck M, Chiriac AM. Chlorhexidine anaphylaxis in three children secondary to oral exposure without evidence of mucosal breach. Pediatr Allergy Immunol. 2022;33(12):1–3. 10.1111/pai.13897
21 Johansen JD, Aalto-Korte K, Agner T, Andersen KE, Bircher A, Bruze M, et al. European Society of Contact Dermatitis guideline for diagnostic patch testing–recommendations on best practice. Contact Dermatitis. 2015;73(4):195–221. 10.1111/cod.12432
22 Beaumont C, Darrigade AS, Barbaud A, Collet E, Raison-Peyron N, Bourrain JL, et al. Multiple cases of sensitization to an antiseptic containing chlorhexidine digluconate/benzalkonium chloride/benzyl alcohol with different profiles of sensitization in adults and children. Contact Dermatitis. 2022;87(1):62–70. 10.1111/cod.14085
23 Mailhol C, Lauwers-Cances V, Rancé F, Paul C, Giordano-Labadie F. Prevalence and risk factors for allergic contact dermatitis to topical treatment in atopic dermatitis: a study in 641 children. Allergy. 2009;64(5):801–6. 10.1111/j.1398-9995.2008.01890.x
24 Darrigade AS, Léauté-Labrèze C, Boralevi F, Taïeb A, Milpied B. Allergic contact reaction to antiseptics in very young children. J Eur Acad Dermatology Venereol. 2018;32(12):2284–7. 10.1111/jdv.15140
25 Tupker RA, Schuur J, Coenraads PJ. Irritancy of antiseptics tested by repeated open exposures on the human skin, evaluated by non-invasive methods. Contact Dermatitis. 1997; 37(5):213–7. 10.1111/j.1600-0536.1997.tb02437.x