
Download
REVIEW ARTICLE
The immunopathology of coronary microembolization and the underlying inflammopathophysiological mechanisms
Li Maa †, Liping Caib †, Jiayue Panc †, Zimin Chenga, Yuanyuan Lva, Jie Zhenga, Peicheng Xua, Hong Zhanga, Xinyu Chena, Yimeng Huanga, Xiaolei Luoa, Jinhe Zhaoa*, Liang Xud*
aDepartment of Cardiovascular Medicine, Tianyou Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, China
bHealth Management Center, Wuhan Third Hospital, Wuhan, China
cXiangtao College of Medicine, Xiangtao College Affiliated to Wuhan University of Science and Technology, Wuhan, China
dDepartment of ICU, Wuhan Wuchang Hospital, Wuhan, China
†Li Ma, Liping Cai, and Jiayue Pan are the first authors
Abstract
In coronary microembolization, inflammatory cell infiltration, patchy necrosis, and extensive intra-myocardial hemorrhage are dominant, which induce myocardial dysfunction with clinical symptoms of chronic ischemic cardiomyopathy. Microembolization can lead to obstruction of the coronary microvessels and result in the micro-infarction of the heart. The inflammation and elevated expression of the tumor necrosis factor in cardiomyocytes and the activation of extracellular ERK are involved in initiating the inflammatory response mechanism. The PI3K/Akt signaling pathway is the enriched pathway, and for controlling, inhibition of PI3K/Akt is necessary. Furthermore, the release of cytokines and the activation of inflammasomes contribute to the enhancement of vascular permeability, which results in edema within the myocardium. The immune response and inflammation represent the primary triggers in this process. The ability to control immune response and inflammation reactions may lead to the development of new therapies for microembolization.
Key words: coronary, emboli, heart, immunopathology, signaling
*Corresponding author: Jinhe Zhao, Department of Cardiovascular Medicine, Tianyou Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, China. Email address: [email protected]; Liang Xu, Department of ICU, Wuhan Wuchang Hospital, Wuhan, China. Email address: [email protected]; [email protected]
Received 9 June 2024; Accepted 22 August 2024; Available online 1 November 2024
Copyright: Ma L, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Autopsy studies in the 1980s, on sudden deaths due to coronary artery disease, presented fissure or rupture of epicardial coronary atherosclerotic plaques and coronary microcirculatory obstruction. The endothelial dysfunction is triggered by mediators such as thromboxane A2, thrombin, and serotonin, and causes cyclic flow variations due to the embolization of platelet aggregates into the microcirculation.1–4
The application of protection devices in percutaneous coronary intervention (PCI) enabled the retrieval of plaque debris, thrombotic material, and factors that are soluble and unable to be retrieved from graft coronary vessels. The increase in plaque erosion incidence was related to a quantitative shift from ST-segment elevation MI (STEMI) to non-STEMI (NSTEMI) over the past 25 years.5–9
Coronary microembolization (CME) is produced during ulceration and spontaneous plaque rupture, as well as coronary intervention. In CME, microscopic examination revealed inflammatory cell infiltration and patchy necrosis, but there was no transmural damage and intra-myocardial or extensive intra-myocardial hemorrhages. Effectively, CME can decrease coronary reserve and induce dysfunction of myocardia with clinical symptoms of chronic ischemic cardiomyopathy.10–13 Therefore, the early detection of CME-induced ischemic lesions plays a major role in the prognosis and prediction of ischemic heart disease and micro-infarct of cardiac injury in suspected patients.14–16
CME causes left ventricular systolic dysfunction that is usually local and subtle, and it also induces microcirculatory impairment, which can cause patchy micro-infarction.10,17–20 The occurrence of CME is a spontaneous phenomenon in the context of acute coronary syndromes (ACS), and it is also a potential consequence of percutaneous coronary interventions. The typical CME consequences include micro-infarcts’ formation, inflammatory responses, contractile dysfunction, and reduction in coronary reserve. Mechanical stress, from interventional manipulation of epicardial coronary atherosclerotic plaques or hemodynamic perturbations with inflammatory destabilization, releases thrombotic material, particulate debris, and other substances that are soluble in the coronary circulation.21–28
The physical substance impedes the coronary microcirculation, while the soluble substance induces endothelium dysfunction and facilitates vasoconstriction. Blocking and dysfunction of the coronary microvascular result in patchy micro-infarcts accompanied by an immunoinflammatory reaction, both contributing to progressive dysfunction of the myocardial contractile. Distal protection devices have the potential to retrieve atherothrombotic debris and also, prevent embolization into the microcirculation. Nevertheless, their impact on clinical outcomes has been underwhelming, except for saphenous vein bypass grafts. The use of devices for the aspiration of thrombus-derived vasoconstrictors and thrombi, and immune-thrombogenic and inflammatory substances has been demonstrated to decrease the thrombus burden, provide protection, and improve perfusion in patients with acute MI.29–34 In this review, we focus on the features and mechanisms of CME and discuss immunopathology and related mechanisms of coronary microembolization.
Microembolization and Cardiac Function
The function of the global left ventricle (LV) is contingent upon the size and number of embolizing particles, as well as the size of the affected coronary perfusion territory. The response may range from transient and subtle LV dysfunction to severe cardiogenic shock.35,36 In CME animal models, CT and MRI demonstrated not only a reduction in global and regional contractile function but also defects of patchy perfusion, edema, and micro-infarcts.37,38–41 The clinical shape of coronary microembolization is unspecific. The elevation of biomarkers, such as troponin (a notable phenomenon, particularly when employing high-sensitivity assays) or creatine kinase, indicates myocardial injury but lacks specificity.42,43
Transient elevations in serum levels of CK, its isoenzyme CK-MB, and troponin I or T following PCI are indicative of periprocedural myocardial injury.44,45 The biomarker release magnitude depends on the clinical conditions of the patient (patients with chronic kidney disease or diabetes mellitus), the content of the vessel undergoing PCI (SVGs or native coronary arteries), and the type of procedure (the rot-ablation or simple stenting). The difference between primary and elective PCI in terms of resultant CME is simply the spontaneous versus iatrogenic nature of its origin in the culprit lesion.46–54 Future investigations and therapies should prioritize elucidating the interaction between inflammatory reactions and platelet aggregation at the epicardial culprit lesion and in the CME. Further analyses of coronary aspirate or trans-coronary gradients from ACS patients could provide additional insights into the pathophysiological mechanisms of CME and facilitate the development of targeted therapies.
Microembolization and Inflammation Signals
Microembolization can lead to the obstruction of coronary vessels and results in micro-infarction of the heart. Nevertheless, the apoptosis contribution to cell death from micro-infarction is relatively minor in comparison to that from necrosis. The obstruction resulting in micro-infarct is characterized by a profound inflammatory reaction, which leads to pyroptotic cell death.55,56 The presence of edema, macrophage, and neutrophil infiltration is observed in the vicinity of the micro-infarct site. The inflammatory reaction is continued by enhanced expression of TNF in cardiomyocytes and macrophages, as well as iNOS.57–65
The activation of extracellular ERK1 and ERK2 plays a pivotal role in initiating the inflammatory response. The presence of inflammation around micro-infarcts is associated with an increase in IGF1 mRNA expression in infiltrating monocytes. This increase represents a potential start signal for the promotion of collateral growth and the angiogenic response, as observed in a long-term model of CME.66,67
Among the inflammatory mediators, TNF exerts a particularly detrimental effect on the microembolized myocardium, exerting negative inotropic effects.61,62,65 In anesthetized animals, NO is formed with increased TNF upstream, while sphingosine is synthesized with increased TNF downstream. The ultimate effect of inflammatory signal transduction appears to be the enhanced formation of ROS, oxidative modification of contractile myofibrils, and a reduction in Ca2+ responsiveness of the contractile machinery.68–70 In coronary microembolization, these pathways can lead to apoptosis via activation of caspase 3 and 9 in myocardium.71
The CANTOS trial presented the IL-1β pathogenetic role in previous MI patients and increased plasma concentrations of the CRP.72 The antagonism (in long-term) of IL-6 and IL-1β can stabilize epicardial atherosclerotic plaques and also inhibit their eventual erosion and/or rupture. In the context of an interventional procedure for a stable or acute coronary syndrome, in which CME can occur and an anti-inflammatory reaction in the CME may be important, the benefit of IL-receptor antagonists and other anti-inflammatory agents is less clear.73,74 IL-6 inhibition not only stabilizes atherosclerotic plaques but also attenuates the downstream effects of inflammation and platelet aggregation.75
Immunopathogenesis of Coronary Microembolization
The pathogenic mechanisms and immunopathology of coronary disease are complex. The PI3K/Akt signaling pathway and platelet activation are the enriched pathways, and pathways such as PI3K/Akt are necessary for the control and inhibition of inflammatory reactions and apoptosis in the cardiovascular direction. The inflammatory mediators, activated platelets, and exposed damaged endothelium interact with one another, resulting in impaired local microcirculation within the coronary artery. This, in turn, leads to the formation of thrombi. A high level of IL-6 is detectable in intracoronary aspirated platelet-leukocyte mixtures obtained from patients with PCI which signals an inflammatory storm as a result of the intervening operation.76–78
In “platelet-inflammation-microthrombosis,” inhibition of platelet adhesion and the inflammatory state can improve cardiac function. Leukocytes and platelets aggregate to form a bridge between leukocytes and endothelial cells, mediated by P-selectin activation. This process, also known as “immunothrombosis,” exacerbates local embolism in the coronary artery. Furthermore, the regulation of integrin conformation via the PI3K/Akt pathway has been demonstrated to attenuate sodium laurate–induced coronary thrombosis. Cardiac dysfunction, as evidenced by the sodium laurate–induced coronary microthrombosis, is cumulative, manifesting as subtle alterations of the left ventricular function and severe cardiogenic shock.79–83
CD62p is a marker of thrombus formation and platelet activation, and Ca2+ serves as the crucial second messenger in cellular processes. The αIIbβ3 is an important membrane protein present on the platelets, which binds to RGD-containing ligands such as fibrin, von Willebrand factor (vWF), and fibrinogen, ultimately cross-linking the platelets to form tight fibrin–platelet thrombi. The αIIbβ3 activation spreads into a high-affinity conformation from the extracellular structural domain that is referred to as an “inside-out” signal. Subsequently, the sites of αIIbβ3-exposed receptor initiate an “outside-in” positive feedback pathway, which causes irreversible clot stabilization and retraction. This process is influenced by the PI3K/AKT pathway. Moreover, the vWF acts as an adhesion molecule that enhances the binding of αIIbβ3 to fibrinogen and promotes the formation of more stable platelet aggregates.84–89
The morphology of platelet cytoskeleton is a significant indicator of their activation status. The platelet cytoskeleton is composed of two actin filament-based components: (a) the cytoplasmic actin filaments, responsible for mediating contractile events and filling the cytoplasm; (b) the membrane skeleton, which coats the plasma membrane and helps regulate its properties including its contours and stability. Upon activation, platelets undergo a rapid increase in actin polymerization, with new filaments rapidly filling extended filamentous pseudopods and forming a network at the periphery of the platelets. The PI3K/Akt pathway is the most important one for αIIbβ3 (ITGB3/ITGA2B) and platelet activation. Upon stimulation of the vWF receptor GPIb-IX-V, the PI3Kβ stimulates Akt phosphorylation. The simulation of G protein-coupled receptors activates ITGB3/ITGA2B, which in turn triggers phospholipase and calcium and release regulatory pathways. In the context of the PI3K/Akt pathway-mediated activation of thrombocytes, the PI3K family of enzymes phosphorylate phospholipase enzymes at the 3′ position of the inositol ring, specifically generating 1,4,5-trisphosphatidylinositol phospholipids (PIP3). The Akt family of protein kinases plays a pivotal role in the PIP3–PI3K signaling cascade, functioning as a major binding protein. PIP33–5 recruits the pH domain-containing kinases PDK1 and Akt to the membrane where PDK1 phosphorylates Akt on Thr308 in the T-loop. On the other hand, Akt is phosphorylated by mTORC2 on Ser473, which results in maximal Akt activity. The three isoforms of Akt (1–3) play an important role in platelet aggregation and thrombus stabilization.90–97
Myocardial Infarction and Coronary Adhesion Molecules
Coronary endothelial cells exhibit relative resistance to ischemia and are capable of surviving hypoxia in vitro for extended periods. However, in vivo, the interruption of antegrade pulsatile flow and shear stress leads to the induction of endothelial cell swelling and blebbing.98–100 The reperfused endothelium exhibits altered calcium homeostasis, which increases cytosolic calcium. This, in turn, activates the endothelial contractile elements, thereby promoting the formation of intercellular gaps and increasing permeability to large molecules. The expression of adhesion molecules by activated platelets and endothelial cells results in the adhesion of platelets and platelet–leukocyte aggregates to the coronary microvasculature.101,102
Moreover, the release of cytokines impairs the stability of cell junctions and enhances vascular permeability. This occurs via the activation of Src and the dissociation of the VEGFR2/vascular endothelial (VE)–cadherin complex.103,104 Activation of the NLRP3 inflammasome in endothelial cells can result in caspase 1-mediated cell death. Endothelium-initiated inflammation, in conjunction with debris from cardiomyocyte necrosis, exerts proinflammatory effects, which result in the recruitment of inflammatory cells and the release of proinflammatory factors, including VEGF, thrombin, matrix metalloproteases, PAF, and myeloperoxidase.105–109 These factors increase vascular permeability, which results in edema of the myocardium via various mechanisms, including the activation of endothelial NO synthase (eNOS) in caveolae by VEGF.110,111
In cardiomyocytes, the reversal of intracellular edema is facilitated by the restoration of ion pump activation, particularly that of the sarcolemmal Na+/K+-ATPase. During ischemia, the accumulation of metabolites elevates interstitial osmolality. Exposure to normal osmotic blood at reperfusion induces immediate interstitial edema.112,113
Disseminated Intravascular Coagulation and Immune Responses
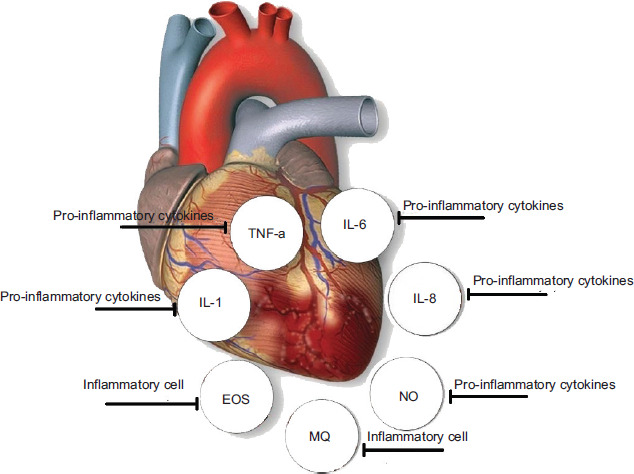
Disseminated intravascular coagulation (DIC) is a common occurrence in critical diseases. It represents the activation of the tissue factor pathway, cascade, and deposition of platelet–fibrin thrombi in the microvasculature.114,115 The hypercoagulability observed in DIC is further compounded by the presence of several other factors, including dehydration, hypoxia, and relative immobility, which are commonly observed in critical conditions. Several pathogenic mechanisms have been identified that may contribute to the development of DIC (Figure 1).116,117
Figure 1 Proinflammatory cytokines, mediators, and cells, related to disseminated intravascular coagulation.
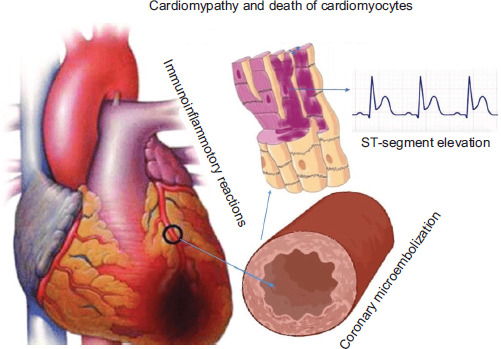
In infection-associated coagulopathy, the inflammatory response and innate immune activation are the primary drivers. It is presumed that coagulation and fibrin deposition are adaptive in the early phase of infection. However, continued inflammation results in a deleterious hyperinflammatory response mediated by a cytokine storm, and also macrophage activation syndrome. A cytokine storm is defined as an auto-amplifying proinflammatory cytokine release that significantly contributes to multiorgan dysfunction syndrome.118–121 Macrophage activation syndrome is a related proinflammatory cascade that is associated with a high incidence of thrombosis and mortality (Figure 2).122,123
Figure 2 Summarized pathway from inflammation to the ST-elevation in ECG.
Numerous proinflammatory cytokines are increased including TNF-α and IL-6, IL-2R, IL-10, and IL-8 (Figure 1).124,125 There is an association between elevated levels of IL-6 and fibrinogen.126 During infections, mononuclear cells express high levels of procoagulant genes including tissue factor, serpins, fibrinogen, and Factors II and X that are related to immune-mediated thrombosis and induce hypercoagulability.127,128 These cells also express genes TLR-9 and thromboxane synthase that promote endothelial dysfunction, platelet activation and aggregation, and vasoconstriction.129
The activation of complement cascade recruits and activates leukocytes, which leads to greatly amplified local secretion of the proinflammatory cytokines and subsequent microvascular damage. The complement system inhibition ameliorates coagulopathy and endothelial dysfunction in sepsis.130,131
Conclusions and Remaining Questions
CME is a prevalent phenomenon in ischemic heart disease, occurring spontaneously in patients with typical consequences such as contractile dysfunction and malignant arrhythmias. Several studies have indicated that CME may be a potential cause of dysfunction of the regional myocardial contractile, which is related to immuno-inflammatory reactions, coagulation thrombi with embolization into the coronary microcirculation, and also, lethal arrhythmias.132–135
The pathological observations found CME as the common cause of death from ischemic heart disease. The microemboli are associated with an inflammatory reaction and micro-infarcts. CME also can induce a marked inflammatory reaction, which is characterized by infiltration of eosinophils, and mulitifocal micro-infarcts.136–138 CME is associated with the development of patchy micro-infarcts, which affect approximately 2% of the respective myocardium. Some of the cardiomyocytes may undergo apoptosis, which is associated with the micro-infarcts and characterized by leukocyte infiltration. Conversely, elevated myocardial TNF-α levels are linked to contractile impairment following CME and result in dysfunction when exogenous TNF-α is infused directly into the coronary artery, even in the absence of microembolization.60,139 TNF-α is found in leukocytes that have infiltrated the area surrounding and within micro-infarcts. Additionally, it is present in cardiomyocytes in the viable border zone surrounding the micro-infarcts. The concentration of TNF-α and sphingosine in the myocardium is increased by microembolization. Pretreatment with NO-synthase inhibitor attenuates the progressive myocardial contractile dysfunction.68,140,141 Here, a signal cascade of TNF-α, NO, and sphingosine is identified and associated with CME (Figure 1). Immune response and inflammation are the key triggers of CME, and CME in turn triggers immune response initiation and inflammation reactions.142–144 Further experimental studies are also required to elucidate the specific immune response and therapeutic targets for the treatment of CME and its consequences.
Ethics Approval and Consent to Participate
The study was approved by the Medical Ethics Committee of Tianyou Hospital Affiliated with Wuhan University of Science and Technology.
Consent for Publication
Not Applicable.
Availability of Data and Materials
Not applicable.
Conflicts of Interests
There are no conflicts of interest.
Funding
Health Commission of Hubei Province Scientific Research Project: subsidy number: B2019013.
Hubei Provincial Health and Health Committee Joint Fund: WJ2019H230.
Authors’ Contributions
LM, LC, JP, ZC, YL, JZ, PX, HZ, XC, YH, XL, JZ, and LX participated in the planning, study, drafting, and writing of the manuscript.
Acknowledgments
Not applicable.
REFERENCES
1 Golino P, Buja M, Sheng-Kun Y, McNatt J, Willerson JT. Failure of nitroglycerin and diltiazem to reduce platelet-mediated vasoconstriction in dogs with coronary artery stenosis and endothelial injury: Further evidence for thromboxane A2 and serotonin as mediators of coronary artery vasoconstriction in vivo. J Am Coll Cardiol. 1990;5:718–26. 10.1016/0735-1097(90)90652-6
2 Folts JD, Gallagher K, Rowe GG. Blood flow reductions in stenosed canine coronary arteries: Vasospasm or platelet aggregation? Circulation. 1985;65:248–55. 10.1161/01.CIR.65.2.248
3 Eidt JF, Allison P, Noble S, Ashton J, Golino P, McNatt J, et al. Thrombin is an important mediator of platelet aggregation in stenosed canine coronary arteries with endothelial injury. J Clin Invest. 1989;84:18–27. 10.1172/JCI114138
4 Folts JD. Deleterious hemodynamic effects of thrombotic/embolic materials on the distal myocardial vasculature. Cardiovasc Res. 1999;42:6–7.
5 Gregorini L, Marco J, Heusch G. Peri-interventional coronary vasomotion. J Mol Cell Cardiol. 2012;52:883–9. 10.1016/j.yjmcc.2011.09.017
6 Fahed AC, Jang IK. Plaque erosion and acute coronary syndromes: Phenotype, molecular characteristics and future directions. Nat Rev Cardiol. 2021;18:724–34. 10.1038/s41569-021-00542-3
7 Kolte D, Libby P, Jang IK. New insights into plaque erosion as a mechanism of acute coronary syndromes. JAMA. 2021;325:1043–4. 10.1001/jama.2021.0069
8 Libby P. The changing landscape of atherosclerosis. Nature. 2021;592:524–33. 10.1038/s41586-021-03392-8
9 Puymirat E, Simon T, Cayla G, Cottin Y, Elbaz M, Coste P, et al. Acute myocardial infarction: Changes in patient characteristics, management, and 6-month outcomes over a period of 20 years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-elevation Myocardial Infarction) 1995 to 2015. Circulation. 2017;14:1908–19. 10.1161/CIRCULATIONAHA.117.030798
10 Cheng L, Chen Y, Pan W, Lu S, Chen Z, Shu X. Effect of microembolization on left ventricular systolic wall motion and dyssynchrony using dipyridamole stress two-dimensional speckle tracking imaging: An experimental study. J Med Ultrasound. 2013;21:189e197. 10.1016/j.jmu.2013.10.001
11 Li L, Qu N, Li DH, Wen WM, Huang WQ. Coronary microembolization induced myocardial contractile dysfunction and tumor necrosis factora mRNA expression partly inhibited by SB203580 through a p38 mitogen-activated protein kinase pathway. Chin Med J (Engl). 2011;124:100–5.
12 Schmitto JD, Ortmann P, Wachter R, Hintze E, Popov AF, Kolat P, et al. Chronic heart failure induced by multiple sequential coronary microembolization in sheep. Int J Artif Organs. 2008;31:348–53. 10.1177/039139880803100412
13 Carlsson M, Jablonowski R, Martin AJ, Ursell PC, Saeed M. Coronary microembolization causes long-term detrimental effects on regional left ventricular function. Scand Cardiovasc J. 2011;45:205–14. 10.3109/14017431.2011.568629
14 Dicks DL, Carlsson M, Heiberg E, Martin A, Saloner D, Arheden H, et al. Persistent decline in longitudinal and radial strain after coronary microembolization detected on velocity encoded phase contrast magnetic resonance imaging. J Magn Reson Imaging. 2009;30:69–76. 10.1002/jmri.21773
15 Carlsson M, Martin AJ, Ursell PC, Saloner D, Saeed M. Magnetic resonance imaging quantification of left ventricular dysfunction following coronary microembolization. Magn Reson Med. 2009;61:595–602. 10.1002/mrm.21869
16 Valero SJ, Moreno R, Reyes RM, Sánchez Recalde A, Galeote G, Calvo L, et al. Pharmacological approach of no-reflow phenomenon related with percutaneous coronary interventions. Cardiovasc Hematol Agents Med Chem. 2008;6:125–9. 10.2174/187152508783955079
17 Perk G, Kronzon I. Non-Doppler two dimensional strain imaging for evaluation of coronary artery disease. Echocardiography. 2009;26:299–306. 10.1111/j.1540-8175.2008.00863.x
18 Madriago E, Sahn DJ, Balaji S. Optimization of myocardial strain imaging and speckle tracking for resynchronization after congenital heart surgery in children. Europace. 2010;12:1341–3. 10.1093/europace/euq169
19 Marwick TH. Measurement of strain and strain rate by echocardiography: Ready for prime time? J Am Coll Cardiol. 2006;47:1313–27. 10.1016/j.jacc.2005.11.063
20 Gorcsan J 3rd, Tanaka H. Echocardiographic assessment of myocardial strain. J Am Coll Cardiol. 2011;58:1401–13. 10.1016/j.jacc.2011.06.038
21 Heusch, G. Myocardial ischaemia–Reperfusion injury and cardioprotection in perspective. Nat Rev Cardiol. 2020;17:773–89. 10.1038/s41569-020-0403-y
22 Heusch G. Coronary microvascular obstruction: The new frontier in cardioprotection. Basic Res Cardiol. 2019;114:45. 10.1007/s00395-019-0756-8
23 Liu Z, Zhao L, Hong D, GaoJ. Remote ischaemic preconditioning reduces myocardial ischaemic reperfusion injury in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Acta Cardiol. 2016;71:596–603. 10.1080/AC.71.5.3167504
24 Stone GW, Maehara A, Muller JE, Rizik DG, Shunk KA, Ben-Yehuda O, et al. Plaque characterization to inform the prediction and prevention of periprocedural myocardial infarction during percutaneous coronary intervention: The CANARY Trial (Coronary Assessment by Near-infrared of Atherosclerotic Rupture-prone Yellow). JACC Cardiovasc Interv. 2015;8:927–36. 10.1016/j.jcin.2015.01.032
25 Kleinbongard P, Heusch G. A fresh look at coronary Microembolization. Nat Rev Cardiol. 2022;19(4):265–80. 10.1038/s41569-021-00632-2
26 Erbel R, Heusch G. Brief review: Coronary microembolization. J Am Coll. Cardiol. 2000;36:22–4. 10.1016/S0735-1097(00)00708-7
27 Topol EJ, Yadav JS. Recognition of the importance of embolization in atherosclerotic vascular disease. Circulation. 2000;101:570–80. 10.1161/01.CIR.101.5.570
28 Libby P, Pasterkamp G, Crea F, Jang IK. Reassessing the mechanisms of acute coronary syndromes. Circ Res. 2019;124:150–60. 10.1161/CIRCRESAHA.118.311098
29 Partida RA, Libby P, Crea F, Jang IK. Plaque erosion: A new in vivo diagnosis and a potential major shift in the management of patients with acute coronary syndromes. Eur Heart J. 2018;39:2070–6. 10.1093/eurheartj/ehx786
30 Athari SS, Athari SM. The importance of eosinophil, platelet and dendritic cell in asthma. Asian Pac J Trop Dis. 2014;4(1):41–7. 10.1016/S2222-1808(14)60413-8
31 Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42:1289–367. 10.1093/eurheartj/ehaa575
32 Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction. Circulation. 2018;138:e618–e651. 10.1161/CIR.0000000000000617
33 Hibi K, Kozuma K, Sonoda S, Endo T, Tanaka H, Kyono H, et al. A randomized study of distal filter protection versus conventional treatment during percutaneous coronary intervention in patients with attenuated plaque identified by intravascular ultrasound. JACC Cardiovasc Interv. 2018;11:1545–55. 10.1016/j.jcin.2018.03.021
34 Feistritzer HJ, Meyer-Saraei R, Lober C, Böhm M, Scheller B, Lauer B, et al. Long-term outcome after thrombus aspiration in non-ST-elevation myocardial infarction: Results from the TATORT-NSTEMI trial: Thrombus aspiration in acute myocardial infarction. Clin Res Cardiol. 2020;109:1223–31. 10.1007/s00392-020-01613-0
35 Skyschally A, Schulz R, Erbel R, Heusch G. Reduced coronary and inotropic reserves with coronary microembolization. Am J Physiol Heart Circ Physiol. 2002;282:H611–4. 10.1152/ajpheart.00797.2001
36 Agress CM, Rosenburg MJ, Binder MJ, Schneiderman A, Clark WG. Blood volume changes in protracted shock resulting from experimental myocardial infarction. Am J Physiol. 1951;166:603–9. 10.1152/ajplegacy.1951.166.3.603
37 Saeed M, Hetts SW, Ursell PC, Do L, Kolli KP, Wilson MW. Evaluation of the acute effects of distal coronary microembolization using multidetector computed tomography and magnetic resonance imaging. Magn Reson Med. 2012;67:1747–57. 10.1002/mrm.23149
38 Nassenstein K, Breuckmann F, Bucher C, Kaiser G, Konorza T, Schäfer L, et al. How much myocardial damage is necessary to enable detection of focal late gadolinium enhancement at cardiac MR imaging? Radiology. 2008;249:829–35. 10.1148/radiol.2493080457
39 Lankarani KB, Honarvar B, Athari SS. The mechanisms underlying Helicobacter pylori–mediated protection against allergic asthma. Tanaffos. 2017;16(4):251–9.
40 Breuckmann F, Nassenstein K, Bucher C, Konietzka I, Kaiser G, Konorza T, et al. Systematic analysis of functional and structural changes after coronary microembolization: A cardiac magnetic resonance imaging study. JACC Cardiovasc Imaging. 2009;2:121–30. 10.1016/j.jcmg.2008.10.011
41 Carlsson M, Jablonowski R, Martin AJ, Ursell PC, Saeed M. Coronary microembolization causes long-term detrimental effects on regional left ventricular function. Scand Cardiovasc J. 2011;45:205–14. 10.3109/14017431.2011.568629
42 Leach IH, Blundell JW, Rowley JM, Turner DR. Acute ischaemic lesions in death due to ischaemic heart disease. An autopsy study of 333 cases of out-of-hospital death. Eur Heart J. 1995;16:1181–5. 10.1093/oxfordjournals.eurheartj.a061073
43 Haller PM, Beer BN, Tonkin AM, Blankenberg S, Neumann JT. Role of cardiac biomarkers in epidemiology and risk outcomes. Clin Chem. 2021;67:96–106. 10.1093/clinchem/hvaa228
44 Herrmann J. Periprocedural myocardial injury: Update. Eur Heart J. 2005;26:2493–519. 10.1093/eurheartj/ehi455
45 Ganesha Babu G, Malcolm WJ, Yellon DM, Hausenloy DJ. Peri-procedural myocardial injury during percutaneous coronary intervention: An important target for cardioprotection. Eur Heart J. 2011;32:23–31. 10.1093/eurheartj/ehq393
46 Bulluck H, Paradies V, Barbato E, Baumbach A, Bøtker HE, Capodanno D, et al. Prognostically relevant periprocedural myocardial injury and infarction associated with percutaneous coronary interventions: A consensus document of the ESC Working Group on Cellular Biology of the Heart and European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2021;42:2630–42. 10.1093/eurheartj/ehab271
47 Baars T, Konorza T, Kahlert P, Möhlenkamp S, Erbel R, Heusch G, et al. Coronary aspirate TNF alpha reflects saphenous vein bypass graft restenosis risk in diabetic patients. Cardiovasc Diabetol. 2013;12:12. 10.1186/1475-2840-12-12
48 Masoume Athari S, Mehrabi Nasab E, Shamsadin Athari S. Study effect of Ocimum basilicum seeds on mucus production and cytokine gene expression in allergic asthma mice model. Rev Fr Allergol. 2018;58(7):489–93. 10.1016/j.reval.2018.08.003
49 Baars T, Kleinbongard P, Böse D, Konorza T, Möhlenkamp S, Hippler J, et al. Saphenous vein aorto-coronary graft atherosclerosis in patients with chronic kidney disease: More plaque calcification and necrosis, but less vasoconstrictor potential. Basic Res Cardiol. 2012;107:303. 10.1007/s00395-012-0303-3
50 Kleinbongard P, Baars T, Möhlenkamp S, Kahlert P, Erbel R, Heusch G. Aspirate from human stented native coronary arteries vs. saphenous vein grafts: More endothelin but less particulate debris. Am J Physiol Heart Circ Physiol. 2013;305:H1222–9. 10.1152/ajpheart.00358.2013
51 Grube E, Gerckens U, Yeung AC, Rowold S, Kirchhof N, Sedgewick J, et al. Prevention of distal embolization during coronary angioplasty in saphenous vein grafts and native vessels using porous filter protection. Circulation. 2001;104:2436–41. 10.1161/hc4501.099317
52 Mehrabi Nasab E, Athari SM, Motlagh B, Athari SS. Effects of oral administration of Ocimum basilicum on goblet cell hyperplasia and upstream cytokine gene expression in allergic asthma. Rev Fr Allergol. 2020;60:64–8. 10.1016/j.reval.2019.02.226
53 Kini A, Kini S, Marmur JD, Bertea T, Dangas G, Cocke TP, et al. Incidence and mechanism of creatine kinase-MB enzyme elevation after coronary intervention with different devices. Catheter Cardiovasc Interv. 1999;48:123–9. 10.1002/(SICI)1522-726X(199910)48:2<123::AID-CCD1>3.3.CO;2-F
54 Esmaeilzadeh A, Tahmasebi S, Athari SS. Chimeric antigen receptor T cell therapy: Applications and challenges in treatment of allergy and asthma. Biomed Pharmacother. 2020;123:109685. 10.1016/j.biopha.2019.109685
55 Chen ZQ, Zhou Y, Chen F, Huang JW, Li HL, Li T, et al. miR-200a-3p attenuates coronary microembolization-induced myocardial injury in rats by inhibiting TXNIP/NLRP3-mediated cardiomyocyte pyroptosis. Front Cardiovasc Med. 2021;8:693257. 10.3389/fcvm.2021.693257
56 Zhou Y, Li T, Chen Z, Huang J, Qin Z, Li L. Overexpression of lncRNA TUG1 alleviates NLRP3 inflammasome-mediated cardiomyocyte pyroptosis through targeting the miR-186-5p/XIAP axis in coronary microembolization induced myocardial damage. Front Immunol. 2021;12:637598. 10.3389/fimmu.2021.637598
57 Hori M, Gotoh K, Kitakaze M, Iwai K, Iwakura K, Sato H, et al. Role of oxygen-derived free radicals in myocardial edema and ischemia in coronary microvascular embolization. Circulation. 1991;84:828–40. 10.1161/01.CIR.84.2.828
58 Yuan Y, Li B, Peng W, Xu Z. Protective effect of glycyrrhizin on coronary microembolization-induced myocardial dysfunction in rats. Pharmacol Res Perspect. 2021;9(1):e00714. 10.1002/prp2.714
59 Hajimohammadi B, Athari SM, Abdollahi M, Vahedi G, Athari SS. Oral administration of acrylamide worsens the inflammatory responses in the airways of asthmatic mice through agitation of oxidative stress in the lungs. Front Immunol. 2020;11:1940. 10.3389/fimmu.2020.01940
60 Dörge H, Neumann T, Behrends M, Skyschally A, Schulz R, Kasper C, et al. Perfusion–contraction mismatch with coronary microvascular obstruction: Role of inflammation. Am J Physiol Heart Circ Physiol. 2000;279:H2587–92. 10.1152/ajpheart.2000.279.6.H2587
61 Arras M, Strasser R, Mohri M, Doll R, Eckert P, Schaper W, et al. Tumor necrosis factor-α is expressed by monocytes/macrophages following cardiac microembolization and is antagonized by cyclosporine. Basic Res Cardiol. 1998;93: 97–107. 10.1007/s003950050069
62 Dörge H, Schulz R, Belosjorow S, Post H, van de Sand A, Konietzka I, et al. Coronary microembolization: The role of TNFa in contractile dysfunction. J Mol Cell Cardiol. 2002;34:51–62. 10.1006/jmcc.2001.1489
63 Wang D, Nasab EM, Athari SS. Study effect of Baicalein encapsulated/loaded Chitosan-nanoparticle on allergic asthma pathology in mouse model. Saudi J Biol Sci. 2021;28:4311–7. 10.1016/j.sjbs.2021.04.009
64 Cao YY, Chen ZW, Jia JG, Chen A, Zhou Y, Ye Y, et al. Establishment of a novel mouse model of coronary microembolization. Chin Med J (Engl). 2016;129:2951–7. 10.4103/0366-6999.195469
65 Li L, Zhao X, Lu Y, Huang W, Wen W. Altered expression of pro-and anti-inflammatory cytokines is associated with reduced cardiac function in rats following coronary microembolization. Mol Cell Biochem. 2010;342:183–90. 10.1007/s11010-010-0482-x
66 Kluge A, Zimmermann R, Münkel B, Mohri M, Sack S, Schaper J, et al. Insulin-like growth factor I is involved in inflammation linked angiogenic processes after microembolisation in porcine heart. Cardiovasc Res. 1995;29:404–15. 10.1016/0008-6363(96)88599-3
67 Chilian WM, Mass HJ, Williams SE, Layne SM, Smith EE, Scheel KW. Microvascular occlusions promote coronary collateral growth. Am J Physiol. 1990;258:H1103–11. 10.1152/ajpheart.1990.258.4.H1103
68 Thielmann M, Dörge H, Martin C, Belosjorow S, Schwanke U, van De Sand A, et al. Myocardial dysfunction with coronary microembolization: Signal transduction through a sequence of nitric oxide, tumor necrosis factor-a and sphingosine. Circ Res. 2002;90:807–13. 10.1161/01.RES.0000014451.75415.36
69 Canton M, Skyschally A, Menabò R, Boengler K, Gres P, Schulz R, et al. Oxidative modification of tropomyosin and myocardial dysfunction following coronary microembolization. Eur Heart J. 2006;27:875–81. 10.1093/eurheartj/ehi751
70 Skyschally A, Gres P, van Caster P, van de Sand A, Boengler K, Schulz R, et al. Reduced calcium responsiveness characterizes contractile dysfunction following coronary microembolization. Basic Res Cardiol. 2008;103:552–9. 10.1007/s00395-008-0732-1
71 Liu YC, Li L, Su Q, Liu T, Tang ZL. Trimetazidine pretreatment inhibits myocardial apoptosis and improves cardiac function in a swine model of coronary microembolization. Cardiology. 2015;130:130–6. 10.1159/000369246
72 Ridker PM, Everett BM, Thuren T, MacFadyen JG, Chang WH, Ballantyne C, et al. Anti-inflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377:1119–31. 10.1056/NEJMoa1707914
73 Cao D, Chiarito M, Mehran R. Treating inflammation prior to percutaneous coronary intervention: Does the heart care? Circ Cardiovasc Interv. 2020;13:e009127. 10.1161/CIRCINTERVENTIONS.120.009127
74 Basso C, Leone O, Rizzo S, De Gaspari M, van der Wal AC, Aubry MC, et al. Pathological features of COVID-19-associated myocardial injury: A multicenter cardiovascular pathology study. Eur Heart J. 2020;41:3827–35. 10.1093/eurheartj/ehaa664
75 Wagner JUG, Bojkova D, Shumliakivska M, Luxán G, Nicin L, Aslan GS, et al. Increased susceptibility of human endothelial cells to infections by SARS-CoV-2 variants. Basic Res Cardiol. 2021;116:42. 10.1007/s00395-021-00882-8
76 Badimon L, Vilahur G. Thrombosis formation on atherosclerotic lesions and plaque rupture. J Intern Med. 2014;276(6):618–32. 10.1111/joim.12296
77 Barbato E, Mehilli J, Sibbing D, Siontis GCM, Collet JP, Thiele H, et al. Questions and answers on antithrombotic therapy and revascularization strategies in non-ST-elevation acute coronary syndrome (NSTE-ACS): A companion document of the 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1368–78. 10.1093/eurheartj/ehaa601
78 Cao YY, Chen ZW, Jia JG, Chen A, Zhou Y, Ye Y, et al. Establishment of a novel mouse model of coronary microembolization. Chin Med J. 2016;129(24):2951–7. 10.4103/0366-6999.195469
79 Cambien B, Wagner DD. A new role in hemostasis for the adhesion receptor P-selectin. Trends Mol Med. 2004;10:179–86. 10.1016/j.molmed.2004.02.007
80 Huang M, Nasab EM, Athari SS. Immunoregulatory effect of mesenchymal stem cell via mitochondria signaling pathways in allergic asthma. Saudi J Biol Sci. 2021;28:6957–62. 10.1016/j.sjbs.2021.07.071
81 Dobesh PP, Finks SW, Trujillo TC. Dual antiplatelet therapy for long-term secondary prevention of atherosclerotic cardiovascular events. Clin Ther. 2020;42(10):2084–97. 10.1016/j.clinthera.2020.08.003
82 Fan ML, Tong HQ, Sun T, Zhang HW, Han J, Cheng SY, et al. Animal model of coronary microembolization under transthoracic echocardiographic guidance in rats. Biochem Biophys Res Commun. 2021;568:174–9. 10.1016/j.bbrc.2021.05.045
83 Galgano L, Guidetti GF, Torti M, Canobbio I. The controversial role of LPS in platelet activation in vitro. Int J Mol Sci. 2022;23(18):10900. 10.3390/ijms231810900
84 Gu Y, Bai Y, Wu J, Hu L, Gao B. Establishment and characterization of an experimental model of coronary thrombotic microembolism in rats. Am J Pathol. 2010;177(3):1122–30. 10.2353/ajpath.2010.090889
85 Guidetti GF, Canobbio I, Torti M. PI3K/Akt in platelet integrin signaling and implications in thrombosis. Adv Biol Regul. 2015;59:36–52. 10.1016/j.jbior.2015.06.001
86 Liu CF, He LH, Wang JX, Wang QQ, Sun CC, Li YQ, et al. Anti-angiogenic effect of Shikonin in rheumatoid arthritis by downregulating PI3K/AKT and MAPKs signaling pathways. J Ethnopharmacol. 2020;260:113039. 10.1016/j.jep.2020.113039
87 Jiang J, Nasab EM, Athari SM, Athari SS. Effects of vitamin E and selenium on allergic rhinitis and asthma pathophysiology. Respir Physiol Neurobiol. 2021;286:103614. 10.1016/j.resp.2020.103614
88 Mega JL, Close SL, Wiviott SD, Shen L, Hockett RD, Brandt JT, et al. Cytochrome p-450 polymorphisms and response to clopidogrel. N Engl J Med. 2009;360:354–62. 10.1056/NEJMoa0809171
89 Moore SF, Hunter RW, Hers I. mTORC2 protein complex-mediated Akt (Protein Kinase B) serine 473 phosphorylation is not required for Akt1 activity in human platelets [corrected]. J Biol Chem. 2011;286(28):24553–60. 10.1074/jbc.M110.202341
90 Moroi AJ, Watson SP. Impact of the PI3-kinase/Akt pathway on ITAM and hemITAM receptors: Haemostasis, platelet activation and antithrombotic therapy. Biochem Pharmacol. 2015;94:186–94. 10.1016/j.bcp.2015.02.004
91 Suo L, Chang X, Zhao Y. The orexin-A-regulated Akt/mTOR pathway promotes cell proliferation through inhibiting apoptosis in pancreatic cancer cells. Front Endocrinol (Lausanne). 2018;9:647. 10.3389/fendo.2018.00647
92 Thomas MR, Storey RF. The role of platelets in inflammation. Thromb Haemost. 2015;114:449–58. 10.1160/TH14-12-1067
93 Haddadzadeh H, Athari SS, Hajimohammadi B. The first record of Linguatula serrata infection of two-humped camel (Camelus bacterinus) in Iran. Iranian J Parasitol. 2009;4(1):59–61.
94 Wang MX, Xiang Q, Sun WX, Zhang HW, Shi RJ, Guo J, et al. Qihuang Zhuyu formula attenuates atherosclerosis via targeting PPARγ to regulate cholesterol efflux and endothelial cell inflammation. Oxid Med Cell Longev. 2022;2022:2226168. 10.1155/2022/2226168
95 Wu X, Pu L, Chen W, Zhao Q, Wu G, Li D, et al. LY294002 attenuates inflammatory response in endotoxin-induced uveitis by downregulating JAK3 and inactivating the PI3K/Akt signaling. Immunopharmacol Immunotoxicol. 2022;44(4):510–8. 10.1080/08923973.2022.2055565
96 Zou J, Swieringa F, de Laat B, de Groot PG, Roest M, Heemskerk JWM. Reversible Platelet Integrin αIIbβ3 activation and thrombus instability. Int J Mol Sci. 2022;23(20):12512. 10.3390/ijms232012512
97 Ding Y, Xiang Q, Zhu P, Fan M, Tong H, Wang M, et al. Qihuang Zhuyu formula alleviates coronary microthrombosis by inhibiting PI3K/Akt/αIIbβ3-mediated platelet activation. Phytomedicine. 2024;125:155276. 10.1016/j.phymed.2023.155276
98 Stempien-Otero A, Karsan A, Cornejo CJ, Xiang H, Eunson T, Morrison RS, et al. Mechanisms of hypoxia-induced endothelial cell death. Role of p53 in apoptosis. J Biol Chem. 1999;274:8039–45. 10.1074/jbc.274.12.8039
99 Maxwell L, Gavin JB. The role of post-ischaemic reperfusion in the development of microvascular incompetence and ultrastructural damage in the myocardium. Basic Res Cardiol. 1991;86:544–53. 10.1007/BF02190704
100 Hausenloy DJ, Chilian W, Crea F, Davidson SM, Ferdinandy P, Garcia-Dorado D, et al. The coronary circulation in acutemyocardial ischaemia/reperfusion injury: A target for cardioprotection. Cardiovasc Res. 2019;115:1143–55. 10.1093/cvr/cvy286
101 Kasseckert SA, Schafer C, Kluger A, Gligorievski D, Tillmann J, Schluter KD, et al. Stimulation of cGMP signalling protects coronary endothelium against reperfusion-induced intercellular gap formation. Cardiovasc Res. 2009;83:381–7. 10.1093/cvr/cvp065
102 Scotland RS, Cohen M, Foster P, Lovell M, Mathur A, Ahluwalia A, et al. C-type natriuretic peptide inhibits leukocyte recruitment and platelet-leukocyte interactions via suppression of P-selectin expression. Proc Natl Acad Sci USA. 2005;102:14452–7. 10.1073/pnas.0504961102
103 Weis S, Shintani S, Weber A, Kirchmair R, Wood M, Cravens A, et al. Src blockade stabilizes a Flk/cadherin complex, reducing edema and tissue injury following myocardial infarction. J Clin Invest. 2004;113:885–94. 10.1172/JCI200420702
104 Weis S, Cui J, Barnes L, Cheresh D. Endothelial barrier disruption by VEGF-mediated Src activity potentiates tumor cell extravasation and metastasis. J Cell Biol. 2004;167:223–9. 10.1083/jcb.200408130
105 Liu Y, Lian K, Zhang L, Wang R, Yi F, Gao C, et al. TXNIP mediates NLRP3 inflammasome activation in cardiac microvascular endothelial cells as a novel mechanism in myocardial ischemia/reperfusion injury. Basic Res Cardiol. 2014;109:415. 10.1007/s00395-014-0415-z
106 Galaup A, Gomez E, Souktani R, Durand M, Cazes A, Monnot C, et al. Protection against myocardial infarction and no-reflow through preservation of vascular integrity by angiopoietin-like 4. Circulation. 2012;125:140–9. 10.1161/CIRCULATIONAHA.111.049072
107 Hami M, Naddaf SR, Mobedi I, Zare Bidaki M, Athari SS, Hajimohammadi B, et al. Prevalence of Linguatula serrata infection in domestic bovids slaughtered in Tabriz Abattoir, Iran. Iranian J Parasitol. 2009;4(3):25–31.
108 Mollenhauer M, Friedrichs K, Lange M, Gesenberg J, Remane L, Kerkenpaß C, et al. Myeloperoxidase mediates postischemic arrhythmogenic ventricular remodeling. Circ Res. 2017;121:56–70. 10.1161/CIRCRESAHA.117.310870
109 Bitencourt CS, Bessi VL, Huynh DN, Menard L, Lefebvre JS, Levesque T, et al. Cooperative role of endogenous leucotrienes and platelet-activating factor in ischaemia-reperfusion-mediated tissue injury. J Cell Mol Med. 2013;17:1554–65. 10.1111/jcmm.12118
110 Weis SM, Cheresh DA. Pathophysiological consequences of VEGF-induced vascular permeability. Nature. 2005;437:497–504. 10.1038/nature03987
111 Feng Y, Venema VJ, Venema RC, Tsai N, Behzadian MA, Caldwell RB. VEGF-induced permeability increase is mediated by caveolae. Invest Ophthalmol Vis Sci. 1999;40:157–67.
112 Garcia-Dorado D, Andres-Villarreal M, Ruiz-Meana M, Inserte J, Barba I. Myocardial edema: A translational view. J Mol Cell Cardiol. 2012;52:931–9. 10.1016/j.yjmcc.2012.01.010
113 Inserte J, Garcia-Dorado D, Hernando V, Soler-Soler J. Calpain-mediated impairment of Naþ/Kþ-ATPase activity during early reperfusion contributes to cell death after myocardial ischemia. Circ Res. 2005;97:465–73. 10.1161/01.RES.0000181170.87738.f3
114 Dhainaut J-F, Shorr AF, Macias WL, Kollef MJ, Levi M, Reinhart K, et al. Dynamic evolution of coagulopathy in the first day of severe sepsis: Relationship with mortality and organ failure. Crit Care Med. 2005;33:341–8. 10.1097/01.CCM.0000153520.31562.48
115 Müller MC, Meijers JCM, Vroom MB, Juffermans NP. Utility of thromboelastography and/or thromboelastometry in adults with sepsis: A systematic review. Crit Care. 2014;18(1):R30. 10.1186/cc13721
116 Hanff TC, Mohareb AM, Giri J, Cohen JB, Chirinos JA. Thrombosis in COVID-19. Am J Hematol. 2020;95(12):1578–89. 10.1002/ajh.25982
117 Wada H. Disseminated intravascular coagulation. Clin Chim Acta. 2004;344:13–21. 10.1016/j.cccn.2004.02.015
118 Haddadzadeh HR, Athari SS, Abedini R, Khazraii Nia S, Khazraii Nia P, Nabian S, et al. One-humped camel (Camelus dromedarius) infestation with Linguatula serrata in Tabriz, Iran. Iran J Arthropod Borne Dis. 2010;4(1):54–9.
119 Chousterman BG, Swirski FK, Weber GF. Cytokine storm and sepsis disease pathogenesis. Semin Immunopathol. 2017;39:517–28. 10.1007/s00281-017-0639-8
120 Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ, HLH Across Speciality Collaboration. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet. 2020;395(10229):1033–4. 10.1016/S0140-6736(20)30628-0
121 England JT, Abdulla A, Biggs CM, Lee AYY, Hay KA, Hoiland RL, et al. Weathering the COVID-19 storm: Lessons from hematologic cytokine syndromes. Blood Rev. 2020;45:100707. 10.1016/j.blre.2020.100707
122 Karakike E, Giamarellos-Bourboulis EJ. Macrophage activation-like syndrome: A distinct entity leading to early death in sepsis. Front Immunol. 2019;10:55. 10.3389/fimmu.2019.00055
123 Crayne CB, Albeituni S, Nichols KE, Cron RQ. The immunology of macrophage activation syndrome. Front Immunol. 2019;10:119. 10.3389/fimmu.2019.00119
124 Chen G, Wu D, Guo W, Cao Y, Huang D, Wang H, et al. Clinical and immunologic features in severe and moderate Coronavirus Disease 2019. J Clin Invest. 2020;130(5):2620–9. 10.1172/JCI137244
125 Henry BM, Oliveira MHS De, Benoit S, Plebani M, Lippi G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin Chem Lab Med. 2020;58(7):1021–8. 10.1515/cclm-2020-0369
126 Ranucci M, Ballotta A, Dedda UD, Bayshnikova E, Dei Poli M, Resta M, et al. The procoagulant pattern of patients with COVID-19 acute respiratory distress syndrome. J Thromb Haemost. 2020;18(7):1747–51. 10.1111/jth.14854
127 Ng LFP, Hibberd ML, Ooi EE, Tang KF, Neo SY, Tan J, et al. A human in vitro model system for investigating genome-wide host responses to SARS coronavirus infection. BMC Infect Dis. 2004;4:34. 10.1186/1471-2334-4-34
128 Giannis D, Ziogas IA, Gianni P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. J Clin Virol. 2020;127:104362. 10.1016/j.jcv.2020.104362
129 Poon TCW, Pang RTK, Chan KCA, Lee NLS, Chiu RWK, Tong YK, et al. Proteomic analysis reveals platelet factor 4 and beta-thromboglobulin as prognostic markers in severe acute respiratory syndrome. Electrophoresis. 2012;33:1894–900. 10.1002/elps.201200002
130 Lupu F, Keshari RS, Lambris JD, Mark Coggeshall K. Crosstalk between the coagulation and complement systems in sepsis. Thromb Res. 2014;133 Suppl 1(0 1):S28–31. 10.1016/j.thromres.2014.03.014
131 Chen ZQ, Zhou Y, Chen F, Huang JW, Zheng J, Li HL, et al. Breviscapine pretreatment inhibits myocardial inflammation and apoptosis in rats after coronary microembolization by activating the PI3K/Akt/GSK-3β signaling pathway. Drug Des Devel Ther. 2021;15:843–55. 10.2147/DDDT.S293382
132 Jorgensen L, Rowsell HC, Hovig T, Glynn MF, Mustard JF. Adenosine diphosphate-induced platelet aggregation and myocardial infarction in swine. Lab Invest. 1967;17:616–44.
133 Erbel R, Heusch G. Coronary microembolization. J Am Coll Cardiol. 2000;36(1):22–4. 10.1016/S0735-1097(00)00708-7
134 Falk E. Unstable angina with fatal outcome: Dynamic coronary thrombosis leading to infarction and/or sudden death. Autopsy evidence of recurrent mural thrombosis with peripheral embolization culminating in total vascular occlusion. Circulation. 1985;71:699–708. 10.1161/01.CIR.71.4.699
135 Leach IH, Blundell JW, Rowley JM, Turner DR. Acute ischemic lesions in death due to ischemic heart disease. An autopsy study of 333 cases of out-of-hospital death. Eur Heart J. 1995;16:1181–5. 10.1093/oxfordjournals.eurheartj.a061073
136 Davies MJ, Thomas AC, Knapman PA, Hangartner JR. Intra-myocardial platelet aggregation in patients with unstable angina suffering sudden ischemic cardiac death. Circulation. 1986;73:418–27. 10.1161/01.CIR.73.3.418
137 Skyschally A, Erbel R, Heusch G. Coronary microembolization. Circ J. 2003;67:279–286. 10.1253/circj.67.279
138 Leistner DM, Kränkel N, Meteva D, Abdelwahed YS, Seppelt C, Stähli BE, et al. Differential immunological signature at the culprit site distinguishes acute coronary syndrome with intact from acute coronary syndrome with ruptured fibrous cap: Results from the prospective translational OPTICO-ACS study. Eur Heart J. 2020;41:3549–60. 10.1093/eurheartj/ehaa703
139 Dörge H, Schulz R, Belosjorow S, Post H, van de Sand A, Konietzka I, et al. Coronary microembolization: The role of TNFαin contractile dysfunction. J Mol Cell Cardiol. 2002;34:51–62. 10.1006/jmcc.2001.1489
140 Zheng J, Long M, Qin Z, Wang F, Chen Z, Li L. Nicorandil inhibits cardiomyocyte apoptosis and improves cardiac function by suppressing the HtrA2/XIAP/PARP signaling after coronary microembolization in rats. Pharmacol Res Perspect. 2021;9:e00699. 10.1002/prp2.699
141 Qian L, Nasab EM, Athari SM, Athari SS. Mitochondria signaling pathways in allergic asthma. J Investig Med. 2022;70(4):863–82. 10.1136/jim-2021-002098
142 Mao Q, Liang X, Wu Y, Lu Y. Nobiletin protects against myocardial injury and myocardial apoptosis following coronary microembolization via activating PI3K/Akt pathway in rats. Naunyn Schmiedebergs Arch Pharmacol. 2019;392:1121–30. 10.1007/s00210-019-01661-y
143 Ghasemi F, Sarabi PZ, Athari SS, Esmaeilzadeh A. Therapeutics strategies against cancer stem cell in breast cancer. Int J Biochem Cell Biol. 2019;109:76–81. 10.1016/j.biocel.2019.01.015
144 Cohen MV, Downey JM. What are optimal P2Y12 inhibitor and schedule of administration in patients with acute coronary syndrome? J Cardiovasc Pharmacol Ther. 2020;25:121–30. 10.1177/1074248419882923