
Download
ORIGINAL ARTICLE
Prevalence of atopic eczema in adolescents from a very low prevalence area (Kosovo): role of wheezing, gender, exercise, and paracetamol
Luljeta Ahmetaja †, A. Elena Martínez-Torresb†, Ylli Ahmetajc, Valbona Gashia, Xhevat Kurhasanid, Violeta Lokaj-Berishaa, Besa Gacaferri-Lumezia, Mirsije Shahinie, Valbona Zhjeqia, Luis García-Marcosf * *, the Global Asthma Network Phase I Kosovo Study Groupg
aInstitute of Physiology & Immunology, Faculty of Medicine, University of "Hasan Prishtina”, Prishtina, Kosovo
bPaediatric Allergy and Pulmonology Units and Nurse Research Group, Virgen de la Arrixaca University Children’s Hospital; and IMIB Biomedical Research Institute, Murcia, Spain
cAAB College. Industriale Prishtinë–Fushë Kosovë, Prishtinë Republika e Kosovës
dUBT Higher Education Institution, Prishtinë Republika e Kosovës
eAlergji Asthma Ylli” Polyclinic, Prishtinë Republika e Kosovës
fPaediatric Allergy and Pulmonology Units, Virgen de la Arrixaca University Children’s Hospital, University of Murcia; and IMIB Biomedical Research Institute, Murcia, Spain
gMembers of the Global Asthma Network Phase I Kosovo Study Group (LN Ahmetaj,* R Baftiu, Y Ahmetaj, M Shahini, G Parduzi, D Ahmetaj, A Kafexholli, D Musliu, A Deva, A Rabushaj, E Blyta, A Breznica, I Jakupi, F Spahiu, University of Prishtina "Hasan Prishtina", Medical Faculty, Kosovo (Prishtina); I Bucaliu-Ismajli, The Principal Center of Family Care (Ferizaj); L Pajaziti, University Hospital Clinic, Clinic of Dermatology, Prishtina, Kosovo (Gjakova); L Hana-Lleshi, General Hospital "Isa Grezda" Gjakova, Kosovo (Gjakova Adults); V Ghashi, Regional Hospital, "Sami Haxhibeqiri" Mitrovica, Kosovo (Gjilan); X Kurhasani, UBT College, Kosovo (Peja); B Gacaferri-Lumezi, University of Prishtina "Hasan Prishtina", Medical Faculty, Kosovo (Peja 6-7); V Zhjeqi, University of Prishtina (Prizren); V Lokaj-Berisha, University of Prishtina (Prizren Adults).
*Kosovo’s principal investigator
†L Ahmentaj and AE Martinez-Torres are joint first authors.
Abstract
Background: The epidemiology of atopic eczema in adolescents in Kosovo is virtually unknown, and the risk factors for the condition in very low-prevalence areas (as it was the case) are not well studied. The objective of the present study was to better know those factors and whether the presence of comorbid wheezing symptoms modifies the factors.
Methods: The cross-sectional survey, Global Asthma Network-validated questionnaire, which includes questions on eczema symptoms and environmental factors (such as smoking, pet ownership, paracetamol usage, truck traffic, siblings, time spent using screens or watching television, and physical exercise), was administered to adolescents in the following main cities of Kosovo: Ferizaj, Gjakova, Gjilan, Peja, Prishtina, and Prizren. Additionally, height and weight were measured at school.
Results: Prevalence of eczema symptoms ranged from 2.2% in Ferizaj to 5.5% in Gjakova. Severe symptoms were <1% in all cities. Eczema ever ranged from 3.0% in Ferizaj to 6.4% in Prizren. Factors significantly associated with the prevalence of current eczema symptoms in the meta-analysis were males (pooled adjusted odds ratio [aOR] 0.50, 95% Confidence Interval [95% CI] 0.37–0.66); physical exercise (pooled aOR 2.79, 95% CI 1.89–4.10); and paracetamol intake (pooled 1.86, 95% CI 1.32–2.64). The corresponding figures for eczema ever were as follows: pooled aOR: 0.68, 95% CI 0.44–1.06; pooled aOR 2.07, 95% CI 1.48–2.90; and pooled aOR 1.19, 95% CI 0.88–1.60. The associations tended to be higher in the subpopulation with eczema and wheezing comorbidity.
Conclusions: The prevalence of atopic eczema is very low in Kosovo and is associated with females, physical exercise, and paracetamol intake. These associations are higher when eczema and wheezing are comorbid conditions.
Key words: adolescents, atopic eczema, epidemiology, exercise, Kosovo, Paracetamol
*Corresponding author: Luis Garcia-Marcos, Department of Paediatrics, Departamental-LAIB, University of Murcia Edificio, Avenida Buenavista s/n, 30120 El Palmar, Murcia, Spain. Email address: [email protected]
Received 14 June 2024; Accepted 2 September 2024; Available online 1 November 2024
Copyright: Ahmetaj L, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
The prevalence of atopic eczema has increased in past decades; its variability is high and depends, in part, on the region of the world and socioeconomic status.1 According the Global Asthma Network’s (GAN) recently published report,2 increase of eczema in adolescents aged 13–14 years was 0.98% per decade during the past 27 years. In the first GAN survey, conducted between 2015 and 2020, the prevalence of eczema in low-, middle low-, and upper middle--income countries, symptoms of both current eczema and lifetime eczema were significantly lower than those in high-income countries.3 In this survey, Kosovo was considered an upper middle-income country.4 Additionally, Kosovo, although not having direct access to the sea, was considered a Mediterranean country. This warm and humid area, compared to other global areas, has shown relatively low prevalence of atopic eczema,5 with some studies pointing at climate and, in particular, the period of sunny hours, as being part of this explanation.1,6
The prevalence of eczema in Kosovo is basically unknown, although some epidemiological data in Balkans existed previously. The International Study of Asthma and Allergies in Childhood (ISAAC) phase III (the methodology of which has been used by GAN) reported data from Albania in the age groups of 6–7 and 13–14 years; this was one of the world’s lowest data for symptoms of current eczema.5 Both in the ISAAC report and in a more detailed study conducted by Zivković et al.,7 the lowest prevalence of current eczema symptoms in Serbia and Montenegro was found to be in Novi Sad (north of Serbia). However, neither of the two reports, nor the previous ones from Balkans,8,9 included the study of risk or protective factors for eczema at individual or center levels. To the best of our knowledge, only one study conducted in Croatia had reported epidemiological factors associated with eczema among adolescents in Balkans.10 Another study focused on the association of traffic pollution with allergic diseases.11
Thus, the epidemiology, including potential risks and protective factors, of eczema in adolescents in the main cities of Kosovo could add important information on the subject as follows: it demonstrated (1) the current magnitude of the problem in an area previously known for low prevalence of the condition; (2) comparison of epidemiological factors in a low-prevalence region to the areas of higher prevalence; (3) comparison between various centers of the same low-prevalence area; and, finally, (4) paths for prevention of the condition.
Methods
The methods of the GAN study are published elsewhere12 and are identical to those of ISAAC. GAN is a cross--sectional study based on written questionnaires distributed in schools in the participating centers. In Kosovo, the survey included the age group of 13–14 years, and the following six centers: Ferizaj, Gjakova, Gjilan, Peja, Prishtina, and Prizren. The fieldwork was carried out between 2017 and 2018.
Questionnaires
The definitions of indicators of atopic eczema were derived from the written questionnaires completed by adolescents at school. The original questionnaire was in English, and translation and back-translation to Albanese followed a specific methodology common to ISAAC and GAN.13
Definitions
“Current eczema symptoms” were defined as a positive answer to the following two questions: “Have you had this itchy rash (as defined in a previous question) at any time in the past 12 months?” and “has this itchy rash at any time affected any of the following places: the folds of the elbows, behind the knees, in front of the ankles, under the buttocks, or around the neck, ears, or eyes?” “Severe eczema symptoms” were defined as symptoms of current eczema being the cause of awakening at night one or more times a week according to the following question: “In the past 12 months, how often, on average, have you (has this child) been kept awake at night by this itchy rash? (never in the past 12 months, less than one night per week, or one or more nights per week).” Finally, “Eczema ever” was defined as a positive answer to: “Have you ever had eczema?”
“Current wheezing” was defined by a positive answer to the following question: “Have you (has your child) had wheezing or whistling in the chest in the past 12 months?” Current wheezing was used to stratify eczema markers in some of the statistical analyses.
Additionally, adolescents responded to the environmental questionnaire. This included questions on smoking, pet ownership, paracetamol use, truck traffic in the street where adolescents lived, siblings, time spent using screens or watching television, and exercise. Additionally, height and weight were measured at school by fieldworkers in a standardized way according to the GAN methods.12
Physical exercise was assessed by the following question: “How many times a week do you engage in vigorous physical exercise activity long enough to make you breath hard? (never or occasionally; once or twice per week; three or more times per week).” Paracetamol intake was surveyed by the following question: “In the past 12 months, how often, on average, have you taken paracetamol for fever? (never; at least once a year; at least once per month).” Overweight was defined as body mass index (BMI) >25.
Sample size and study power
As for any GAN center, all students (selected by grade or age) aged 13–14 years in all schools (Ferizaj, Gjakova, Gjilan, Peja, and Prizren) or in a random sample of them (Prishtina) were invited to participate to achieve the minimum required sample size of 1000. Additional details of the sample size and power are described elsewhere.12,14 Participation proportions in Kosovo (≥80.0%) were described above in detail.15
Statistical analysis
To calculate participation proportions, the denominator was the number of adolescents and the numerator was the number of core questionnaires returned with at least one data symptom. For prevalence estimations, positive answers to a specific symptom in the center were divided by the number of completed questionnaires.
All variables included in the GAN environmental questionnaire were used as independent variables in logistic regression analyses (univariate or multivariate), in which three eczema markers (current symptoms, severe symptoms, and current eczema) were the dependent variables within each center. As the number of cases with severe symptoms was very low, logistic regression analyses were not performed. Factors that showed significant (P < 0.05) values of adjusted odds ratios (aOR) in the multivariate logistic regression analyses for at least one center were subsequently meta-analyzed (random effects), including the results of six centers. A forest plot was built, including the pooled effect together with 95% Confidence Interval (95% CI) and prediction interval. Measures of heterogeneity, such as Q and I2, were also calculated.
To test whether the presence of current wheezing modified the associations between environmental factors and eczema markers, a multilevel mixed effects logistic regression model was performed on a complete sample of adolescents, including the same variables as within the center logistic regressions, and using the individual as the first level and the center as the second.
Most statistical calculations were made using the Stata SE® V18 software package (Stata Corp., College Station, TX, USA) except meta-analyses that were carried out using the Comprehensive Meta-Analysis (CMA) V4.0 software package (Biostat, Englewood, NJ, USA).
Ethics
Prior to the beginning of the study, permission was asked and authorization issued by the education authorities of each municipality. Passive informed consent was used. The study was approved by the Ethics Committees of the Ministry of Health and the Ministry of Education of Kosovo according to the Helsinki declaration (approval No. 21/550).
Results
Demographic and environmental characteristics of the six Kosovar centers were already described.15 Table 1 shows the prevalence of current eczema symptoms, severe eczema symptoms, and eczema ever overall with and without wheezing, together with the respective 95% CIs. Overall, the proportion of adolescents with eczema and wheezing symptoms was much lower than that with only eczema symptoms. The prevalence of severe eczema symptoms was very low and similar among centers.
Table 1 Prevalence of current eczema symptoms, severe eczema symptoms, and eczema ever, overall, and with and without wheezing in six Kosovar cities (% and 95% Confidence Interval [95% CI])†
| Ferizaj N = 890 | Gjakova N = 676 | Gjilan N = 1200 | Peja N = 1433 | Prishtina N = 1056 | Prizren N = 1427 | |
|---|---|---|---|---|---|---|
| Current eczema symptoms | 2.2 (1.5–3.5) | 5.5 (4.0–7.5) | 4.1 (3.1–5.4) | 5.0 (4.0–6.3) | 5.3 (4.1–6.8) | 4.6 (3.6–5.8) |
| Without wheezing | 2.0 (1.3–3.2) | 5.3 (3.9–7.3) | 3.2 (2.3–4.4) | 3.6 (2.8–4.7) | 4.1 (3.1–5.5) | 3.7 (2.8–4.8) |
| With wheezing | 0.2 (0.06–0.9) | 0.2 (0.02–1.1) | 0.9 (0.5–1.7) | 1.5 (1.0–2.3) | 1.3 (0.7–2.2) | 1.0 (0.6–1.7) |
| Severe eczema symptoms | 0‡ | 0.7 (0.3–1.8) | 0.6 (0.3–1.2) | 0.6 (0.3–1.1) | 0.5 (0.2–1.1) | 0.6 (0.3–1.1) |
| Without wheezing | 0‡ | 0.6 (0.2–1.6) | 0.5 (0.2–1.1) | 0.4 (0.2–0.9) | 0.4 (0.1–1.0) | 0.4 (0.2–0.9) |
| With wheezing | 0‡ | 0.1 (0.02–1.1) | 0.08 (0.01–0.6) | 0.1 (0.04–0.6) | 0.1 (0.01–0.7) | 0.1 (0.04–0.6) |
| Eczema ever | 3.0 (2.1–4.4) | 6.8 (5.1–9.0) | 4.2 (3.2–5.5) | 5.7 (4.6–7.0) | 4.0 (3.0–5.3) | 6.4 (5.3–7.8) |
| Without wheezing | 2.4 (1.6–3.6) | 6.0 (4.4–8.0) | 3.4 (2.5–4.6) | 4.7 (3.7–5.9) | 3.7 (2.7–5.0) | 5.1 (4.1–6.4) |
| With wheezing | 0.7 (0.3–1.5) | 0.9 (0.4–2.1) | 0.8 (0.4–1.5) | 1.1 (0.7–1.8) | 0.3 (0.1–0.9) | 1.5 (0.1–2.3) |
†See text for definitions.
‡No cases.
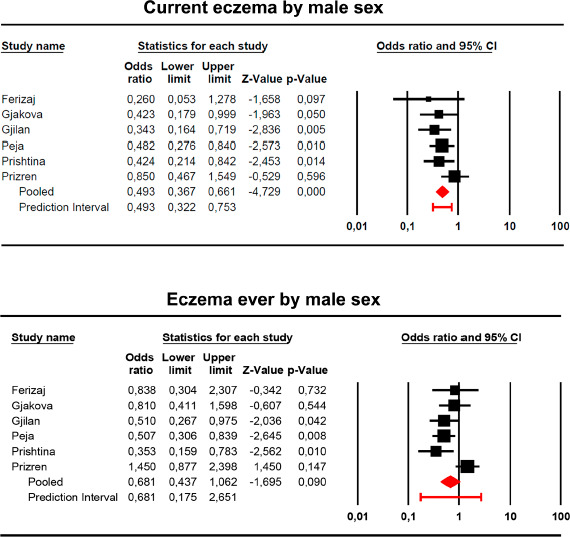
Tables S1 and S2 include associations found in univariate and multivariate logistic regressions of different factors for current eczema symptoms and eczema ever, respectively, per center. Factors that were consistently associated with current eczema symptoms and eczema ever in most centers were gender, physical exercise, and paracetamol usage. Forest plots of these three factors showed a trend that males (Figure 1) were associated with lower prevalence of eczema: pooled aOR 0.49; 95% CI 0.37–0.66 for current eczema; and pooled aOR 0.68; 95% CI 0.44–1.06 for eczema ever.
Figure 1 Forest plot of random meta-analysis of the association of gender with current eczema symptoms (flexural itchy rashes—upper panel; Q = 5.03, P = 0.412; I2 = 0.68%,) and eczema ever (lower panel; Q = 13.7, P = 0.018; I2 = 63.5%).
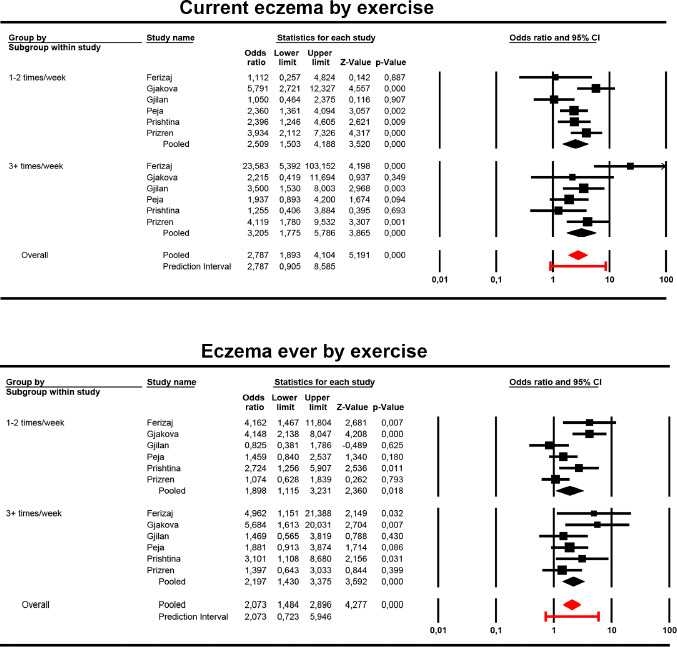
Figure 2 shows that physical exercise was associated with higher prevalence of current eczema symptoms and eczema ever, with no apparent dose–effect relationship. The pooled aOR and 95% CI for any frequency of physical exercise were 2.79 (1.89–4.10) and 2.07 (1.48–2.90) for current eczema symptoms and eczema ever, respectively.
Figure 2 Forest plot of random meta-analysis of the association of physical exercise with current eczema symptoms (flexural itchy rashes—upper panel; Q = 24.34, P = 0.011 [overall]; I2 = 54.81% [overall]) and eczema ever (lower panel; Q = 24,31, P = 0.011; I2 = 54.75%).
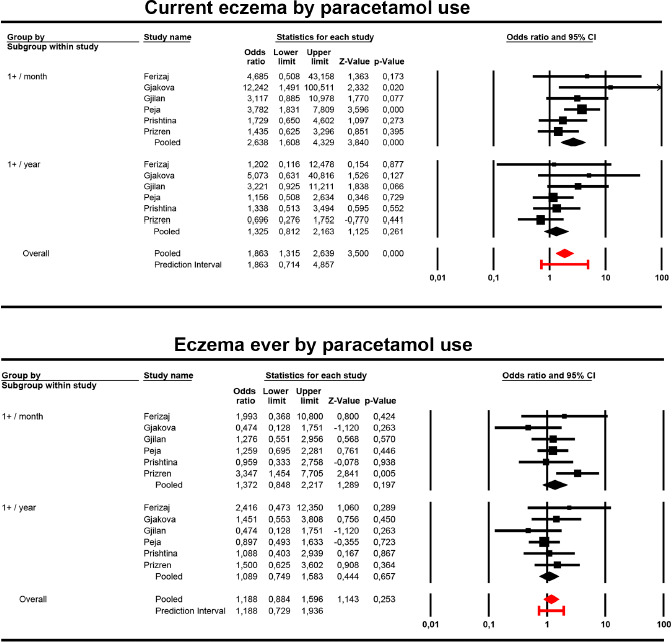
Contrary to exercise, paracetamol intake appeared to have a dose–response pattern of association, especially for current eczema symptoms. The pooled aOR were 1.33 and 2.64, and 95% CI were 0.81–2.16 and 1.61–4.33 for the intake of “at least once a year” and for “at least once a month,” respectively. The corresponding data for eczema ever were: pooled aOR 1.09, 95% CI 0.75–1.58) and pooled aOR 1.37 and 95% CI 0.85–2.22, respectively (Figure 3).
Figure 3 Forest plot of random meta-analysis of the association of paracetamol intake with current eczema symptoms (flexural itchy rash—upper panel; Q = 16.31, P = 0.130 [overall]; I2 = 32.57% [overall]) and eczema ever (lower panel; Q = 12.26, P = 0.344; I2 = 10.29%).
According to the results of multilevel analyses, stratification by wheezing did not change the patterns of associations, although in the case of children who suffered from skin plus respiratory symptoms, these associations appeared as stronger. However, a low number of children in the eczema and wheezing group was considerably lower than in the eczema without wheezing group, making comparisons difficult (Table 2).
Table 2 Associations (adjusted† odds ratios) and their 95% CI (in parentheses) between gender, exercise, and paracetamol intake with current eczema symptoms (upper panel) and eczema ever (lower panel) in six Kosovar cities in the mixed effects multilevel logistic regression analyses.
| Current eczema symptoms | |||
|---|---|---|---|
| Overall | With wheezing | Without wheezing | |
| Males | 0.52 (0.39–0.68) | 0.52 (0.39–0.71) | 0.50 (0.27–0.92) |
| Physical exercise | |||
| Never or occasionally | 1 | 1 | 1 |
| Once or twice a week | 2.59 (1.97–13.41) | 2.22 (1.65–3.00) | 6.10 (2.90–12.4) |
| Three or more times a week | 3.11 (2.14–4.53) | 2.30 (1.47–3.57) | 10.0 (4.47–22.5) |
| Paracetamol in the last 12 months | |||
| Never | 1 | 1 | 1 |
| At least for one time | 1.50 (0.98–2.30) | 1.34 (0.85–2.10) | 3.70 (0.84–16.3) |
| At least for one time per month | 2.75 (1.81–4.17) | 2.39 (1.54–3.72) | 7.16 (1.69–30.5) |
| Eczema ever | |||
| Ever | With wheezing | Without wheezing | |
| Males | 0.72 (0.56–0.92) | 0.69 (0.52–0.90) | 0.88 (0.50–1.56) |
| Physical exercise | |||
| Never or occasionally | 1 | 1 | 1 |
| Once or twice a week | 1.68 (1.29–2.19) | 1.56 (1.17–2.09) | 2.31 (1.27–4.19) |
| Three or more times a week | 2.04 (1.40–2.97) | 1.78 (1.16–2.74) | 3.32 (1.57–7.00) |
| Paracetamol in last 12 months | |||
| Never | 1 | 1 | 1 |
| At least for one time | 1.16 (0.83–1.62) | 1.14 (0.80–1.64) | 1.29 (0.53–3.10) |
| At least for one time per month | 1.44 (1.02–2.03) | 1.29 (0.88–1.88) | 2.34 (1.00–5.47) |
†Adjusted for all variables in the table, and for age, screen and television time, siblings, truck frequency, cat and dog ownership, tobacco smoking, vaping, and overweight.
Discussion
In this cross-sectional epidemiological study, we discovered a very low prevalence of any of the three atopic eczema markers, compared to other GAN centers.3
Although no study was conducted on the epidemiology of atopic eczema in Kosovo, there were some in Balkans. In the ISAAC phase III survey,5 carried out around 2002, Tiranë (Albania) reported the prevalence of eczema markers as defined in the present study as follows: current eczema symptoms, 2.0%; severe eczema symptoms, 0.2%; and eczema ever, 2.9%. Furthermore, the corresponding data for Rijeka (Croatia) and Skope (Republic of Macedonia) were 2.9%, 0.2%, and 8.5%; and 2.7%, 0.3%, and 3.7%, respectively. Data were available from five centers in Serbia and Montenegro, with the following proportions: current eczema symptoms, 2.8%–8.0%, severe eczema symptoms, 0.5%–1.3%, and eczema ever, 8.2–17.9%, respectively. The study report by Zivković et al.7 on Serbia and Montenegro elaborated further the data included in the ISAAC phase III report and showed low prevalence proportions of other eczema markers.
Apart from offering the first epidemiological data on atopic eczema in Kosovo, it was interesting to study epidemiological factors that could be associated with this condition in a very low-prevalence geographical area, where, to the best of our knowledge, those factors were not studied among adolescents. Male gender was independently associated with a significant lower prevalence of both current eczema symptoms and eczema ever (if Prizren is excluded in the latter case) (Figure 1). The prevalence of severe eczema symptoms was excessively low to allow any multivariate statistics. The influence of gender on atopic eczema was previously studied in adolescents in Balkans: Stipic-Markovic et al.9 found no association between eczema markers and gender in Zagreb among adolescents included in the ISAAC phase III survey. However, other studies discovered that different eczema markers were significantly more prevalent in females in this age group, similar to the study conducted by Mercer et al. in Cape Town (South Africa).16 In the EPI-CARE study, a recently conducted international cross-sectional study comprising children aged 6 months–<12 years and adolescents aged 12–<18 years using ISAAC methods and defining atopic dermatitis with the same criteria as defined in the present study, found that prevalence differences by gender, in one or other direction, existed only in some countries.17 However, Silverberg et al. did not report these differences separately in the two age groups studied.17 In the BAMSE (Swedish abbreviation for Children, Allergy, Milieu, Stockholm, Epidemiology) longitudinal population-based cohort study carried out in Stockholm, Sweden, the follow-up visit of children aged 11–14 years demonstrated a significantly higher prevalence among females when using an eczema questionnaire specifically designed for the study.18 The same results were discovered in a large international cross-sectional study among adults aged 18–65 years19 as well as in a Swedish study comprising individuals aged 17–75 years which used the GA2LEN (a network of excellence of leading European clinical and research facilities in the field of allergology and asthma) questionnaire to assess eczema symptoms.20 These findings were shared by other studies as well.21,22 A recent BAMSE cohort report comprising individuals aged 24 years further broadened the finding concerning lower prevalence of eczema markers in males.23 Sex hormones appeared to have a role in this difference after puberty.24
The current eczema symptoms and eczema ever were also associated with physical exercise, apparently not in a dose–response manner. Doing regular exercise was significantly associated with the overall prevalence of both atopic eczema markers, although this was not the case in some of the centers (Figure 2). As observed, exercise was associated with eczema in the past as well, although the information is quite limited. In a systematic review and meta-analysis conducted by Kim and Silverberg25 in 2016, only seven manuscripts were located after searching all relevant literature databases since their existence. Three studies contained some association between exercise and eczema, three studies showed an inverse relationship, and one study did not find any association. Only five of these seven studies had enough data to be included in the meta-analysis which yielded nonsignificant summary effects, but, interestingly, the only study comprising adolescents showed a significant positive association.26 Two other studies (not included in the meta-analysis) which had positive associations comprised children or adolescents.27,28 Only one of the studies showing no association comprised adolescents. It should be noted that this study included 481 individuals.29 All these studies comprising adolescents and children used the ISAAC methodology, which required a sample size of 3000. More recent studies offer additional information. For instance, Jago et al.,30 using accelerometers in the Avon Longitudinal Study of Parents and Children (ALSPAC) population of 6473 adolescents, concluded that the period of vigorous exercise (in minutes) is not related to either asthma or eczema but is inversely associated with obesity. The nature of ISAAC study (cross-sectional) versus the ALSPAC study (longitudinal) and the different ways of measuring physical exercise (simple questionnaire vs. accelerometer) could explain the discrepancy. However, it cannot be ruled out that low to moderate exercise is associated with higher prevalence of eczema, while moderate to vigorous is not. It could be that low-intensity exercise with skin exposure to environment and climate aggression and sweat could facilitate mild eczema flares in not highly predisposed individuals. In contrast, highly predisposed individuals avoid vigorous exercise to escape severe flares of eczema. In fact, as previously observed, in adults, disease severity is associated with decreased levels of physical activity secondary to itch.31 The curve of association between the amount of exercise and the severity of eczema (and thus, awareness in self-reported surveys) is inverted U shape.
On the other hand, Honjo et al. discovered a positive independent association of exercise-induced wheezing with eczema in a group of 12,405 asthmatic children aged 6–18 years following ISAAC definitions.32 This was probably comparable with our findings that the association of exercise with eczema was higher in the adolescents who reported current wheezing (Table 2). We are not able to confirm whether the proportion of atopy was higher in wheezing individuals than in non-wheezing individuals, but this possibility cannot be ruled out.
The third factor that was consistently associated with eczema markers was paracetamol usage, both at least for one time in the last year and at least for one time in last month (Figure 3). This was more consistent for current eczema symptoms than for eczema ever and was probably determined in individuals having both eczema and wheezing (Table 2).
Various reports linking the use of paracetamol with eczema are disclosed, even demonstrating that this association is higher when several allergic diseases coexist.33–36 Thus, it cannot be stated whether the association between paracetamol and eczema is controlled by asthma and/or rhino-conjunctivitis, and/or allergy. The present study demonstrated that the association with frequent use of paracetamol (at least for one time in the last month) applied even to adolescents without current wheezing, but only for the current symptoms of the condition. A previous study demonstrated the effects of early paracetamol intake on eczema in children aged 6–7 years having neither asthma nor rhino-conjunctivitis symptoms.37 This probably indicated that the drug impairs the antioxidant system, crucial to maintain skin integrity after aggression.38
The cross-sectional disposition of the current study precluding to obtain any causal relationship was its limitation. On the other hand, the study was conducted using validated methods with a quite larger sample with high participation proportion, which was representative of the whole country of Kosovo. It had an additional interest of being an area with quite low prevalence of atopic eczema.
Conclusions
In summary, this study demonstrated that in an area of low prevalence of atopic eczema, gender, physical exercise, and paracetamol usage are associated with the number of eczema cases, as well as those in adolescents without current asthma symptoms. Lower prevalence was discovered in males whereas mild-to-moderate physical exercise and frequent use of paracetamol were associated with higher prevalence of the condition.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors acknowledged all participating children and their parents as well as all teachers who facilitated the fieldwork. Especial thanks to T. Hoxha and H. Hoti, physicians at the Main Family Medicine Center (Prishtina), who provided support to the study.
Financial support
A. Elena Martinez-Torres and L. Garcia-Marcos were partly funded by Instituto de Salud Carlos III, Spain (Grant No. PI17/0170).
REFERENCES
1 Mosam A, Todd G. Global epidemiology and disparities in atopic dermatitis. Br J Dermatol. 2023;188 (6):726–37. 10.1093/bjd/ljad042
2 Langan SM, Mulick AR, Rutter CE, Silverwood Richard J, Asher I, García-Marcos L, et al. Trends in eczema prevalence in children and adolescents: A Global Asthma Network Phase I Study. Clin Exp Allergy 2023;53(3):337–52. 10.1111/cea.14276
3 García-Marcos L, Asher MI, Pearce N, Ellwood E, Bissell K, Chiang CY, et al. The burden of asthma, hay fever and eczema in children in 25 countries: GAN Phase I study. Eur Respir J 2022; 60(3):2102866. 10.1183/13993003.02866-2021
4 Serajuddin B and Hamadeh. New World Bank country classifications by income level: 2020-2021. [Internet]. [cited 2020]. Available from: https://blogs.worldbank.org/opendata/new-world-bank-country-classifications-income-level-2020-2021 (Accessed: March 15, 2021).
5 Odhiambo JA, Williams HC, Clayton TO, Robertson CF, Asher MI. Global variations in prevalence of eczema symptoms in children from ISAAC phase three. J Allergy Clin Immunol. 2009;124(6):1251–8.e23. 10.1016/j.jaci.2009.10.009
6 Suárez-Varela MM, García-Marcos Alvarez L, Kogan MD, González AL, Gimeno AM, Aguinaga Ontoso I, et al. Climate and prevalence of atopic eczema in 6-to 7-year-old school children in Spain. ISAAC phase III. Int J Biometeorol. 2008;52(8):833–40.10.1007/s00484-008-0177-0
7 Zivković Z, Vukašinović Z, Cerović S, Radulović S, Zivanović S, Panić E, et al. Prevalence of childhood asthma and allergies in Serbia and Montenegro. World J Pediatr. 2010;6(4):331–6. 10.1007/s12519-010-0207-y
8 Banac S, Tomulic KL, Ahel V, Rozmanic V, Simundic N, Zubovic S, et al. Prevalence of asthma and allergic diseases in Croatian children is increasing: Survey study. Croat Med J. 2004;45(6):721–6.
9 Stipic-Markovic A, Pevec B, Pevec MR, Custovic A. Prevalence of symptoms of asthma, allergic rhinitis, conjunctivitis and atopic eczema: ISAAC (International Study of Asthma and Allergies in Childhood) in a population of schoolchildren in Zagreb]. Acta Med Croatica. 2003;57(4):281–5.
10 Munivrana Skvorc H, Plavec D, Munivrana S, Skvorc M, Nogalo B, Turkalj M. Prevalence of and risk factors for the development of atopic dermatitis in schoolchildren aged 12–14 in northwest Croatia. Allergol Immunopathol (Madr). 2014;42(2):142–8. 10.1016/j.aller.2012.10.008
11 Vlaski E, Stavric K, Seckova L, Kimovska Hristova M, Isjanovska R. The self-reported density of truck traffic on residential streets and the impact on asthma, hay fever and eczema in young adolescents. Allergol Immunopathol (Madr). 2014;42(3):224–9. 10.1016/j.aller.2012.10.011
12 Ellwood P, Asher MI, Billo NE, Bissell K, Chiang CY, Ellwood EM, et al. The Global Asthma Network rationale and methods for phase I global surveillance: Prevalence, severity, management and risk factors. Eur Respir J. 2017;49(1):1601605. 10.1183/13993003.01605-2016
13 Ellwood P, Williams H, Ait-Khaled N, Bjorksten B, Robertson C, Group IPIS. Translation of questions: The International Study of Asthma and Allergies in Childhood (ISAAC) experience. Int J Tuberc Lung Dis. 2009;13(9):1174–82.
14 Ellwood P, Ellwood E, Rutter C, Perez-Fernandez V, Morales E, Garcia-Marcos L, et al. Global Asthma Network Phase I surveillance: Geographical coverage and response rates. J Clin Med. 2020;9(11) :3688. 10.3390/jcm9113688
15 Ahmetaj L, Martinez-Torres AE, Ahmetaj Y, Ismajli I, Gashi V, Kurhasani X, et al. The role of Human Development Index in the epidemiology of asthma in adolescents in Kosovo: A cross-sectional multicentre Global Asthma Network (GAN) study. Allergol Immunopathol (Madr). 2023;51(2):59–70. 10.15586/aei.v51i2.781
16 Mercer MJ, Joubert G, Ehrlich RI, Nelson H, Poyser MA, Puterman A, et al. Socioeconomic status and prevalence of allergic rhinitis and atopic eczema symptoms in young-adolescents. Pediatr Allergy Immunol. 2004;15(3):234–41. 10.1111/j.1399-3038.2004.00125.x
17 Silverberg JI, Barbarot S, Gadkari A, Simpson EL, Weidinger S, Mina-Osorio P, et al. Atopic dermatitis in the pediatric population: A cross-sectional, international epidemiologic study. Ann Allergy Asthma Immunol. 2021;126(4):417–28 e2. 10.1016/j.anai.2020.12.020
18 Ballardini N, Kull I, Soderhall C, Lilja G, Wickman M, Wahlgren CF. Eczema severity in preadolescent children and its relation to sex, filaggrin mutations, asthma, rhinitis, aggravating factors and topical treatment: A report from the BAMSE birth cohort. Br J Dermatol. 2013;168(3):588–94. 10.1111/bjd.12196
19 Barbarot S, Auziere S, Gadkari A, Girolomoni G, Puig L, Simpson EL, et al. Epidemiology of atopic dermatitis in adults: Results from an international survey. Allergy. 2018;73(6):1284–93. 10.1111/all.13401
20 Ronmark EP, Ekerljung L, Lotvall J, Wennergren G, Ronmark E, Toren K, et al. Eczema among adults: prevalence, risk factors and relation to airway diseases. Results from a large-scale population survey in Sweden. Br J Dermatol. 2012;166(6):1301–8. 10.1111/j.1365-2133.2012.10904.x
21 Abuabara K, Ye M, McCulloch CE, Sullivan A, Margolis DJ, Strachan DP, et al. Clinical onset of atopic eczema: Results from 2 nationally representative British birth cohorts followed through midlife. J Allergy Clin Immunol. 2019;144(3):710–9. 10.1016/j.jaci.2019.05.040
22 Saeki H, Tsunemi Y, Fujita H, Kagami S, Sasaki K, Ohmatsu H, et al. Prevalence of atopic dermatitis determined by clinical examination in Japanese adults. J Dermatol. 2006;33(11):817–9. 10.1111/j.1346-8138.2006.00187.x
23 Johansson EK, Bergstrom A, Kull I, Melen E, Jonsson M, Lundin S, et al. Prevalence and characteristics of atopic dermatitis among young adult females and males–report from the Swedish population-based study BAMSE. J Eur Acad Dermatol Venereol. 2022;36(5):698–704. 10.1111/jdv.17929
24 Kanda N, Hoashi T, Saeki H. The roles of sex hormones in the course of atopic dermatitis. Int J Mol Sci. 2019;20(19):4660. 10.3390/ijms20194660
25 Kim A, Silverberg JI. A systematic review of vigorous physical activity in eczema. Br J Dermatol. 2016;174(3):660–2. 10.1111/bjd.14179
26 Al-Sahab B, Atoui M, Musharrafieh U, Zaitoun F, Ramadan F, Tamim H. Epidemiology of eczema among Lebanese adolescents. Int J Public Health. 2008;53(5):260–7. 10.1007/s00038-008-7085-2
27 Mitchell EA, Beasley R, Keil U, Montefort S, Odhiambo J. The association between tobacco and the risk of asthma, rhinoconjunctivitis and eczema in children and adolescents: Analyses from phase three of the ISAAC programme. Thorax. 2012;67(11):941–9. 10.1136/thoraxjnl-2011-200901
28 Foliaki S, Annesi-Maesano I, Tuuau-Potoi N, Waqatakirewa L, Cheng S, Douwes J, et al. Risk factors for symptoms of childhood asthma, allergic rhinoconjunctivitis and eczema in the Pacific: An ISAAC phase III study. Int J Tuberc Lung Dis. 2008;12(7):799–806.
29 Brescianini S, Brunetto B, Iacovacci P, D'Ippolito C, Alberti G, Schirru MA, et al. Prevalence of self-perceived allergic diseases and risk factors in Italian adolescents. Pediatr Allergy Immunol. 2009;20(6):578–84. 10.1111/j.1399-3038.2008.00793.x
30 Jago R, Salway RE, Ness AR, Shield JPH, Ridd MJ, Henderson AJ. Associations between physical activity and asthma, eczema and obesity in children aged 12–16: An observational cohort study. BMJ Open. 2019;9(1):e024858. 10.1136/bmjopen-2018-024858
31 Schwartzman G, Lei D, Ahmed A, Chavda R, Gabriel S, Silverberg JI. Association of adult atopic dermatitis severity with decreased physical activity: A cross-sectional study. Dermatitis.2023;34(3):218–23.10.1097/DER.0000000000000921
32 Honjo S, Murakami Y, Odajima H, Adachi Y, Yoshida K, Ohya Y, et al. An independent relation of atopic dermatitis to exercise-induced wheezing in asthmatic children. Allergol Int. 2019;68(1):26–32. 10.1016/j.alit.2018.04.013
33 Beasley R, Clayton T, Crane J, von Mutius E, Lai CK, Montefort S, et al. Association between paracetamol use in infancy and childhood, and risk of asthma, rhinoconjunctivitis, and eczema in children aged 6–7 years: Analysis from phase three of the ISAAC programme. Lancet. 2008;372(9643):1039–48. 10.1016/S0140-6736(08)61445-2
34 Beasley RW, Clayton TO, Crane J, Lai CK, Montefort SR, Mutius E, et al. Acetaminophen use and risk of asthma, rhinoconjunctivitis, and eczema in adolescents: International Study of Asthma and Allergies in Childhood phase three. Am J Respir Crit Care Med. 2011;183(2):171–8. 10.1164/rccm.201005-0757OC
35 Suárez-Varela MM, García-Marcos L, Fernández-Espinar JF, Bercedo-Sanz A, Aguinaga-Ontoso I, González-Díaz C, et al. Is acetaminophen use associated with atopic eczema and other allergic diseases in adolescents? Iran J Allergy Asthma Immunol. 2013;12(2):115–23.
36 Xiao D, Su X, Qu Y, Zhou Y, Pan L, Li X, et al. Association of acetaminophen exposure with increased risk of eczema in children: A meta-analysis. J Am Acad Dermatol. 2019;81(2):642–4. 10.1016/j.jaad.2019.04.017
37 Garcia-Marcos L, Gonzalez-Diaz C, Garvajal-Uruena I, Pac-Sa MR, Busquets-Monge RM, Suarez-Varela MM, et al. Early exposure to paracetamol or to antibiotics and eczema at school age: modification by asthma and rhinoconjunctivitis. Pediatr Allergy Immunol. 2010;21(7):1036–42. 10.1111/j.1399-3038.2010.01037.x
38 Puri P, Nandar SK, Kathuria S, Ramesh V. Effects of air pollution on the skin: A review. Indian J Dermatol Venereol Leprol. 2017;83(4):415–23. 10.4103/0378-6323.199579
Supplementary
Table S1 Associations (non-adjusted and adjusted† odds ratios) and their 95% CI (in parentheses) between epidemiological factors and current eczema in six Kosovar cities.
| Ferizaj n = 890 | Gjakova n = 676 | Gjilan n = 1200 | Peja n = 1433 | Prishtina n = 1056 | Prizren n = 1427 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | aOR | OR | aOR | OR | aOR | OR | aOR | OR | aOR | OR | aOR | |
| Males | 0.29 (0.10–0.89) | 0.26 (0.05–1.28) | 0.40 (0.18–0.90) | 0.42 (0.18–1.00) | 0.58 (0.32–1.05) | 0.34 (0.16–0.72) | 0.49 (0.30–0.80) | 0.48 (0.28–0.84) | 0.40 (0.22–0.73) | 0.42 (0.21–0.84) | 1.25 (0.76–2.05) | 0.85 (0.47–1.55) |
| Physical exercise | ||||||||||||
| Never or occasionally | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Once or twice a week | 1.21 (0.33–4.38) | 1.11 (0.26–4.82) | 4.99 (2.49–10.0) | 5.79 (2.72–12.3) | 1.20 (0.56–2.56) | 1.05 (0.46–2.37) | 2.97 (1.76–5.01) | 2.36 (1.36–4.09) | 2.52 (1.41–4.50) | 2.40 (1.25–4.60) | 4.79 (2.71–8.47) | 3.93 (2.11–7.33) |
| Three or more times a week | 8.66 (3.04–24.6) | 23.6 (5.39–103.2) | 2.37 (0.52–10.8) | 2.21 (0.42–11.7) | 3.47 (1.68–7.17) | 3.50 (1.53–8.00) | 2.13 (1.03–4.41) | 1.94 (0.89–4.20) | 1.23 (0.46–3.31) | 1.26 (0.41–3.88) | 5.14 (2.39–11.0) | 4.12 (1.78–9.53) |
| Television/computer (hours) | 1.10 (0.85–1.41) | 1.17 (0.82–1.67) | 1.11 (0.87–1.41) | 1.10 (0.83–1.45) | 1.23 (1.04–1.45) | 1.34 (1.10–1.62) | 1.09 (0.95–1.26) | 1.03 (0.89–1.21) | 1.21 (1.02–1.44) | 1.09 (0.89–1.33) | 1.44 (1.24–1.68) | 1.28 (1.07–1.53) |
| Older siblings (number) | 0.68 (0.43–1.07) | 0.57 (0.30–1.10) | 1.30 (0.91–1.85) | 1.87 (1.17–2.99) | 0.91 (0.69–1.20) | 1.01 (0.74–1.40) | 1.15 (0.93–1.43) | 1.13 (0.89–1.44) | 1.15 (0.90–1.48) | 1.03 (0.74–1.44) | 1.15 (0.92–1.43) | 1.11 (0.84–1.45) |
| Younger siblings (number) | 1.18 (0.76–1.83) | 1.15 (0.60–2.22) | 0.97 (0.66–1.43) | 1.36 (0.83–2.23) | 1.38 (1.04–1.85) | 1.56 (1.10–2.21) | 0.91 (0.71–1.16) | 0.91 (0.69–1.21) | 0.74 (0.54–1.01) | 0.69 (0.46–1.04) | 0.71 (0.54–0.94) | 0.83 (0.60–1.14) |
| Truck frequency on weekdays | ||||||||||||
| Never | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Seldom (not often) | NA | NA | NA | 0.37 (0.09–1.61) | NA | 1.52 (0.43–5.43) | NA | 1.27 (0.48–3.39) | NA | 037 (0.15–0.91) | NA | 0.96 (0.34–2.66) |
| Frequently through the day | NA | NA | NA | 0.72 (0.17–3.01) | NA | 1.30 (0.33–5.09) | NA | 1.35 (0.48–3.81) | NA | 0.50 (0.19–1.27) | NA | 1.20 (0.41–3.48) |
| Almost the whole day | NA | NA | NA | 0.67 (0.13–3.42) | NA | 1.60 (0.34–7.45) | NA | 1.27 (0.39–4.14) | NA | 0.23 (0.05–0.94) | NA | 2.04 (0.60–6.92) |
| Paracetamol in last 12 months | ||||||||||||
| Never | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| At least once a year | 0.97 (0.18–5.36) | 1.20 (0.12–12.5) | 6.27 (0.84–47.0) | 5.07 (0.63–40.8) | 3.85 (1.14–13.0) | 3.22 (0.93–11.2) | 1.26 (0.56–2.83) | 1.16 (0.51–2.63) | 1.67 (0.67–4.21) | 1.34 (0.51–3.49) | 0.80 (0.36–1.78) | 0.70 (0.28–1.75) |
| At least once a month | 3.42 (0.76–15.4) | 4.68 (0.51–43.2) | 14.0 (1.81–108.2) | 12.24 (1.49–100.5) | 5.21 (1.54–17.7) | 3.12 (0.88–11.0) | 5.25 (2.62–10.5) | 3.78 (1.83–7.81) | 3.11 (1.25–7.72) | 1.73 (0.65–4.60) | 1.88 (0.92–3.83) | 1.43 (0.62–3.30) |
| Cat ownership last 12 months | 3.86 (1.23–12.1) | 7.10 (1.59–31.7) | 1.03 (0.36–3.01) | 1.30 (0.41–4.10) | 0.79 (0.31–2.04) | 0.95 (0.34–2.64) | 1.27 (0.69–2.36) | 1.07 (0.55–2.11) | 0.56 (0.17–1.83) | 0.40 (0.08–1.88) | 0.88 (0.40–1.19) | 0.70 (0.29–1.68) |
| Dog ownership last 12 months | 1.14 (0.40–3.23) | 0.39 (0.90–1.67) | 1.07 (0.43–2.63) | 0.66 (0.21–2.07) | 0.59 (0.27–1.27) | 0.51 (0.22–1.19) | 1.60 (0.98–2.62) | 1.52 (0.88–2.62) | 0.76 (0.34–1.72) | 0.71 (0.26–1.98) | 1.37 (0.80–2.33) | 1.17 (0.62–2.23) |
| Tobacco smoking ever | 1.55 (0.20–12.0) | NA | NA | NA | 3.02 (0.67–13.5) | 8.14 (0.86–77.4) | NA | NA | 2.07 (0.47–9.21) | 0.34 (0.006–20.7) | 2.82 (0.96–8.24) | 0.62 (0.11–3.50) |
| Tobacco smoking currently | 2.58 (0.33–20.5) | NA | 4.41 (0.48–40.5) | NA | 2.64 (0.33–21.3) | 0.44 (0.02–9.24) | NA | NA | 1.75 (0.22–13.9) | 2.92 (0.05–182.3) | 2.16 (0.49–9.51) | 2.30 (0.25–21.1) |
| Vaping currently | 1.78 (0.40–7.94) | 0.62 (0.05–7.18) | NA | NA | 1.72 (0.84–3.52) | 1.87 (0.80–4.40) | 1.69 (0.82–3.50) | 1.90 (0.81–4.46) | 2.60 (1.26–5.37) | 2.45 (1.03–5.81) | 2.45 (1.36–4.42) | 1.59 (0.78–3.25) |
| Excess weight | ||||||||||||
| Overweight | 1.65 (0.37–7.28) | 1.62 (0.25–10.5) | 0.37 (0.05–2.78) | 0.47 (0.06–3.77) | 0.44 (0.10–1.82) | 0.52 (0.12–2.30) | 1.15 (0.54–2.46) | 1.05 (0.45–2.42) | 0.51 (0.15–1.65) | 0.56 (0.16–1.92) | 1.38 (0.67–2.84) | 1.31 (0.61–2.81) |
| Obesity | NA | NA | NA | NA | 1.68 (0.39–7.28) | 2.45 (0.52–11.6) | 0.87 (0.11–6.56) | 0.91 (0.12–7.18) | 1.66 (0.68–4.02) | 1.28 (0.41–3.97) | NA | NA |
†Adjusted for all variables given in the table. NA: not applicable due to very low numbers.
Table S2 Associations (non-adjusted and adjusted† odds ratios) and their 95% CI (in parentheses) between epidemiological factors and eczema ever in six Kosovar cities.
| Ferizaj N = 890 | Gjakova N = 676 | Gjilan N = 1200 | Peja N = 1433 | Prishtina N = 1056 | Prizren N = 1427 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | aOR | OR | aOR | OR | aOR | OR | aOR | OR | aOR | OR | aOR | |
| Males | 0.96 (0.45–2.08) | 0.84 (0.30–2.31) | 0.81 (0.43–1.51) | 0.81 (0.41–1.60) | 0.56 (0.31–1.01) | 0.51 (0.27–0.98) | 0.57 (0.36–0.89) | 0.51 (0.31–0.84) | 0.50 (0.26–0.97) | 0.35 (0.16–0.78) | 1.28 (0.84–1.96) | 1.45 (0.88–2.40) |
| Physical exercise | ||||||||||||
| Never or occasionally | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Once or twice a week | 4.29 (1.85–9.94) | 4.16 (1.47–11.8) | 3.81 (2.01–7.21) | 4.15 (2.14–8.05) | 0.98 (0.47–2.08) | 0.82 (0.38–1.79) | 1.66 (0.98–2.79) | 1.46 (0.84–2.54) | 3.04 (1.52–6.08) | 2.72 (1.26–5.91) | 1.43 (0.89–2.29) | 1.07 (0.63–1.84) |
| Three or more times per week | 3.68 (1.00–13.5) | 4.96 (1.15–21.4) | 3.68 (1.18–11.5) | 5.68 (1.61–20.0) | 1.48 (0.60–3.60) | 1.47 (0.56–3.82) | 1.65 (0.84–3.26) | 1.88 (0.91–3.87) | 2.43 (0.92–6.41) | 3.10 (1.11–8.68) | 1.47 (0.70–3.06) | 1.40 (0.64–3.03) |
| Television/computer (hours) | 1.00 (0.80–1.26) | 0.96 (0.72–1.29) | 1.18 (0.95–1.45) | 1.23 (0.95–1.58) | 1.15 (0.97–1.35) | 1.11 (0.92–1.33) | 1.05 (0.92–1.21) | 1.07 (0.92–1.23) | 1.01 (0.82–1.23) | 0.98 (0.77–1.24) | 1.24 (1.09–1.41) | 1.19 (1.02–1.39) |
| Older siblings (number) | 0.84 (0.58–1.20) | 0.79 (0.48–1.30) | 1.04 (0.76–1.43) | 1.05 (0.70–1.57) | 0.91 (0.69–1.20) | 0.88 (0.65–1.20) | 0.93 (0.75–1.16) | 0.88 (0.69–1.11) | 0.79 (0.58–1.09) | 0.75 (0.50–1.12) | 0.94 (0.77–1.14) | 0.91 (0.72–1.15) |
| Younger siblings (number) | 0.91 (0.61–1.35) | 0.82 (0.46–1.46) | 0.83 (0.57–1.20) | 0.92 (0.59–1.43) | 0.98 (0.72–1.33) | 0.97 (0.68–1.38) | 0.92 (0.73–1.17) | 0.86 (0.66–1.12) | 0.87 (0.62–1.22) | 0.72 (0.46–1.13) | 0.93 (0.75–1.16) | 1.02 (0.79–1.33) |
| Truck frequency on weekdays | ||||||||||||
| Never | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Seldom (not often) | 0.57 (0.15–2.19) | 0.35 (0.07–1.72) | 1.26 (0.36–4.44) | 0.88 (0.23–3.43) | 5.98 (0.81–44.4) | 5.74 (0.75–43.8) | 0.90 (0.44–1.83) | 0.73 (0.35–1.52) | 1.98 (0.45–8.59) | 1.52 (0.33–7.00) | 1.13 (0.56–2.27) | 1.52 (0.62–3.70) |
| Frequently through the day | 1.25 (0.34–4.64) | 1.05 (0.23–4.89) | 1.64 (0.48–5.68) | 1.22 (0.32–4.69) | 8.12 (1.06–62.1) | 7.89 (1.00–61.9) | 1.38 (0.65–2.94) | 1.12 (0.51–2.44) | 2.67 (0.60–11.9) | 2.48 (0.52–11.8) | 1.54 (0.73–3.23) | 2.04 (0.80–5.17) |
| Almost the whole day | 1.30 (0.30–5.59) | 0.54 (0.09–3.13) | 1.04 (0.22–4.82) | 0.82 (0.16–4.15) | 11.2 (1.36–92.5) | 10.5 (1.22–89.9) | 0.48 (0.15–1.56) | 0.39 (0.12–1.29) | 2.45 (0.46–12.9) | 1.73 (0.29–10.2) | 0.81 (0.25–2.66) | 0.65 (0.15–2.76) |
| Paracetamol in last 12 months | ||||||||||||
| Never | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| At least once a year | 1.47 (0.47–4.65) | 2.42 (0.47–12.3) | 1.64 (0.67–4.01) | 1.45 (0.55–3.81) | 1.13 (0.50–2.53) | 0.96 (0.42–2.21) | 1.03 (0.58–1.83) | 0.90 (0.49–1.63) | 1.42 (0.56–3.64) | 1.09 (0.40–2.94) | 1.66 (0.74–3.73) | 1.50 (0.62–3.60) |
| At least once a month | 1.15 (0.35–3.81) | 1.99 (0.37–10.8) | 0.74 (0.22–2.49) | 0.47 (0.13–1.75) | 1.70 (0.76–3.77) | 1.28 (0.55–2.96) | 1.56 (0.89–2.73) | 1.26 (0.70–2.28) | 1.80 (0.69–4.72) | 0.96 (0.33–2.76) | 3.21 (1.50–6.87) | 3.35 (1.45–7.70) |
| Cat ownership last 12 months | 1.88 (0.54–6.48) | 1.81 (0.44–7.40) | 1.89 (0.85–4.24) | 2.21 (0.92–5.32) | 1.36 (0.63–2.96) | 1.48 (0.65–3.39) | 1.58 (0.91–2.76) | 1.55 (0.85–2.84) | 1.11 (0.39–3.19) | 1.65 (0.51–5.39) | 1.21 (0.67–2.20) | 1.37 (0.68–2.77) |
| Dog ownership last 12 months | 1.40 (0.60–3.30) | 1.38 (0.50–3.76) | 0.81 (0.34–1.97) | 0.78 (0.29–2.13) | 0.76 (0.37–1.54) | 0.68 (0.32–1.47) | 1.03 (0.63–1.70) | 1.00 (0.59–1.70) | 0.58 (0.20–1.65) | 0.62 (0.19–2.01) | 0.96 (0.59–1.56) | 0.92 (0.52–1.62) |
| Tobacco smoking ever | 2.50 (0.56–11.1) | 0.88 (0.07–11.0) | NA | NA | 1.36 (0.18–10.4) | 6.75 (0.66–68.6) | 0.53 (0.07–3.94) | 0.76 (0.08–7.10) | 1.39 (0.18–10.7) | 0.32 (0.01–16.6) | 1.94 (0.67–5.64) | 2.47 (0.64–9.53) |
| Tobacco smoking currently | 4.27 (0.93–19.6) | 4.97 (0.37–67.3) | NA | NA | NA | NA | 0.59 (0.08–4.39) | 0.85 (0.09–8.16) | 2.46 (0.31–19.7) | 7.20 (0.13–389.1) | 1.51 (0.35–6.59) | NA |
| Vaping currently | 2.99 (0.99–9.08) | 0.96 (0.18–5.31) | NA | NA | 1.46 (0.70–3.07) | 1.60 (0.71–3.59) | 1.09 (0.49–2.42 | 1.30 (0.52–3.26) | 1.58 (0.60–4.16) | 1.64 (0.55–4.91) | 1.34 (0.74–2.44) | 0.96 (0.48–1.91) |
| Excess weight | ||||||||||||
| Overweight | NA | NA | 0.29 (0.04–2.18) | 0.33 (0.04–2.48) | 1.43 (0.59–3.43) | 1.59 (0.64–3.90) | 1.29 (0.65–2.56) | 1.25 (0.62–2.54) | 1.83 (0.79–4.26) | 2.45 (0.98–6.12) | 1.69 (0.93–3.07) | 1.53 (0.80–2.91) |
| Obesity | 3.36 (0.96–11.8) | 3.99 (0.72–22.1) | NA | NA | 0.85 (0.11–6.39) | 0.79 (0.10–6.13) | NA | NA | 1.18 (0.35–3.97) | 1.83 (0.51–6.54) | 1.81 (0.62–5.22) | 2.01 (0.56–7.17) |
†Adjusted for all variables in the table. NA: not applicable due to very low number.