
Download
ORIGINAL ARTICLE
Real-World Study of Ragweed Sublingual Immunotherapy in Hungary
Adrienne Nagya*, Katalin Baloghb, Csilla Csákic, Beáta Fábosd, Edit Mohácsie, Gábor Pappf
aHeim Pál National Pediatric Institute, Budapest, Hungary
bBuda Allergy Centrum, Budapest, Hungary
cCalvinistic Pulmonological Centrum, Törökbálint, Hungary
dKaposi Mór Teaching Hospital, Kaposvár, Hungary
eSt. Janos North-Buda Centrum Hospital, Budapest, Hungary
fUniversity of Pécs, Szigetvár, Hungary
Abstract
Background: Ragweed (Ambrosia elatior) has become invasive in Europe, causing significant respiratory issues. Subcutaneous allergen immunotherapy (SCIT) has long been used to manage pollen allergies, but sublingual immunotherapy (SLIT) has gained interest.
Objective: This study aimed to evaluate the clinical benefits of ragweed SLIT under real-world in a cohort of Hungarian patients allergic to ragweed pollen.
Methods: We retrospectively reviewed the clinical records of 57 patients during the 2015 and 2016 ragweed pollen seasons. Patients were divided into two groups: Group 1 (n = 29), who had not received immunotherapy, and Group 2 (n = 28), who had previously undergone immunotherapy with another sublingual preparation. All patients were treated with Oraltek® ragweed for 4–6 months, initiating 2–4 months before the pollen season and rest of the period was 2 months of the 2016 pollen season. Symptom score (SS), medication score (MS), and combined symptom and medication score (CSMS) were evaluated intra- and intergroup.
Results: Pollen counts were consistent between 2015 and 2016. All patients showed significant improvement in SS, MS, and CSMS, with a large effect size (>0.8). Group 2 had significantly lower SS and CSMS in 2015 because of prior immunotherapy. By 2016, both groups exhibited marked improvements, with Group 1 showing a 75% improvement in CSMS. No local or systemic reactions were recorded, indicating a high safety profile.
Conclusions: Ragweed SLIT significantly improved symptoms and reduced use of medication in patients allergic to ragweed pollen. The treatment was effective even in patients with previous immunotherapy, with a high benefit–risk ratio demonstrated by the absence of adverse reactions. These findings support the use of Oraltek SLIT for managing ragweed pollen allergy.
Key words: allergic rhinitis, immunotherapy safety, ragweed, real-life study, respiratory allergies, sublingual immunotherapy
*Corresponding author: Adrienne Nagy, Heim Pál National Pediatric Institute, Budapest, Hungary. Email address: [email protected]
Received 11 June 2024; Accepted 8 August 2024; Available online 1 September 2024
Copyright: Nagy A, et al.
License: This open access article is licensed under Creative Commons Attribution 4.0 International (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/
Introduction
Ragweed (Ambrosia elatior), native to North America, has become invasive in Europe, Australia, and Asia.1,2 In a comprehensive epidemiological study across multiple European centers involving more than 3000 patients with confirmed respiratory symptoms, the impact of ragweed pollen was evident.3 Notably, substantial differences were observed among countries, with prevalence ranging from 19.5% in South Bavaria to as high as 60% in Hungary.4,5
Subcutaneous allergen immunotherapy (SCIT) has been employed for more than a century in the management of pollen allergies, ragweed pollen being one of the most prominent allergens.6 Sublingual immunotherapy (SLIT) extracts has garnered increasing interest because of superior safety profile compared to SCIT with native unmodified allergen extracts.7
In this study, our objective was to assess the clinical benefits of ragweed SLIT under real-life conditions in a cohort of Hungarian patients allergic to this pollen.
Material and Methods
Patients
We searched clinical records of patients who had received SLIT with ragweed pollen allergenic extract during two consecutive ragweed pollen seasons (2015 and 2016), before the COVID pandemic, from six outpatient clinics in Hungary. Finally, we found the clinical records of 57 patients sensitized to ragweed pollen with clinical symptomatology of rhinoconjunctivitis and who were treated with specific SLIT. We conducted a comprehensive pilot retrospective review of these clinical records.
These records included data on both symptoms and medication use. All these patients underwent treatment with Oraltek® Ragweed for a period of 4–6 months, both prior to and during the 2016 pollen season. Of these patients, 29 (referred to as Group 1) were not under treatment with specific immunotherapy, while the remaining 28 patients (Group 2) had previously undergone immunotherapy with a different allergen sublingual extract of ragweed pollen. All patients (Groups 1 and 2) were mild polysensitized to other pollens, but their relevant allergen was ragweed pollen, meaning that their symptoms were worst and serious during ragweed pollen season in the year prior to being treated with specific immunotherapy. All patients had clinical symptomatology during the ragweed pollen season, exhibited positive results in skin prick tests for ragweed pollen, and had specific Immunoglobulin E (IgE) levels of class 2 or higher. Demographic information of these patients is shown in Table 1.
Table 1 Epidemiological data of patients.
| All | Group 1 | Group 2 | |
|---|---|---|---|
| n | 57 | 29 | 28 |
| male/female | 35/22 | 17/12 | 18/10 |
| age (IQR) | 38 (25, 44) | 39 (27, 47) | 36 (17, 43) |
Allergen extract
Sublingual allergenic preparation of ragweed pollen was used (Oraltek® ragweed sublingual spray, Inmunotek, Spain). The strength was 30,000 Therapeutic Units (TU)/mL. The content of the major allergen Amb a 1 was 10 µg/mL. The daily dose was 2 sublingual puffs, corresponding to 2 µg of Amb a 1.
Outcomes
Symptom score (SS), medication score (MS), and combined symptom and medication score (CSMS) of all patients under study during the peak ragweed pollen seasons (described below) were compared. Intra- and intergroup analysis of SS, MS and CSMS was also performed. SS, MS and CSMS were graded as described by Pfaar et al.8 Briefly, each individual symptom, such as itchy nose, sneezing, runny nose, blocked nose, itchy/red eyes, and watery eyes, was scored 0–3 and the sum was divided by 6. Medication was scored as 1 for the use of oral and/or topical (eyes or nose) non-sedative H1 antihistamines (H1A), as 2 for the use of Intranasal corticosteroids (INS) with/without H1A, and as 3 for the intake of oral corticosteroids with/without INS, with/without H1A. CSMS was the sum of SS and MS, 6 being the maximum possible value.
Additionally, we documented the number of days on which SS, MS and CSMS scores of both 0 and 1 occurred during these two pollen seasons.
Peak pollen season
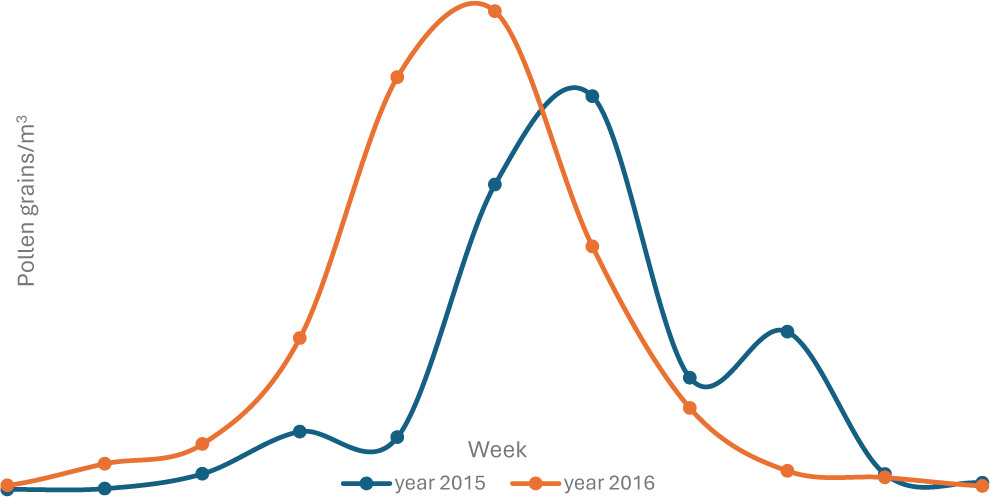
Symptoms following exposure to ragweed pollen can manifest with as few as 5–20 pollen grains/m3.9,10 We considered peak pollen season as the period in which the pollen counts were >5 grains/m3. For the year 2015, this encompassed weeks 32–39, while for 2016, it extended from weeks 31–39.
Statistics
The Excel spreadsheet (Microsoft Corp., Redmond, WA, USA) and the statistical software IBM SPSS v.20 (SPSS Inc., Chicago, IL, USA) were used. For descriptive statistics, median with the corresponding first and third interquartile (IQR) range was used. For comparative statistics, Mann–Whitney’s test (M-W) was used to compare -pollen counts between 2015 and 2016. For SS, MS and CSMS, Mann–Whitney’s test was used for intergroup comparisons, and Wilcoxon’s test for used for intragroup comparisons. The effect size, with the corresponding 95% Confidence Interval (95% CI), was also calculated. An effect size of 0.5–0.8 was considered medium, and that of >0.8 was considered large.11 Fisher’s Exact test was used to compare the number of patients who had experienced a score of ≤1 in SS, MS and CSMS. Phi coefficient was calculated to assess and to interpret the effect size of Fisher’s Exact test (very strong, strong, moderate, weak or negligible when the value was >0.70, 0.40, 0.30, 0.20 or 0, respectively).12,13
Ethics
The study was approved by the Medical Ethics Committee of the Heim Pál Children's Hospital, Budapest, Hungary.
Results
Pollen counts
No differences between the counts of pollen grains were observed for both years (Figure 1). The median and IQR of ragweed pollen grains/m3 in 2015 was 60 (31, 135), and 58 (19, 169) in 2016 (P = 0.963).
Figure 1 Counts of pollen grains during 2015 and 2016.
Safety
No systemic reactions were recorded in clinical files. Three local reactions in the oral mucosa were recorded for three patients. All these reactions were mild and resolved after few minutes without the use of medication.
SS, MS and CSMS
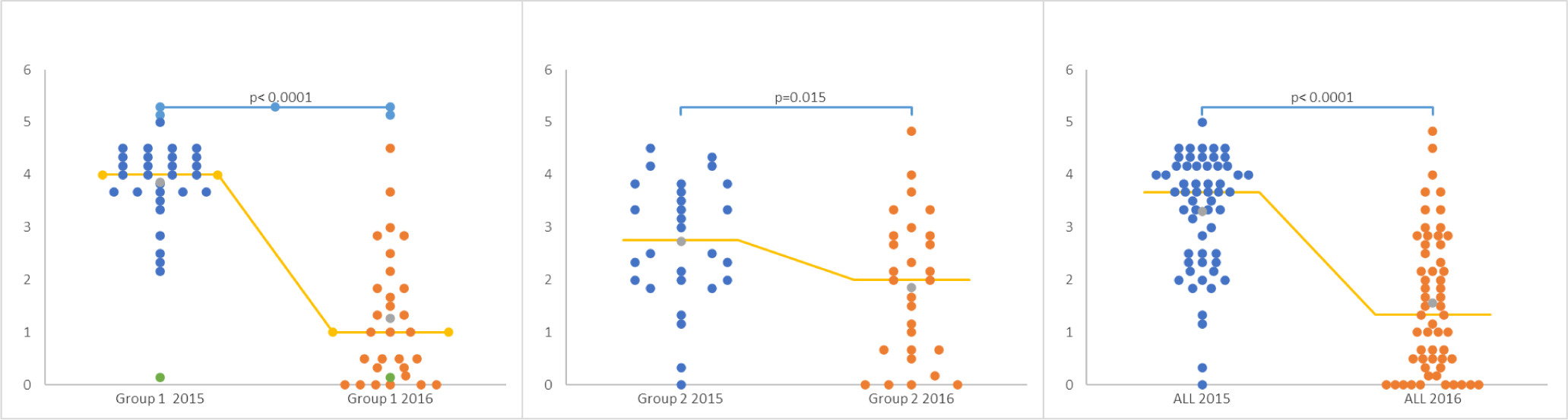
All patients experienced significant improvement in SS, MS and CSMS, including the patients who were treated previously with specific immunotherapy with ragweed allergen extract (Group 2). In the year 2015, Group 2, compared to Group 1, had significantly less SS and CSMS because of previous specific immunotherapy. Comparison between two pollen seasons showed that the effect size related to CSMS, SS and MS of all patients was large (>0.8). Table 2 shows the results of descriptive and comparative statistics. Figure 2 shows scattergrams for the evolution of SS, MS and CSMS from 2015 to 2016.
Table 2 Descriptive (median with the corresponding IQR range) and comparative (% of improvement, Wilcoxon’s test and effect size) statistics of SS, MS and CSMS of all patients and both groups. It includes comparison between both groups (Mann–Whitney test).
| Patients | Median (IQR) | Comparison intragroup | |||||
|---|---|---|---|---|---|---|---|
| 2015 | 2016 | % improvement | P (Wilcoxon) | Effect size | Interpretation of Effect size | ||
| CSMS | All | 3.7 (2.5, 4.2) | 1.3 (0.5, 2.7) | 65% | <0.001 | 1.412 (0.831, 1.992) | Very large |
| 1 | 4.0 (3.7, 4.3) | 1.0 (0.3, 1.8) | 75% | <0.001 | 2.647 (1.650, 3.644) | Very large | |
| 2 | 2.8 (2.0, 3.7) | 2.0 (0.7, 2.8) | 29% | 0.015 | 0.614 (0.144, 1.372) | Medium | |
| Comparison between groups 1 and 2 P (Mann-Whitney) | <0.001 | 0.089 | |||||
| SS | All | 1.7 (1.3, 2.2) | 0.5 (0.0, 1.0) | 71% | <0.001 | 1.286 (0.715, 1.856) | Large |
| 1 | 2.2 (1.7, 2.3) | 0.5 (0.0, 0.8) | 77% | <0.001 | 2.746 (1.731, 3.760) | Very large | |
| 2 | 1.3 (0.8, 1.7) | 0.7 (0.2, 1.0) | 46% | 0.021 | 0.714 (0.050, 1.478) | Medium | |
| Comparison between groups 1 and 2 P (Mann-Whitney) | <0.001 | 0.317 | |||||
| MS | All | 2.0 (2.0, 2.0) | 1.0 (0.0, 2.0) | 50% | <0.001 | 0.992 (0.442, 1.543) | Lage |
| 1 | 2.0 (2.0, 2.0) | 0.0 (0.0, 1.0) | 100% | <0.001 | 1.649 (0.806, 2.492) | Very large | |
| 2 | 2.0 (1.0, 2.0) | 1.0 (0.0, 2.0) | 50% | 0.021 | 0.496 (0.256, 1.248) | Small | |
| Comparison between groups 1 and 2 P (Mann-Whitney) | 0.055 | 0.080 | |||||
Figure 2 Scattergrams of CSMS for Group 1, Group 2, and all patients. Comparison of CSMS between 2015 and 2016 (Wilcoxon’s test).
The number of patients free of SS, MS and CSMS and those having a score of ≤1 for SS, MS and CSMS was highly significant for all patients and more for the patients of Group 1, with an important effect size (Table 3).
Table 3 The number of patients having a score of ≤1 of SS, MS and CSMS and those free for SS, MS and CSMS
| Patients with days with the score ≤ 1 | |||
|---|---|---|---|
| Group1 n (%) | Group2 n (%) | All n (%) | |
| CSMS 2015 | 0 (0%) | 4 (14%) | 2 (4%) |
| CSMS 2016 | 16 (55%) | 10 (36%) | 26 (46%) |
| P (Fisher's exact test) | < 0.001 | 0.121 | < 0.001 |
| PHI (effect size) | 0.617 | 0.247 | 0.489 |
| Interpretation effect size | strong | weak | strong |
| SS 2015 | 1 (3%) | 10 36%) | 11 (19%) |
| SS 2016 | 24 (83%) | 21 (75%) | 45 (79%) |
| P (Fisher's exact test) | < 0.001 | 0.007 | < 0.001 |
| PHI (effect size) | 0.801 | 0.395 | 0.597 |
| Interpretation effect size | very strong | moderate | strong |
| MS 2015 | 2 (7%) | 4 (14%) | 12 (21%) |
| MS 2016 | 23 (79%) | 15 (54%) | 38 (67%) |
| P (Fisher's exact test) | < 0.001 | 0.004 | < 0.001 |
| PHI (effect size) | 0.731 | 0.415 | 0.46 |
| Interpretation effect size | very strong | strong | strong |
| Patients with days with the score = 0 | |||
| Group1 | Group2 | All | |
| CSMS 2015 | 0 (0%) | 4 (14%) | 1 (2%) |
| CSMS 2016 | 6 (21%) | 4 (14%) | 10 (18%) |
| P (Fisher's exact test) | 0.023 | > 0.999 | 0.008 |
| PHI (effect size) | 0.34 | 0 | 0.267 |
| Interpretation effect size | moderate | negligible | weak |
| SS 2015 | 0 (0%) | 4 (14%) | 4 7%) |
| SS 2016 | 9 (31%) | 6 (21%) | 15 (26%) |
| P (Fisher's exact test) | 0.002 | 0.729 | 0.010 |
| PHI (effect size) | 0.429 | 0.093 | 0.259 |
| Interpretation effect size | strong | negligible | weak |
| MS 2015 | 2 (7%) | 4 (14%) | 6 (11%) |
| MS 2016 | 15 (52%) | 10 (36%) | 25 (44%) |
| P (Fisher's exact test) | < 0.001 | 0.121 | < 0.001 |
| PHI (effect size) | 0.492 | 0.247 | 0.375 |
| Interpretation effect size | strong | weak | moderate |
Discussion
In this study, we showed the data of a retrospective case study using a sublingual preparation under real-life clinical conditions. Improvement in SS, MS and CSMS recorded in 2016, compared to the scores recorded in 2015, was >50%, with a large effective size. Patients treated previously with immunotherapy also experienced significant improvement. The effectiveness of the treatment was not associated with systemic adverse reactions, as only three mild local reactions were reported, which indicates a high benefit–risk ratio. In fact, a low number of mild local reactions, resolved spontaneously after few minutes without medication, indicate better safety profile than the provided with other ragweed SLIT preparations, especially tablets based on lyophilised allergen extract.14–16
We acknowledge that this was a retrospective case study and had no control group to compare the results. Therefore, a great proportion of improvement (65%) could not be compared with the one obtained by using other sublingual preparations when compared to placebo, which ranged from 15%17 for a liquid glycerinated preparation to around 26% using oral lyophilizate.14–16 In any case, our results supported the use of SLIT in patients allergic to ragweed pollen, and was in line with the results of few previous publications on this type of immunotherapy in the management of this pollinosis.
Conflict of interest
The authors declare no potential conflict of interest with respect to research, authorship, and/or publication of this article.
Author Contributions
AN: Conceptualization, Investigation, Project administration, Supervision, Formal análisis, Writing – review & editing; KB: Investigation, Writing – review & editing; CC: Investigation, Writing – review & editing; BF: Investigation, Writing – review & editing; EM: Investigation, Writing – review & editing; GP: Investigation, Writing – review & editing
REFERENCES
1. Global Invasive Species Database (GISD). 2021. Species profile Ambrosia artemisiifolia. Available from: http://www.iucngisd.org/gisd/species.php?sc=1125 (Accessed May 2021).
2. Oswalt ML, Marshall GD. Ragweed as an example of worldwide allergen expansion. Allergy Asthma Clin Immunol. 2008;4(3):130. 10.1186/1710-1492-4-3-130
3. Bousquet PJ, Burbach G, Heinzerling LM, Edenharter G, Bachert C, Bindslev-Jensen C, et al. GA2LEN skin test study III: Minimum battery of test inhalent allergens needed in-epidemiological studies in patients. Allergy. 2009;64(11):1656–62. 10.1111/j.1398-9995.2009.02169.x
4. Ruëff F, Przybilla B, Walker A, Gmeiner J, Kramer M, Sabanés-Bové D, et al. Sensitization to common ragweed in Southern Bavaria: Clinical and geographical risk factors in atopic patients. Int Arch Allergy Immunol. 2012;159(1):65–74. 10.1159/000335192
5. Makra L, Matyasovszky I. Assessment of the daily ragweed pollen concentration with previous-day meteorological variables using regression and quantile regression analysis for Szeged, Hungary. Aerobiologia. 2011;27(3):247–59.
6. Clowes GHA. A preliminary communication on the treatment of autumnal hay fever by vaccination with an aqueous extract of the pollen of ragweed. Proc Soc Exp Biol Med. 1913;10(3):70–2. 10.3181/00379727-10-49
7. Canonica GW, Passalacqua G. Noninjection routes for immunotherapy. J Allergy Clin Immunol. 2003;111(3):437–48; quiz 449. 10.1067/mai.2003.129
8. Pfaar O, Klimek L, Gerth van Wijk R. Clinically relevant outcome measures for new pharmacotherapy, allergen avoidance and immunotherapy trials in allergic rhinoconjunctivitis. Curr Opin Allergy Clin Immunol. 2015;15(3):197–203. 10.1097/ACI.0000000000000164
9. Emberlin J. The effects of patterns in climate and pollen abundance on allergy. Allergy. 1994;49(18 Suppl):15–20. 10.1111/j.1398-9995.1994.tb04233.x
10. Banken R, Comtois P. Concentration of ragweed pollen and prevalence of allergic rhinitis in 2 municipalities in the Laurentides. Allergy Immunol (Paris). 1992;24(3):91–4.
11. Cohen J. Statistical power analysis for the behavioral -sciences, 2nd ed. London: Academic Press; 1977.
12. Robbins T, Lim Choi Keung SN, Sankar S, Randeva H, Arvanitis TN. Application of standardised effect sizes to hospital discharge outcomes for people with diabetes. BMC Med Inform Decis Mak. 2020;20(1):150. 10.1186/s12911-020-01169-z
13. Sullivan GM, Feinn R. Using effect size-or why the P value is not enough. J Grad Med Edu. 2012;4(3):279–82. 10.4300/JGME-D-12-00156.1
14. Kim H, Waserman S, Hébert J, Blaiss M, Nelson H, Creticos P, et al. Efficacy and safety of ragweed sublingual immunotherapy in Canadian patients with allergic rhinoconjunctivitis. Allergy Asthma Clin Immunol. 2014;10(1):55–55. 10.1186/1710-1492-10-55
15. Nolte H, Hébert J, Berman G, Gawchik S, White M, Kaur A, et al. Randomized controlled trial of ragweed allergy immunotherapy tablet efficacy and safety in North American adults. Ann Allergy Asthma Immunol. 2013;110(6):450–6.e4. 10.1016/j.anai.2013.03.013
16. Creticos PS, Maloney J, Bernstein DI, Casale T, Kaur A, Fisher R, et al. Randomized controlled trial of a ragweed allergy immunotherapy tablet in North American and European adults. J Allergy Clin Immunol. 2013;131(5):1342–9.e6. 10.1016/j.jaci.2013.03.019
17. Skoner D, Gentile D, Bush R, Fasano MB, McLaughlin A, Esch RE. Sublingual immunotherapy in patients with allergic rhinoconjunctivitis caused by ragweed pollen. J Allergy Clin Immunol. 2010;125(3):660–6, 666.e1–e4. 10.1016/j.jaci.2009.12.931